






Neonatal Outcomes in Maternal Heart Disease: A Study
Neonatal Outcomes in Maternal Heart Disease: A Multidisciplinary Approach toward Congenital and Acquired Conditions
Yaiza Fernandez Munoz 1, Aura S. Eguizabal, BS 2, Alexander Goldman, BA 7, Jiaqi Zhang, MS 3, Ijeoma Iwekaogwu, BS 3, Elisa Padron, BSA2, Elizabeth B. Sherwin, MPH3, Graciela Carabello, MD 3,5, Karl-Stephane Louis-Jacques, BA 6, Gabriela Briceño Silva, MD 8, Sabrina Montgomery, BA 9, Meryl Sperling, MD 4, Abha Khandelwal, MD5, Katherine Bianco, MD 4
- University of California, Berkeley
- Stanford School of Medicine, Stanford University
- Department of Obstetrics and Gynecology, Stanford University
- Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, Stanford University
- Department of Medicine, Division of Cardiovascular Medicine, Stanford University
- Meharry Medical College
- Northwestern University
- Universidad de Oriente, Venezuela
- Charles R. Drew University of Medicine and Science, College of Medicine
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Author1, X., Author2, Z., et al., 2025. Neonatal Outcomes in Maternal Heart Disease: A Multidisciplinary Approach toward Congenital and Acquired Conditions. Medical Research Archives, [online] 13(9).
https://doi.org/10.18103/mra.v13i9.6904
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i9.6904
ISSN 2375-1924
Abstract
Background: Neonatal outcomes are directly affected by maternal heart disease, which remains one of the leading causes of preventable pregnancy-related deaths in the United States. Limited data compares maternal and neonatal outcomes among this high-risk population. We describe neonatal outcomes among pregnancies with and without heart disease in a tertiary care center with coordinated multidisciplinary care.
Methods: This was a cohort study of pregnancies affected by maternal cardiac diseases that received multidisciplinary care (maternal-fetal medicine, obstetrics, cardiology, anesthesiology, genetics) in a single tertiary center between 2012 and 2024. Study groups consisted of pregnancies with maternal acquired heart disease (AHD) (n = 242), maternal congenital heart disease (CHD) (n = 224), and a comparison group of pregnancies without maternal heart disease from November 2020 through April 2021 (n = 183). Neonatal outcomes including birth weight, gestational age, Apgar scores, and NICU admissions, were compared by Pearson Chi-Square, Fisher Exact, and Kruskal-Wallis rank sum tests. A pairwise comparison was conducted for significant differences. A sensitivity analysis was performed by logistic and linear regression to adjust for beta-blocker use during pregnancy. Significance was set at alpha = 0.05.
Results: Maternal heart disease, particularly CHD, was associated with increased adverse neonatal outcomes compared to the comparison cohort. Infants born to people with CHD or AHD had lower birth weights, shorter gestational ages, lower Apgar scores, and higher NICU admission rates compared to those without heart disease (Table 1) (p < 0.01 for all comparisons). The proportion of small for gestational age infants born to people with CHD was significantly higher than those born to people with AHD (p = 0.007). After adjusting for beta-blocker exposure during pregnancy, the odds for small for gestational age in neonates of patients with CHD were 2.29 times higher than in those with AHD (p = 0.006). All other outcomes were similar in the CHD and AHD cohorts.
Conclusion: Maternal heart disease is associated with increased risk of adverse neonatal outcomes, necessitating a multidisciplinary approach in prenatal care. Infants born to individuals with CHD had a higher risk for small for gestational age compared to those with AHD. Further studies are needed to better understand this biological difference.
Keywords
Maternal heart disease, Congenital heart disease (CHD), Acquired heart disease (AHD), Neonatal outcomes, Small for gestational age, Perinatal outcomes, High-risk pregnancy, Maternal-fetal medicine
Introduction
Maternal heart disease remains one of the leading causes of preventable pregnancy-related deaths in the US, with a mortality rate which has more than doubled since the year 2000. A 2019 CDC report on maternal mortality determined that cardiovascular conditions (including cardiomyopathy, myocardial infarction, and cerebrovascular accidents) were the cause of more than 33% of pregnancy-related deaths. According to a data report by the California Pregnancy-Associated Mortality Review (CA-PAMR) published by the California Maternal Quality Care Collaborative (CMQCC), cardiovascular disease (CVD) continued to be the leading cause of pregnancy-related deaths in 2017-2019. Cardiac disease was the third leading cause of indirect maternal deaths in the 2020-2022 period in the UK, and the 2nd cause in France between 2016 and 2018. While the 21st century’s overall increasing maternal mortality rate can be partially attributed to the rising average maternal age, it is notable that an increasing number of patients with CHD are surviving to childbearing age, therefore acutely contributing to this rising statistic. Fortunately, within this same timeframe, notable technological advancements and procedural refinements have also developed.
