





Myxedema Coma: Oral vs. IV Levothyroxine Efficacy
A case report on Myxedema Coma: Is enteral route as good as intravenous levothyroxine in an Indian intensive care setting?
Dr Prasanth NVSN1, Dr BabySailaja K2, Dr Renuka MK3,
- Prasanth NVSN Senior Resident, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamilnadu, India.
- Baby Sailaja KAssociate Professor, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamilnadu, India.
- Renuka MKProfessor, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamilnadu, India.
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Prasanth, NVSN, BabySailaja. K, Renuka MK, 2025. A case report on Myxedema Coma: Is enteral route as good as intravenous levothyroxine in an Indian intensive care setting? Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6719
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i7.6719
ISSN 2375-1924
ABSTRACT
Myxedema coma is a rare life-threatening clinical condition in patients with longstanding severe untreated hypothyroidism, wherein adaptive mechanisms fail to maintain homeostasis. We report a rare case involving a 35-year-old male with an intellectual disability, who arrived at our intensive care unit in a comatose state. Following a thorough examination of numerous potential differential diagnoses, the patient was determined to be suffering from myxedema coma a rare presentation. The patient responded well to tablet levothyroxine administered via a nasogastric tube, achieving the desired positive outcome. Due to the exceptionally low incidence of this condition in our country, we were initially diverted into considering more frequent causes of coma. The coexistence of a pre-existing intellectual disability, coupled with factors like Herpes Zoster infection, hyponatremia, and bradycardia, posed hurdles in promptly diagnosing this condition, which was further complicated by its rarity. This case report describes the management of myxedema coma and depicts the clinical and logistic challenges faced while managing this case. This case also emphasizes the importance of readiness and the ability to adapt treatment to individual circumstances.
Keywords: intensive care, hypothyroidism, herpes zoster infection, oral levothyroxine, myxedema coma
Introduction
Thyroid hormones, triiodothyronine (T3) and thyroxine (T4) play an important role in the regulation of growth and metabolism in the body. By acting at the cellular level, they virtually control all the vital organs in the body. Hypothyroidism is an endocrine disorder characterised by deficiency of the circulating thyroid hormones. It affects almost all the organ systems leading to a chronic compensated state of homeostasis. The clinical manifestations are nonspecific and includes lethargy, cold intolerance, fatigability, bradycardia and weight gain Myxedema coma (MC) is an uncommon fatal condition resulting from decompensation of long-standing, neglected or untreated hypothyroidism due to loss of adaptive mechanisms of homeostasis, following an insult. It is often triggered by many precipitating factors such as non-compliance to thyroid medication, sepsis, exposure to cold environment, certain drugs, stress etc. The salient features of MC include altered mental status and hypothermia among other clinical manifestations. This condition is extremely rare in western countries owing to advances in the early detection of subclinical hypothyroidism by using screening tests and prompt hormonal replacement therapy. The reported incidence of MC is 2.6 cases and 1.1 cases per million per year in United states and Japan respectively. Its incidence is unknown among the Indian population owing to the rarity of the disease and failure to prioritize this condition among the potential diagnoses of coma. However, it is crucial to consider the readiness for handling certain sporadic conditions as it often carries a high mortality. The in-hospital mortality of unidentified or untreated MC was reported to be as high as 26% from a retrospective multi center cohort study in France and 29.5% from inpatient database analysis in Japan.
The main stay of treatment for MC remains unknown owing to the limited evidence from the available literature in the form of case reports and case series. The latest guidelines from the American Thyroid Association (ATA) task force recommends a starting dose of 200 to 400 mcg levothyroxine intravenous (IV) followed by maintenance dose of 1.6 mcg/kg/day. Supplementation of IV hydrocortisone (200-400 mg/ day) should be continued till clinical improvement or co-existent adrenal insufficiency is ruled out. Additionally, supportive measures such as mechanical ventilation, correction of hypothermia, fluid resuscitation, and management of any associated electrolyte abnormalities are crucial. A thorough investigation for identifying the precipitant cause is of paramount importance. In this context, we present the case of a patient from a remote village in Tamil Nadu, India who presented with this rare medical condition complicated by an associated Varicella zoster infection. We aim to outline the difficulties encountered in the clinical and logistics management of this condition despite effectively diagnosing it.
CASE PRESENTATION
A 35-year-old male, a known hypothyroid patient on irregular medication, was admitted to the critical care unit of a tertiary care hospital. He presented with complaints of fever, rash, and altered sensorium which persisted for three days. A history of exposure to active Varicella Zoster infection (VZV) was present in the family. The patient apparently exhibited signs of mild intellectual disability potentially indicative of Down syndrome; from his childhood which was however not evaluated formally. A thorough workup was not undertaken during this admission as patient did not show any cognitive impairment later. On arrival to the emergency department (ED) he was found to have altered sensorium, [Glasgow Coma Scale (GCS) score of 6 /15] for which he was intubated and placed on mechanical ventilation. His admission vitals were heart rate of 40 bpm, blood pressure of 90/60 mm Hg, and temperature of 92o F (rectal). Our priority was to initiate resuscitation by administering intravenous fluids, vasopressors, and empirical antibiotic (Piperacillin and Tazobactam) considering probable sepsis stemming from the present illness. External warmers and blankets were provided to correct severe hypothermia. Several concerns needed attention of which bradycardia associated with moderate hypotension were of initial priority. The electrocardiogram (ECG) conducted upon presentation indicated a junctional rhythm with no signs of heart block.
