





Neurogenic Sexual Dysfunction: Diagnosis and Management
Algorithm for the Diagnosis and Management of Symptoms of Neurogenic Sexual Dysfunction
Artem Valeryevich Bershadsky, MD, PhD¹, Andrey Avgustovich Belkin, MD, DSc², Roman Vyacheslavovich Salyukov, MD, DSc³
- Urologist at the Center for Medical Rehabilitation, Clinical Institute of Brain Berezovsky city, Russia
- Professor, Department of Neurology and Department of Anesthesiology and Intensive Care, Ural State Medical University, Yekaterinburg, Russia; Ural State Medical University, Ministry of Health of the Russian Federation, Yekaterinburg, Russia
- Professor, Department of Urology with Courses in Oncology, Radiology, and Andrology, Faculty of Advanced Training of Medical Workers, Peoples’ Friendship University of Russia, Ministry of Science and Higher Education of the Russian Federation; Associate Professor, Department of Medical Rehabilitation, Faculty of Continuing Medical Education, Pirogov Russian National Research Medical University, Ministry of Health of the Russian Federation; Research Fellow, Russian Scientific Center of Roentgenoradiology, Ministry of Health of the Russian Federation, Moscow, Russia
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Bershadsky, A.V., et al., 2025. Algorithm for the Diagnosis and Management of Symptoms of Neurogenic Sexual Dysfunction at the Rehabilitation Treatment Stage. Medical Research Archives, [online] 13(4).
https://doi.org/10.18103/mra.v13i4.6496
COPYRIGHT: © 2025 European Society of Medicine.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6496
ISSN 2375-1924
ABSTRACT
Background: Neurogenic sexual dysfunction (NSD) is a frequent yet underdiagnosed consequence of neurological disorders such as spinal cord injury (SCI), multiple sclerosis (MS), stroke, and Parkinson’s disease (PD). Despite its significant impact on psychosocial well-being and quality of life, NSD remains insufficiently addressed in standard rehabilitation protocols.
Objective: To describe an original, context-adapted clinical algorithm for the diagnosis and management of neurogenic sexual dysfunction during the rehabilitation phase, based on the PLISSIT model and augmented by a structured feedback mechanism.
Methods: A modified diagnostic and therapeutic protocol was developed and implemented in a neurorehabilitation center in Russia, addressing systemic barriers such as the absence of sexual health professionals, lack of guidelines, and limited physician training. The model utilizes the first three stages of PLISSIT—Permission, Limited Information, and Specific Suggestions—and introduces a home-based feedback protocol to replace the Intensive Therapy phase. This protocol includes functional evaluation, educational counseling, environmental adaptation, and structured self-assessment after the first sexual attempt.
Results: All ten participants (aged 23–52) with chronic spinal cord injury and their partners completed the diagnostic protocol, including a structured feedback questionnaire. Sexual activity was conducted either in a home environment (8 couples) or in a designated guest room within the rehabilitation facility (2 couples). Among six male participants, five achieved erection and four reported successful penetration; two experienced orgasm, and one reported ejaculation. Among four female participants, three reported vaginal dryness and two reported discomfort during intercourse. Spasticity was noted in seven participants, and positioning difficulties were reported in six cases. Genital hypoesthesia or altered sensation was identified in nine participants. Eight participants reported post-activity fatigue, and two noted transient cardiovascular symptoms. All couples followed at least one clinical recommendation: lubricants were used in six cases and positioning aids in eight. Three male participants used phosphodiesterase type 5 inhibitors. Feedback forms were fully completed in all cases, with high adherence across physiological, emotional, and partner-related domains.
Conclusion: This adapted PLISSIT-based algorithm provides a feasible, replicable approach to the early diagnosis and treatment of sexual dysfunction within rehabilitation settings. The structured feedback loop enhances ecological validity, empowers patients, and facilitates targeted, multidisciplinary care. Further multicenter studies are warranted to validate its broader applicability.
Keywords: Neurogenic sexual dysfunction, PLISSIT model, spinal cord injury, rehabilitation, feedback protocol, patient-centered care, sexual health, multidisciplinary approach.
Sexual health is a fundamental component of overall well-being and personal identity, even in the context of severe neurological impairment. According to the World Health Organization, sexual health is a basic human right and integral to quality of life. However, sexual dysfunction of neurogenic origin (NSD) remains an underrecognized and underaddressed consequence of spinal cord injury (SCI), multiple sclerosis (MS), stroke, and other neurological disorders. Studies indicate that NSD affects up to 80% of individuals with neurological conditions, yet it is rarely addressed systematically in standard rehabilitation protocols¹²³.
Sexual dysfunction can be classified into three interrelated categories: primary dysfunction, resulting from direct damage to neural pathways; secondary dysfunction, associated with neurological sequelae such as spasticity, bladder or bowel dysfunction, and fatigue; and tertiary dysfunction, which encompasses psychological, relational, and sociocultural factors such as anxiety, altered body image, or reduced self-esteem⁴⁵⁶. These domains interact dynamically, complicating both diagnosis and treatment. Despite increasing awareness of its prevalence, NSD is often omitted from routine care due to barriers including lack of clinician training, discomfort with the topic, absence of clear guidelines, and limited access to sexual health professionals⁷.
A growing body of evidence highlights the importance of integrating sexual rehabilitation into multidisciplinary care for neurological patients. Interventions that combine education, pharmacological support, physical therapy, and psychosexual counseling have demonstrated improvements in patient satisfaction, adherence to rehabilitation, and psychosocial adjustment⁸. Among the tools available to guide clinical work in this domain, the PLISSIT model (Permission, Limited Information, Specific Suggestions, Intensive Therapy) has been widely adopted. It provides a structured, stepwise approach to addressing sexual concerns. However, in real-world settings—particularly in systems with constrained resources—the final stage of the model (Intensive Therapy) is frequently inaccessible.
In our clinical experience, many patients with SCI and other neurological conditions receive little or no guidance regarding sexual recovery, despite expressing significant concerns⁹. Additionally, hospital-based assessments often fail to reflect the lived experience of sexual activity, which depends on emotional readiness, partner interaction, and environmental comfort—factors not replicable in sterile or institutional settings.
To address these gaps, we developed an adapted diagnostic and therapeutic algorithm based on the first three levels of the PLISSIT model, enriched with a structured, real-world feedback protocol. This protocol is designed to assess sexual function not only from a physiological standpoint, but also through the lens of contextual, emotional, and interpersonal dynamics. Following preparatory counseling and individualized recommendations, patients and their partners are invited to attempt sexual activity in a familiar, emotionally supportive environment and complete a structured feedback questionnaire within 24 hours.
The aim of this study is to describe the implementation of this novel, feedback-informed PLISSIT-based model in a neurorehabilitation setting and to evaluate its feasibility, clinical utility, and acceptability among patients and their partners. We hypothesize that the use of structured feedback collected under ecological conditions will improve diagnostic precision, inform therapeutic decisions, and enhance partner engagement in the rehabilitation process.
