





Natural Killer Lymphocytes & COVID-19: Impact on Stay
Relationship between Natural Killer Lymphocytes and Length of Stay in Patients with Depression admitted with Corona Virus-19
Tarik Wasfie, MD 1; Hadeel Barrawi, DO 1; Heather Kirkpatrick, PhD2; Samson Ndukwe, MD, MBA 3; Bilal Ali OMS, IV 3; Kimberly Barber, PhD 2; Jennifer Hella, MPH 2; Avery Jackson, MD 4
- Department of Surgery and Family Practice Henry Ford Genesys Hospital
- Department of Medical Education Henry Ford Genesys Hospital
- Central Michigan University College of Medicine
- Department of Neurosurgery – Michigan Neurosurgical Institute
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: Wasfie, T., Barrawi, H., et al., 2025. Relationship between Natural Killer Lymphocytes and Length of Stay in Patients with Depression admitted with Corona Virus-19. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6818
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6818
ISSN 2375-1924
ABSTRACT
Introduction: The recent unexpected COVID-19 pandemic had a serious and sudden impact on the world population physically and mentally. In the current study, we collected data prospectively on COVID-19 infected patients with depression/anxiety admitted to the hospital to evaluate the effect of these illnesses on patient length of stay and the level of Natural Killer Lymphocytes.
Methods: This project was a prospective study of patients admitted between July 2021 – July 2022 with COVID-19 to our community hospital. Patients completed the PHQ-9 and GAD-7 questionnaires to assess levels of depression and anxiety. A blood draw was done to check levels of natural killer lymphocyte cells (NKL). Data collected included age, sex, race, history of diabetes, hypertension, chronic obstructive pulmonary disease, hyperlipidemia, chronic kidney disease, obesity, length of stay, and mortality. Student’s t-Test, Chi-square, and Pearson’s correlation were used to identify the relationship of these patients to their NKL response and length of stay.
Results: There were a total of 67 patients enrolled. Of those 67 patients, 49 (73.1%) had labs drawn to measure NKL levels and were included in the analysis. Mean age was 61.8 (SD: 11.4). Over half of the participants were female (n=26, 53.1%). There were 30 (61.2%) patients with depression and 22 (44.9%) with anxiety. There were 26 (53.1%) patients with hypertension, 16 (32.7%) with diabetes, and 14 (28.6%) patients with chronic obstructive pulmonary disease. The mean Natural Killer lymphocyte was 82.3% (SD ±12.1) (which includes (CD3-CD16+CD56 dim and CD3-CD16+CD56 bright). The overall relationship between length of stay and combined NKL demonstrated a nonsignificant weak negative correlation (n=45, r= -0.07, p=.65). Patients with pre-existing chronic kidney disease had the highest NKL cell level (88.2) and the lowest LOS (5.4 days), and patients with Hypertension and hyperlipidemia had the lowest natural killer lymphocyte cell level (80.2 and 80.1 respectively) had the highest length of stay (8.6 and 10.1 days respectively).
Conclusion: Depression and anxiety did not influence length of stay of COVID-19 patients. NKL response and its relation to length of stay largely dependent on the associated comorbid conditions. Diabetes mellitus in patients with COVID-19 is a significant predictor of length of stay.
Keywords
Natural Killer Lymphocytes, Length of Stay, Depression, COVID-19, Anxiety
INTRODUCTION
The impact of mental illness on patient’s immune system has been studied in the past. A patient’s immune system can be compromised as a result of modulation in the endocrine system during stress, depression, or anxiety episodes. With the COVID-19 pandemic and the sudden impact it had on people’s social and economic life, a psychological burden with a negative effect on human mental health was unavoidable. Younger adults, essential workers (such as health workers, police, firefighters, etc.), racial and ethnic minorities, and volunteers reported disproportionately high levels of depression and anxiety, as well as other mental illnesses, with a resulting increase of substance and alcohol abuse as well as suicidal ideation.
