





Nanofat and HD PRP in Aesthetic Medicine: An Overview
Overview of Use of Nanofat (fully emulsified tSVF + HD Platelet-Rich Plasma (PRP) in Aesthetic and Regenerative Medicine Cases
Robert Alexander, MD, FICS1,2
- Organization: Regenevita Health Division: Aesthetic/Reconstructive Surgery – Regenerative Medicine City: Hamilton, MT Country/Territory: USA
- Organization: University of Washington (Seattle) School of Medicine & Dentistry Division: Surgery City: Seattle, WA Country/Territory: USA
OPEN ACCESS
PUBLISHED: 28 February 2025
CITATION: Alexander, R., 2025. Overview Of Use of Nanofat (fully emulsified tSVF + HD Platelet-Rich Plasma (PRP) in Aesthetic and Regenerative Medicine Cases. Medical Research Archives, [online] 13(2). https://doi.org/10.18103/mra.v13i2.6260
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i2.6260
ISSN 2375-1924
ABSTRACT
Paper presents a brief review of cellular and biocellular uses of both cellular Stromal Vascular Faction (cSVF) elements and evolving applications of tissue Stromal Vascular Fraction (tSVF) components combined with important blood derivatives in repair and regeneration. Use of autologous stem/stromal components in human homeostasis and healing has shaped an evolving paradigm shift in many disciplines of Medicine & Surgery. Mass production or patentability of a patient’s own cell and stromal elements is a very unlikely possibility, making the use of these protections by large pharmaceutical companies unavailable. This is a factor in the financial support for research funding from these entities. The heterogeneous nature & mixture of autologous cells in the stem/stromal elements offer unique uses and efficacies, which are complimented in the actual multipotent cells and their supportive cells proving to be critically important in optimizing their functions in aging, healing and regeneration processes. Appreciation that the paracrine secretive factors play such an integral role in the regenerative milieu, have led to examination of stem/stromal cell signaling via exosomal & microvesicles paracrine communications. Discussion of terms, who are providing these services, and the realm of applications evolving is discussed. Appreciation of the contribution of “blood–derived biologicals” (in this context, meaning platelet-rich plasma concentrates or bone marrow derivatives) to enhance the repair and regenerative uses of stem/stromal elements in our own bodies. Use of Nanofat and the blood derivatives are proving to be a most safe and efficacious minimally invasive means of dealing with grafting or orthobiologic therapies.
Keywords: tSVF, cSVF, Adipose Derived Stem/Stromal Cells, Mesenchymal Stem Cells (MSC), Extracellular Matrix (ECM), Paracrine Signaling, Intercellular Communication, Exosomes/Microvesicles, Biocellular Therapies, Orthobiologic Therapy, PRP, HD PRP, Ultrasound, Chronic Wounds
THE EUROPEAN SOCIETY OF MEDICINE
Medical Research Archives, Volume 13 Issue 2
REVIEW ARTICLE
Introduction
The evolution of Biocellular Therapies has rapidly evolved because understanding the natural elements of human wound healing are now better identified, can be isolated, and concentrated (without unwanted mature adipocytes). These can then be deployed to exact targets to promote wound healing, revascularization, and repair of form/function. Once poorly understood or underappreciated, now many regenerative and aesthetic surgeons, are effectively able to identify, concentrate and deliver to specific the native microenvironments (such as autologous Nanofat and blood derivatives) to areas of need. This facilitates the ability to more quickly and effectively contributes to the healing, reparative and regenerative processes in our own bodies.

Figure 1: Photomicrograph of Limb Bud, demonstrating the close association of microcapillaries, with invested adipocytes, minimal ECM, and stem/stromal cells. NOTE: These elements represent the future contents of limbs, from neurovascular, ECM, stem/stromal cells, fat cells, bone, joints, supportive structures (ligament/tendons, muscle issues of smooth, skeletal and cardiac-types that form all elements in development.
This paper will introduce some of the key concepts and uses of the Autologous Biocellular products, and the logic of their critical importance in the reparative processes. The combination of tSVF in very small aggregates (Nanofat) plus important blood or marrow-derived products has come to be known generically as Autologous Biocellular Therapies. This paper examines the value of using these critical autologous mixtures, which have shown to comprise the unique and effective use in our natural human healing processes. Now the unwanted terminally differentiated cells (adipocyte) can be effectively removed. Nanofat, in combination (with addition blood-derivative products, has proven important in initiating the inflammatory response. When subsequently mixed with the attached stem/stromal cells, and precisely delivered to areas of need, use now offers an important contribution for repair and wound healing.
The combination of High-Density Platelet-Rich Plasma (HD PRP) and Nanofat has been increasingly studied and reported. It is recognized for its value in the ability and potential to enhance regeneration, repair, and healing in various medical conditions and tissues. These include many degenerative diseases, wounds, ischemic wounds, and musculoskeletal (MSK) disorders. This Chapter is intended to provide a brief overview of the uses of Nanofat + HD PRP/BMAC in the enhancement of dealing with the underlying mechanisms commonly found in aging, trauma, degenerative changes, iatrogenic surgical interventions, and local tissue changes. With scientific evidence evolving and increased understanding, the effective uses of this combination is approaching a stage at which “custom” blood-derived products are available. This enhances uses of stem/stromal cells to be accurately placed into degenerative or damaged targets.
Use of guided high-definition ultrasonography with needle guidance is considered of great importance for the ability to provide a concentrated Nanofat and blood-derivative to multiple precise sites. This is well documented to be valuable to wound enhancing activities. The Biocellular treatments are created from small aggregates of Nanofat enhanced with the provision of important growth factors and signal protein elements contributed by such blood derivatives. These blood derivatives are believed to be critical in the first 2-3 weeks of initial inflammatory healing, and further contribute by stimulating available stem/stromal cell activities within the wound. This is considered critical to vascularization and perfusion improvements of the areas of damaged or degeneration tissues. The three processing steps, consisting of Nanofat, HD PRP, and needle guidance with high-definition ultrasonography, ensure that the diagnosed tissue needs can be comprehensively treated.
1. Regeneration and Repair Mechanisms
HD PRP: Contains a high concentration of platelets storing the many growth factors, cytokines, chemokines plus various signal proteins (e.g., PDGF, TGF-β, VEGF, etc.) which promote tissue regeneration, angiogenesis (formation of new blood vessels), and cellular proliferation. To qualify as a high-density platelet product, it is generally agreed that concentration of baseline platelets should be equal to or >4X circulating platelets. There exists confusion as to what is the optimal concentration, but experience would suggest availability of higher concentrations provide more of the valuable contents within the platelets. This is considered an important contributor to the initial wound reactions. Many are reports show that use of select (“custom”) blood-derivative products such as leukocyte-rich HD PRP (LR-HD PRP) are important in contaminated wounds and injury.
Nanofat & Micronized Fat (tSVF): Nanofat is an important form of adipose-derived stem/stromal cells rich in regenerative cells and their stromal (supportive cells) elements. Maintaining the attached regenerative cell population to the scaffolding elements (ECM & perivascular tissues), are important in early intercellular signaling and in the wound healing processes. Nanofat provides an intact microenvironment (niche) capable of allowing early cell-to-cell communications (both sending and receiving via exosomes and microvesicles from mesenchymal and pericyte/endothelial origin). This helps immune modulation and inflammatory reduction plus participating in the vascular response so important in our wound healing and chronic degenerative applications. This early communication between the degenerative/damaged cells of the various tissue sites (recipient), and the transplanted stem/stromal cells (donor) has proven to be of great importance. Current beliefs are that the small aggregate Nanofat product provides adipocyte-free emulsified product while maintaining the native microenvironment for early response. Many practitioners have reported that this currently represents the most efficient derivative in this regenerative process and treatment. It is recognized that both Micronized or Nanofat from tSVF works with Biocellular therapeutic applications.
Nanofat (Small Aggregate tSVF): This author currently believes NANOFAT to be the most potent form for use of adipocyte-depleted tissue stromal vascular fraction (tSVF) portion of the Biocellular modalities. The logic of maintaining attachment of many stem/stromal cells is currently felt to establish early communication and response in the regenerative processes. As the Nanofat retains the important existing microenvironment, it is able to take early advantage of essential cell-to-cell communications with damaged, aging, or other parts of recipient site. Since Nanofat is essentially devoid of mature lipid-storing adipocytes it is considered an advantage in that removal of debris and extracellular free lipids would require local cellular wound responses to deal with the irritation. Without these potential impediments, it is thought to further facilitate the rate of healing and repair. This help is also additionally considered to facilitate repair/regeneration features when combined with the HD PRP. The combination has proven to be of greater importance than either the cellular OR the biological blood-derivatives in the entire early inflammatory reactions needed in wounds or degenerative sites.
2. Biocellular Applications Uses In Degenerative Processes
Musculoskeletal – Periarticular, Joint and Muscle Repair: HD PRP provides essential growth factors+ that stimulate the repair of damaged tissues. Nanofat-derived stem/stromal cell elements are capable of differentiation into the mesodermal cell groups ranging from all forms of muscle tissue, bone, cartilage, tendon/ligaments, etc. In addition, in vitro, these cells have demonstrated additional capabilities outside their germ layer. This is termed pluripotent (versus multipotent) and includes nerve tissue/Schwann sheath formation, solid organ derivatives, etc. as examples. It is important to note a key fact exists between these stem cells, that is, essentially all such derived cells have the overlapping capabilities of mesenchymal stem cells (MSCs) and their precursors (pericytes). This is important since they demonstrate the same capabilities regardless of their tissue of origin.