Materials and Methods
Study Design and Setting
This study was conducted as a prospective observational pilot within a neurorehabilitation program at Clinical institute of brain, aimed at evaluating the feasibility and clinical utility of a structured diagnostic and feedback-based algorithm for the assessment and management of neurogenic sexual dysfunction (NSD) following spinal cord injury (SCI). The protocol was based on a modified PLISSIT framework and incorporated structured sexual counseling, personalized recommendations, and post-coital self-assessment via a feedback questionnaire.
Participants
A total of 10 adult patients (aged 23–52) with chronic consequences of traumatic spinal cord injury participated in the study. All individuals were undergoing rehabilitation and presented with varying levels of spinal lesions (cervical, thoracic, or lumbosacral), verified through neurological assessment and imaging. The time since injury ranged from 8 months to 4 years.
Inclusion Criteria
Participants were eligible if they met the following criteria:
-
Documented history of spinal cord injury with residual neurogenic dysfunction;
-
Medical stability to engage in sexual activity;
-
Absence of active infectious disease (e.g., urinary tract infection, decubitus infection, or systemic inflammation);
-
Presence of a stable sexual partner willing to participate;
-
Ability to attempt sexual intercourse either in a dedicated guest room at our institute or in home conditions with full adherence to provided recommendations;
-
Consent to complete a structured feedback questionnaire within 24 hours after the attempted intercourse.
Intervention Protocol
Each participant and their partner underwent:
-
Multidisciplinary functional evaluation involving a neurologist, urologist, physical therapist, and occupational therapist;
-
A semi-structured educational session led by a neuro-urologist, covering the neurophysiology of sexual function, expected challenges, and adaptive strategies;
-
Delivery of an individualized instruction sheet, including ergonomic recommendations, hygiene protocols, pharmacological support if applicable, and use of sexual aids (e.g., lubricants, pillows, vibrators).
Feedback Collection
Following the sexual activity, both the patient and their partner independently completed a custom-designed feedback questionnaire. This tool included Likert-scale and open-ended questions on:
-
Physical comfort, spasticity, and pain;
-
Quality of erection and orgasm (in men), or lubrication and pain (in women);
-
Emotional experience, confidence, and intimacy;
-
Environmental and positioning factors;
-
Suggestions for improvement and unmet needs.
Ethical Considerations
The study was approved by the local Institutional Ethics Committee. All participants provided written informed consent. Personal data were anonymized, and couples were informed of their right to withdraw from the study at any stage without consequences to their medical care.
Sexuality in Neurological Patients:
The Rationale for Integration into Rehabilitation Programs
Sexuality remains a fundamental aspect of human well-being and identity, even in the context of severe neurological disease. According to the WHO (2004), sexual health is a basic human right and an integral component of quality of life¹⁰. Despite this, sexual concerns are often neglected in clinical practice, particularly among patients with chronic neurological impairments. Neurogenic sexual dysfunction (NSD) is a prevalent yet underrecognized consequence of disorders such as spinal cord injury (SCI), multiple sclerosis (MS), and stroke. These conditions compromise sexual function through a combination of neurological disruption, somatic disability, and psychosocial maladaptation¹¹.
Contemporary classification distinguishes between primary, secondary, and tertiary components of NSD. Primary dysfunction arises from direct neurogenic disruption of afferent and efferent pathways controlling sexual response. Secondary dysfunction reflects comorbid neurological symptoms—bladder and bowel dysfunction, spasticity, fatigue, cognitive or sensorimotor deficits—that impede sexual activity. Tertiary dysfunction encompasses the psychological and sociocultural consequences of chronic illness, including loss of body image, anxiety, low self-esteem, and relationship disruption¹². These levels interact dynamically, compounding the clinical burden and contributing to reduced quality of life, emotional distress, and social isolation.
Findings from qualitative and quantitative research confirm the strong association between NSD and depression, anxiety, and decreased life satisfaction in both men and women. Common manifestations include reduced libido, erectile and orgasmic dysfunction in men, and anorgasmia, dyspareunia, and lubrication deficits in women¹³. These symptoms persist across all stages of disease progression and are often intensified by the absence of targeted medical or psychological intervention¹⁴. Notably, despite the high prevalence of NSD, most healthcare professionals do not address sexuality proactively during consultations. Studies cite lack of training, time constraints, and cultural taboos as common barriers¹⁵.
Integration of sexual health into neurological rehabilitation represents both a clinical need and an opportunity to improve outcomes. Evidence from neurorehabilitation studies indicates that incorporating sexual counseling, pelvic floor therapy, pharmacologic treatment (e.g., PDE-5 inhibitors, hormone therapy), and neuromodulation techniques leads to improved patient-reported satisfaction and psychosocial adjustment¹⁶. Moreover, addressing sexual function contributes positively to adherence with broader rehabilitation goals, particularly in the domains of intimacy, self-care, and interpersonal relationships¹⁷.
In rehabilitation practice, restoring pelvic autonomic function is a cornerstone of managing NSD. Multimodal interventions combining somatic rehabilitation with targeted neuro-urological approaches (e.g., sacral neuromodulation, electrostimulation, functional training) are especially promising. However, successful implementation requires trained personnel and a paradigm shift: from viewing sexual dysfunction as an ancillary concern to recognizing it as a core determinant of recovery and reintegration¹⁸.
Early Diagnosis and Multidisciplinary Management of Neurogenic Sexual Dysfunction During Rehabilitation
Neurogenic sexual dysfunction (NSD) is a frequent and disabling consequence of neurological disorders, including spinal cord injury (SCI), multiple sclerosis (MS), and Parkinson’s disease (PD). Failure to recognize and address NSD in a timely manner leads to progression of symptoms, deterioration of emotional well-being, and a measurable decline in quality of life. Early identification and a coordinated, multidisciplinary intervention are critical at the rehabilitation stage to optimize functional outcomes¹⁹.
Importance of Early Diagnosis
Accurate and timely diagnosis of NSD begins with a comprehensive clinical evaluation. This includes:
-
Detailed sexual history, encompassing changes in libido, arousal, orgasmic response, genital sensation, and partner dynamics.
-
Neurological examination, focusing on spinal and peripheral pathways involved in sexual reflex arcs and autonomic control.
Targeted physiological assessments, such as somatosensory evoked potentials (SSEPs), bulbocavernosus reflex testing, and electromyography (EMG) of the pelvic floor, to evaluate the integrity of neurogenic control mechanisms.