Natural Killer Lymphocyte Cells (NKL) are white blood cells that are part of the innate immune system. Unlike other adaptive defense systems, they can recognize and kill virally infected cells immediately without having encountered them before. This unique ability is the result of a balance between NKL cells activating and inhibiting receptors, which respond to molecules on the surface of targeted cells. A new study shows certain NKL cells are activated when encountering a cell infected with SARS-COV-2. These cells contain a peptide from the virus that triggers a reaction in the NKL cells. Invariant forms of NKL cells are found in a low number in the airway system of patients with chronic obstructive pulmonary disease (COPD) or asthma. Based on these findings, therapeutic measures to modulate the immune system by targeting the NKL cell function have shown promising results.
In a meta-analysis and systematic review Vai et al. looked specifically at mental health illness in patients with COVID-19 and the risk of higher morbidity and mortality and found increased risk of hospitalization of patients with mental illness associated with COVID-19 and a subsequent increase in mortality. The immune response secondary to a SARS-CoV-2 infection has been extensively investigated during the pandemic, however, despite the advancements made toward understanding the relationships between the immunological response in COVID-19 infections and patient outcomes research has yet to identify how mental illnesses impacts the outcome of patients with such infections. Depression and anxiety have long been shown to influence the immune system response, reducing the ability of the body to fight the infection. Furthermore, any extended period of stress has been shown to be detrimental to physical and mental health. The presence of cortisol, the primary stress hormone, leads to various physiological responses at a molecular level including increases in blood glucose level for brain consumption and tissue repair, inhibition of pro-inflammatory cytokines such as IL-1 Beta, IL-6, and TNF-alpha, apoptosis of pro-inflammatory T cells, and a reduction of neutrophil chemotaxis, natural killer cell activities, and B cell antibody production.
Our knowledge of the impact of COVID-19 on mental health remains limited, however, some studies have identified factors such as gender, age and socio-economic status as being associated with poor physical and psychological health of those patients. We hypothesized that COVID-19 infection in patients with depression and or anxiety will have a decreased immune response to the disease, and therefore an increase in the length of stay (hospital and intensive care unit). Their management of COVID-19 would also be more challenging as we are combining the care and management of physical disease in a mentally ill patient. We additionally investigated the relationship between the NKL response and the length of stay in those patients.
METHODS
We examined 67 consented consecutive patients admitted with a positive COVID-19 infection from July 2021 through July 2022 to our 400-bed community hospital. Patients on ventilatory support were excluded from the study as they were unable to consent and communicate to complete the questionnaires. Patients’ data collected included age, sex, race, comorbid conditions (such as diabetes mellitus, hypertension, chronic kidney disease, chronic obstructive pulmonary disease, obesity, hyperlipidemia, history of depression, and history of anxiety), length of stay (LOS) in the hospital and the intensive care unit (ICU), and mortality. Screening questionnaires for depression and anxiety were given to patients (PHQ-9 and GAD-7) during their hospital admission. These measures are reliable, valid, and frequently used in medical settings to assess depression and anxiety. In addition, they provide the severity levels of depression and anxiety. Patients were approached regarding participating in the study on the first day of their admission. They could choose to consent at that time or be given some time to consider participating. The patient was provided with a copy of the consent form at that time. Once the patient decided to participate and was consented, they were provided the PHQ-9 and GAD-7 questionnaires for completion. Those patients with depression and or anxiety were divided into three groups according to the degree of severity (no or minimal, moderate, and severe). After the completion of the questionnaires and the consent, additional data was collected from the patient’s electronic medical record. Blood samples were collected for NKL cyto screening assay, which included the following lymphocytes subset panels; PCT CD3-CD16 + CD56 dim (Cytotoxic NK-Cells), and PCT CD3-CD16 -CD56 bright (cytokine-secreting NK cells). NKL cells are identified by absence of CD3 and the expression of CD16 and/or CD56. NKL cells are divided according to the expression of CD16 and CD56 into Cytotoxic NK cells (CD4-CD16+CD56dim) that represents approximately 90 percent of NKL cells, and cytokine-secreting or regulatory NKL cells (CD3-CD16-CD56bright) that represents approximately 10 percent of NKL cells. NKL cells act against virally infected cells and tumor cells and may be increased or decreased in various immunologic abnormalities. NKL cells also have a role in the adaptive immune responses through cytokine production. NK-like T cells have properties of both T cells and NKL cells, expressing both CD3 and NKL associated antigens. The cytotoxic NKL cells (CD3-CD16+CD56dim) and cytokine-secreting or regulatory NK cells (CD3-CD16-CD56bright) are reported as a percentage of the total NKL cells. All other populations are reported as a percentage of the total lymphocytes. This test was developed, and its performance characteristics were determined by Associated Regional and University Pathologist (ARUP) Laboratories. It has not been cleared or approved by the US Food and Drug Administration. This test was performed in a Clinical Laboratory Improvement Amendment (CLIA) certified laboratory and is intended for clinical purposes (Schultz-Florey 2021).