In recent years, multidisciplinary care models have emerged as the best care to manage high-risk pregnancies in patients with maternal heart disease. Our group and others have shown that this collaborative approach has improved the management of cardiac complications, enabling more women with pre-existing heart conditions to reduce adverse prenatal outcomes. Nevertheless, further research is needed to understand the specific complications and impact of maternal CHD and AHD on both parents and their offspring. Studies have found that refined practices and multidisciplinary care have demonstrated improvement of maternal heart disease in pregnancy and neonatal outcomes.
Maternal heart disease is linked to an increased risk of adverse neonatal outcomes, though the specific complications and distinct outcomes remain less well understood. Several maternal heart conditions have been associated with a significant reduction in fetal growth rate, preterm delivery, and reduced birth weight. Evidence suggests that these outcomes are primarily driven by the disease process itself, particularly reduced uteroplacental perfusion and chronic hypoxia in cyanotic or hemodynamically significant lesions, rather than by medications used to treat the condition. However, certain treatments, such as beta-blockers, also contribute to adverse neonatal outcomes, most notably by increasing the risk of fetal growth restriction and small-for-gestational-age. Improved understanding is needed to guide prenatal counseling, delivery planning, and care in this high-risk population.
Due to the nature of these high-risk pregnancies, we studied pregnancies affected by maternal cardiac diseases that received multidisciplinary care in a single tertiary center between 2012 and 2024. There were two main objectives for this study. The first objective was to examine the overall impact of maternal heart disease on neonatal outcomes. For the second objective, we focused on comparing neonatal outcomes among those with maternal congenital heart disease (CHD) compared to acquired heart disease (AHD).
Methods
We conducted a retrospective cohort study at a single tertiary care academic medical center, examining pregnancies affected by maternal cardiac disease between January 1, 2012, and March 31, 2024. Eligible cases were identified through institutional databases and electronic medical records, focusing on individuals who received coordinated multidisciplinary care throughout pregnancy at a single tertiary care center. The multidisciplinary care team included specialists in maternal-fetal medicine (MFM), cardiology, obstetrics, anesthesiology, and genetics.
The study population included three groups: (1) pregnancies in individuals with acquired heart disease (AHD, n = 242), (2) pregnancies in individuals with congenital heart disease (CHD, n = 224), and (3) a comparison group of pregnancies in individuals without known cardiac disease (n = 183). We defined maternal AHD as any cardiac condition diagnosed previous to or during pregnancy, including but not limited to cardiomyopathy, valvular disease, arrhythmias, ischemic heart disease, and hypertensive heart disease. Maternal CHD was defined as structural cardiac abnormalities present in the pregnant individual from birth, with or without prior surgical correction. Data for the comparison group was obtained from a prior study which was from the same institution and was collected between Nov 2020 and April 2021. It included individuals without preexisting cardiac conditions who met the same inclusion criteria as the study groups, including routine obstetric care at the same site and were not diagnosed with gestational diabetes or other high-risk conditions during the study period.
Primary neonatal outcomes assessed included preterm birth (<37 weeks gestation), low birth weight (<2500 grams), small for gestational age (birth weight <10th percentile for gestational age), NICU admission, Apgar scores at 1 and 5 minutes, neonatal mechanical ventilation (anytime during hospitalization), and perinatal mortality (death before neonate discharge). Categorical variables were compared across groups using Pearson’s Chi-Square or Fisher’s Exact tests, as appropriate. Continuous variables were compared using the Kruskal-Wallis rank sum test due to non-normal distributions. Pairwise comparisons were conducted when overall group differences were statistically significant. Bonferroni correction was applied to control family-wise error rate for all pairwise comparisons (adjusted alpha level = 0.0167). Additionally, a sensitivity analysis was conducted for patients with CHD and AHD to further investigate neonatal outcomes that had significant overall differences. The multivariable logistic and linear regression were employed to adjust for beta-blocker exposure during pregnancy. All tests were two-sided, and the alpha level was 0.05. Statistical analyses were performed using R 4.4.1.