Although advanced diagnostic tools may aid in delineating the neurophysiological basis of dysfunction, diagnosis is often clinical and requires specialized expertise. The subtleties of NSD, particularly when overlapping with urinary or bowel symptoms, necessitate structured screening within routine neurological rehabilitation.²⁰
THE ROLE OF A MULTIDISCIPLINARY TEAM
Effective rehabilitation of NSD requires coordinated input from urologists, neurologists, physical medicine specialists, clinical psychologists, and sexual health professionals. Each discipline contributes to a holistic, patient-centered plan of care.²¹ Key components include:
-
Personalized rehabilitation protocols, tailored to the degree and type of neurological impairment.
-
Pharmacological therapy, such as phosphodiesterase type 5 inhibitors and hormone replacement, targeting vascular and hormonal contributors to dysfunction.
-
Physical interventions, including pelvic floor muscle training and electrical stimulation, to restore motor and autonomic function in the pelvic region.
-
Psychosexual counseling, addressing body image concerns, relationship dynamics, emotional adaptation, and expectations related to sexual recovery.
Integration of these approaches within the rehabilitation continuum enables a shift from symptom-oriented care to functional and psychosocial restoration.
Neurophysiological Mechanisms of Sexual Function and Their Disruption in Neurological Disorders
Sexual function is governed by a complex integration of central, spinal, and peripheral nervous system pathways, involving both autonomic and somatic components. It is modulated by neurochemical signaling, hormonal regulation, and afferent feedback from genital and extragenital zones.²²
Disruption of these mechanisms at any level—cortical, subcortical, spinal, or peripheral—may result in neurogenic sexual dysfunction (NSD), frequently observed in patients with spinal cord injury (SCI), multiple sclerosis (MS), stroke, and other neurological diseases.
CENTRAL REGULATION
Key brain regions involved in sexual function include:
-
Hypothalamus (especially the paraventricular nucleus), which integrates hormonal and autonomic control, and modulates erection and ejaculation via oxytocinergic pathways.
-
Limbic system, notably the amygdala and hippocampus, which governs emotional and motivational aspects of sexual behavior. Bilateral amygdala lesions can result in hypersexuality, as seen in Kluver–Bucy syndrome.
-
Prefrontal cortex, responsible for cognitive modulation of sexual responses, impulse control, and inhibition of socially inappropriate behavior.
-
Thalamus and cingulate gyrus, which process sensory inputs relevant to sexual arousal and pleasure.
-
Periaqueductal gray (PAG) in the midbrain, involved in balancing excitatory and inhibitory signals during sexual arousal and coordinating autonomic outflow.³
SPINAL AND PERIPHERAL PATHWAYS
Peripheral sexual function is mediated by three main neural pathways:
-
Parasympathetic (S2–S4):
Mediates vasodilation and engorgement of erectile tissue via acetylcholine and nitric oxide (NO). Essential for penile and clitoral erection and vaginal lubrication. -
Sympathetic (T11–L2):
Controls ejaculation, detumescence, and closure of the bladder neck to prevent retrograde ejaculation through noradrenergic signaling. -
Somatic (S2–S4, via pudendal nerve):
Coordinates rhythmic contraction of the perineal muscles (bulbospongiosus and ischiocavernosus) involved in orgasm and maintenance of erection.²⁴
IMPACT OF NEUROLOGICAL LESIONS ON SEXUAL FUNCTION
Cerebral lesions may impair sexual desire, arousal, and emotional regulation. Damage to the frontal lobes can suppress libido and affect behavioral inhibition. Amygdala involvement may trigger disinhibition or hypersexuality, while PAG dysfunction may impair autonomic balance and lead to sexual hypoactivity.
Spinal cord injury results in segmental disruption of reflexogenic and psychogenic sexual responses, depending on lesion level:
-
Above T6: Reflexogenic erection is often preserved, but psychogenic pathways are disrupted.
-
Below L2: Psychogenic input may remain, while reflex arcs are compromised.
-
S2–S4 lesions: Both reflexogenic and psychogenic components are impaired, leading to severe erectile and ejaculatory dysfunction.²⁵
In women, analogous mechanisms affect vaginal lubrication, genital vasocongestion, and orgasmic response, with neurogenic disruption resulting in dryness, anorgasmia, and dyspareunia.
Understanding the neurophysiology of sexual function is essential for the accurate diagnosis and management of NSD. Clinicians should assess both psychogenic and reflexogenic components, integrating neurological, urological, and sexual histories. Functional neuroimaging (e.g., fMRI), electrophysiological tests (e.g., SSEPs, bulbocavernosus reflex latency), and urodynamic studies can help localize lesions and differentiate between central and peripheral dysfunction.
Sexual function is regulated by a hierarchically organized neural network involving cortical, spinal, and peripheral mechanisms. Neurological diseases frequently disrupt this network, leading to NSD. A thorough understanding of neurophysiological control and site-specific patterns of dysfunction is vital for accurate diagnosis and the development of individualized rehabilitation protocols. Incorporating electrophysiological and imaging tools enhances diagnostic precision and informs the design of targeted interventions aimed at restoring sexual health in neurologically impaired patients.²⁵
Diagnosis of Neurogenic Sexual Dysfunction
The diagnostic approach to neurogenic sexual dysfunction is based on a standardized, stepwise evaluation that incorporates clinical history, neurological examination, functional testing, and patient-reported outcomes.²⁶ This comprehensive diagnostic framework is summarized in Table 1 and provides a practical guide for structured assessment in rehabilitation settings.
Table 1
| Diagnostic Modality | Purpose | Clinical Relevance |
|---|---|---|
| Sexual history and clinical interview | Assessment of libido, arousal, orgasm, and relationship factors | First-line method for identifying type, onset, and impact of dysfunction |
| Neurological examination | Evaluation of sensory and motor deficits, reflexes, sacral integrity | Localizes neurological lesion (central vs. peripheral); correlates with dysfunction |
| Urological / Gynecological exam | Inspection of genital anatomy, mucosa, and pelvic muscle tone | Identifies somatic contributors (atrophy, spasticity, sensory loss) |
| Pharmacologically induced erection test (men) | Intracavernosal injection of prostaglandins | Assesses vascular and neurogenic integrity of erectile tissue |
| SSEPs (Somatosensory Evoked Potentials) | Measures afferent conduction from genital regions | Detects spinal or peripheral sensory pathway dysfunction |
| Bulbocavernosus Reflex (BCR) | Reflex integrity of pudendal nerve and sacral spinal cord | Objective indicator of sacral segment (S2–S4) function |
| Pelvic floor EMG | Assessment of voluntary and reflexive pelvic floor muscle activation | Helps differentiate central vs. peripheral motor impairment |
| Functional MRI (fMRI) | Visualizes brain activation during arousal tasks | Research tool; useful in differentiating psychogenic vs. organic dysfunction |
| Urodynamic testing | Measures bladder compliance, detrusor activity, sphincter function | Detects coexisting lower urinary tract dysfunction linked to NSD |
| Hormonal panel | Testosterone, estradiol, prolactin, LH, FSH | Identifies hypogonadism, endocrine disorders contributing to dysfunction |
| Metabolic profile | Glucose, insulin, lipid panel | Screens for diabetes, insulin resistance, and metabolic syndrome |
Diagnostic Algorithm: Application of the PLISSIT Model in Neurogenic Sexual Dysfunction
A structured, phased approach is essential for the assessment of neurogenic sexual dysfunction (NSD), particularly in the rehabilitation context. The PLISSIT model (Permission, Limited Information, Specific Suggestions, Intensive Therapy), initially developed in behavioral sex therapy and now widely adopted in neurorehabilitation, offers a practical framework for addressing sexual concerns in patients with neurological disorders.²⁷
The model comprises four escalating levels of clinical engagement:
-
Permission involves creating a safe, nonjudgmental space for patients to voice concerns regarding sexual function, validating their experiences as part of holistic care.