Descriptive statistics were analyzed for all variables with continuous variables reported as means (SD) and categorical variables reported as frequencies (percentages). Student’s t-Test (continuous variables), Chi-square analysis (dichotomous variables), Pearsons’s correlation (between LOS and T cell response), one-way ANOVA to look for a difference between the depression and anxiety groups and LOS, and a multiple linear regression analysis was completed to see if there is a relationship between LOS and various comorbid conditions. Institutional review board approval was obtained prior to the implementation of the study.
RESULTS
There were a total of 67 patients enrolled in the study. There were 49 (73.1%) patients who had blood draws and were included in the analysis. There were 23 (46.9%) males and 26 (53.1%) females. The mean age was 61.8 ± 11.4 years (range 30 – 82 years) and the total length of stay was 8.3 ± 4.5 days. There were four mortalities, all of them had some degree of depression and two of them had some degree of anxiety. See Table 1 for full demographic data, mean PHQ-9 scores, GAD-7 scores, and NKL levels. The mean NKL and LOS by comorbid condition are listed in figure 1.
| N=49 | |
|---|---|
| Age (Years, SD) | 61.8 (11.4) |
| Gender | |
| Male (n,% ) | 23 (46.9) |
| Female (n,% ) | 26 (53.1) |
| Comorbid Conditions* (n,% ) | |
| Diabetes Mellitus | 16 (32.7) |
| Hypertension | 26 (53.1) |
| Chronic obstructive pulmonary disease | 14 (28.6) |
| Hyperlipidemia | 11 (22.4) |
| Chronic Kidney Disease | 10 (14.9) |
| Depression (as a comorbid condition) | 4 (8.2) |
| Anxiety (as a comorbid condition) | 4 (8.2) |
| Length of Stay (mean, SD) | 8.3 (4.5) |
| Natural killer lymphocyte (mean, SD) | 82.3 (12.1) |
| Mean PHQ-9 Score (SD) | 7.7 (6.3) |
| Mean GAD-7 Score (SD) | 3.9 (4.3) |
The mean age among those with depression was 61.8 (SD ± 10.5) years old. The gender breakdown was 16 (53.3%) females and 14 (46.7%) males. When looking at comorbid conditions, there were 15 (50%) patients with hypertension, 10 (33.3%) with diabetes mellitus, 8 (26.7%) with COPD, and 4 (13.3%) with acute renal disease. The largest number of patients scored as having no or minimal depression (n=19, 38.8%). The mean LOS was 7.4 (SD ± 4.0) days in the no or minimal depression group, which was the lowest of the depression category groups. The mild depression group had a mean LOS of 9.3 (SD ± 3.7) and the moderate/severe group had a mean LOS of 8.7 (SD ± 6.1), with no statistical differences (p=0.47) (Table 2).