Figure 2: Use of sterile field Ultrasonographic Imaging for diagnostic and therapeutic Targeting of supportive structures Tissue Remodeling: The Biocellular contributions, with the synergy provided, between the addition of blood-derivatives (growth factors and cytokines/chemokines) and the stem/stromal complex, with its ECM scaffolding interact WITH the damaged or degenerative sites directly. This facilitates the repair of tissues in concert with the local existing microenvironments to help remodel and regenerate damaged, aging and degenerative structures. This impact is potentially seen to be helping slow down, or reverse, damaged/degenerative processes and assisting the needed healing processes per se. This is a result of both inflammatory modulation, immune protection and revascularization + perfusion improvements. More detail is beyond the scope of this Chapter, but is available in the peer-reviewed literature.
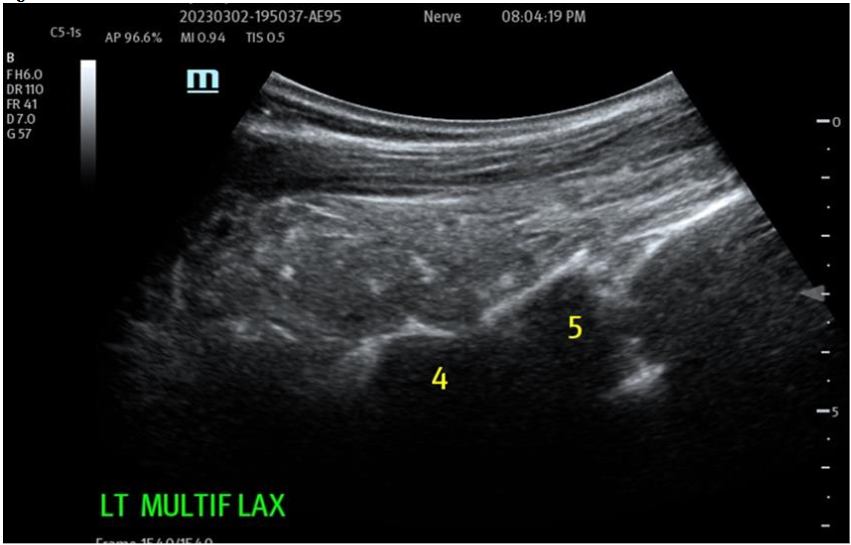
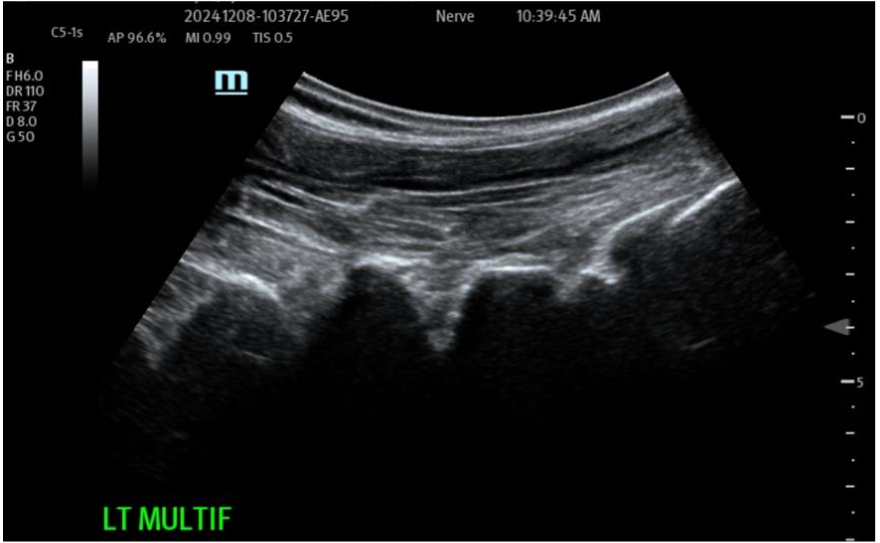

Figure 3A: Pre-operative treatment site Multifidus (loss of function dynamically) at L4-5 and above. Multiple targets IM for return of function and architecture. NOTE: Likely most common site that accompanies Lumbar facets pain seen together and is treated. Figure 3B: Post-Biocellular treatment (18 mon.) Piriformus Syndrome.
Help With Perfusion: A common factor slowing or stopping wound healing is poorly vascularized and inflamed damaged/degenerative sites. These stem/stromal cells and HD PRP are particularly effective in impact on existing and of new vessels. This is manifested by evidence of better perfusion so important in healing. As in many poor perfusion states, such as pressure sores, ischemic limb/wounds (crush, explosive, ischemic etc.), it is nearly impossible to obtain an effective or long-term repair, and reduce or avoid, recurrence without a substantial vascular perfusion.
Ischemic Tissues and Structures: As in tissue remodeling above, combining Nanofat with important growth factors (such as VEGF from cells and blood-derivatives), work together with the stem/stromal cell population. This is seen in quieting inflammatory and immunological activities, while stimulating both re-vascularization and neo-vascularization critical to wound and limb healing. Many issues follow the poorly perfused wound sites, and are believed to directly contribute to wound failures to close, or recur. Combined with proper debridement, care and enhanced granulation tissue formation, a vascular bed can be restored effectively to the point in many cases that grafting, or flap rotations, are not required.