Results
Table 1 describes the study population. A total of 649 pregnancies were included in the analysis: 224 in the maternal CHD group, 242 in the maternal AHD group, and 183 in the comparison group with no documented heart disease. All patients in the CHD and AHD groups received multidisciplinary care at a single tertiary care center. Compared to those with heart disease, the comparison group had a higher proportion non-Hispanic individuals, individuals with private insurance, and vaginal deliveries. Age and parity were similar between groups.
| Characteristics | Acquired Heart Disease (n = 242) | Congenital Heart Disease (n = 224) | No Heart Disease (n = 183) |
|---|---|---|---|
| Maternal Age (Years) | 33 [30, 36] | 32 [28, 36] | 33 [30, 35] |
| Maternal Age Group | < 35 Years 144 (60%) | 152 (67.9%) | 128 (69.9%) |
| >= 35 Years 98 (40%) | 72 (32.1%) | 55 (30.1%) | |
| Maternal Race | Asian 47 (19.4%) | 56 (25.0%) | 67 (36.6%) |
| Black 5 (2.1%) | 5 (2.3%) | 4 (2.2%) | |
| Caucasian 117 (48.3%) | 98 (43.8%) | 98 (53.6%) | |
| Pacific Islander 5 (2.1%) | 1 (0.5%) | 2 (1.1%) | |
| Other 73 (30.2%) | 65 (29.0%) | 14 (7.7%) | |
| Maternal Ethnicity | Non-Hispanic 175 (72.3 %) | 156 (69.6%) | 162 (88.5%) |
| Hispanic 67 (27.7%) | 68 (30.4%) | 21 (11.5%) | |
| Insurance | Private 163 (67.4%) | 146 (65.2%) | 171 (93.4%) |
| Public 74 (30.6%) | 76 (33.9%) | 12 (6.6%) | |
| Other 5 (2.1%) | 2 (0.9%) | 0 (0.0%) | |
| Nulliparous | 120 (49.6%) | 118 (52.7%) | 111 (60.7%) |
| Delivery Mode | Vaginal 129 (53.3%) | 127 (56.7%) | 126 (68.9%) |
| Cesarean 113 (46.7%) | 97 (43.3%) | 57 (31.1%) | |
| Beta Blocker Use During Pregnancy | 75 (31%) | 29 (13%) | Unavailable |
Objective 1- Compare neonatal outcomes among those with and without maternal heart disease
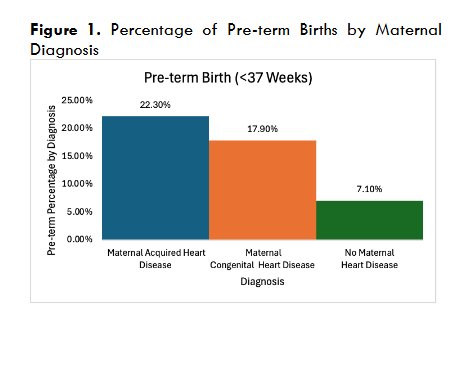
Infants born to individuals with maternal heart disease (acquired heart disease or congenital heart disease) had lower birth weights compared to those in the comparison group (median: 3,082g vs 3,073g vs 3,319g, p < 0.01). The proportion with preterm birth (<37 weeks’ gestation) was higher in both acquired heart disease and congenital heart disease groups compared to those without heart disease (proportion: 22% vs 18% vs 7%, p < 0.01; Figure 1).
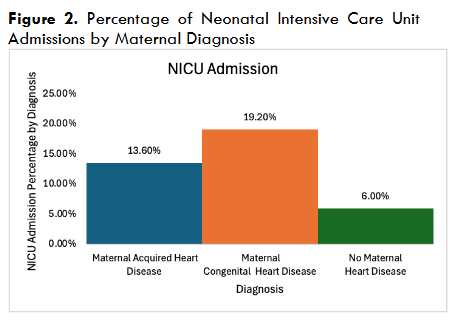
Neonates in the acquired heart disease and congenital heart disease groups were more likely to be admitted to the NICU compared to the comparison group (14% vs 19% vs 6%, p < 0.01; Figure 2).