| N (%) * | LOS N (SD) | p-value |
|---|---|---|
| Depression Categories | ||
| No/Minimal Depression | 19 (38.8) | 7.4 (4.0) |
| Mild Depression | 14 (28.6) | 9.3 (3.7) |
| Moderate/Severe Depression | 12 (24.5) | 8.7 (6.1) |
| Missing | – | – |
| Mean PHQ-9 Score (n, SD) | – | – |
| Anxiety Categories | ||
| No/Minimal Anxiety | 25 (51.0) | 7.8 (4.6) |
| Mild Anxiety | 16 (32.7) | 8.6 (3.9) |
| Moderate/Severe Anxiety | 4 (8.2) | 10.5 (6.6) |
| Missing | – | – |
| Mean GAD-7 Score (n, SD) | – | – |
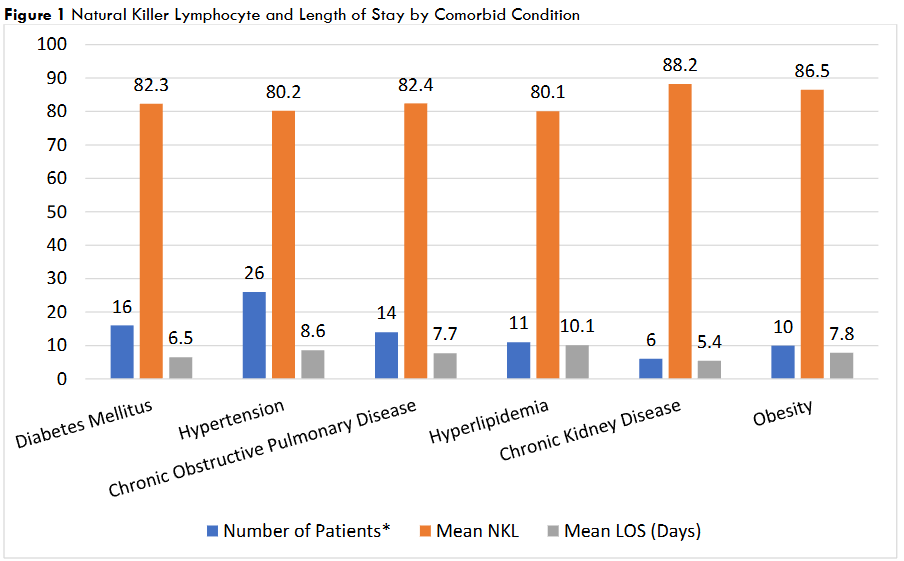
Figure 1 Natural Killer Lymphocyte and Length of Stay by Comorbid Condition
The mean age among those with anxiety was 61.6 (SD ± 9.4) years old, there were 10 females (45.5%) and 12 (54.5%) males. When looking at comorbid conditions, there were 11 (50%) patients with hypertension, 7 (31.8%) with diabetes mellitus, 7 (31.8%) with COPD, and 3 (13.6%) with acute renal disease. The mean LOS was 9.0 (SD ± 4.4) and the mean NKL was 82.4 (SD ± 13.1). The majority of patients scored as having no or minimal anxiety (n=27, 55.1%). The mild anxiety group had 18 (36.7%) patients, and the moderate/severe group had 4 (8.2%) patients. Those in the no or minimal anxiety group had a mean LOS of 7.8 (SD ± 4.6) days, which was the lowest among the groups (mild: 8.6, SD ± 3.9; moderate or severe: 0.5 (SD ± 6.6). There are no statistical differences in LOS between the anxiety groups (p=0.51) (Table 2).
Using a Pearson Correlation test, the overall relationship between LOS and the combined NKL cell count demonstrated a non-significant negative weak correlation (n= 45, r= -0.07, p= 0.65). Among patients reporting no depression, the relationship was a positive correlation (i.e. higher NKL with a higher LOS) that was not significant (n= 19, r= 0.13, p= 0.60). Patients with pre-existing CKD had the highest NKL and lowest LOS, while Hypertension and Hyperlipidemia had the lowest NKL level and highest LOS. The level of NKL and LOS, in relation to patients with other comorbid conditions, are in Table 2. A multiple linear regression analysis was conducted to look at the relationship between LOS and the following predictor variables: age, NKL cell combined, COPD, HTN, DM, and CKD. It was found that diabetes significantly predicted LOS (p=0.03). Age (p=0.08), NKL (p=0.75), COPD (p=0.51), HTN (p=0.78), and CKD (0.07) were not significant predictors of LOS.