Figure 4. A: Chronic non-healed wound from CVS groin B: Post-Marginal Debridement, treated with HD PRP/PPP+ Activated. Wound topically treated and subcutaneous injection of Biocellular mix (70% Nanofat: 30% HD PRP) at 7 Days showing granulation and marginal ingrowth at 10 days. C: Post-Operative closed wound site at 4 weeks, without use of STSG required, and minimal resultant scar formation.
Improved Skin Quality: The Biocellular combination can improve skin texture, elasticity, vascularity, age related pigmentation. The overall quality of appearance and anti-aging effects due to the regenerative effects of growth factors and stem/stromal cells demonstrate effects of enhanced circulation. These changes are often strikingly seen when the biocellular treatment is for Volumization and Nanofat transfer with placement of HD PRP within the subdermal plane as the only performed procedure. In addition, pigmentary alterations are frequently accompanying the surface changes realized.

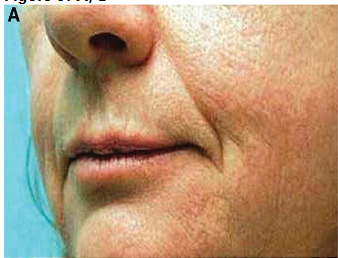

Figure 5A: Pre-Operative Facial Skin, Treatment tSVF + HD PRP. Figure 5B: Post-Treatment at 1 Year following subdermal tSVF and HD PRP. Note: pore size reduction, maintained volumetric therapy at cheeks, nasolabial fold, lip area, much improve vascularization.
Other Established Uses With Biocellular Therapy:
Biocellular therapy has been shown to improve outcomes and rate of healing in burns, trauma, and complicated bone and soft tissue surgeries (such as in flap procedures). It is documented to have a safe and efficient impact in these types of injuries, particularly if activated on superficial wounds with use of human recombinant thrombin. This protocol favorably impacts not only on the rate of wound and marginal responses, but also MUCH less difficulty in stimulating essential granulation tissue. In effect, this also providing for less frequently demanded dressing changes for patients plus a more rapid closure. Use of activated HD PRP has also permitted surgeons to avoid placement of external drains in many cases. Further, this impact has also modified actual indications for use of flaps and skin grafting in elderly patients. The advance of not having an additional, entirely new wound site in some frail patients makes care more comfortable. This avoidance of stress with patients having limited ability to tolerate more surgery/anesthesia while maintaining the ability to achieve the full wound repairs essential to the tissues involved.
3. Biocellular (Orthobiologic) Uses in Musculoskeletal (MSK) Disorders
Tendon and Ligament Repair: Inclusion of several growth factors found in HD PRP, contribute to the healing of tendons and ligaments. Of importance, Nanofat stem/stromal cells can differentiate into tenocytes and limit overreaction of fibroblasts trying to form scar tissues. This aids in tendon restoration of elasticity and ligament strength are critically important in regeneration and prevention of recurrence. Further, many such regenerations result in little, or no, scarring evidence in the long-term follow up examinations and imaging.

Figure 6: Case 3: One-year post-treatment with Biocellular targeted Treatment. NOTE: Completely normal appearance of Achilles Tendon with restoration of normal echotexture of tendon without Scar formation and no bursal effusion residual.
Bone Healing: Biocellular treatment promotes bone healing through the stimulation of osteoblast activity in the osteogenesis processes. Nanofat-derived stem/stromal cells are thought to further enhance bone regeneration by differentiating into osteoblasts (as well demonstrated In Vitro and In Vivo uses. This has proven to be helpful in many circumstances of fibrous non-union or contaminated fractures, particularly using leukocyte-rich HD PRP LR-PRP) blood derived products in open, contaminated wound situations.
Cartilage Healing: Although Hyaline Cartilage is very slow to repair due to lack of internal vascularity, it has been shown to occur. More often the response is towards a form of fibrocartilage, which does often improve the comfort in the areas of intra-articular structure and osteoarthritis. It is also known that the addition of low hematocrit form of HD PRP in combination with the Nanofat also has impact to this process and helps with favoring a desired type of a “benign” inflammatory environment. When some blood derivatives only are utilized without Nanofat, a “flare” of inflammatory response may be encountered following such placement. This event may be significantly reduced simply by reduction of inflammatory reaction seen by modulation provided by Nanofat addition. Further, use of only blood-derivatives not only may flare, but may often require several interval treatments to provide much or long-term help.
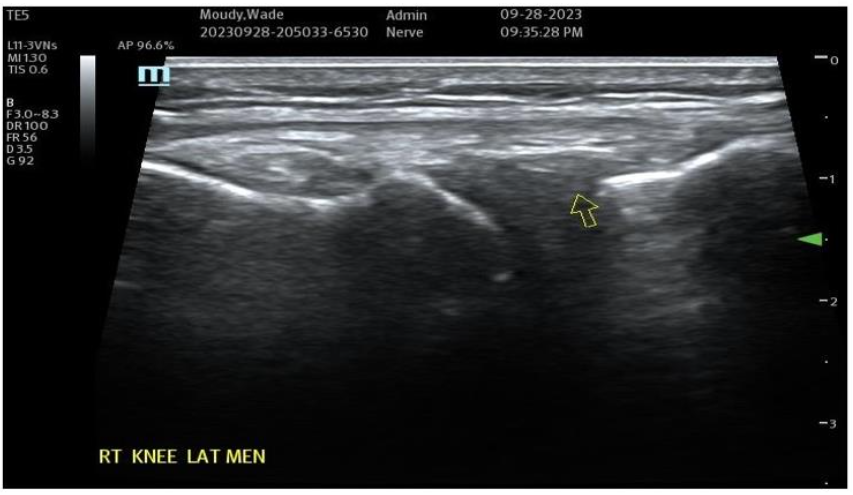

Figure 7A: Pre-Treatment Medial Meniscal/MCL Damage and Inflammatory Changes. Figure 7B: Post-Treatment with Biocellular Product (Orthobiologic) mix of Nanofat + HD PRP, this target Medial Meniscus areas (1 target of many in Knee).
Muscular/Scar Repair: The ability of the biocellular mixture in the repair of torn, damaged or failed muscular structures is quite remarkable. This is accentuated in light of the difficulties relative to internal muscle repair of damage as seen in trauma or invasive surgery. Often rapid responses are realized, with both avoidance of scarring OR the reduction of scarring present has been well shown in many clinical cases. With enhanced vascularity and perfusion within the damaged muscular tissues, limited or less scar formations are important advantages. Some Providers define a ”toxic” inflammatory reactions as those that lead to tissue scarring. This is seen in unstable or excessive inflammatory scar reactions which are not desirable. Avoidance of excesses or hypertrophic scarring is a clear advantage to wound healing and long-term outcomes for patients. Nanofat stem/stromal elements are capable of forming smooth, skeletal and cardiac muscle. Biocellular therapy helps a more stable and less inflammatory environment. This coupled with the existing damaged muscle can lead to excellent reformation and return to function. This modality is becoming very common to include direct intramuscular guided placements to improve the internal architecture (sonographic echotexture restoration), and confirmed with dynamic testing of the musculature during the ultrasound from diagnostic and treatment when tracked in follow up examinations.
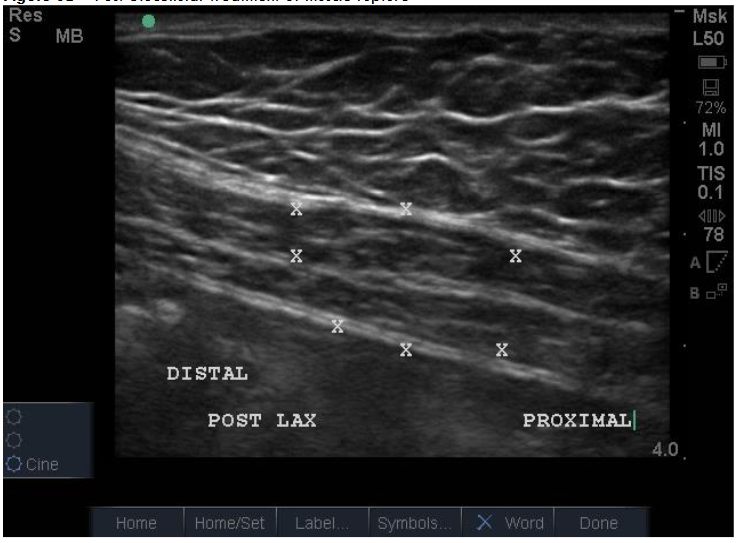