-
Limited Information provides tailored evidence-based explanations of how neurological conditions and related symptoms affect sexual health.
-
Specific Suggestions includes individualized recommendations for managing identified issues, such as strategies to improve arousal, positioning, or partner communication.
-
Intensive Therapy refers to referral to specialized care—sexual medicine, psychotherapy, or neuropsychology—when complex dysfunctions exceed the scope of routine rehabilitation.
In NSD, where sexual impairment may result from a combination of central nervous system lesions, autonomic and somatic pathway disruption, cognitive deficits, and psychosocial factors, this model allows for stratified diagnostic clarity.²⁸ It facilitates the identification of barriers that patients may be reluctant to report spontaneously, and guides clinicians in adjusting interventions based on symptom severity and patient readiness.
However, real-world implementation of the PLISSIT model presents several challenges:
-
Initiating the dialogue:
At the Permission stage, many clinicians feel unprepared or uncomfortable initiating conversations about sexuality. Cultural taboos, lack of formal training, and concerns about patient discomfort often contribute to silence around sexual health. Surveys indicate that even experienced neurologists and rehabilitation professionals seldom address sexual dysfunction unless patients raise the issue directly. -
Knowledge limitations:
At the Limited Information and Specific Suggestions stages, clinicians may lack adequate understanding of sexual neurophysiology, pharmacological options, or rehabilitative strategies. The absence of formal training in sexual medicine during core medical education contributes to inconsistent and superficial management of NSD. -
Interdisciplinary coordination:
Implementing Specific Suggestions requires integration of neurological, urological, gynecological, endocrine, and psychological expertise. This demands a multidisciplinary structure that may not be available in all rehabilitation settings. -
Access to specialized care:
At the Intensive Therapy level, access to qualified sexual health professionals is limited in many regions, especially in underserved or rural areas. This restricts the model’s final tier of care delivery, leaving complex dysfunctions inadequately addressed.
Despite these barriers, the PLISSIT model remains a validated and adaptable tool for structuring sexual health assessment. It empowers clinicians to address NSD systematically, build therapeutic trust, and guide patients toward appropriate interventions.²⁹
For patients with neurological impairment—such as those with spinal cord injury, multiple sclerosis, or Parkinson’s disease—who face multi-level sexual dysfunction, this model provides a nuanced diagnostic algorithm that aligns with the complexity of their clinical presentation.
To further investigate the diagnostic gap in routine clinical care, we conducted a local mini-survey at our neurorehabilitation center among patients with confirmed neurogenic sexual dysfunction. A total of 211 individuals undergoing inpatient or outpatient treatment completed an anonymous questionnaire.
Only 10% of respondents reported that a healthcare provider had initiated a conversation about sexual function during their hospital stay. At the same time, 58.2% of patients indicated a strong desire to discuss issues related to neurogenic sexual dysfunction with a medical professional.
The results of this survey are presented in Figure 1 and Figure 2 below and illustrate a marked discrepancy between patients’ informational and emotional needs and the current clinical practice. These findings further emphasize the urgency of integrating systematic sexual health assessments into neurorehabilitation and support the rationale for the present study.
Figure 1
Have you discussed your sexual function with a physician or rehabilitation specialist after the onset of your condition?
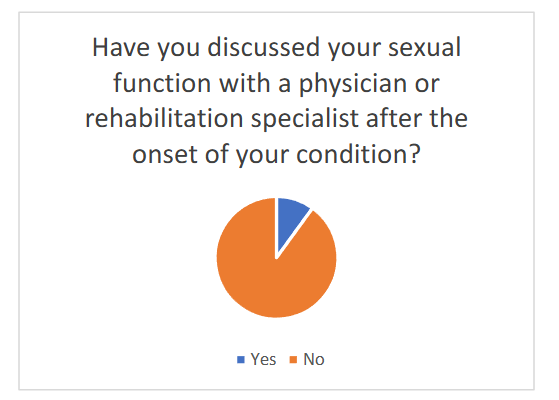
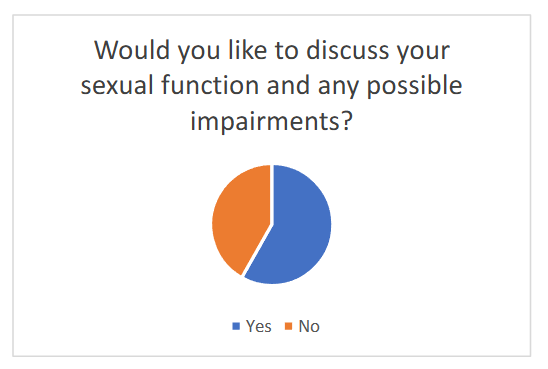
Figure 2
Would you like to discuss your sexual function and any possible impairments?
A Novel Methodology for the Identification and Objectification of Symptoms of Neurogenic Sexual Dysfunction
In our clinical neurorehabilitation center, we have developed and implemented an original diagnostic and therapeutic algorithm for working with patients who experience sexual dysfunction as a result of neurological disease or injury.
The foundation of this approach is the PLISSIT model—an evidence-based, four-stage framework for the clinical management of sexual concerns (Permission, Limited Information, Specific Suggestions, Intensive Therapy). Recognizing the structural and organizational specificities of the Russian healthcare system, we adapted this model to better fit the realities of local clinical practice and rehabilitation infrastructure.
Rationale for Model Adaption
Several challenges have shaped our approach to the clinical management of neurogenic sexual dysfunction (NSD):
-
The absence of national guidelines on the assessment and treatment of NSD at various stages of care;
-
A lack of specialized professionals (e.g., sexologists or sexual health psychologists) within standard rehabilitation teams;
-
Limited knowledge and experience among neurologists, urologists, and rehabilitation physicians regarding NSD assessment and intervention;
-
The absence of quality indicators related to the restoration of sexual function as a rehabilitation outcome;
-
A lack of familiarity among clinicians with early diagnostic features of neurogenic sexual disorders and the need for structured evaluation.
In light of these systemic constraints, we focused our efforts on maximizing the potential of the first three stages of the PLISSIT model—Permission, Limited Information, and Specific Suggestions—while creating a feedback loop that effectively replaces the rarely available “Intensive Therapy” stage.
