






NGOs’ Role in COVID-19 Response in Rural Mozambique
The Importance of Non-Governmental Organizations in Response to the Corona Virus Pandemic in Rural Mozambique: A Case Study
Angelea Panos¹, Patrick T. Panos²*
- Social & Behavioral Sciences, Utah Valley University, Orem, Utah, USA
- College of Social Work, University of Utah, Salt Lake City, Utah, USA
OPEN ACCESS
PUBLISHED 31 October 2024
CITATION Panos, A., Panos, PT., 2024. The Importance of Non-Governmental Organizations in Response to the Corona Virus Pandemic in Rural Mozambique: A Case Study. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5910
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5910
ISSN 2375-1924
ABSTRACT
Introduction/Importance: In response to the overwhelming public health demands of the COVID-19 pandemic, many communities were not served due to the shortage of medical supplies and access to healthcare, particularly in developing countries. Consequently, the World Health Organization (WHO) began an initiative to engage the “untapped resources” of Civil Society Organizations (CSOs) /Non-Governmental Organizations (NGOs) working within various developing and underserved countries. In order to better prepare for future public health emergencies, it is critical to assess the experiences of CSOs/NGOs in responding to the COVID-19 pandemic in partnership with marginalized communities.
Objectives of Study: The primary research objectives of this study were (1) Document the challenges that the frontline NGO/community partnerships faced in responding to rural villages’ needs associated with COVID-19 within Mozambique, (2) Document the frontline NGO/ community partnership responses in addressing rural villages’ needs associated with COVID-19 in rural Mozambique.
Background: This case study examines the NGO Care-for-Life (CFL) within its partnership with rural villages in Mozambique in response to COVID-19. Care-for-Life is one of the few formally recognized NGOs in Mozambique that takes a holistic approach to community development in rural villages.
Methods: Data for this study was collected using qualitative methods, including in-depth interviews (26), focus group discussions (5), household surveys, and non-participation observation.
Results: Based on household surveys, villages with the CFL/community partnership experienced an approximate 4% increase in overall deaths during the pandemic, while surrounding villages without an NGO/ community partnership experienced an approximate 15% increase in overall deaths. The general findings strongly suggest that NGO/CSO community partnerships can have a significant impact on a community’s ability to respond to a public health emergency.
Conclusions: The results of this case study suggest that the use of CSOs/NGOs during a crisis can enhance public health responses in emergencies such as pandemics.
Keywords: Africa, Mozambique, COVID-19, public health, rural communities, case study.
Introduction
Since the emergence of the Coronavirus (COVID-19) pandemic beginning in 2019, there have been approximately 775 million cases worldwide¹, resulting in over 7 million deaths². Unfortunately, due to differences in healthcare resources and economic development, there were significant disparities in how countries could detect, assess, report, and respond to the pandemic³. While Africa had a lower overall prevalence rate of Covid compared to other regions of the world¹, the pandemic demonstrated the structural weaknesses that interfered with the continent’s public health systems’ abilities to respond due to their dependence on the outside world for its healthcare commodities such as vaccines, personal protective equipment, and other medical supplies. As Happi and Nkengasong stated, “The COVID-19 pandemic has exposed how easily international cooperation and multilateral agreements can dissolve, especially in the face of a global crisis — and just how vulnerable this dependence leaves Africa”⁵(p.22). As the UN Sustainable Development Group asserted, “the magnitude of the challenge and the continent’s underlying vulnerabilities cannot be underplayed”⁶(p.10). Specifically, they noted the unique challenges faced by Africa, including food insecurity, a lack of medical supplies, a loss of income and livelihood, difficulties in applying sanitary and physical distancing measures, a looming debt crisis, as well as related political and security risks.
At the beginning of the pandemic, the country of Mozambique faced many of the same problems as the rest of Africa with its public health challenges. For example, in 2020, Mozambique was one of the world’s poorest countries⁷, and was ranked tenth worldwide in infant mortality, thirty-ninth in maternal mortality, and the bottom four worldwide in life expectancy at birth⁸. Furthermore, approximately two-thirds of its population lived and worked in rural, undeveloped areas of the country⁸,⁹. Therefore, most of the population had limited access to healthcare due to a shortage of medical personnel and a limited medical infrastructure for distributing medications to its dispersed population¹⁰.
Adding to these difficulties, in the year before the first reported case of COVID-19 in 2020, Mozambique experienced two weather-related disasters that decimated many of the clinics and healthcare facilities¹¹,¹². First, on March 14, 2019, Tropical Cyclone Idai, a Category 4 storm, struck Mozambique near the city of Beira. This was immediately followed by Tropical Cyclone Kenneth, another Category 4 storm, that hit the same area on April 25, 2019. The UN described these two storms as “one of the worst weather-related disasters ever to hit the southern hemisphere”¹³(¶12). As a result of these two storms, seven surgical rooms and the emergency room at the Beira Central Hospital were rendered non-functional, and a total of 94 medical facilities across Mozambique were destroyed¹⁴,¹⁵. Additionally, rains making the area an “inland sea” that further destroyed transportation and infrastructure throughout the region¹⁷. Consequently, the city of Beira and its surrounding villages across the province, isolated from healthcare facilities and supplies, were ill-prepared to address the global health crisis that they would next face.