Figure 8A: Traumatic Rupture Right Rectus Abdominus (American Football Helmet) Defect, Pre-Treatment at 48 hours. Figure 8B: Post-Biocellular treatment of muscle rupture, patient returned to full-contact professional football within 2 weeks pain free. Treatment was with use tSVF + HD PRP+ (activated with human recombinant thrombin) at 70% tSVF and 30% HD PRP (by volume). Patient pain free at 1 week, returned to full contact in two weeks without recurrence or pain. Post-treatment exam at approximately 4 months. NOTE: no visible scarring resulting from intramuscular tear.
Biocellular Uses In Neuropathy:
Many examples of important epineural-dissections and fascial inflammatory conditions have been improved with applications of a biocellular mixture, including use of PPP products are becoming a very common, safe and effective protocols. Often by “resting” simulated, entrapped or irritated peripheral sensory nerves, long-term relief is attained. This is considered partially due to fibrin conversion which may provide addition protection while reducing the nerve axonal irritation. This has become a more effective and commonplace option, particularly in areas such as inflamed fascia as in the thoraco-lumbar fascial (TLF), Piriformis/Sciatic areas, and Ilio-Tibial Band (ITB). The PPP or biocellular elements are also capable of providing soothing impacts of the area, plus helping limit inflammatory response and promote recovery. It may be a combination of the anti-inflammatory action of the stem/stromal cells and the fibrinogen contained to form a fibrin protection of irritated nerve structures often missed in regenerative efforts and not available in invasive surgical procedures.
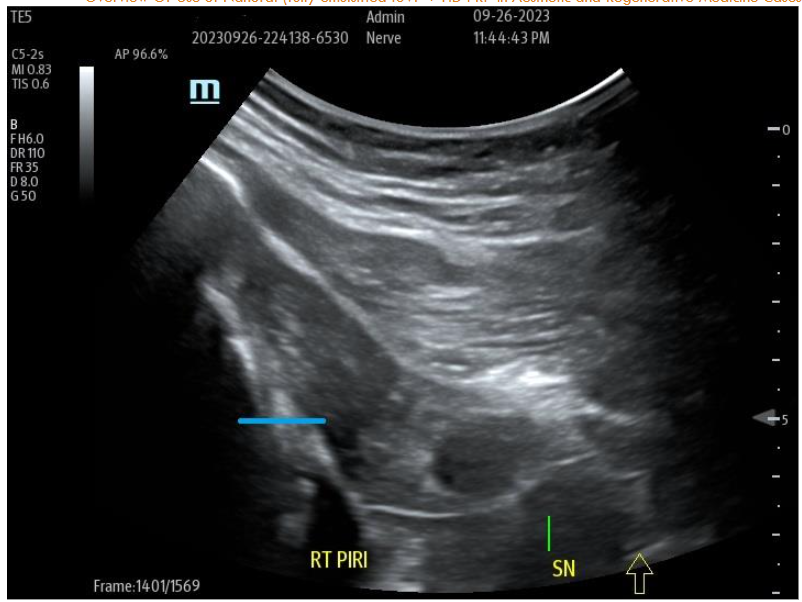