Our central premise is that sexual function, to be meaningfully assessed and rehabilitated, must be addressed in a real-world, emotionally comfortable setting, closely aligned with the patient’s normal life context.
The Importance of Contextual Assessment
A unique feature of our approach is the explicit recognition that sexual function cannot be reliably evaluated in clinical or hospital settings, especially in the early post-acute phase.
The sexual act is not a purely mechanical process; it requires:
-
Emotional readiness
-
Environmental familiarity
-
Partner dynamics
These factors are often suppressed or distorted in institutional environments.
Thus, a key element of our algorithm is ensuring that the couple has the opportunity to attempt sexual activity in familiar, emotionally neutral surroundings, informed by new physical realities and individualized clinical recommendations.
This provides the only realistic basis for identifying actual dysfunctions and implementing effective, patient-tailored interventions.
Algorithm Structure: A Stepwise Model
Step 1: Functional and Physiological Evaluation
A multidisciplinary team comprising:
-
neurologist
-
urologist
-
physical therapist
-
occupational therapist
performs a detailed assessment of the patient’s current physical capacity. This includes:
-
Motor and sensory evaluation relevant to sexual function;
-
Assessment of postural tolerance, muscle tone, spasticity, and endurance;
-
Identification of safe and feasible sexual positions.
The aim is to formulate specific recommendations for the couple regarding physical adaptations and positioning strategies to facilitate successful intercourse.
Step 2: Educational Counseling Session with the Couple
This session is conducted by a neuro-urologist and includes:
-
A detailed explanation of the neurophysiological mechanisms responsible for NSD;
-
A review of the specific impairments identified in the patient (e.g., loss of reflexogenic erection, genital sensory deficits, autonomic dysfunction);
-
Emphasis on preparing the couple for their first attempt at sexual activity following disease onset.
Importantly, couples are informed that the absence of spontaneous sexual response during hospitalization is not a reliable diagnostic indicator.
For example:
Just as detrusor function cannot be assessed in a patient with an indwelling catheter, sexual function cannot be meaningfully assessed in the absence of appropriate psychological and environmental stimuli.
The consultation concludes with written personalized recommendations, including:
-
Guidelines for preparing the physical environment
(lighting, support devices, temperature); -
Advice on preparing the patient’s body
(bladder management, spasticity control, lubrication); -
Suggested use of medical devices and sexual aids
(vacuum erection devices, lubricants, vibrators).
Step 3: Home-Based Attempt and Feedback Collection
A distinctive and novel component of our approach is the use of a structured feedback questionnaire, completed by the couple after their attempt at sexual activity.
This tool enables:
-
The objectification of symptoms in the patient’s natural environment;
-
Identification of previously unreported barriers to sexual intimacy;
-
Motivation for the couple to remain actively engaged in the rehabilitation process.
The feedback form documents outcomes such as:
-
erection quality and duration
-
pain or discomfort
-
emotional response
-
communication between partners
-
post-coital experience
This not only guides the clinical team in further planning but also enhances the couple’s awareness of progress and challenges.
Step 4: Differential Diagnosis and Personalized Intervention
Using data from both the clinical evaluation and the feedback form, clinicians differentiate organic versus psychogenic contributors to NSD.
At this point:
-
A psychologist or sexologist may be engaged to address affective or cognitive factors;
-
The neuro-urologist may initiate or adjust pharmacologic therapy
(e.g., PDE-5 inhibitors, hormone replacement); -
Technical solutions such as assistive positioning devices or neuromodulation may be considered.
The couple is then invited to continue the cycle, with repeated feedback and adaptation, promoting a dynamic and responsive rehabilitation process.
Clinical and Scientific Implications
Our algorithm offers an accessible, replicable approach to the diagnosis and early management of NSD within real-world constraints.
It addresses gaps in:
-
clinical competence
-
infrastructure
-
patient-centered practice
The emphasis on contextual, real-life evaluation and on interactive collaboration with the couple distinguishes this approach from traditional hospital-based strategies.
From a research perspective, the feedback questionnaire constitutes a valuable tool for outcome monitoring and future multicenter validation.
It also offers potential for integration into digital health platforms and tele-rehabilitation services for sexual function—an emerging area of interest in post-pandemic rehabilitation medicine.
Structured Preparation and Feedback Protocol for Sexual Activity in Neurorehabilitation: A Patient-Centered Model
In the context of neurogenic sexual dysfunction (NSD), particularly following spinal cord injury or other neurological disorders, restoration of sexual function is a vital, though often under-addressed, component of rehabilitation.
To support patients and their partners during this challenging transition, we developed a structured Preparation and Feedback Protocol (PFP) designed to enhance clinical outcomes through practical guidance and post-activity analysis.
Psychological Preparation and Partner Communication
Emotional readiness and dyadic understanding are critical prerequisites for successful sexual reintegration.
Patients and their partners are encouraged to:
-
Engage in open dialogue about expectations, fears, and changes in function;
-
Normalize anxiety related to first post-injury sexual experiences;
-
Prioritize emotional intimacy and mutual respect over performance-oriented goals.
These preparatory steps are facilitated by clinical staff (usually a neuro-urologist or trained rehabilitation psychologist) using semi-structured discussions and printed guidance materials.
Practical Preparation and Positioning
To ensure physical safety and maximize comfort, patients are advised to rehearse positions and prepare their environment in advance.
Recommendations include testing positions such as:
-
Supine with partner on top (for reduced exertion);
-
Side-lying (for patients with balance impairments).
Motivation for the couple to remain actively engaged in the rehabilitation process.
The feedback form documents outcomes such as erection quality, duration, pain or discomfort, emotional response, communication between partners, and post-coital experience. This not only guides the clinical team in further planning but also enhances the couple’s awareness of progress and challenges.
Step 4: Differential Diagnosis and Personalized Intervention
Using data from both the clinical evaluation and the feedback form, we differentiate organic versus psychogenic contributors to NSD. At this point:
-
A psychologist or sexologist is engaged to address affective or cognitive factors;
-
The neuro-urologist may initiate or adjust pharmacologic therapy (e.g., PDE5 inhibitors, hormone replacement);
-
Technical solutions such as assistive positioning devices or neuromodulation may be considered.
The couple is then invited to continue the cycle, with repeated feedback and adaptation, which promotes a dynamic, responsive rehabilitation process.
Clinical and Scientific Implications
Our algorithm offers an accessible, replicable approach to the diagnosis and early management of NSD within real-world constraints. It addresses gaps in clinical competence, infrastructure, and patient-centered practice.
The emphasis on contextual, real-life evaluation and on interactive collaboration with the couple distinguishes this approach from traditional hospital-based strategies.
From a research perspective, the feedback questionnaire constitutes a valuable tool for outcome monitoring and future multicenter validation. It also offers potential for integration into digital health platforms and tele-rehabilitation services for sexual function—a growing area of interest in post-pandemic rehabilitation medicine.