Additionally, the length of initial hospital stay was longer among infants born to individuals in the maternal heart disease groups (median: 3 vs 3 vs 2, p < 0.01) (Table 2).
| Key Metrics | Maternal Acquired Heart Disease (n = 242) | Maternal Congenital Heart Disease (n = 224) | No Maternal Heart Disease (n = 183) | P-Value |
|---|---|---|---|---|
| Pre-term Birth (<37 Weeks) | 54 (22.3%) | 40 (17.9%) | 13 (7.1%) | < 0.001 |
| Gestational Age (Weeks) | 38.3 [37.0, 39.3] | 38.8 [37.3, 39.4] | 39.0 [38.0, 40.0] | < 0.001 |
| Birthweight (Grams) | 3,082 [2,693, 3,466] | 3,073 [2,702, 3,350] | 3,319 [2,995, 3,578] | < 0.001 |
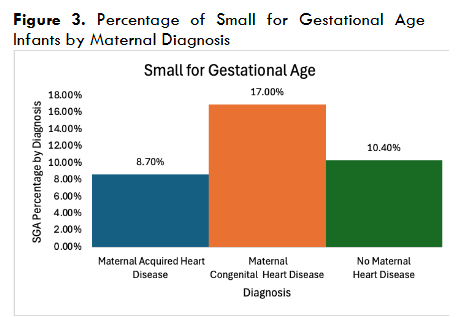
| Small for Gestational Age | 21 (8.7%) | 38 (17.0%) | 19 (10.4%) | 0.02 |
| Apgar score at 5 minutes <7 | 4 (1.7%) | 7 (3.1%) | 1 (0.5%) | 0.2 |
| NICU Admission | 33 (13.6%) | 43 (19.2%) | 11 (6.0%) | < 0.001 |
| Mechanical Ventilation During Hospitalization | 15 (6.2%) | 19 (8.5%) | 3 (1.6%) | 0.011 |
| Length of Initial Hospitalization (Days) | 3 [2,4] | 3 [2,4] | 2 [2,3] | < 0.001 |
| Death before Discharge | 0 (0) | 4 (1.8%) | 1 (0.5%) | 0.056 |
Objective 2 – Acquired Heart Disease vs. Congenital Heart Disease Impact on Neonatal Outcomes
Infants born to individuals with congenital heart disease were more likely to be small for gestational age compared to those with acquired heart disease and comparison group (CHD vs AHD: 17.0% vs 8.7%, p = 0.007; CHD vs comparison, p = 0.057).
Furthermore, no significant differences were observed between groups in Apgar scores at 1 and 5 minutes. Similarly, rates of cesarean delivery and the need for mechanical ventilation were comparable across CHD and AHD groups (p = 0.46, 0.34 correspondingly). However, pairwise statistical testing confirmed that the CHD and AHD groups both had worse neonatal outcomes across several domains (birth weight, pre-term birth, NICU admission, length of hospital stay) compared to the comparison group (p < 0.01 for all comparisons).
Sensitivity Analysis – Adjusting for Beta Blocker Exposure
After adjusting for the use of beta blocker during the pregnancy, the odds of small for gestation age in neonates born to patients with congenital heart disease is 2.29 times (95% confidence interval (CI): 1.29, 4.18) higher than in those with acquired heart disease, and this result is statistically significant (p = 0.006). There were no statistically significant differences between congenital and acquired heart disease groups in other neonatal outcomes after adjustment.
| Neonatal Outcome | Odds Ratio / Coefficient [95% Confidence Interval] | P value |
|---|---|---|
| Pre-term Birth (<37 weeks) | 0.79 [0.49, 1.26] | 0.33 |
| Birthweight (Grams) | -69 [-194, 57] | 0.28 |
| Small for Gestational Age | 2.29 [1.29, 4.18] | 0.006 |
| NICU Admission | 1.60 [0.96, 2.68] | 0.07 |
| Mechanical Ventilation During Hospitalization | 1.30 [0.64, 2.70] | 0.47 |
| Length of Initial Hospitalization (Days) | -0.12 [-2.7, 2.5] | 0.93 |
Discussion
Our primary objective found that maternal heart disease, including congenital and acquired maternal heart disease, is associated with adverse neonatal outcomes compared to pregnancies not affected by maternal heart disease. This retrospective study has a large sample size of total pregnancies (n=649) over twelve years at a single tertiary center. However, as investigators on the topic of maternal CHD and AHD, there are other studies to compare against. Our findings are novel in that we investigate neonatal outcomes as opposed to just maternal outcomes within CHD and AHD. Our findings on neonatal outcomes are in line with the current literature, which emphasizes maternal heart disease as a leading contributor to an increased maternal mortality rate associated with more adverse neonatal outcomes.