Figure 9A: Pre-Treatment U/S of degenerative Piriformis (sciatic radicular symptoms) no history of trauma, degenerative Pattern within Piriformis musculature with loss of muscle echotexture. Figure 9B: Post-treatment of site at nine months post-treatment with tSVF + HD PRP (70% tSVF: 30% HD PRP (6X – concentration HD PRP) with return of improved muscular echotexture and elimination of radicular sciatic symptoms.
Pain Reduction:
The anti-inflammatory properties of a COMBINATION of NANOFAT + HD PRP/BMAC can often contribute to help reduce pain and improve function in MSK disorders. There are many reports dealing with osteoarthritis and tendinopathies, muscle tears, and periarticular essential tissues. This anti-inflammatory action, coupled with the revascularization often results in long-term improvements. It is important to not underestimate another derivative of the blood products, specifically, Platelet Poor Plasma (PPP) which contains additional growth factors and other important wound healing elements which have shown to sooth and “rest” inflamed bursae and nerve irritations.
6. Biocellular (Orthobiologics In MSK): Why the Combination Works:
Synergistic Effects: The Biocellular combination leverages a growth factor-rich environment provided by blood-derivative along with the stem/stromal cell-rich properties of Nanofat, the active paracrine communication, and the bioactive ECM together. This synergy enhances tissue regeneration and repair beyond what either component could achieve alone. The stem/stromal cells are highly capable of contributing to the repair and autologous ECM and its replenishment of scaffolding is necessary for effective wound healing.
Multifaceted Approach: The dual approach of such combined contributors also addresses both the cellular and biochemical aspects of healing processes. HD PRP (or BMAC) provides the biochemical signals necessary for healing. NANOFAT supplies the cellular building blocks, PLUS, providing modulation of the site induced inflammatory and immunological reactions. This may help by resulting either by addressing causation of injury or degeneration during the early and later wound healing cascade.
Enhanced Intercellular Communication: The growth factors in Blood-derivatives can stimulate the migration and proliferation of stem/stromal cells from Nanofat may lead to more complete regeneration and repair. By provision of a transplantable, “intact microenvironment” (Nanofat), the ability to more rapid site ability to “send and receive” much needed signaling facilitates the cellular responses. This is a complex environment during the healing processes, and helps insure that needed elements are available in early degenerative/wound healing regardless of causation. Essentially, the advantages of immediate intercellular communications and early response (both from grafted cells as well as resident damaged cells) is believed to permit earlier and more effective tissue responses important in the healing cascade.
7. How HD PRP & PPP (from peripheral blood or bone marrow are isolated:
At the time of this writing, there are many misconceptions and more than 55 existing systems claiming to provide PRP. This number often confuses practitioners by claims often made by representatives as to the content or potency of their products. This is a valuable documentation tool to track patient outcomes and effectiveness of providers. It is often not practical to do the blood derivative without use of known and proven concentration systems which have shown to accomplish the HD PRP concentration if not confirmed via clinical baseline to concentration via hemocytometry.
Simple spinning of blood (single or double) and removal of the “PRP concentrates” has been shown to rarely reach the level of 2-3X circulating platelet level. As this is commonplace, some practitioners have concluded that PRP concentration does not work, or perhaps is ineffective. Many providers do not understand the various protocols, system capabilities, or actually document the actual concentrations achieved. Optimally as a general rule, using concentrations of >4 times circulating platelet is considered the threshold. It is important to realize that only a few protocols ACTUALLY achieve that platelet concentration and concomitant platelet. Those who do not actually test or have access to a hemocytometer are often left with the claims of industry representatives. It is important to know the delivered concentrations to be able to determine how they impact outcomes. Recording the delivered concentrations is VERY helpful to be able to compare results in patients. It is important to clearly document the concentrations used, which is an important metric in tracking and determining actual outcomes over longer time frames.
There are some available systems which can provide consistently and accurately without this testing. If practices are unable to test the baselines and concentrations, it is strongly recommended that you use one of those systems and its protocols.
It is beyond the scope of this Chapter to provide a comprehensive explanation and identification of all such systems. We would recommend the above reference on the subject, and learn and appreciate the gradual customization capabilities of different blood-derivatives and how to select which to use in various applications and situations. It is well established that the importance of such concentrations directly impacts the proliferation and migration reactions of the stem/stromal cells themselves.
8. Overview Of How Nanofat Is Created:
The process of Nanofat creation begins with routine use of sterile, closed syringe microcannula lipoaspiration (microcannula, meaning less than 2.4 mm OD) to acquire subdermal adipose tissue complex (ATC). Initially, utilization of a multiport infiltrator cannula (2.2 mm and 15 cm length) to uniformly and effectively distribute the important “carrier suspensory fluid” (often referred to as tumescent fluid). This solution is a very dilute local anesthesia bearing liquid essential to permitting the gentle and easy removal of the ATC. The local anesthesia and epinephrine solution used by this author is found below. This low concentration of local and vasoconstrictor is easily removed via centrifugation prior to final development of the Microfat (partially emulsified), or fully emulsified Nanofat product. It is VERY important to then perform a task of “pre-tunneling”, which means the multiport infiltration cannula is moved many times in the same plane and areas to provide thorough distribution of the dilute carrier fluid (with very dilute local, 0.05-0.1% and 1:1 million to 1:500,000 epinephrine). This provides both patient comfort and to effectively mobilize the tSVF. Rather than think of this fluid as a local anesthetic only, remember its most important contribution is to allow the tumescent solution to become a suspension fluid for gentle extraction of loosened tSVF from the subdermal ATC.
NOTE: The most overlooked technical and important step is effective “pre-tunneling”. It is simple to do and yields the best tSVF for grafting and patient comfort with distribution of the local solution contained. This should be consistently a part of the process, which means moving the infiltration cannula within the same plane and tissues as planned for harvesting multiple times. As noted, this, in effect, further separates the tSVF from the subdermal ATC, while also effectively spreading the contained local anesthetic more thoroughly for patient comfort. The author’s uses microharvesting technique for recovery of the small aggregate, mobilized tSVF components. This is completed via use of gentle subdermal lipoaspiration via a standard luer syringe (20cc-50/60cc) and low-pressure harvest via a 2.2 mm and 15cm length spiral microcannula harvester.
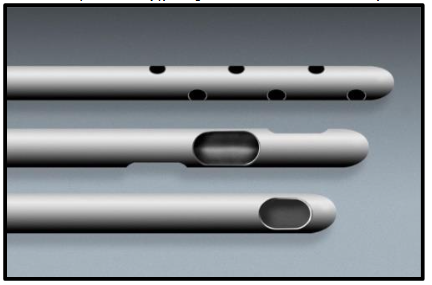


Figure 10A: This is an optional universal lock system to be used externally on the syringe plunger (NOTE: There is also a lock system that is mounted to the syringe flange). Figure 10B: Close of images of the microcannulas: Top: Multiport Infiltrator close up Middle: Off-Set Spiral Harvester (Carraway) close up Bottom: Single Port Injection (comes in varying lengths and diameter (up to 19 gauge), use in neural or hydro-dissection (PPP) applications and grafting. Figure 10C: Sample of sterile luer-to-luer transfer used in maintaining sterile chain in centrifugation, graduated 2.4, 1.4, and 1.2 internal diameters for micronization and prior to Nanofat creation, and for loading treatment syringes depending on surgeon preference or site needs.
The harvested specimen is passed off the sterile field and back table, and is next centrifuged for 3 minutes at approximately 800 G-force to create a gradient density separation into three distinct layers. The lower layer is termed the “infranatant fluid”, middle layer the tSVF graft material, and the upper layer of free lipid (oil like) (“supernatant fluid”). See FIGURE 11. Following centrifugation, the infranatant is discarded with excess local and mostly cellular debris. The graft (tSVF) is transferred via sterile luer-to-luer to a 20cc sterile syringe for return to the back sterile table. NOTE: Sterility of the graft tissues is ensured by use of sterile luer transfers (with the transfer used to retrieve the graft STAYING with the actual centrifuged syringe and discarded. Through this process, the sterile product within the new syringe can be returned to the sterile field leaving the luer-to-luer transfer with the centrifuged original harvesting syringe. Once taken within a new sterile syringe, it can be taken to the sterile back tray or table for processing of the Microfat first (partial emulsification) and then taken to completion of Nanofat creation.

Figure 11: Post-Centrifugation, Density Gradient Separation Established At 800 G-Force, 3 Min. NOTE: Top Layer: Free Lipid (not desired); Middle Layer: tSVF graft (saved & used); Lower Layer (infranatant) excess local/fluid mix + significant debris (not desired or used).
Upon return to the sterile back table, the graft-only layer is then passed multiple passes (approximately 10-20 times) through 1.4mm, then 1.2 mm respectively. This provides a “partially emulsified “product, and some providers use this known as: Micronized tSVF for volumization or orthobiologic applications. This effectively results in the majority (approximately 40-60%) of mature adipocytes being removed, effectively reducing the significantly larger aggregates and many unwanted adipocytes (due to size differential and sheer forces). Some practitioners elect to use it in a micronized form, but more experienced users move to further reduce the aggregate size. This is accomplished via a chamber-less, screen (offset 600 u/400 u) device which effectively eliminates (approximately 99%+) the remaining large, mature adipocytes. This effectively leaves the viable stem/stromal aggregate with very small attachments to the ECM and small vessels attachments. Testing is now being done for a novel luer-to-luer set that is believed to be a more efficient and effective way to create the micronized product prior to developing the Nanofat product with less number of passes through the transfers.