Structured Preparation and Feedback Protocol for Sexual Activity in Neurorehabilitation: A Patient-Centered Model
In the context of neurogenic sexual dysfunction (NSD), particularly following spinal cord injury or other neurological disorders, restoration of sexual function is a vital, though often under-addressed, component of rehabilitation.
To support patients and their partners during this challenging transition, we have developed a structured Preparation and Feedback Protocol (PFP) designed to enhance clinical outcomes through practical guidance and post-activity analysis.
Psychological Preparation and Partner Communication
Emotional readiness and dyadic understanding are critical prerequisites for successful sexual reintegration. Patients and their partners are encouraged to:
-
Engage in open dialogue about expectations, fears, and changes in function;
-
Normalize anxiety related to first post-injury sexual experiences;
-
Prioritize emotional intimacy and mutual respect over performance-oriented goals.
These preparatory steps are facilitated by clinical staff (usually a neuro-urologist or trained rehabilitation psychologist) using semi-structured discussions and printed guidance materials.
Practical Preparation and Positioning
To ensure physical safety and maximize comfort, patients are advised to rehearse positions and prepare their environment in advance.
Recommendations include testing positions such as:
-
Supine with partner on top (for reduced exertion);
-
Side-lying (for patients with balance impairments).
Additional recommendations include:
-
Use of pillows, bolsters, or adaptive supports to offload pressure from joints and spine;
-
Pre-activity hygiene, especially for those with catheters or stomas (e.g., ensuring bladder emptying and device fixation).
Patients are counseled on muscle tone management, including the use of pre-activity massage or warm baths in cases of spasticity, and on sensory changes, which may include hypoesthesia or allodynia.
Medication and Device Use
Medical support may include:
-
Use of phosphodiesterase-5 inhibitors or intracavernosal agents under physician supervision;
-
Application of water-based lubricants to reduce friction and discomfort, particularly in cases of vaginal dryness;
-
Optional introduction of sexual aids, including vibrators and positioning devices.
These tools are framed not as compensatory but as facilitators of a new, adapted mode of sexual expression.
Environmental and Sensory Modulation
To optimize arousal and emotional engagement, couples are encouraged to:
-
Eliminate clinical cues (e.g., visible medical supplies);
-
Enhance sensory input (e.g., lighting, music, scent, erotic imagery);
-
Stimulate alternative erogenous zones with preserved sensitivity (e.g., neck, chest, inner arms).
Patients are also guided to explore and map residual sensory responses, which may differ significantly from pre-injury patterns.
Feedback Questionnaire: Structure and Clinical Utility
Following the initial attempt at sexual activity, couples complete a structured Feedback Questionnaire.
This tool facilitates clinical assessment of functional outcomes and informs further intervention.
Questions are divided into sections for the patient, partner, and couple together.
Patient Self-Assessment
Adherence to Instructions
-
Were the preparation guidelines followed?
-
Which recommendations were most useful?
-
Which instructions could not be implemented, and why?
Sexual Function
-
Was an erection achieved?
-
Was penetration possible?
-
What was the duration of the erection?
Orgasmic and Ejaculatory Function
-
Was orgasm achieved?
-
Was ejaculation present?
Physical Comfort
-
Were there any spasms, pain, or discomfort?
-
Was the chosen position comfortable?
Sensory and Motor Control
-
Were any genital sensations perceived?
-
Could movement or positioning be controlled?
Fatigue and Physiological Response
-
Was there post-activity fatigue or tension?
-
Any breathing or cardiovascular symptoms?
Emotional Experience
-
Did you feel confident?
-
Were there moments of anxiety or distress?
Perceived Needs
-
What would you change about the experience?
-
What additional tools or support would help?
Partner’s Assessment
Interaction and Comfort
-
Was the position manageable for you?
-
Did you need additional support?
Understanding Partner’s Needs
-
Did you understand your partner’s physical responses?
Emotional Response
-
Did you feel connected and intimate?
-
Were there moments of emotional difficulty?
Adjustment to Limitations
-
Was adapting to the new situation difficult?
-
What changes would ease the experience?
Joint Reflection Process Evaluation
-
What aspects went well?
-
What presented difficulties?
Future Directions
-
Would you like to try alternative positions?
-
Do you feel the need for further consultation?
Emotional and Physical Satisfaction
-
Did you feel satisfied after the experience?
-
Do you expect the next encounter to be more comfortable?
Long-Term Planning
-
Do you have concerns about continued intimacy?
-
What would make future sexual experiences more fulfilling?
Clinical and Scientific Implications
The Preparation and Feedback Protocol represents a novel, patient-centered strategy for the objectification of NSD symptoms outside the clinical setting. By shifting the focus to the couple’s real-life experience and reinforcing adaptive behaviors, this model allows for:
-
Better differentiation between psychogenic and neurogenic components of dysfunction;
-
Personalized adjustment of pharmacologic, rehabilitative, and psychotherapeutic strategies;
-
Active partner involvement in the rehabilitation process, enhancing relational dynamics and adherence.
The feedback questionnaire also provides a standardized data source for monitoring progress, evaluating interventions, and identifying barriers.
Results
All ten participants (aged 23–52) with chronic spinal cord injury and their partners successfully completed the full diagnostic protocol, including the structured feedback component.
Sexual activity was conducted either in a specially designated guest room at the rehabilitation institute or in the participants’ home environment. Each couple submitted the completed feedback questionnaire within 24 hours following the sexual activity.
Among male participants:
-
Five of six reported achieving an erection;
-
Four were able to achieve penetration;
-
Orgasm was reported by two men;
-
Ejaculation occurred in one case.
Among the four female participants:
-
Three reported vaginal dryness;
-
Two experienced discomfort or pain during intercourse.
Spasticity during sexual activity was noted by seven participants, while six reported difficulties with positioning due to increased muscle tone or contractures. Altered or diminished genital sensation was identified in nine of ten participants. Post-activity fatigue was reported in eight cases, and two participants described transient cardiovascular symptoms, including tachycardia and shortness of breath.
All ten couples adhered to at least one of the clinical recommendations provided during preparatory counseling.
-
Six participants used lubricants;
-
Eight utilized pillows or positioning aids;
-
Three male participants received phosphodiesterase type-5 inhibitors.
All partners completed their respective sections of the feedback form. Nine reported that they were able to understand and accommodate the patient’s physical needs during sexual activity. Eight couples engaged in sexual activity at home, while two used the guest room provided at the rehabilitation center.
Environmental modifications—such as adjustments to lighting, incorporation of music, and removal of visible medical equipment—were implemented in seven cases to improve comfort and intimacy.
Discussion
Neurogenic sexual dysfunction (NSD) is a multifactorial condition that significantly impairs quality of life in individuals with spinal cord injury and other neurological disorders. Despite growing recognition of its prevalence and psychosocial impact, sexual rehabilitation remains insufficiently addressed in routine clinical protocols.