Several prior studies have reported similar associations between maternal CHD and adverse neonatal outcomes. For example, a study of maternal heart disease (CHD & AHD) and perinatal outcomes reported that maternal heart disease was associated with increased odds of preterm birth, IUGR, the need for assisted vaginal delivery, maternal ICU admission, and maternal hospitalization. Similarly, a 2024 study found that neonates born to individuals with maternal heart disease had significantly higher rates of preterm birth, NICU admission, and longer NICU stays, highlighting the need for tailored perinatal management. These findings are likely explained by underlying placental abnormalities associated with maternal heart disease. In pregnancies complicated by CHD, studies have shown impaired placental development and perfusion. For instance, one study found that CHD pregnancies are associated with reduced placental weight, villous maldevelopment, and maternal vascular malperfusion, which contribute to impaired oxygen and nutrient exchange, leading to fetal growth restriction. Similarly, echocardiographic studies demonstrate reduced umbilical venous blood flow relative to fetal weight in CHD, indicating compromised placental function. Beyond these findings, mechanistic studies have shown that abnormal fetal cardiovascular physiology in congenital heart disease disrupts normal placental-fetal circulation, contributing further to impaired growth. Furthermore, we reinforce current evidence supporting the importance of multidisciplinary intervention for improving birthing outcomes in high-risk pregnancies. Current studies emphasize that patients with complex maternal heart disease benefit most from structured, team-based management models that integrate maternal-fetal medicine, cardiology, anesthesiology, and neonatology.
Our secondary objective found that maternal CHD presents a higher risk for infants to be born small-for-gestational-age as compared to maternal AHD. This is a hypothesis-generating novel finding that requires further investigation and could significantly impact future treatment for this cohort.
Those affected by maternal heart disease are more likely to receive cardiac medications, including beta blockers. Among others, a recent analysis from the ESC EORP Registry of Pregnancy and Cardiac Disease evaluated perinatal outcomes after in-utero exposure to beta-blockers in women with heart disease. This study among others found that beta-blocker exposure was associated with an increased risk of low birth weight, small-for-gestational-age births and preterm delivery, likely because of the effect of these medications on uteroplacental blood flow and fetal growth regulation. Similar population-based studies also show increased risks of neonatal hypoglycemia and bradycardia following late-pregnancy β-blocker exposure, underscoring the need for careful monitoring. Given these findings, we conducted a secondary sensitivity analysis adjusting for beta-blocker use in our cohort to determine whether this variable explained the differences observed between the CHD and AHD groups. After this adjustment, the association between CHD and small-for-gestational-age births remained statistically significant, with a more than twofold increase in odds compared to AHD. This suggests that beta-blocker use alone does not fully explain the elevated risk of fetal growth restriction in CHD and highlights the role of underlying cardiac or placental pathophysiology as mentioned above. In contrast, other neonatal outcomes, including birth weight, NICU admission, mechanical ventilation, and length of stay, did not significantly differ between CHD and AHD after adjustment. These results reinforce that while beta-blockers are an important clinical consideration, structural and physiological factors specific to congenital heart disease may be more influential in driving certain neonatal risks, particularly small for gestational age.
Our study makes several important contributions to the existing literature on maternal heart disease and neonatal outcomes. We directly compared congenital and acquired heart disease, rather than grouping them together as many previous studies have done and identified distinct differences in neonatal outcomes. We focused specifically on neonatal measures, including birth weight, gestational age, Apgar scores, and NICU admissions, addressing a gap left by studies that primarily emphasize maternal or perinatal outcomes. In addition, we conducted the study in a multidisciplinary care setting that integrated maternal-fetal medicine, obstetrics, cardiology, anesthesiology, and genetics, allowing us to examine outcomes within a high-risk management model. We applied rigorous statistical methods, including the Kruskal-Wallis rank sum test for non-parametric comparisons, Chi-Square and Fisher’s Exact tests for categorical variables, and pairwise analyses to detect differences between cohort groups.