After the World Health Organization (WHO) declared the COVID-19 pandemic an international public health emergency in January 2020, it began its response by engaging with the Ministry of Health (MoH), international partner organizations, and global health institutions. Subsequently, due to the response demands of the pandemic, it was realized that many communities were not being served as a result of shortages in medical supplies and limited access to healthcare, particularly in developing countries. Consequently, the WHO began an initiative to engage the “untapped resources” of Civil Society Organizations (CSOs) working within various developing and underserved countries¹⁸,¹⁹. A CSO is a non-profit, voluntary group of citizens that works to improve
society on a local, national, or international level. Civil Society Organizations (CSOs) can be non-governmental organizations (NGOs), civic organizations, cooperatives, social movements, professional groups, or business groups²⁰. The WHO¹⁸(p¹) described this effort as follows:
In 2020-2021, with the support of the COVID-19 Solidarity Response Fund, the World Health Organization (WHO) provided direct financial and technical support to 54 grassroots civil society organizations (SCOs) in 40 countries, serving over 80 million people in situations of vulnerability, including migrants, refugees, internally displaced persons, persons with disabilities, older persons, youth groups, women and children in distress, hard-to-reach Indigenous communities, hidden social and ethnic minorities, informal workers and front-line care providers.
Connecting communities to services and fostering participatory governance, the CSO Empowerment Initiative sought to mitigate the impact of the COVID-19 pandemic on the most vulnerable… Guided by the commitment to the 3Es (enable, empower, engage), the Initiative called on partners to create an enabling environment for empowering communities with a strong voice to engage in decision-making and shared accountability for building resilience to emergencies beyond COVID-19.
In order to better prepare for future public health emergencies, it is critical to assess the experiences of CSOs/NGOs in responding to the COVID-19 pandemic. Therefore, the purpose of this case study is to determine the experiences of the frontline community development NGO, known as Care for Life, in addressing COVID-19 within rural Mozambican villages as part of the government’s solidary response as recommended by the WHO¹⁸,¹⁹.
Objectives of Study
The primary research objectives of this study were as follows:
-
Document the challenges that the frontline NGO/community partnership faced in responding to rural villages’ needs associated with COVID-19 within Mozambique.
-
Document the frontline NGO/community partnership responses in addressing rural villages’ needs associated with COVID-19 in rural Mozambique.
Background
CARE-FOR-LIFE
Care-for-Life (CFL) is one of the few formally recognized NGOs in Mozambique that takes a holistic approach to community development in rural villages. The agency and its program have been more fully described in professional journals elsewhere regarding its impact on maternal and infant mortality in these villages, as well as community empowerment²¹,²². To assist the reader to more fully understand the program and its impact on a community’s ability to deal with a public health emergency, a brief summary of the organization’s approach to community development is provided below.
FAMILY PRESERVATION PROGRAM
Care-for-Life (CFL) uses a holistic approach, known as the Family Preservation Program (FPP), to intervene with individual families living within marginalized, rural villages in Mozambique. Typically, these villages contain 200 to 300 families in size (or approximately 1000 individuals). The FPP consists of providing comprehensive education and mentorship to teach skills that empower the community to address their own needs, and they do not give food, jobs, or handouts of any kind. A main focus of the FPP is the election and training of community leadership to ensure the community develops its own leadership and skills needed eventually to work independently of CFL. The framework for providing the village with needed leadership and skills is achieved first by dividing the community into eight zones (consisting of approximately 25 to 30 families each) and then organizing them into two groups, with the community electing group leaders within each zone. Next, CFL assists these zone leaders in selecting community members from within their zone to act as promoters, concentrating on eight areas of focus: Health, Education, Psycho-Social Well-being, Income Generation, Agriculture, and Home Improvement. As a result, CFL helps to establish what is known as the Zone Support Group, consisting of eight community volunteer leaders (2 group leaders and 6 promoters). Consequently, at the community level, a leadership framework known as the Community Support Group is established consisting of a total of 64 community leaders who are trained and mentored to work with the rest of the community (see Figure One).
