

Non-Operative Management of Stable Atlas Fractures
Characterizing Non-Operative Management for Stable Atlas Fractures: Insights from the Jefferson and Gehweiler Classification Scheme
Michael F. Shannon1,2,3,4, Rahul Ramanathan1,2,3, Feier Chang2,5, Christopher Gonzalez Jr1,2,3, Christopher Como1,2,3, Yunting M. Tang1,2,3, Anthony Oyekan1,2,3, Stephen Canton1,2,3, Jacob Weinberg1,2,3, John Bonamer1,2,3, Yan Ma2,5, Jeremy Shaw1,2, Richard Wawrose1,2,3, Joon Y. Lee1,2,3, Amir Abtahi2,6, Michael Spitnale1,2,3
- Department of Orthopedic Surgery, University of Pittsburgh, Pittsburgh, PA
- Pittsburgh Orthopedic Spine Research (POSR) Group, University of Pittsburgh, Pittsburgh, PA
- The Orland Bethel Musculoskeletal Research Center (BMRC), Pittsburgh, PA
- University of Pittsburgh School of Medicine, Pittsburgh, PA
- Department of Biostatistics, University of Pittsburgh, Pittsburgh, PA
- Department of Orthopedic Surgery, Vanderbilt Health, Nashville, TN
OPEN ACCESS
PUBLISHED: 31 December 2025
CITATION: Shannon, M., Ramanathan, R., et al. Characterizing Non-Operative Management for Stable Atlas Fractures: Insights from the Jefferson and Gehweiler Classification Scheme. J. Bone Miner. Res. 41(12).
https://doi.org/10.18103/mra.v13i2. 7177
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i2. 7177
ISSN: 2375-1924
Abstract
Background: Burst fractures of the C1 vertebra (atlas) have been characterized using both the Jefferson and Gehweiler classification schemes. Management of atlas fractures is largely determined by the integrity of the transverse atlantal ligament. Non-operative therapy is often indicated for stable fractures with an intact ligament. However, strict management guidelines have not been established, and more research is required to better characterize the patient population and complication profile.
Aims: The purpose of this study was to characterize and compare patient characteristics, risk factors, and outcomes of non-operatively managed stable atlas fractures according to classification scheme.
Methods: Patients who sustained isolated, stable C1 fractures and were managed non-operatively were included; patients with concomitant C2 or subaxial cervical fractures were excluded. Medical records were reviewed to collect demographics, management, injury mechanism, fracture pattern, past medical history, and outcome data. Jefferson and Gehweiler Classifications were manually assigned. Variables were analyzed using multinomial regression and analysis of variance where appropriate.
Results: After applying inclusion and exclusion criteria, 173 unique patients (91 males, 82 females) were eligible for analysis. Patients with Jefferson type IV fracture were significantly younger, more often polytrauma cases, and sustained higher-energy injuries. Length of stay, polytrauma percentages, rates of high-energy mechanisms, dependent functional status at 6 months, incidence of complications, age at time of fracture, and Age-Adjusted Charlson Comorbidity Index were significantly different between Gehweiler types. Overweight and obese status modulated odds for both Jefferson and Gehweiler fracture patterns. Complications were significantly lower with Gehweiler types I and III, though overall incidence was low. Only 4 deaths were recorded within 90 days.
Conclusion: This work contributes a large study to a limited body of literature describing outcomes of non-operative management for stable atlas fractures and stratifies outcomes in relation to the Jefferson and Gehweiler Classification schemata. These findings strengthen the existing evidence for safety and efficacy of conservative management and serve as a basis for a direct comparison of outcomes between operatively in the and non-operatively managed cohorts future. Further work is needed to clarify the relationship between fracture pattern, type of conservative management, and occurrence of complications.
Keywords: Atlas, Fracture, Trauma, Cervical Spine, Conservative Management
Introduction
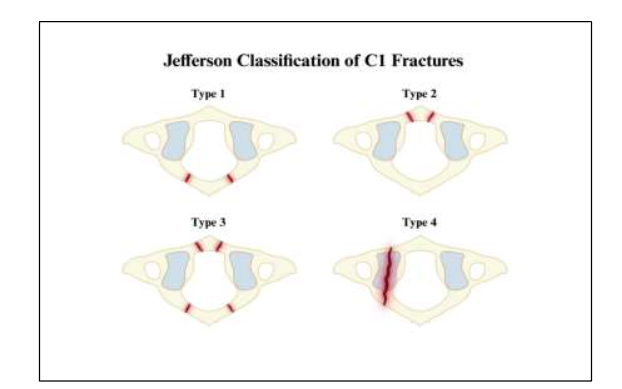
The Jefferson fracture, a burst-type fracture of the C1 vertebra (atlas), accounts for approximately 3-13% of fractures in the cervical spine. Originally described by Sir Geoffrey Jefferson in 1920, the Jefferson fracture pattern is classically characterized by bilateral fractures of both anterior and posterior arches on the C1 ring. This fracture often occurs with the application of a sudden axial load to the vertex of the skull, transmitting force downward through the occiput to the C1 ring.