This study should be reviewed in consideration of its retrospective design, which did not allow for patient long-term follow-up. This limits our ability to make longitudinal assessments of developmental outcomes or ongoing health complications beyond the neonatal period. While this does not influence the criteria or results for this study, it limits the potential for future study using this cohort. Although we know key metrics of the neonates such as birth weight, NICU admission rates, preterm birth rates, and length of initial hospitalizations, we lack more clinical data (complete placental pathology or fetal echocardiographic measures) that might explain underlying mechanisms of observed outcomes such as fetal growth restriction. Furthermore, this study should not be interpreted as establishing causality, but rather as hypothesis generation, because results may be due to unobserved or observed variables. Unmeasured confounders such as the severity of maternal disease, variation in medication adherence, or environmental and social factors may have contributed to the associations we observed.
Another potential limitation of our study is that it is not contextualized within the parameters of alternative socioeconomic variables. Racial and ethnic disparities demonstrate significant discrepancies for maternal and birth outcomes, considering the pregnancy-related mortality ratio (PRMR) for Black birthing people was three to four times higher than the PRMRs for all other racial/ethnic groups in California between 2017 and 2019. Our study did not stratify by race or ethnicity, which prevents us from examining how maternal heart disease interacts with known disparities in access, quality of care, and health outcomes. Prior work has consistently shown that structural racism and inequities in access to quality maternal care drive disparities in severe maternal morbidity and mortality in the United States. While these factors fell outside of the purview of this study, it may be beneficial for future studies to investigate how maternal heart disease diagnosis fits within this framework, as these inequities may reflect differences in access and quality of multidisciplinary care. This discussion falls under the broader matter of social determinants of health, all of which should be investigated in relation to maternal heart disease and neonatal outcomes, as there is a substantial body of research linking social determinants of health like geography, income, and education to broad health outcomes.
Additionally, our sensitivity analysis was limited by sample size and was restricted to patients with complete data on beta-blocker exposure, which may affect the generalizability of those adjusted findings. Lastly, since this study was conducted at a single, coordinated suburban tertiary care center, the findings may be influenced by the unique clinical resources and referral patterns of this setting. Tertiary centers inherently have a population with higher disease incidence and case severity, thus skewing results toward more complex or higher-acuity cases. Therefore, our findings may have limited generalizability to broader or lower-risk obstetric populations and should not be assumed to apply broadly to other healthcare systems or countries. Multi-center studies could help determine how these outcomes translate across diverse populations and care environments.
Future studies should begin by examining clinical factors that may contribute to adverse neonatal outcomes in pregnancies complicated by maternal heart disease. One important area of focus is the role of beta-blocker use, which is commonly prescribed in this population and has been associated with fetal growth restriction. Investigating how beta-blocker use during pregnancy correlates with maternal weight gain, a known predictor of fetal growth, could help clarify whether medication use contributes independently to risks like small-for-gestational-age birth. In addition to these clinical parameters, prospective studies should also aim to uncover the biological basis for our findings in Objective 2. For instance, a prospective study could determine how maternal heart disease impacts fetal blood flow and the acid-base balance of the fetus. Fetal gas interpretation through means of umbilical cord blood gas analysis could serve as a useful base for biological sampling as it provides a strong indication of past, present and future fetal health based on acid-based metrics. The procedure is noninvasive and should be performed immediately at birth.
We found that maternal heart disease (CHD and AHD) is associated with adverse neonatal outcomes, reinforcing existing literature (Objective 1). Additionally, this study introduced that CHD carries a higher risk of small-for-gestational-age births compared to AHD (Objective 2). From our discoveries regarding CHD and AHD, we believe future studies should investigate biological mechanisms, social determinants, and long-term outcomes to build upon this foundational work. Through continued investigation, the aim is to improve multidisciplinary care for this high-risk and often vulnerable population.