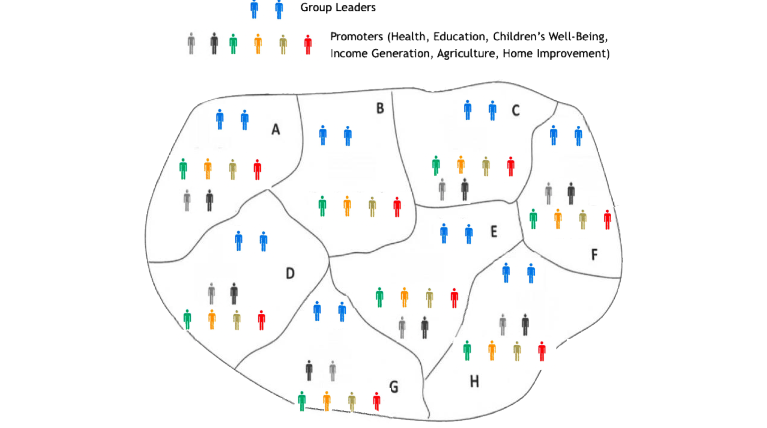
Figure 1. Care-for-Life Community Leadership Organization²³
Throughout the process, it is made clear that all community leaders are volunteers working for their community and will not receive any remuneration from CFL. These community leaders are then provided four two-hour training sessions regarding how to use the FPP in working with families in their zones and how to support the overall development of their communities. Subsequently, these community leaders participate in a one-hour Community Leadership Meeting every two weeks, where CFL field officers provide further leadership training and direct mentorship, as well as discuss individual families within their village. Furthermore, after the community leadership meeting, CFL field officers accompany group leaders to visit each family in the village within their homes. Additionally, the Zone Support Group (i.e., two group leaders and the six promoters) will also meet with each individual family on their own in the alternate weeks. The goal is to train and support local leadership to develop community cooperation and improvements.
During the meetings with the CFL field officers and Zone Support Group, each family selects ten goals that meet their own objectives from the eight areas of emphasis. The Zone Support Group members are responsible for monitoring each of their families’ progress towards these goals, providing appropriate support, and reinforcing concepts and skills that are taught in community classes. Through this process, communication is established between community members and its leadership while providing support to every individual family. Furthermore, each week zone leaders encourage, track, and document family members’ participation in FPP community activities, classes, and programs.
COMMUNITY ACTIVITIES, EDUCATION, & PROGRAMS
Providing age-appropriate knowledge and skills through community classes, followed by community-wide initiatives to implement these newly taught skills, is a major focus of the FPP. As mentioned
above, the FPP consists of eight areas of community development emphasis²³:
-
Community Participation and Leadership Development
-
Education
-
Health & Hygiene
-
Food Security & Development
-
Sanitation
-
Income Generation
-
Home Improvement
-
Psycho-social well-being
Family Preservation Program (FPP) classes consist of 31 individual lessons that cover different aspects of the eight areas of emphasis. In addition to teaching knowledge and skills, each lesson contains specific key behavioral change objectives. For instance, one community health class teaches the importance of proper sanitation, followed by basic instructions for building a simple, properly functioning latrine. Consequently, during their weekly visits, community leaders will encourage each family to actually construct a simple latrine for their household, using the proper techniques learned in the community class. Additionally, the community leaders can support families in carrying out the construction by helping them problem-solve challenges and coordinate cooperation with neighboring families. Overall, CFL works with the village using the FPP for approximately two years to solidify and maintain improvements, before exiting the village.
STUDY SETTING
This study occurred in five villages surrounding Mozambique’s fourth-largest city of Beira where the two typhoons had struck (see Figure Two). Nazaré, a village near Beira in one of Mozambique’s poorest regions, was part of a five-year randomized study (2012–2017) evaluating the Care-for-Life (CFL) Family Preservation Program (FPP). The study aimed to assess the program’s impact on reducing infant mortality ratios (IMRs) and maternal mortality ratios (MMRs). Initially, both intervention and comparison villages had similar IMR and MMR levels. By the study’s end in 2017, the intervention villages, including Nazaré, showed significantly lower IMRs (2.3 times lower) and MMRs (4.6 times lower) than the comparison villages. The CFL program’s holistic approach was found to effectively support community development and health outcomes. CFL continued to monitor the community to determine the sustainability of the improvements observed within Nazaré. Therefore, shortly after the cyclones had struck the area, follow-up data was collected to determine how the village of Nazaré responded to the natural disasters. Mixed methods data was collected over a nine-month period (beginning three weeks post-cyclones in November of 2019) to measure the community’s resiliency to disaster. Quantitative results demonstrated that the village of Nazaré responded effectively to the weather-related disaster by decreasing disease, increasing sanitation, and improving food security, skill continuity, and community norms. More specifically, the study demonstrated that the leadership established by CFL program leaders positively influenced community empowerment and resiliency in responding to disasters²².

Figure 2. Map of Study Location
Adapted from Mapsopensource.com, Creative Commons (CC) Attribution by 3.2⁴
Methods
DATA COLLECTION
This study builds upon and extends the 2020 Nazaré follow-up study,²² as described above, that examined the community’s response to the COVID-19 pandemic. Therefore, the original data was initially collected in July and August of 2020, with the four-year follow-up completed in August of 2024 to include four additional villages being serviced by CFL (for a total of five villages). Additionally, brief assessments of neighboring villages, not assisted by CFL, were conducted to allow for comparison purposes. Data for this study was collected using qualitative methods, including in-depth interviews (26), focus group discussions (5), household surveys, and non-participation observation. Due to the social disruption and limited access that occurred in rural Mozambique because of concerns about COVID-19 and difficulties caused by the cyclones, study participants were purposively selected (key informant or maximal diversity sampling), including community leadership, study staff, community members, and local governmental authorities. (see Table One for demographic characteristics of participants).