Figure 12: Chamberless NANOFAT screen; Graduated ID Luer-to-Luer Transfers *Multiuses in Micronizing and Nanofat. Figure 13: Loading of disposable chamberless NANOFAT screen. • Upper port is used for transferring the micronized (partially emulsified) tSVF through the screen to create Nanofat • NOTE: Recommend use of 0.6-0.7 cc PPP PRIOR to pushing the tSVF to facilitate easy transfer. • Author uses 10cc-20cc Sterile syringes for the transfers (recipient syringe-horizontal) to same size syringes.
NOTE: A very useful suggestion to users of this chamberless Nanofat device is to use a small volume of patient’s PPP (approximately 0.7-0.8 cc) prior to passage of the micronized graft through to a sterile receiving syringe. This makes the final full emulsification significantly easier than passage with a dry Nanofat device. Many experienced practitioners are electing to do an additional centrifugation to remove any additional free lipids (however, this is not a universal decision), and it is not established that it enhances the efficacy of the graft mixed with the blood derivative (either HD PRP or BMA). The determination of the actual nature and volume needed for a specific treatment (e.g. volumization grafting, or MSK treatment) must include a calculation of exact volume needs of the case. This is determined by the Provider. In MSK therapy, it is important to remind of the important value of using of a high quality, needle-guidance system as recommended. Diagnostic volumes, identified locations for precise placement and recording is important to do outcome tracking. NOTE: It is considered of high importance to use the Ultrasound technology in combination with review of quality imaging (typically MRI, CT, and X-Rays).
In Orthobiologic applications (MSK) the ratio recommended is in a ratio of 70% Nanofat graft: 30% concentrated blood-derivative proportion as determined by volume. This is the final Nanofat product consisting of very small aggregates with the concentrated blood-derivative to re-suspend the Nanofat to injectable form. With significantly higher vascular perfusions often encountered in aesthetic surgery (particularly in the head and neck region), the Biocellular Regimen concentration has been proven biologically effective for grafting augmentations, using a ratio of 90% graft:10% concentrated blood derivative (HD PRP or BMAC) as compared with orthobiologic targets. This product can be used topically in open wounds, or injected into the existing subdermal fat deposits (for volumization and vascular-related or damaged skin surface changes). In addition, in many instances of lipodystrophic patients, practitioners have the option of providing grafts that are “Cell Enriched” via use of isolate cSVF derivative, in circumstances where maintaining maximum volumes is desired. More on this option later in this Chapter.
Once completed, the Biocellular Regimen (mixture) may then load into the desired sterile syringe sizes an indicated for deployment to the desired treatment areas. The concentrated blood-derivative offers insurance that the proper placement is maintained due to the fibrin generated with contact with collagen (recipient targets and graft). To ensure that effect, many use a dilute CaCl2 solution to help reduce any anticoagulant contained in the processing of the blood derivatives (PRP/PPP and BMA).
Advances In Cell-Enrichment Of Nanofat In Biocellular Treatments
In the last 5-8 years, multiple reports of use of cSVF have emerged as effective therapeutic regimens for both aesthetic and reconstructive surgery (particularly augmentation grafting for improved retention and volumization). This has likewise proven advantageous in regenerative medicine (Orthobiologics, MSK, and for potentials for systemic deployment). The ability to use these cells in aesthetic plastic surgical cases involve use of Nanofat (tSVF) small aggregates, to accompany the isolated cSVF (which needs to find attachments for early functions). When delivered simultaneously, it is believed to be an important factor in use of the Biocellular Therapy. In Orthobiologic uses (MSK), the same combination appears to have a significantly positive effect, particularly in cases of extreme deterioration, damage and in cases of prolonged duration of chronic tissue inflammatory degradation. The chronic depletion of the local stem/stromal cells will impact the site’s capability to augment or repair. In some advanced cases, this depletion is considered to be a challenge for use of Nanofat + HD PRP ONLY relative to healing, but with the added cellular concentrations (cSVF) provides a more accelerated and effective therapeutic modality. In both applications and indication, there appears to be clinically significant improvement in those cases in which Biocellular Therapy may be indicated.