Laboratory investigations done in the ED revealed haemoglobin of 9.3g/dL, white blood cell (WBC) count of 14,840 cells/cubic mm, serum sodium – 128 mEq/L, serum potassium – 3.4 mEq/L. Blood gas analysis (ABG) on room air showed pH-7.22; PaCO2 – 55 mm Hg; PaO2 – 82 mm Hg, and HCO3 – 26mEq. Serum sample sent for PCR (VZV) was positive. However thyroid Function tests (TFT) sent subsequently in ICU revealed a Thyroid stimulating hormone (TSH) value > 1000 mu IU/ml and Thyroxine or free T4 (FT4) – 0.07 ng/dL.
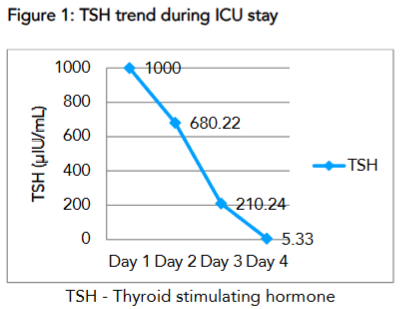
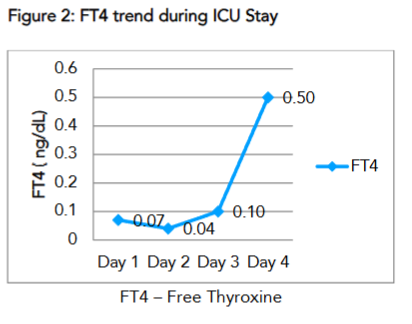
| Thyroid function Test | Day 1 | Day 2 | Day 3 | Day 4 | Reference range |
|---|---|---|---|---|---|
| TSH ( uIU/mL) | >1000 | 680.22 | 210.24 | 5.33 | 0.270 – 4.200 uIU/mL |
| FT4 ( ng/dL) | 0.07 | 0.04 | 0.10 | 0.50 | 0.93 – 1.7 ng/dL |
The constellation of symptoms alongside the elevated TSH value now prompted us to diagnose myxedema coma. We attempted to meticulously follow recommendations provided by the American Thyroid Association Task Force. Their suggestions favoured an intravenous administration of levothyroxine, but we had to modify our treatment plan due to logistic reasons. Along with intravenous corticosteroids, the patient received a single stat dose of tablet Levothyroxine 400mcg, followed by a daily maintenance dose of 100 mcg via nasogastric tube till clinical recovery and normalisation of thyroid function tests. We conducted daily follow-up of the thyroid function tests and observed a notable improvement in TSH which showed a progressive decline reaching therapeutic levels on day 4. and FT4 levels over four days.
The levels of FT4 increased incrementally and was accompanied by clinical improvement of the patient, as a result, he was extubated on day 7 of ICU stay. The subsequent day he was shifted to the ward from where he was discharged on day 10 of hospital admission.
Discussion
Myxedema coma is a medical emergency associated with high mortality if treatment is delayed. As it is a rare entity the diagnosis is often delayed or missed. In this case report, the patient with a chronic hypothyroid status, presented to emergency department with altered mental status and hypotension complicated by a VZV infection. The initial suspicion was sepsis secondary to viral infection and acute viral encephalitis which led to delay in sending the thyroid hormone assay and starting thyroxine.
Once the patient was received in ICU, the presence of hypotension, bradycardia, hyponatremia along with hypothermia and altered sensorium raised a high index of suspicion of MC, which are the hallmark features of this condition. This was later confirmed with the thyroid function test. Similar diagnostic dilemma was encountered by S Charoensri et.al. In their case report, the patient developed all the above signs and symptoms despite being on supplemental oral thyroxine which was triggered by a hospital acquired pneumonia. This study also underscores the failure of homeostatic mechanisms in hypothyroidism to any stress response.