Conclusion
Through this retrospective cohort study, we found that maternal heart disease, both maternal acquired heart disease and maternal congenital heart disease, is significantly associated with adverse neonatal outcomes, including lower birth weight, preterm birth, higher NICU admissions, and longer hospital stays. These findings highlight the importance of multidisciplinary prenatal care to address the specific risks posed by CHD and AHD. Furthermore, infants born to individuals with maternal CHD had a significantly higher risk of being small-for-gestational-age compared to those with maternal AHD and those not affected by maternal heart disease. Our sensitivity analysis suggests that the elevated risk of small for gestational age in CHD compared to AHD is not solely explained by beta-blocker use. Further research is needed to explore the biological mechanisms underlying these adverse neonatal outcomes and their long-term implications.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Human and Animal Rights
All reported studies/experiments with human or animal subjects performed by the authors have been previously published and complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Funding Statement
R25HL147666, MedScholar Award, Stanford Leader in Health disparities, Stanford-HBMC Summer Program
References
- Centers for Disease Control and Prevention. How does CDC identify severe maternal morbidity? Published February 8, 2021. Accessed July 1, 2025. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/smm/severe-morbidity-ICD.htm
- Collier AY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. NeoReviews. 2019;20(10):e561-e574. doi:10.1542/neo.20-10-e561
- California Maternal Quality Care Collaborative. CA-PAMR recent data. Accessed July 1, 2025. https://www.cmqcc.org/research/maternal-mortality-review-ca-pamr/ca-pamr-recent-data
- MBRRACE-UK. Maternal mortality 2020-2022. National Perinatal Epidemiology Unit. Accessed July 1, 2025. https://www.npeu.ox.ac.uk/mbrrace-uk/data-brief/maternal-mortality-2020-2022#causes-of-maternal-deaths-uk-2020-2022
- Saucedo M, Deneux-Tharaux C. Maternal mortality in France, 2016–2018: frequency, causes and women’s profile. Gynecol Obstet Fertil Senol. 2024;52(4):185-200. doi:10.1016/j.gofs.2024.02.020
- Mehta LS, Warnes CA, Bradley E, Burton T, Economy K, Mehran R, Safdar B, Sharma G, Wood M, Valente AM, Volgman AS, & On behalf of the American Heart Association Council on Clinical Cardiology; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular and Stroke Nursing; and Stroke Council. Cardiovascular Considerations in Caring for Pregnant Patients: A Scientific Statement From the American Heart Association. Circulation, 2020;141(23). https://doi.org/10.1161/CIR.0000000000000772
- Kovacevic, A., Elsässer, M., Fluhr, H., Müller, A., Starystach, S., Bär, S., & Gorenflo, M. (2021). Counseling for fetal heart disease-current standards and best practice. Translational pediatrics, 10(8), 2225–2234. https://doi.org/10.21037/tp-20-181
- Easter SR, Valente AM, & Economy KE. Creating a Multidisciplinary Pregnancy Heart Team. Current treatment options in cardiovascular medicine, 2020;22(1), 3. https://doi.org/10.1007/s11936-020-0800-x
- Gonzalez JM, Harris I, Jimenez Ramirez N, Myers D, Killion M, Thiet MP, Bianco K. Maternal cardiac disease and perinatal outcomes in a single tertiary care center. J Matern Fetal Neonatal Med. 2023;36(2). doi:10.1080/14767058.2023.2223336
- Mayer F, Bick D, Taylor C. Multidisciplinary care for pregnant women with cardiac disease: a mixed methods evaluation. Int J Nurs Stud. 2018;85:96-105. doi:10.1016/j.ijnurstu.2018.05.010
- Davis M, Arendt K, Bello N, et al. Team-based care of women with cardiovascular disease from pre-conception through pregnancy and postpartum: JACC Focus Seminar 1/5. J Am Coll Cardiol. 2021;77(14):1763-1777. doi:10.1016/j.jacc.2021.02.033
- Siu SC, Colman JM, Sorensen S, et al. Adverse neonatal and cardiac outcomes are more common in pregnant women with cardiac disease. Circulation. 2002;105(18):2179-2184. doi:10.1161/01.cir.0000015699.48605.08