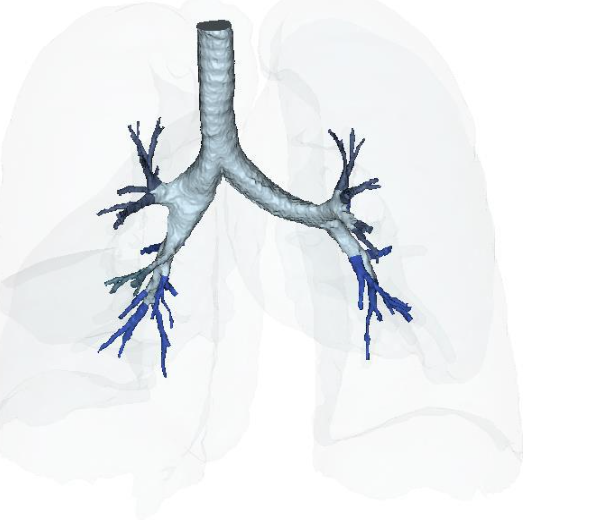
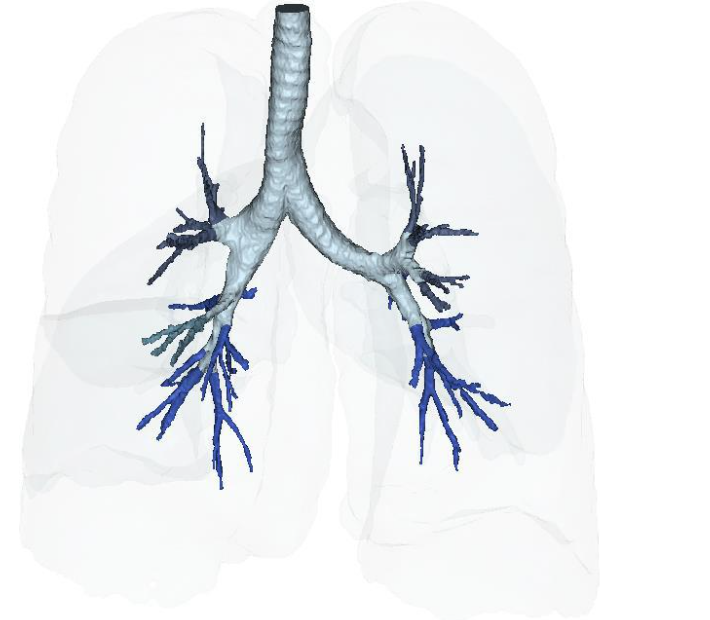
Figure 15A: Vascular Perfusion Changes Pre-treatment of Long COVID-19 lung vascular changes. Figure 15B: Post IV deployment cSVF therapy in Long COVID-19 clinical trial NCT04326036 at 6 months. Figure 16A: Restoration of the near terminal Tracheobronchial tree, pre-treatment showing blunting and loss of distal bronchioles. Figure 16B: Post-treatment IV cSVF with elongation of distal bronchiolar tree at six months. NOTE: With this post-treatment changes with cSVF was an accompanying reduction in airway resistance and pressures within the lung parenchyma. Higher pressures in pre-treatment image were located in the Upper lobes (less efficient and higher pressures in pre-treatment), whereas the shift from upper to lower lung parenchyma accompanied improve vascular supply and perfusion, and patients no longer experienced difficulties in inhalation capabilities.
Conclusion:
The Biocellular potential offered by use of Nanofat with inclusion of concentrated blood-derivatives has rapidly been recognized as delivering significant promise for enhancing tissue regeneration, repair, and healing across a wide range of medical conditions. Their synergistic effects create a robust environment for use of patient’s own cellular and blood-derived products enhance repair and healing, making this combination the most powerful tool in modern regenerative medicine. A great advantage for such uses of minimally invasive options to open surgical efforts, and using only a patient’s own Autologous Tissues. These therapeutic modalities are not going replace the needs for invasive surgeries, however, should be thought of as complimenting the options for less invasive procedures OR assisting in necessary surgical procedures by aiding in wound healing and repair. The options of using autologous and minimally traumatic care of soft tissue (muscular, tendon/ligamental, fibrocartilage, and ischemic areas are a very attractive and effective option. Ongoing clinical reports and clinical studies are now reporting or in progress and need standardization for practitioners to be able to speak the same language. Once minimally invasive options are understood, the return of form and function of the tissues will become a reality and be recognized as a paradigm shift in Medicine and Surgery. This information will be enhanced with more case and series documentations and advancing with addition of controlled, blinded studies. These uses are rapidly emerging, and often with optimized protocols for use, and will provide better understanding of the potential. Many uses of these therapeutic approaches have shown excellent safety, efficacy and efficiency. After the last 15-20+ year experiences, it is becoming a great alternative and likely represents the future of many regenerative demands. With the availability of bioactive combinations such as Biocellular Therapy, it is likely to improve the response rate and successful regeneration with the growing understanding of the exosomal/microvesicle communication so prevalent in the cSVF group of mesenchymal stem cells (MSC). This is probable to enhance the ability for Providers to become very active in the process of healing. Remember that ALL cells communicate via these paracrine functions, however, the stem/stromal group of cells are known to be very effective at receiving and responding to tissue signals put out in the degenerative or wound healing processes. In summary, both adipose t-SVF in the form of Nanofat in combination of truly “customized abilities” of concentrated Blood-derivatives) are coming very soon. They offer the promise of the ability to obtain maximal outcomes, while avoiding many open invasive cases (or improving their outcomes in cases where even total joint replacements). These are rapidly emerging as powerful tools in the fields of immunomodulation and pain management. Their ability to influence immune responses and promote healing processes positions them as promising candidates for many future therapeutic applications in regenerative medicine. The role of adipose tissue derived Nanofat and unique custom blood derivative are revolutionizing Regenerative Medicine. The control of immunomodulation, inflammatory mediation and pain reduction are becoming an accepted reality in Medicine and Surgery. It is so important to recognize and optimize some of the potentials of autologous adipose derived abilities. These therapeutics can be designed to take advantages of both inflammatory and anti-inflammatory effects, making it a critical player in maintaining systemic metabolism and homeostasis. The stromal vascular fraction (SVF), which includes a heterogeneous population of cells such as adipose-derived stem/stromal cells, has shown promise in treating autoimmune and neurodegenerative diseases. Research indicates that SVF can offer some T-Cell (TH1) cell-mediated advantages in pathology. It is suggested that these potentials in modulating immune responses, particularly helping antigen-presenting cells such as macrophages, dendritic, and B Cells and other Treg (T cell regulatory) cells, may help provide an important immunomodulatory effect. This could become crucial for conditions where inflammation plays a central role in many pathologies or degenerative disorders. Nanofat, a refined form of adipose tSVF, has been studied for its efficacy in pain relief, particularly in conditions like osteoarthritis. The MSC/Pericyte and monocyte populations are known to attract Treg cells to targets needing maintenance or to help repair. With advancements in understanding the full potential applications for safe and effective uses of cSVF for cell-enrichment protocols in aesthetic and reconstructive surgery, orthobiologics (MSK), and general wound healing is proving of great value. This, plus, the ability of limited need for more invasive interventions while providing an effective autologous modality have resulted in near complete restoration of damaged tissues and return of function. Clinical and preclinical studies have demonstrated that Nanofat significantly reduces pain symptoms and protects cartilage from damage. The mechanism behind this pain relief is thought to involve the promotion of angiogenesis and collagen deposition, which are essential for tissue repair and regeneration. Both Nanofat and tSVF along with blood-derivatives have shown similar benefits in pain management, indicating that they may be interchangeable in certain therapeutic contexts. The ability of these adipose-derived products to enhance healing and reduce inflammation makes them valuable in treating chronic pain conditions. In conclusion, both adipose-derived NANOFAT with select blood-derivatives are emerging as powerful tools in the fields of immunomodulation and pain management. Their ability to influence immune responses and promote healing processes positions them as promising candidates for future therapeutic applications in regenerative medicine.
References
- Zuk PA, Zhu M, Mizuno H, Huang J, Futrell JW, et al. (2001) Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng 7: 211-228.
- Zuk P (2013) Adipose-Derived Stem Cells in Tissue Regeneration: A Review. Stem Cells Pg: 35.
- Alexander RW (2012) Understanding adipose-derived stromal vascular fraction (AD-SVF) cell biology and use on the basis of cellular, chemical, structural and paracrine components: a concise review. Journal of Prolotherapy 4: 855-869.
- Everts, P., Podesta, L., Alexander, RW (2024), Comprehensive Guide Of Cellular Blood Derived & MSC cell based Autologous Prep Tissue Repair, Regeneration, and Wound Healing. Intertech Open.1006741, Sept 2024, Doi: 10,5772/intechopen.1006741
- Alexander, Robert W., (2019) “Overview of Cellular Stromal Vascular Fraction (cSVF) & Biocellular Use of Stem/Stromal Cells & Matrix (tSVF +HD PRP) in Regenerative Medicine, Aesthetic Medicine, and Plastic Surgery”, Journal of Stem Cell Research, Development & Therapy, Doi: 10 24966/SRDT-2060/S1003.