The findings of this pilot study underscore the feasibility and clinical relevance of an adapted diagnostic and therapeutic algorithm based on the PLISSIT model, augmented by a structured feedback mechanism implemented during the rehabilitation phase.A key insight from this study is the diagnostic value of evaluating sexual activity in ecologically valid settings.
Traditional clinical assessments often fail to capture the contextual, emotional, and functional nuances of sexual dysfunction in individuals with neurological impairment.
Through structured post-activity feedback questionnaires completed in real-life environments, clinicians were able to identify previously undocumented symptoms such as position-dependent spasticity, sensory-motor mismatch, and autonomic dysregulation.
These findings align with recent literature emphasizing the importance of home-based and patient-reported outcome measures in neurorehabilitation.
Participants’ reports of physical challenges—including erection instability, lubrication difficulties, and positional discomfort—highlight the complexity of NSD, which often involves a combination of primary neurological impairment and secondary biomechanical and psychological factors.
Notably, nine of ten patients reported altered or diminished genital sensation, reinforcing the need for targeted neurosensory assessment during rehabilitation.
The structured educational and preparatory sessions emerged as a cornerstone of patient readiness and engagement. All participants adhered to at least one clinical recommendation, and over 80% reported partial or full implementation of preparatory strategies.
Partner involvement played a pivotal role in emotional and functional outcomes. Feedback from partners revealed significant emotional strain during initial attempts at resuming intimacy, yet also reflected increased dyadic cohesion and mutual understanding.
The feedback instrument itself was perceived not merely as a data collection tool but as a therapeutic mechanism promoting communication and joint reflection.
This dual function suggests that structured self-assessment can serve both evaluative and psychotherapeutic purposes in the rehabilitation process.
Conclusion
Neurogenic sexual dysfunction remains one of the most underaddressed dimensions of rehabilitation following spinal cord injury and other neurological conditions.
The present study introduces a novel, patient-centered approach that adapts the PLISSIT model to the realities of neurorehabilitation practice.
By integrating contextual evaluation, structured feedback, and active partner involvement, this model enables clinicians to capture real-world insights into sexual functioning that cannot be obtained in traditional clinical environments.
The high completion rate of the feedback protocol confirms its feasibility and acceptability among patients and their partners.
Importantly, the feedback instrument not only serves as a clinical assessment tool but also fosters communication, emotional intimacy, and collaborative rehabilitation.
cooperation. In this sense, the model addresses not just functional recovery but also psychosocial reintegration—a critical yet frequently neglected domain in neurological rehabilitation.
Importantly, the algorithm’s structure bridges the gap between biomedical and psychosocial models of sexual health, offering a scalable framework that can be adapted to varying institutional capacities. The reliance on practical counseling, ergonomic adaptation, and patient empowerment allows implementation even in resource-limited settings where specialized sexological services may be unavailable. As such, the model responds to systemic challenges documented in multiple health systems and contributes to the growing call for inclusive, evidence-informed sexual rehabilitation protocols.
Nevertheless, further research is warranted. Future studies should validate the model in larger and more heterogeneous populations, incorporate standardized outcome measures such as the IIEF and FSFI, and evaluate long-term effects on sexual function, relationship satisfaction, and quality of life. The integration of digital health technologies, including telemedicine consultations and mobile app-based feedback collection, may also enhance accessibility and longitudinal monitoring.
In conclusion, the adapted PLISSIT model presented here offers a practical, replicable, and therapeutically valuable framework for addressing NSD within the rehabilitation continuum. By prioritizing patient experience, partner engagement, and ecological validity, it advances a more holistic vision of neurological recovery—one that recognizes sexuality as a core domain of human health and dignity.
References
1. Ramezani M, Ryan F, Sahraian MA, Simani L. The impact of brain lesions on sexual dysfunction in patients with multiple sclerosis: A systematic review of magnetic resonance imaging studies. Multiple Sclerosis and Related Disorders. Published online October 2021:103336. doi:https://doi.org/10.1016/j.msard.2021.103336
2. Shridharani AN, Brant WO. The treatment of erectile dysfunction in patients with neurogenic disease. Translational Andrology and Urology. 2016; 5(1):8801-8101. doi:https://doi.org/10.3978/j.issn.2223-4683.2016.01.07
3. Groen J, Pannek J, Castro Diaz D, et al. Summary of European Association of Urology (EAU) Guidelines on Neuro-Urology. European Urology. 2016;69(2):324-333. doi:https://doi.org/10.1016/j.eururo.2015.07.071
4. Thomas C, Konstantinidis C. Neurogenic Erectile Dysfunction. Where Do We Stand? Medicines. 2021;8(1):3. doi:https://doi.org/10.3390/medicines8010003
5. Guo ZN, He SY, Zhang HL, Wu J, Yang Y. Multiple sclerosis and sexual dysfunction. Asian Journal of Andrology. 2012;14(4):530-535. doi:https://doi.org/10.1038/aja.2011.110
6. Courtois F, Gérard M, Charvier K, Vodušek DB, Amarenco G. Assessment of sexual function in women with neurological disorders: A review. Annals of Physical and Rehabilitation Medicine. 2018;61(4):235-244. doi:https://doi.org/10.1016/j.rehab.2017.04.004
7. Rees PM, Fowler CJ, Maas CP. Sexual function in men and women with neurological disorders. The Lancet. 2007;369(9560):512-525. doi:https://doi.org/10.1016/s0140-6736(07)60238-4
8. New PW, Seddon M, Redpath C, Currie KE, Warren N. Recommendations for spinal rehabilitation professionals regarding sexual education needs and preferences of people with spinal cord dysfunction: a mixed-methods study. Spinal Cord. 2016;54(12): 1203-1209. doi:https://doi.org/10.1038/sc.2016.62
9. Yara Casáis Suárez. CRITICAL REVIEW. THE PLISSIT MODEL: A PROPOSED CONCEPTUAL SCHEME FOR THE BEHAVIORAL TREATMENT OF SEXUAL PROBLEMS. Published May 1, 2022.