DISCUSSION
Those with psychological stressors have been reported to have a higher risk of respiratory viral infections, therefore patients with anxiety or depressive illness are vulnerable to viral infections, such as COVID-19. However, subsequent reports on stressors didn’t associate psychological stress with immune changes. Furthermore, in some cases physical vulnerability as a function of age or other associated disease, i.e. comorbid disease, increases the immune change during stressors such as respiratory illnesses. Which might explain the higher rate of mortality and morbidity in the elderly male patients as they have a high rate of comorbid conditions. Cytotoxic Killer T-cell are very cytotoxic as reflected by a higher production of cytokines such as gamma interferon and tumor necrosis factor. Furthermore, Cytotoxic Killer T-cells are the key players in control of viral infections as they performed targeted cell killing in SARS-CoV-2 infection. The expression of differentiation in the subpopulation of the T-lymphocytes is an important hallmark of the existence of these cells with cytotoxic potential, which is necessary for viral infection control. In the elderly, the response is low which might be the reason that those patients will frequently develop severe COVID-19 infections.
The relationship between the NKL response and LOS in each of the associated comorbid conditions demonstrates an inverse relationship in patients with hypertension and hyperlipidemia. These patients exhibited a low NKL response and a higher LOS (8.6 and 10 days, respectively). On the other hand, patients with chronic kidney disease and obese patients had a higher level of response to NKL and a length of stay (5.4 and 7.8 days, respectively). The reviewed literature showed that the outcome (morbidity and mortality) of diabetic patients infected with COVID-19 depends largely on the blood glucose level control and they recommend having better control for reduction in mortality and morbidity. In the regression analysis of our COVID-19 patients, diabetes mellitus was the only significant predictor of LOS. Furthermore, the limited NKL response of our diabetic patients to COVID-19 infection had a minimal influence on LOS (6.5 days). Whether this might be related to uncontrolled high blood sugar levels or not needs to be investigated further.
In our sample of patients with COPD admitted with COVID-19, the benefit of high NKL in reducing the LOS is severely diminished. This may indicate that COPD patients had their NKL reach an exhausted state where they are no longer stimulating the immune system enough to improve survival. We know now that NKL cells are already present in the bronchial tree of patients with COPD long before their exposure to COVID-19. Patients with COPD are at a higher risk of associated comorbid conditions such as depression or anxiety disorders, which in turn increase their symptom burden and subsequent re-hospitalization as compared to the general population. While COPD is a high risk for any suspected illness, including rhinoviral infection, the addition of depression to the picture will undoubtedly delay and prolong the recovery of these patients. Finally, our understanding of the facts that contribute to the impact of COVID-19 on mental health remain limited and identifying risk factors such as gender, age, social determinants of health, use of media and poor physiological and physical health are yet to be defined.
LIMITATIONS
The small sample size in our study limits the generalizability of our findings. We excluded the sickest patients, i.e., those on a ventilator. The sample size was not large enough for our ‘positive’ correlation to reach significance. A larger sample size could have shown this correlation to be significant. These patients could have fallen into the depression category and may have increased the LOS. This study should be replicated in the future with a larger (greater than 100) sample size.
CONCLUSION
Depression and anxiety in patients admitted with COVID-19 did not influence the patient’s LOS. However, diabetes mellitus in patients with COVID-19 was a significant predictor of LOS. Natural Killer Lymphocyte Cells exhibited a varying degree of responses in relation to the LOS and was largely dependent on the associated comorbid conditions of the patient at the time of his infection with COVID-19.