- Sahu AK, Harsha MM, Rathoor S. Cardiovascular diseases in pregnancy: a brief overview. Curr Cardiol Rev. 2022;18(1):e250821195824. doi:10.2174/1573403X17666210825103653
- Gelson E, Curry R, Gatzoulis MA, Swan L, Lupton M, Steer P, Johnson M. Effect of maternal heart disease on fetal growth. Obstet Gynecol. 2011;117(4):886-891. doi:10.1097/AOG.0b013e31820cab69
- Cauldwell M, Steer P, Sterrenburg M, et al. Birth weight in pregnancies complicated by maternal heart disease. Heart. 2019;105(4):391-398. doi:10.1136/heartjnl-2018-313551
- Sørbye IK, Haualand R, Wiull H, Letting AS, Langesæter E, Estensen ME. Maternal beta-blocker dose and risk of small-for-gestational-age in women with heart disease. Acta Obstet Gynecol Scand. 2022;101(7):794-802. doi:10.1111/aogs.14363
- Kong CW, Tay JA, Chen H, Ersbøll AS. Beta-blockers in pregnancy: impacts on the fetus and neonate. Int J Cardiol. 2024. doi:10.1016/j.ijcard.2024.05.031
- Sperling MM, Leonard SA, Miller SE, Hurtado J, El-Sayed YY, Herrero T, Faig J, Carter S, Blumenfeld YJ. Fasting compared with fed and oral intake before the 1-hour oral glucose tolerance test: a randomized controlled trial. Obstet Gynecol. 2023;141(1):126-133. doi:10.1097/AOG.0000000000005013
- R Foundation for Statistical Computing. R: A language and environment for statistical computing. Vienna, Austria. https://www.r-project.org/
- Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, et al. ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J. 2018;39(34):3165-3241. doi:10.1093/eurheartj/ehy340
- Gonzalez JM, Harris I, Jimenez Ramirez N, et al. Maternal cardiac disease and perinatal outcomes in a single tertiary care center. J Matern Fetal Neonatal Med. 2023;36(2):2223336. doi:10.1080/14767058.2023.2223336
- Bender A, Heimann K, Tinneberg HR, et al. Neonatal outcomes and length of NICU stay in pregnancies complicated by maternal heart disease. Arch Gynecol Obstet. Published online 2024. doi:10.1055/a-2311-4945
- Snoep MC, Aliasi M, van der Meeren LE, Jongbloed MRM, DeRuiter MC, Haak MC. Placenta morphology and biomarkers in pregnancies with congenital heart disease: a systematic review. Placenta. 2021;112:189-196. doi:10.1016/j.placenta.2021.07.297
- Ho DY, Josowitz R, Katcoff H, et al. Mid-gestational fetal placental blood flow is diminished in the fetus with congenital heart disease. Prenat Diagn. 2020;40(11):1432-1438. doi:10.1002/pd.5791
- Rychik J, Donofrio MT, Falkensammer CB, et al. Fetal cardiovascular physiology in congenital heart disease. Circulation. 2014;129(13):1349-1361. doi:10.1161/CIRCULATIONAHA.113.005701
- White D. Development of a center of excellence for caring for pregnant women who have heart disease. J Obstet Gynecol Neonatal Nurs. 2019;48(3 Suppl):S21.
- Canobbio MM, Warnes CA, Aboulhosn J, et al. Management of pregnancy in patients with complex congenital heart disease: a scientific statement from the American Heart Association. Circulation. 2017;135(8):e50-e87. doi:10.1161/CIR.0000000000000458
- Ramlakhan KP, Roos-Hesselink JW, Basso T, et al; ROPAC Investigators. Perinatal outcomes after in utero exposure to beta-blockers in women with heart disease: data from the ESC EORP registry of pregnancy and cardiac disease (ROPAC). Int J Cardiol. 2024;410:132234. doi:10.1016/j.ijcard.2024.132234
- Bateman BT, Patorno E, Desai RJ, et al. Late pregnancy β blocker exposure and risks of neonatal hypoglycemia and bradycardia. Pediatrics. 2016;138(3):e20160731. doi:10.1542/peds.2016-0731
- Nicholls-Dempsey L, Badeghiesh A, Baghlaf H, Dahan MH. How does high socioeconomic status affect maternal and neonatal pregnancy outcomes? A population-based study among American women. Eur J Obstet Gynecol Reprod Biol X. 2023;20:100248. doi:10.1016/j.eurox.2023.100248
- Armstrong L, Stenson BJ. Use of umbilical cord blood gas analysis in the assessment of the newborn. Arch Dis Child Fetal Neonatal Ed. 2007;92(6):F430-F434. doi:10.1136/adc.2006.099846