Table 1. Demographic Characteristics of Qualitative Study Participants
| Age (Years) | Female | Male | % |
|---|---|---|---|
| 19–35 | 13 | 7 | 34.5% |
| 35–45 | 19 | 12 | 53.4% |
| 41–51 | 3 | 4 | 12.1% |
| Total (N=58) | 35 | 23 | 100% |
For this study, a semi-structured guide further covered relevant contextual and qualitative data analysis, with one theme focusing in particular on challenges and responses to COVID-19. The semi-structured guides were designed to encourage a narrative account of participants’ experiences over time throughout the public health emergency. The data collection tools were piloted, and — as is typical for qualitative research — revisions made during data collection to allow a focus on emerging issues. Interviews and discussions were transcribed, translated, and analyzed using framework analysis, combining data- and theory-driven perspectives. Due to the lack of electricity, all data from individual and focus group interviews were transcribed by hand as close to verbatim as possible, and then translated into English by experienced translators. The researchers for whom the translations were given also took verbatim notes. Subsequently, the Portuguese transcripts were translated into English and backed to Portuguese to check for accuracy. Then, appropriate edits were made to the finalized English transcripts. Note-takers present during interviews contributed throughout all stages of analysis.
In the initial part of the study (beginning in November of 2019 and August of 2020), volunteer study students used to survey all households within the village, as well as to make non-participatory observations of the village. The surveys and observations were comprehensive, in that all households (n = 285) with people still living in the village were visited. This data was used to measure the change that occurred in the village over a nine-month period in response to the cyclones. The four-year follow-up study in 2024 followed the same process to gather additional qualitative data focused on COVID-19 experiences, and it included four additional CFL-assisted villages, as well as neighboring villages (not assisted by CFL) to allow for comparisons.
ETHICAL CONSIDERATIONS
Participants were read verbatim statements that clearly stated that their sharing of data was voluntary and that there was no consequence for refusal to participate at any point during the survey. It was also made clear that no incentive was to be given for participation in the survey. Responding to the survey questions was considered to be the granting of permission for the participants’ data to be used.
Given that no interventions were being given as part of this study, and the study only consisted of voluntary interviews and surveys, the University of Utah’s Institutional Review Board (IRB) granted “Exempt” status to the project.
Results
The goal of conducting the qualitative interviews and focus groups was to determine the challenges faced by rural Mozambican communities to the COVID-19 pandemic, and the effectiveness of CSOs, like CFL, in mitigating the impact of COVID-19 following WHO recommendations¹⁸. Several themes emerged around which the reporting of results is organized.
CFL AND MOZAMBICAN GOVERNMENT’S SOLIDARY RESPONSE
As described above, Mozambique had a fragile health system, socioeconomic vulnerabilities, infrastructural limitations, and limited capacity for distributing medical supplies prior to the pandemic¹⁰. Since the early days of the pandemic, there was a shortage in medical supplies and personal protective equipment (PPE) as global supply chains shut down²⁵. On March 22, 2020, Mozambique reported its first case of COVID-19²⁶. One week later, with the support of the Mozambique parliament, President Felipe Nyusi declared a COVID-19 state of emergency²⁷. With 95% of COVID-19 cases occurring in urban areas, the country’s public health interventions were focused on its population centers²⁸. Consequently, by default, CSOs and NGOs were forced to fill the gaps in responding to COVID-19 in the rural parts of Mozambique. Although no formal agreements were made with these organizations, informal support was provided in the form of providing accurate pandemic information as it became available, as well as educational supplies. Informational workshops were consistently provided throughout the pandemic to deliver accurate medical information and recommendations to vulnerable communities, which was considered critically important to stopping the spread of the disease²⁹.
Although little could be given regarding concrete resources, an almost universal response voiced by agency staff was of appreciation for the information that was provided. As one participant stated, “There were no resources to give but the information they gave us could be passed onto the communities. Everyone was scared, so we were grateful to learn what we could do to protect ourselves.”
COMMUNITY PARTICIPATION AND LEADERSHIP
During the pandemic, many public health measures made it difficult to provide information to isolated and distant communities throughout Mozambique. As part of the State of Emergency, the government actions included the closing of the country’s borders, closing schools, stopping cultural events such as religious acts/festivities, and ceasing all sporting events³⁰. In particular, social distancing requirements and the closure of public transportation made it difficult for the limited number of public health workers to reach the rural parts of the country. Consequently, CSOs and NGOs became the main conduit for transmitting information to relatively isolated areas, since these agencies typically had the established relationships and procedures needed to efficiently work and communicate with isolated communities.