The next hurdles encountered in the management of our patient were, firstly, uncertainty in the route and dose of thyroxine and secondly the availability of IV formulation. Due to the uncommon presentation, randomized controlled trials are not feasible to look at appropriate dosing and efficacy of various routes of drug administration. Though the IV route ensures precise bioavailability of drug, it is often associated with life threatening complications. With rapid restoration of hormone levels, excessive activation of the norepinephrine receptors leads to adverse cardiac events. Contrarily, the pharmacokinetics of oral formulation is affected by several factors, especially gastric atony seen in MC leading to unpredictable serum levels of the drug. Based on expert opinions and available case reports, the ATA task force guidelines gave strong recommendation but weak evidence for IV thyroxine as the mainstay of treatment for MC. However, owing to the rare occurrence of MC, high cost of IV formulation compared to tablets and infrequent use, the drug is not readily available in our country. Such logistic issues were reported by other investigators. Due to the above hurdles, it was necessary to customize the approach to suit our present scenario. There were a few case reports and case series which looked at usage of oral levothyroxine and its efficacy and outcomes in patients with MC. In the prospective analysis of 23 patients with MC, Dutta et.al found no significant difference in the mortality among the patients who received oral as compared to IV thyroxine. Similarly, in their study, Arlot et al. found no difference in the clinical stabilisation of the patients irrespective of oral or IV administration of levothyroxine despite rapid increase in the serum FT4 levels achieved by the later route. Hence, we resorted to administer crushed tablet levothyroxine via nasogastric tube on an empty stomach. Despite the critical condition at presentation, this patient showed notable improvement with tailored treatment, including enteral levothyroxine, corticosteroids and supportive measures such as mechanical ventilation and infection control. The patient was successfully extubated on day 7 and discharged from the hospital on day 10, highlighting the importance of early recognition and intervention in improving outcomes.
Myxedema coma, although associated with a high mortality rate, has a favourable prognosis with prompt and appropriate therapy. The patient’s rapid stabilisation following treatment also underscores the efficacy of enteral levothyroxine when IV formulations are unavailable, reinforcing findings from other case reports in similar settings. The amalgamation of the above few factors warrants our alternate enteral dose regimen to manage this medical emergency in resource limited settings.
Conclusions
Myxedema coma is relatively rare in India, with true incidence often unknown due to underreporting. Treatment typically involves supportive care and hormone supplementation, with intravenous levothyroxine being the mainstay. However, hurdles in management of these patients lie in early recognition, drug cost and availability. The financial burden of expensive medications and ICU expenses can be overwhelming for patients and their families. The limited availability of intravenous levothyroxine further complicates treatment options. In the absence of specific recommendations endorsing the use of oral levothyroxine, its utilization as an alternative option appears justifiable, particularly in settings with limited alternatives. Overall, addressing these challenges is crucial to improve outcomes and enhance the readiness of the healthcare system to handle such medical emergencies.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Funding Statement:
Nil
Acknowledgments:
None
References:
- Elshimy G, Chippa V, Correa R. Myxedema. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 14, 2023.
- Bourcier S, Coutrot M, Ferré A, et al. Critically ill severe hypothyroidism: a retrospective multicenter cohort study. Ann Intensive Care. 2023;13(1):15. Published 2023 Mar 9. doi:10.1186/s13613-023-01112-1
- Chen DH, Hurtado CR, Chang P, Zakher M, Angell TE. Clinical Features and Outcomes of Myxedema Coma in Patients Hospitalized for Hypothyroidism: Analysis of the United States National Inpatient Sample. Thyroid. 2024;34(4): 419-428. doi:10.1089/thy.2023.0559
- Ono Y, Ono S, Yasunaga H, Matsui H, Fushimi K, Tanaka Y. Clinical characteristics and outcomes of myxedema coma: Analysis of a national inpatient database in Japan. J Epidemiol. 2017;27(3):117-122. doi:10.1016/j.je.2016.04.002
- Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid. 2014;24(12):1670-1751. doi:10.1089/thy.2014.0028
- Wall CR. Myxedema coma: diagnosis and treatment. Am Fam Physician. 2000;62(11):2485-2490.
- Charoensri S, Sriphrapradang C, Nimitphong H. Split high-dose oral levothyroxine treatment as a successful therapy option in myxedema coma. Clin Case Rep. 2017;5(10):1706-1711. Published 2017 Sep 8. doi:10.1002/ccr3.1131
- Liu H, Li W, Zhang W, Sun S, Chen C. Levothyroxine: Conventional and Novel Drug Delivery Formulations. Endocr Rev. 2023;44(3):393-416. doi:10.1210/endrev/bnac030
- Dutta P, Bhansali A, Masoodi SR, Bhadada S, Sharma N, Rajput R. Predictors of outcome in myxoedema coma: a study from a tertiary care centre. Crit Care. 2008;12(1):R1. doi:10.1186/cc6211
- Roy N, Majumder A, Sanyal D, Chaudhuri SR, Sarkar S, Pathak A. Legions of Presentations of Myxedema Coma: A Case Series from a Tertiary Hospital in India. J ASEAN Fed Endocr Soc. 2020;35(2):233-237. doi:10.15605/jafes.035.02.12
- Arlot S, Debussche X, Lalau JD, et al. Myxoedema coma: response of thyroid hormones with oral and intravenous high-dose L-thyroxine treatment. Intensive Care Med. 1991;17(1):16-18. doi:10.1007/BF01708403
- Rajendran A, Bhavani N, Nair V, Pavithran PV, Menon VU, Kumar H. Oral levothyroxine is an effective option for myxedema coma: a single-centre experience. Eur Thyroid J2021;10:52–58. doi: 10.1159/00050785
- Gadaen RJ, Tummers-de Lind van Wijngaarden RF. Hypothyroid Crisis: Oral or Intravenous Treatment? A Report of Two Cases. Eur J Case Rep Intern Med. 2021;8(9):002752. Published 2021 Sep 10. doi:10.12890/2021_002752