- Everts, P., Onishi, K., Jayaram, P. et al. (2020) Platelet-rich Plasma: New performance understandings and therapeutic considerations in 2020, Internat J Molecular Sciences, 7794.
- Etulain, J. (2018), Platelets in wound healing and regenerative medicine. Platelets, 29 (6): 556-568.
- Hu, M, Borrelli, M, Lorenz, H. et al. (2018) Mesenchymal stromal cells and cutaneous wound healing: A comprehensive review of the background, role, and therapeutic potential. Stem Cell Internatl, 6901983.
- Everts, P., Podesta, L., Alexander, RW (2024), Comprehensive Guide of Cellular Blood Derived & MSC cell based Autologous Prep Tissue Repair, Regeneration, and Wound Healing. Intertech Open.1006741, Sept 2024, Doi: 10,5772/intechopen.1006741
- Alexander RW (2016) Understanding Mechanical Emulsification (Nanofat) Versus Enzymatic Isolation of Tissue Stromal Vascular Fraction (tSVF) Cells from Adipose Tissue: Potential Uses in Biocellular Regenerative Medicine. Journal of Prolotherapy 8: 947-960.
- Alderman, D, Alexander, RW, Harris, G. et al. (2011) Stem cell prolotherapy in regenerative medicine: Background, theory, and protocols. J Prolo 3(3):689-708.
- Gnecchi, M.; Zhang, Z.; Ni, A.; Dzau, V.J. Paracrine mechanisms in adult stem cell signaling and therapy. Circ. Res. 2008, 103, 1204–1219.
- Caplan, A. (2007) Adult mesenchymal stem cells for tissue engineering versus regenerative medicine. J Cell Phys, 213(2): 341-347
- Gentile, P., Gharles-de-Sa, L et al. (2020) Systematic Review: Adipose-derived mesenchymal stem cells, platelet-rich plasma and biomaterials as new regenerative strategies in chronic skin wounds and soft tissue defects. Internatl J. Molecular Sciences, 21(4): 1236.
- Everts, P, Podesta, L, Alexander, RW (2024) A comprehensive guide of cellular blood derived and mesenchymal stem cell-based autologous biological preparations for tissue repair, regeneration, and wound healing. Internatl J. Molecular Sci. . 2(20): 7794.
- Xu” P.. Yu, Q. Juang, H. et al. (2019) Nanotat increases angiogenesis and fat graft survival via VEGF/TGF’-beta and HGF signaling. Intematl J Molecular Sciences. 20(21) 5390.
- Maltllli. N. 0lira. F. I”rizziero. A. et al. (2020) Guidelines for the use of platelet-rich plasma in the management of musculoskeletal pathologies. Muscles, Ligament and Tendon J. l0(3): 432.
- Pas. H. Winters. M. Haisma. H. et al. (2017) Stem cell injections in knee osteoarthritis: A svstematic review of the literature. Brit J Sports Med. 5l(15): 1125- 1133.
- Caplan, A. l. (2007). Adult mesenchymal stem cells for tissue engineering versus regenerative medicine. Joumal of Cellular Physiology. 213(2). 341-347.
- Nakagami, H.; Maeda, K.; Morishita, R.; lguchi, S.; Nishikawa, T.; Takami, Y; Kikuchi, Y; Saito, Y.; Tamai, K.; Ogihara, T.; et al. (2005) Novel autologous cell therapy in ischemic limb disease through growth factor secretion by cultured adipose tissue-derived stromal cells. Arter. Thromb. Vasc. Biol. 25: 2542-2547.
- Shantsila, E.; Watson, T.; Lip, G. (2007) Endothelial progenitor cells in cardiovascular disorders. J. Am. Coll. Cardiol. 49: 741-752.
- Alexander, RW. (2019) Overview of cellular stromal vascular fraction (cSVF) and biocellular uses of stem/stromal cells and matrix (tSVF + HD-PRP) in regenerative medicine, aesthetic medicine, and plastic surgery. J Stem Cell Res Dev. DOI 10/24966/SRDT-2060/S1003.
- Dicker, A.; Le Blanc, K.; Astrdm, G. et al. (2005) Functional studies of mesenchymal stem cells derived from adult human adipose tissue. Exp. Cell Res. 308: 283-290.
- Gimble, J.; Katz, A.; Bunnell, B. (2016) Adipose-derived stem cells for regenerative medicine Circ. Res. 100: 1249-1260.
- Tonnard, P, Vaepaele, A., Peeters, G., et al. (2013) Nanofat grafting: basic research and clinical implications. Plas Recon Surg. 132(4):1017-1026, Doi: 10.1097/PRS.0b013e31829fe1b0.
- Sadati, K., Corrado, A., Alexander, RW. (2006) Platelet-Rich plasma (PRP) utilized to promote greater graft volume retention in autologous fat grafting. Amer J Cosm Surg. 23(4): 203-211.
- Kim, W; Park, B.; Park, S. et al. (2009) Antiwrinkle effect of adipose-derived stem cell: Activation of dermal fibroblast by secretory factors. J. Dermatol. Sci. 53: 96-102.
- Everts. P. A.. Onishi. K., Jayaram. P., (2019). Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Internat J. of Molecular Sciences. 2(20): 7794.
- Newman, R.E.; Yoo, D.; LeRoux, M.A, et al. (2009) Treatment of inflammatory diseases with mesenchymal stem cells. lnflamm. Allergy Drug Targets. 8, 110-123.
- Zhou, T.; Yuan, Z; Weng, J. et al. (2021) Challenges and advances in clinical applications of mesenchymal stromal cells. J. Hematol. Oncol. 14:
- Gentile, P. (2020) Systematic Review: Adipose-derived mesenchymal stem cells, platelet-rich plasma and biomaterials as new regenerative strategies in chronic skin wounds and soft tissue defects. Internatl J. Molecular Sciences, 21(4): 1236.
- Rigotti. G.. Charles-de-Sri. L.. Gontijo-de-Amorim. N. et al. (2016). Expanded Stem Cells. Stromal-Vascular Fraction. And Platelet-Rich Plasma Enriched Fat: Comparing Results of Different Facial Rejuvenation Approaches in a Clinical Trial. Aesthetic Surg J., 36(3): 261-270
- Tate-Oliver, K, Alexander, RW. (2013) Combination of autologous adipose-derived tissue stromal vascular fraction plus high density platelet-rich plasma or bone marrow concentrates in Achilles Tendon Tears. J Prolo, 5:895-912.
- Fitzpatrick, J., Bulsara, M., Zheng, M. et al. (2017) The effectiveness of platelet-rich plasma in the treatment of tendinopathy: A meta-analysis of randomized controlled clinical trials. Am J. Sports Med. 45(1): 226-233 Doi: 10.1177/0363546516643716.
- Andia, I, Maffulli, N. (2013) Platelet-rich plasma for managing pain and inflammation in osteoarthritis. Nat Rev Rheumatol 9(12): 721-730 Doi: 10.1038/nrrheum.2013.141.
- Alderman, D. (2024) Micronized Fat/PRP Knee Health. Presented at “Catch The Wave Of Regenerative Therapies” at the 5th Annual Global Conference, SDARTS , August 2024, San Diego, CA.
- Suh, Y., Ahn, B., Kim. M., et al. (2019) Nanofat and platelet-rich plasma for the treatment of atrophic scars: A comparative study. J. Cosm Derm. l8(4): 1053-1059. Doi: l0.1111/jocd.12785.
- Everts, P, Podesta, L, Alexander, RW (2024) A comprehensive guide of cellular blood derived and mesenchymal stem cell-based autologous biological preparations for tissue repair, regeneration, and wound healing. Internatl J. Molecular Sci. . 2(20): 7794.
- Fadadu, P., Mazzola, A., Hunter, C., et al. (2019) Review of concentration yields in commercially available platelet-rich-plasma (PRP) systems: A call for PRP Standardization. Reg. Anesth. Pain Med. 44:652-659.
- Alexander, RW. (2011) Autologous fat grafts as mesenchymal stromal/stem cell source for use in prototherapy: A simple technique to acquire lipoaspirants. J. Prolo. 3(3):680-688.
- Alexander, RW (2024) Unpublished data
- Alexander, RW. (2020) Overview of COVID-19 Lung Damage Clinical Trial Using Cellular Stromal Vascular Fraction (cSVF) and Functional Respiratory Imaging (FRI) Analysis of Pulmonary Injury & Post-Viral (SARSCoV-2) Adult Respiratory Distress Syndrome (ARDS). Stem Cell Res. 1(1)-1-19.
- Alexander, RW. (2023) Preliminary Report on Residual Lung Damage in Long COVID-19 Using AD-cSVF In Clinical Trial NCT#04326036. J Stem Cell Res.4(2):1-26.
- Guo, J., Nguyen, A., Banyard, D., et al. (2019) Stromal vascular fraction: A regenerative reality: Part 2: Mechanism of action. J Plas Recon and Aesth Surg. 69(2): 180-188.
- Kokai, L., Marra, K., Rubin, J. (2020) Adipose stem cells: Biology and clinical applications for tissue repair and regeneration. J. Trans Res. 63(4): 399-408.
- Xu, H., Zhang, C., Zhang, S. et al. (2023) Stem cell enriched fat grafts versus autologous fat grafts in reconstructive surgery. 76(3): 570-580.
- Alexander, RW. (2023) Preliminary Report on Residual Lung Damage in Long Covid-19 Using AD-cSVF in Clinical Trial (NCT#04326036). J. Stem Cell Res. 4(2): 1-26.