ACKNOWLEDGEMENTS
The authors acknowledge the assistance of Dr. Andrew Heneke from the Pathology Department and Debbie Cicchini for their continuous effort and dedication to obtain the supportive materials for this study.
REFERENCES
- Calabrese JR, Kling MA, Gold PW. Alterations in immunocompetence during stress, bereavement, and depression: focus on neuroendocrine regulation. Am J Psychiatry. 1987;144(9):1123-1134. doi:10.1176/ajp.144.9.1123.
- Burvill PW. Physical illness in the elderly. A study of patients in mental hospitals, geriatric hospitals and nursing homes. Gerontol Clin (Basel). 1970;12(5):288-296. doi:10.1159/000245291
- Yu L, McCracken LM. COVID-19 and the mental health in the UK: Depression, anxiety and insomnia and their associations with persistent physical symptoms and risk and vulnerability factors. Br J Clin Psychol. 2024;63(1):92-104. doi:10.1111/bjc.12446.
- Bu F, Steptoe A, Fancourt D. Depressive and anxiety symptoms in adults during the COVID-19 pandemic in England: A panel data analysis over 2 years. PloS Med. 2023;20(4):e1004144. doi:10.1371/journal.pmed.1004144.
- Zhu C, Zhang T, Li Q, Chen X, Wang K. Depression and anxiety during the COVID-19 pandemic: Epidemiology, mechanism, and treatment. Neurosci Bull. 2023;39(4):675-684. doi:10.1007/s12264-022-00970-2.
- Czeisler MÉ, Tynan MA, Howard ME, et al. Public attitudes, behaviors, and beliefs related to COVID-19, stay-at-home orders, nonessential business closures, and public health guidance – United States, New York city, and Los Angeles, May 5-12, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(24):751-758. doi:10.15585/mmwr.mm6924e1.
- Titus AR, Mezuk B, Hirschtick JL, McKane P, Elliot MR, Fleischer NL. Patterns and predictors of depressive and anxiety symptoms within a population-based sample of adults diagnosed with COVID-19 in Michigan. Soc Psychiatry Psychiatr Epidemiol. 2023;58(7):1099-1108. doi:10.1007/s00127-023-02453-9.
- Westmeier J, Paniskaki K, Karaköse Z, et al. Impaired cytotoxic CD8+ T cell response in elderly COVID-19 patients. mBio. 2020;11(5):e02243-20. doi:10.1128/mBio.02243-20.
- Cook KD, Waggoner SN, Whitmire JK. NK cells and their ability to modulate T cells during virus infections. Crit Rev Immunol. 2014;34(5):359-88. doi:10.1615/critrevimmunol.2014010604.
- Vijayanand P, Seumois G, Pickard C, et al. Invariant natural killer T cells in asthma and chronic obstructive pulmonary disease. N Engl J Med. 2007;356(14):1410-22. doi:10.1056/NEJMoa064691.
- Rijavec M, Volarevic S, Osolnik K, Kosnik M, Korosec P. Natural killer T cells in pulmonary disorders. Respir Med. 2011;105 Suppl 1:S20-S25. doi:10.1016/S0954-6111(11)70006-3.
- Vai B, Mazza MG, Colli CD, et al. Mental disorders and risk of COVID-19-related mortality, hospitalization, and intensive care unit admissions: a systematic review and meta-analysis. Lancet Psychiatry. 2021;8(9):797-812. doi:10.1016/S2215-0366(21)00232-7.
- Song H, Fall K, Fang F, et al. Stress related disorders and subsequent risk of life threatening infections: population based sibling controlled cohort study. BMJ. 2019;367:I5784. doi:10.1136/bmj.l5784.
- Segerstrom SC, Miller GE. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull. 2004;130(4):601-30. doi:10.1037/0033-2909.130.4.601.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self- report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient health questionnaire. JAMA. 1999;282(18):1737-44. doi:10.1001/jama.282.18.1737.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-13. doi:10.1046/j.1525-1497.2001.016009606.x.
- Löwe B, Decker O, Müller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46(3):266-274. doi:10.1097/MLR.0b013e318160d093.