In the case of CFL, it had pre-established community leadership and organization that could be adapted to the public health restrictions of the pandemic regarding social distancing and transportation. Adapting the established organization within the villages was critical since personal protective clothing (PPC), face masks, and hand sanitizers were unavailable during the beginning of the pandemic. Agency staff gave an extensive list of the challenges that they faced.
Without public transportation, workers were required to use the few agency vehicles to reach the villages. Due to social distancing requirements within the vehicles, however, the number of staff that could be transported was limited. Therefore, to allow staff to maintain employment, they took turns and rotated days in which they would work.
Additionally, staff time in the villages was decreased as travel time increased due to needing to meet staff at different pickup points near their homes, and the need for staff to decontaminate at the end of the day (e.g., showering and changing clothes). Due to time constraints, staff needed to be extremely efficient with their time and efforts within the community. As one CFL staff member stated, “Each step of the way, we had to think through things and problem-solve everything. We needed to decide what we needed to do and then how we would do it.”
Care-for-Life (CFL) staff indicated that the leadership organizational structure was invaluable in responding to the needs of the village, although several modifications were required. Previous to the pandemic, CFL would provide training and workshops at the village level with follow-up support sessions given by zone leadership. Due to public health restrictions, however, workshops and classes could no longer be held in the larger community settings with whole families attending, with training of families occurring through zone leadership. Through this method, every family in the village was contacted and given public health instruction. As an unanticipated result, CFL discovered that working with the smaller groups was a more effective method of teaching within the village. As one staff member described it, “When we moved things down to the zone level, our trainings were better attended and with more participation and discussion. Also, families tended to better apply what we taught them.” As a result, the decision was made to incorporate this approach as a long-term change to their program, with all education and training now being done at the zone level despite the end of the pandemic. As one staff member said, “The closer you are to families and people, the more effective you can be.”
During these group and individual outreach efforts, CFL staff were able to share government information and pamphlets (See Figure Three). Much information focused on the need for social distancing, mask washing, handwashing, or the need to avoid greetings consisting of handshaking. This directed teaching of public health knowledge allowed community leaders to respond more effectively to the disease.
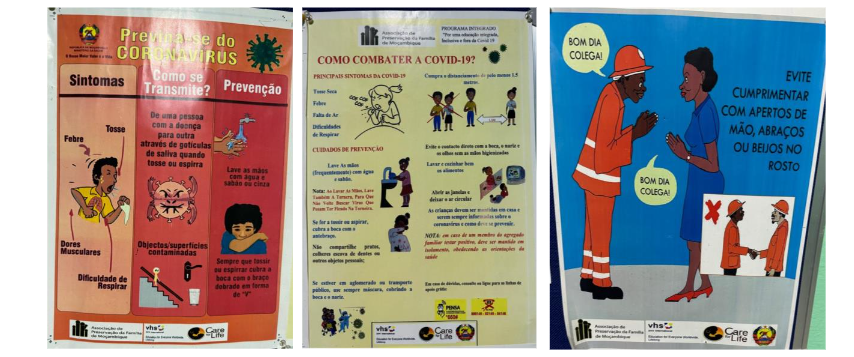
Figure 3. Public Health Posters
HEALTHCARE TREATMENT
As the pandemic progressed in Mozambique, the ability of rural inhabitants to access needed healthcare was almost nonexistent. More than half of all Mozambicans required more than an hour or more walk to reach the nearest healthcare facility where medical supplies and medications were of short supply, and where there was a lack of trained medical personnel (e.g., there were only three doctors per 100,000 people)³¹. Consequently, most of the limited available medical resources were provided only to “those who could pay,” resulting in the majority of the rural population not having access to any type of healthcare³².
A local leader stated, “We had to figure out how to help people on our own.”
In discussing healthcare challenges with local leaders, it was clear that the leadership structures within the village were a critical component of the village’s responses. For example, when a person became sick, zone leaders coordinated the delivery of food so that the person or family could remain quarantined and not spread the disease. In another example, one leader related how when a person began having difficulty breathing, a tub was provided so the family could place them into a hot bath so that they could breathe in the steam. Each step of the way, the established leadership structure allowed for a more effective and coordinated response to the pandemic.
An area of frustration expressed by local leaders was the lack of access to vaccinations. Initially, the prioritization of cities and the need for refrigeration prevented access to vaccinations by the rural and marginalized communities throughout Mozambique. Furthermore, when vaccinations did become available more broadly, they were initially restricted to the elderly. Finally, frustration was expressed that when the vaccine was given, a person was only given the first shot of the two-part injection series. On the other hand, CFL staff expressed appreciation that they were relatively high on the prioritization list for vaccination since they were seen as frontline workers.