https://www.researchgate.net/publication/377335731_CRITICAL_REVIEW_THE_PLISSIT_MODEL_A_PROPOSED_CONCEPTUAL_SCHEME_FOR_THE_BEHAVIORAL_TREATMENT_OF_SEXUAL_PROBLEMS
10. Inoue S. Hormonal and circuit mechanisms controlling female sexual behavior. Frontiers in neural circuits. 2024;18. doi:https://doi.org/10.3389/fncir.2024.1409349
11. Hull EM, Dominguez JM. Neuroendocrine Regulation of Male Sexual Behavior. Comprehensive Physiology. Published online September 19, 2019: 1383-1410. doi:https://doi.org/10.1002/cphy.c180018
12. Jennings KJ, de Lecea L. Neural and Hormonal Control of Sexual Behavior. Endocrinology. 2020; 161(10). doi:https://doi.org/10.1210/endocr/bqaa150
13. Jiang X, Sun M, Chen J, Pan Y. Sex-specific and state-dependent neuromodulation regulates male and female locomotion and sexual behaviors. Research. Published online February 12, 2024. doi:https://doi.org/10.34133/research.0321
14. Thomas HN, Thurston RC. A biopsychosocial approach to women’s sexual function and dysfunction at midlife: A narrative review. Maturitas. 2016;87: 49-60. doi:https://doi.org/10.1016/j.maturitas.2016.02.009
15. Kyu HA, Chotipanvithayakul R, McNeil EB, Thu NL. Cultural taboos and low sexual and reproductive health literacy among university students in Magway city, Myanmar. Culture, Health & Sexuality. Published online November 2, 2024:1-15. doi:https://doi.org/10.1080/13691058.2024.2420704
16. Elliott S, Hocaloski S, Carlson M. A Multidisciplinary Approach to Sexual and Fertility Rehabilitation: The Sexual Rehabilitation Framework. Topics in Spinal Cord Injury Rehabilitation. 2017; 23(1):49-56. doi:https://doi.org/10.1310/sci2301-49
17. Auger LP, Aubertin M, Grondin M, Auger C, Filiatrault J, Rochette A. Assessment methods in sexual rehabilitation after stroke: a scoping review for rehabilitation professionals. Disability and Rehabilitation. Published online March 9, 2021:1-23. doi:https://doi.org/10.1080/09638288.2021.1889047
18. Argiolas A, Argiolas F, Giacomo Argiolas, Maria Rosaria Melis. Erectile Dysfunction: Treatments, Advances and New Therapeutic Strategies. Brain Sciences. 2023;13(5):802-802.
doi:https://doi.org/10.3390/brainsci13050802
19. Hatzichristou D, Rosen RC, Derogatis LR, et al. Recommendations for the clinical evaluation of men and women with sexual dysfunction. The Journal of Sexual Medicine. 2010;7(1 Pt 2):337-348. doi:https://doi.org/10.1111/j.1743-6109.2009.01619.x
20. Kokay W, Power E, McGrath M. A mixed study systematic review and meta-analysis of sexuality and sexual rehabilitation in LGBTQI+ adults living with chronic disease. Archives of Physical Medicine and Rehabilitation. Published online August 2022. doi:https://doi.org/10.1016/j.apmr.2022.07.018
21. Pieters R, Kedde H, Bender J. Training rehabilitation teams in sexual health care: A description and evaluation of a multidisciplinary intervention. Disability and Rehabilitation. 2017; 40(6):732-739. doi:https://doi.org/10.1080/09638288.2016.1271026
22. Cornil CA, de Bournonville C. Dual action of neuro-estrogens in the regulation of male sexual behavior. General and Comparative Endocrinology. 2018;256:57-62. doi:https://doi.org/10.1016/j.ygcen.2017.05.002
23. Sakamoto H, Takanami K, Zuloaga DG, et al. Androgen regulates the sexually dimorphic gastrin-releasing peptide system in the lumbar spinal cord that mediates male sexual function. Endocrinology. 2009;150(8):3672-3679. doi:https://doi.org/10.1210/en.2008-1791
24. Rodriguez-Nieto G, Emmerling F, Dewitte M, Sack AT, Schuhmann T. The Role of Inhibitory Control Mechanisms in the Regulation of Sexual Behavior. Archives of Sexual Behavior. 2019;48(2): 481-494. doi:https://doi.org/10.1007/s10508-018-1283-7
25. Elliott SL. Problems of sexual function after spinal cord injury. Progress in Brain Research. 2006;152:387-399. doi:https://doi.org/10.1016/S0079-6123(05)52026-0
26. Lombardi G, Musco S, Kessler TM, Marzi VL, Lanciotti M, Del Popolo G. Management of sexual dysfunction due to central nervous system disorders: a systematic review. BJU International. 2015;115:47-56. doi:https://doi.org/10.1111/bju.13055
27. Fronek P, Booth S, Kendall M, Miller D, Geraghty T. The Effectiveness of a Sexuality Training Program for the Interdisciplinary Spinal Cord Injury Rehabilitation Team. Sexuality and Disability. 2005; 23(2):51-63. doi:https://doi.org/10.1007/s11195-005-4669-0
28. Taylor B, Davis S. Using the Extended PLISSIT model to address sexual healthcare needs. Nursing Standard. 2006;21(11):35-40. doi:https://doi.org/10.7748/ns2006.11.21.11.35.c6382
29. Mick JM. Sexuality assessment: 10 strategies for improvement. Clinical Journal of Oncology Nursing. 2007;11(5):671-675. doi:https://doi.org/10.1188/07.CJON.671-675
30. Ahn SH, Kim JH. Healthcare Professionals’ Attitudes and Practice of Sexual Health Care: Preliminary Study for Developing Training Program. Frontiers in Public Health. 2020;8. doi:https://doi.org/10.3389/fpubh.2020.559851
31. Tuncer M, Oskay ÜY. Sexual Counseling with the PLISSIT Model: A Systematic Review. Journal of Sex & Marital Therapy. 2021;48(3):1-10. doi:https://doi.org/10.1080/0092623x.2021.1998270
32. Sinković M, Towler L. Sexual Aging: a Systematic Review of Qualitative Research on the Sexuality and Sexual Health of Older Adults. Qualitative Health Research. 2018;29(9):10497323 1881983. doi:https://doi.org/10.1177/1049732318819834
33. Macleod A, McCabe MP. How Well Do Measurement Scales Reflect the Actual Experience of Sexuality in Mid-Life and Beyond? Sexual Medicine Reviews. 2019;7(1):29-45. doi:https://doi.org/10.1016/j.sxmr.2018.04.004
34. Courtois F, Alexander M, McLain AB (Jackson). Women’s Sexual Health and Reproductive Function After SCI. Topics in Spinal Cord Injury Rehabilitation. 2017;23(1):20-30. doi:https://doi.org/10.1310/sci2301-20
35. Del Popolo G, Cito G, Gemma L, Natali A. Neurogenic Sexual Dysfunction Treatment: A Systematic Review. European Urology Focus. Published online December 2019. doi:https://doi.org/10.1016/j.euf.2019.12.002
36. Denys P, Chartier-Kastler E, Even A, Joussain C. How to treat neurogenic bladder and sexual dysfunction after spinal cord lesion. Revue Neurologique. 2021;177(5):589-593. doi:https://doi.org/10.1016/j.neurol.2020.07.013
37. Benevento BT, Sipski ML. Neurogenic bladder, neurogenic bowel, and sexual dysfunction in people with spinal cord injury. Physical therapy. 2002;82(6):601-612. https://pubmed.ncbi.nlm.nih.gov/12036401/