- Schultze-Florey CR, Chukhno E, Goudeva L, et al. Distribution of major lymphocyte subsets and memory T-cell subpopulations in healthy adults employing GLP-conforming multicolor flow cytometry. Leukemia. 2021;35(10):3021-3025. doi:10.1038/s41375-021-01348-5.
- Hoffman RS, Koran LM. Detecting physical illness in patients with mental disorders. Psychosomatics. 1984;26(9):654-60. doi:10.1016/S0033-3182(84)72974-4.
- Galić K, Dodaj A, Ćorluka-Čerkez V, et al. Study of depression and anxiety in patients with asthma and chronic obstructive pulmonary disease. Psychiatr Danub. 2019;31(Suppl 1):112-117.
- Glaser R, Kiecolt-Glaser JK. Stress-induced immune dysfunction: implications for health. Nat Rev Immunol. 2005;5(3):243-51. doi:10.1038/nri1571.
- Momen NC, Plana-Ripoll O, Agerbo E, et al. Association between mental disorders and subsequent medical conditions. N Eng J Med. 2020;382(18):1721-1731. doi:10.1056/NEJMoa1915784.
- Matheson FI, Smith KLW, Moineddin R, Dunn JR, Glazier RH. Mental health status and gender as risk factors for onset of physical illness over 10 years. J Epidemiol Community Health. 2014;68(1):64-70. doi:10.1136/jech-2013-202838.
- Fousteri G, Kuka M. The elusive identity of CXCR5+ CD8 T cells in viral infection and autoimmunity: Cytotoxic, regulatory, or helper cells? Mol Immunol. 2020;119:101-105. doi:10.1016/j.molimm.2020.01.007.
- Voskoboinik I, Whisstock JC, Trapani JA. Perforin and granzymes: function, dysfunction and human pathology. Nat Rev Immunol. 2015;15(6):388-400. doi:10.1038/nri3839.
- Katipoglu B, Naharci MI, Yurdakul ES. Risk factors predicting hospital length of stay in older patients with type 2 diabetes with Covid-19. J Diabetes Metab Disord. 2022;21(2):1443-1449. doi:10.1007/s40200-022-01078-0.
- Ciric VM, Rancic NK, Pesic MM, Radojkovic DB, Milenkovic N. Factors associated with length of hospitalization in patients with diabetes and mild COVID-19: Experiences from a tertiary university center in Serbia. Medicina (Kaunas). 2024;60(5):788. doi:10.3390/medicina60050788.
- Soff S, Yoo YJ, Bramante C, et al. Association of glycemic control with long COVID in patients with type 2 diabetes: findings from the National COVID Cohort Collaborative (N3C). BMJ Open Diabetes Res Care. 2025;13(1):e004536. doi:10.1136/bmjdrc-2024-004536.
- Zhang J, Ma Y, To WL, et al. Impact of COVID-19 infection on mortality, diabetic complications and haematological parameters in patients with diabetes mellitus: a systematic review and meta-analysis. BMJ Open. 2025;15(3):e090986. doi:10.1136/bmjopen-2024-090986.
- Mannheim J, Johnson D. COVID-19 and diabetes: an epidemiologic overview. Pediatr Ann. 2024;53(7):E258-E263. doi:10.3928/19382359-20240502-07.
- He Y, Zheng Q, Zhifang Z, et al. When COVID-19 meets diabetes: a bibliometric analysis. Diabetes Res Clin Pract. 2025;223:112118. doi:10.1016/j.diabres.2025.112118.
- Fairclough L, Urbanowicz RA, Corne J, Lamb JR. Killer cells in chronic obstructive pulmonary disease. Clin Sci (Lond). 2008;114(8):533-41. doi:10.1042/CS20070356.
- Rahi MS, Thilagar B, Balaji S, et al. The impact of anxiety and depression in chronic obstructive pulmonary disease. Adv Respir Med. 2023;91(2):123-134. doi:10.3390/arm91020011.