HEALTHCARE & SANITATION SUPPLIES
As mentioned above, PPC, masks, and hand sanitizers were unavailable in most of the country, let alone in rural areas. Although social distancing was practiced, there were many situations in which masks were advisable. Once again, the NGO/village partnership allowed for innovation and problem-solving. When asked how they responded to this shortage, local leaders stated that because CFL had transportation availability, the NGO was able to locate and purchase fabric for the village, along with patterns for masks from the internet. Community leadership was then able to organize the production of masks for the village (see Figure 4). Unsurprisingly, villages surrounding the CFL villages were unable to obtain materials. Furthermore, as the CFL villages’ needs were met, a small cottage industry of mask production was started to supply surrounding villages.

Figure 4. Production of Homemade Masks
During the interviews, the lack of hand sanitizers was identified as a major problem that needed to be addressed. Based upon information provided to them by CFL, the community leadership recognized the need for consistent handwashing using uncontaminated water. Due to the often- centralized village water sources, a need to develop a touchless handwashing system that could be dispersed throughout the villages was recognized. Figure Five shows the innovative solution developed by community leadership, and soap was subsequently bartered for by the villages.
This innovation was developed with other NGOs, including Save the Children, to assist the communities they were serving. A survey of surrounding villages without NGO partnerships failed to innovate or adopt this solution.

Figure 5. Touchless Handwashing System
FOOD SECURITY & ECONOMICS
As a result of the State of Emergency, the pandemic had a dramatic effect on the Mozambican economy.³⁴ Laws enforcing social distancing closed stalls in markets and dramatically affected the need for day laborers. Basic food staples such as rice and cornmeal became unavailable³⁵. Consequently, the economic security of the rural communities was dramatically impacted³⁶. As one person stated, “We had no jobs. We could not sell in the marketplace. All we could do was die of hunger.” During interviews, it was commonly expressed that the NGO staff and community zone leadership played a critical role in organizing a collective response to an economic emergency. Care-for-Life (CFL) staff bartered for limited amounts of seeds and community zone leaders organized community gardens. Furthermore, community elders revived traditional farming methods that required fewer external inputs, and the resulting harvest was distributed throughout the village. Finally, interviewees described small cottage economies being established in the communities.
PSYCHO-SOCIAL WELL-BEING
As illustrated throughout this paper, a significant theme that was repeatedly expressed described how neighbors and extended families assisted those in need by sharing food, resources, and labor within the villages. Community-based organizations and local leaders were repeatedly reported to have had a pivotal role in coordinating these efforts, ensuring that vulnerable households, such as those with elderly or sick family members, received the necessary support. In surveying surrounding villages, this level of community cohesiveness and mutual support was not reported.
IMPACT
Due to limited COVID-19 testing and inadequate record-keeping in the rural villages of Mozambique, the precise prevalence and mortality rates due to the disease can only be estimated. Based on household surveys, villages with the CFL/community partnership experienced an approximate 4% increase in overall deaths during the pandemic, while surrounding villages without an NGO/community partnership experienced an
approximate 15% increase in overall deaths. While these are only estimates based upon likely imprecise data, the general findings strongly suggest that NGO/CSO/community partnership can have a significant impact on a community’s ability to respond to a public health emergency.
Limitations and Recommendations
Overall, the results of this study should be considered with caution due to the limitations associated with all case studies. Specifically, this study was conducted within a specific setting, involving somewhat unique communities and agencies, occurring within a historically exceptional situation and time period. Therefore, generalizing these findings to other settings and situations should be done with caution. Additionally, given the limited selection of participants, the possibility of bias cannot be overlooked. Finally, the need for caution is intensified by the imprecise nature of the gathered data.
Despite these limitations, there are several recommendations that can be made based on the results. First, there was a clear improvement in a community’s ability to respond to a public health crisis when CSO/NGO/community partnerships are leveraged. This is particularly true in communities where CSOs/NGOs have developed relationships and have developed community leadership structures. Consequently, in preparing for future global pandemics, a need to include such partnerships in the framework of an emergency plan is critical. Specifically, sufficient reserves of public health basics such as PPE, masks, and hand sanitizers should be in sufficient quantities needed to provide CSOs/NGOs with protection in providing a frontline response. Additionally, future plans should look beyond having WHO “solidarity response” partnerships used simply as a method of providing communities with information. Rather, planning should examine how public health officials and programs can support the partnerships’ innovation and problem-solving in responding to an overwhelming public health emergency. Finally, more research examining solidarity response partnerships within globally diverse marginalized communities should be further examined to understand how to maximize their effectiveness across cultures and settings.
Conclusion
The results of this case study suggest that the use of CSOs/NGOs during a crisis can enhance public health responses in emergencies such as pandemics. Using established trusted relationships with local communities and their leaders, the CSOs/NGOs can provide accurate information, distribute essential supplies, and assist in outreach to marginalized and vulnerable communities and their members. Recognizing these CSOs/NGOs as an important resource during public health emergencies can lead to better preparation, coordination, and training in advance of crises and future pandemics.
Conflict of Interest Disclosure:
We have no known conflicts of interest to disclose.
Funding/Support:
No external funding was obtained or used for this research study.
Acknowledgements:
None.
Author Note
The authors wish to acknowledge the administrators and staff of Care-for-Life who provided the logistical support needed to conduct these evaluations. The authors also wish to acknowledge the inspiring efforts of the Mozambican communities and their willingness to share their stories.
References
1. World Health Organization. WHO COVID-19 dashboard| Cases. 2024. Updated August 4, 2024. Accessed August 19, 2024. https://data.who.int/dashboards/covid19/cases?n=o
2. World Health Organization. WHO COVID-19 dashboard| Cases. 2024. Updated August 4, 2024. Accessed August 19, 2024. https://data.who.int/dashboards/covid19/deaths?n=o
3. Judson SD, Torimiro J, Pigott DM, et al. COVID-19 data reporting systems in Africa reveal insights for future pandemics. Epidemiology and Infection. 2022;150:e119. doi:10.1017/S0950268822001054
5. Happi CT, Nkengasong, JN. Two years of COVID-19 in Africa: Lessons for the world. Nature, 2020; 601, 22-25. Published online January 2, 2022. https://www.nature.com/articles/d41586-021-03821-8
6. UN Sustainable Development Group. (2020, May 20). Policy Brief: Impact of COVID-19 in Africa. UN Sustainable Development Group; May 2020. Accessed August 19, 2024 from: https://unsdg.un.org/resources/policy-brief-impact-covid-19-africa
7. Heritage Foundation. 2021 Index of economic freedom|Mozambique. Accessed August 15, 2021 from https://www.heritage.org/index/country/mozambique
8. The CIA World Factbook. Mozambique. Updated August 7, 2024. Accessed August 16, 2021 from https://www.cia.gov/the-world-factbook/countries/mozambique/
9. World Bank. The World Bank in Mozambique. Accessed August 15, 2021 from https://www.worldbank.org/en/country/mozambique/overview
10. World Health Organization-Africa. Health topics (Mozambique)| Essential medicines. Accessed August 16, 2024 from https://www.afro.who.int/countries/mozambique/topic/health-topics-mozambique
11. Isbell T, Bhoojedhur, S. (2019, May 7). Cyclones add to Mozambique’s public health challenge. Afrobarometer Dispatch. May 7, 2019; No. 297. Accessed August 20, 2024 from https://www.researchgate.net/publication/332935718_Cyclones_add_to_Mozambique%27s_public_health_challenges
12. World Health Organization-Africa. Restoring essential health services after Cyclone Idai in Mozambique. Published July 5, 2019. Accessed August 23, 2024 from https://www.afro.who.int/news/restoring-essential-health-services-after-cyclone-idai-mozambique
13. Rodgers L, Fletcher G., Bryson M. Cyclone Idai: how the storm tore into Southern Africa. BBC.com. Published March 22, 2019, Access August 23, 2024 from https://www.bbc.com/news/world-africa-47638696
14. United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA). Southern Africa: Tropical Cyclone Kenneth, flash Update No. 2. April 25, 2019. Accessed August 23, 2024 from https://reliefweb.int/sites/reliefweb.int/files/resources/ROSEA_20190425_SouthernAfrica_TCKenneth_FlashUpdate_final%20draft.pdf
15. World Health Organization-Africa. As post-cyclone resettlement begins, 200000 people lack access to health services in Mozambique. June 21, 20219. Accessed August 24, 2024 from https://www.afro.who.int/news/post-cyclone-resettlement-begins-200-000-people-lack-access-health-services-mozambique
16. World Bank Photo Collection. (2019, May 19). The Beira Central Hospital whose roof was destroyed during Cyclone Idai. May 19, 2019. Accessed August 24, 2024 from https://www.flickr.com/photos/worldbank/40793489423
17. Brackett, R, Wright, P. In Mozambique, torrential rain keeps food, other aid from reaching Cyclone Kenneth victims. The Weather Channel. April 30, 2019. Accessed August 20, 2024 from https://weather.com/news/news/2019-04-25-tropical-cyclone-kenneth-mozambique?cm_ven=PS_GGL_DSA_09162019_1%26par%3DMK_GGL%26gclid%3DCjwKCAjw4KyJBhAbEiwAaAQbE28mPYeWDre-UTw9s7GUBvpuXssE0SFdN93Cqlip-LJ55te3UXnU5xoCi-UQAvD_BwE
18. World Health Organization. Community assets and civil society outreach in critical times: an initiative to engage civil society organizations in the COVID-19 response. World Health Organization, 2022. https://www.google.com/books/edition/_/vHoOEQAAQBAJ?hl=en&gbpv=1&pg=PP1
19. Baldé T, Billaud A, Beadling CW, Kartoglu N, Anoko JN, Okeibunor JC. The WHO African Region Initiative on Engaging Civil Society Organizations in Responding to the COVID-19 Pandemic: Best Practices and Lessons Learned for a More Effective Engagement of Communities in Responding to Public Health Emergencies. Disaster Med Public Health Prep. 2023 Aug 8;17:e445. doi: 10.1017/dmp.2023.99. PMID: 37551088.
20. UN Development Programme. UNDP and civil society. 2024. Accessed August 20, 2024 from https://www.undp.org/partners/civil-society-organizations
21. Panos A, Panos P, Gerritsen-McKane R, Tendai T. The Care for Life Family Preservation Program: Outcome evaluation of a holistic community development program in Mozambique. Research on Social Work Practice, 2020; 30(1): 84-96. Published May 1, 2019. https://doi.org/10.1177/1049731519844324
22. Panos, P, Panos, A. Aftermath of Covid and Cyclones Idai and Kenneth: A naturalistic experiment examining empowerment and resiliency in rural Mozambique. Research on Social Work Practice, 2020; 3(5: 544-561. Published August 24, 2022. https://doi.org/10.1177/10497315221117547
23. Care-for-Life. Guide to the Family-Preservation-Program. Care-for-Life. 2012.
24. Mapsopensource.com. Accessed August 22, 2021 from http://mapsopensource.com/mozambique-map.html. (Creative Commons (CC) Attribution by 3)
25. Gereffi G. What does the COVID-19 pandemic teach us about global value chains? The case of medical supplies. J of Inter Bus Policy. 2020;3(3 ):287-301. doi:10.1057/s42214-020-00062-w
26. World Health Organization- Africa. World Health Organization: A case of COVID-19 confirmed in Mozambique. Published March 23, 2020. Accessed September 1, 2024, from https://www.afro.who.int/news/world-health-organization-case-covid-19-confirmed-mozambique
27. Esau I. (2020, April 1). Parliament approves state of emergency in Mozambique amid Covid-19 fears. Upstream. Published April 1, 2020. Accessed August 29, 2024 from https://www.upstreamonline.com/coronavirus/parliament-approves-state-of-emergency-in-mozambique-amid-covid-19-fears/2-1-786033?message=[nuxt]+instance+unavailable&stack&statusCode=404&statusMessage=[nuxt]+instance+unavailable&url=/coronavirus/parliament-approves-state-of-emergency-in-mozambique-amid-covid-19-fears/2-1-786033
28. UN-Habitat. Assessment of vulnerability and response to COVID-19 in the Municipalities of Mozambique. 2021. Accessed September 1, 2024 from https://unhabitat.org/assessment-of-vulnerability-and-response-to-covid-19-in-the-municipalities-of-mozambique
29. James S. How we’re working with Civil Society in Mozambique to slow and stop the transmission of Coronavirus. Aga Khan Foundation. April 17, 2020. Accessed September 3, 2024 from https://www.akf.org.uk/how-were-working-with-civil-society-in-mozambique-to-slow-and-stop-the-transmission-of-coronavirus/
30. Prista A. Efficacy of government laws to contain SARS-CoV-2 spread in Mozambique. J Public Health Afr. 2023;14(3):2218. Published 2023 Apr 20. doi:10.4081/jphia.2023.2218.
31. USAID. Mozambique| Global Health. Accessed September 3, 2024 from https://www.usaid.gov/mozambique/global-health
32. Jimenez MA, Daniel E. Mozambique’s response to COVID-19: Challenges and questions. IGC Blog. Published May 5, 2020. Accessed September 3, 2024 from https://www.theigc.org/blogs/covid-19/mozambiques-response-covid-19-challenges-and-questions
33. Amentie M, Morka A, Senbeta M, et al. Indigenous Knowledge of Medicine for COVID-19 or Related Disease in Benishangul Gumuz Regional State: Phenomenological Design. J Multidiscip Healthc. 2022;15:679-688. Published April 2, 2022. doi:10.2147/JMDH.S351328
34. Barletta G, Castigo F, et al. The impact of COVID-19 on consumption poverty in Mozambique. WIDER Working Paper 2021/94. Helsinki: UNU-WIDER. Assessed August 15, 2024 from https://www.wider.unu.edu/sites/default/files/Publications/Working-paper/PDF/wp2021-94-impact-COVID-19-consumption-poverty-Mozambique.pdf
35. Squarcina M, Egger E-M. Effects of the COVID-19 crisis on household food consumption and child nutrition in Mozambique. WIDER Working Paper 2022/169. Helsinki: UNU-WIDER. Assessed August 15, 2024 from https://doi.org/10.35188/UNU-WIDER/2022/302-4.
36. Krauss JE, Artur L, et al. To prevent this disease, we have to stay at home, but if we stay at home, we die of hunger’ – Livelihoods, vulnerability and coping with Covid-19 in rural Mozambique. World Development. 2022;151. Accessed August 15, 2024 from https://www.sciencedirect.com/science/article/pii/S0305750X21003727?via%3Dihub