Since its inception, the Jefferson classification has been expanded to include fracture complexes with a subtotal combination of the anterior ring, posterior ring, and lateral masses. These fractures, termed Jefferson-Variants, show some degree of variability in classification within the literature. A three-part scheme and four-part scheme have both been described, although differences in clinical utility between these systems are not well established.
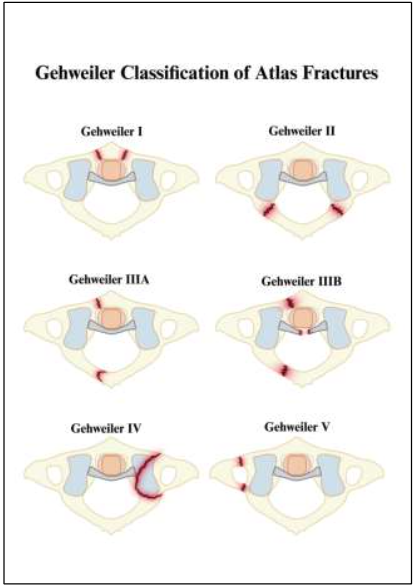
Although atlas burst fractures are often eponymously associated with the Jefferson classification system, other descriptive schemata have been developed. The Gehweiler classification has seen widespread use and formed the basis of treatment algorithms for atlas fracture management in Europe. Despite an increase in utilization, literature evaluating the clinical utility of the Gehweiler criteria is limited. Although the interobserver agreement for assigning Gehweiler type via radiography has been reported as moderate to high in small case series, further study is needed to assess clinical applications of the classification system. More recently, the AO Spine Society has also developed a representative set of criteria to classify fractures of the upper cervical spine, further increasing the options available to clinicians for description and management guidelines.
Management of atlas fractures is largely contingent upon the stability of the fracture complex. Because cervical flexion and extension are greatest at the atlantooccipital joint and most axial rotation in the cervical spine occurs at the atlantoaxial junction, the craniovertebral junction is especially prone to instability. In the trauma setting, transmission of axial force to the adjacent transverse atlantal ligament (TAL) can tear the ligament, whether complete or subtotal in thickness. Associated tearing of the TAL may result in C1-C2 vertebral instability and carries a greater risk of complication. As such, management depends largely on the integrity of the TAL. Stable fractures, characterized by an intact TAL, may warrant more conservative, non-operative treatment via external immobilization with a cervical collar or halo vest.
Decision-making in the management of C1 fractures remains clinically challenging. In addition to assessment of fracture stability, selection of treatment may be influenced by the presence of concomitant cervical spine injuries and other patient characteristics. Prior studies on atlas fracture outcomes have described good prognosis with appropriately limited activity and adherence to immobilization. However, outcome studies have historically been limited to small case series. No universally accepted standards of treatment have been validated as evidence is limited, and practices vary greatly. Notably, most studies within the existing literature do not stratify outcomes according to subtypes within each classification scheme. It therefore remains uncertain whether specific Jefferson or Gehweiler subtypes carry different risks of complications, functional decline, or prolonged hospitalization when treated non-operatively. Larger studies that evaluate outcomes across fracture morphologies are needed to guide prognostic counseling, optimize follow-up intensity, and reduce unwarranted variability in conservative management.
The objectives of this study were: (1) to describe the patient characteristics, risk factors, and outcomes associated with non-operative management of stable atlas fractures in a large sample, and (2) to compare risk according to fracture pattern as classified by the Jefferson and Gehweiler classification schemes.
METHODS
Study Design and Patient Population
In this IRB-approved multicenter retrospective cohort study, patients diagnosed with isolated stable atlas fractures at one of two academic institutions were identified via searches for key words in operative, radiographic, and chart presentation with stable isolated atlas fracture, and non-operative management. Exclusion criteria included age <18, concomitant C2 or subaxial cervical fractures, operative management, and treatment with halo vest immobilization. Additionally, patients whose fracture patterns were indeterminate or did not meet established criteria for Jefferson or Gehweiler classification were excluded from the corresponding classification-specific analyses.
Fracture Characteristics and Outcomes
Electronic medical records were reviewed manually by trained study personnel to collect information on demographics, management, injury mechanism, fracture pattern and injury complex, hospitalization length, discharge disposition, complications, ambulatory status, dependent functional status, 30-day readmission, and past medical history at time of intake. Age-Adjusted Charlson Comorbidity Index (CCI) score, a validated morbidity index to predict likelihood of 10-year mortality, was calculated manually for each patient at the time of initial presentation. The Modified 5-Item Frailty Index (mFI-5) was used to calculate frailty scores at intake, and changes in mFI-5 during hospitalization were recorded where available. Injury mechanism was used to classify fracture energy as either low energy or high energy. The fracture pattern interpreted from imaging or described in the corresponding radiology report was used to manually assign Jefferson and Gehweiler classifications for each patient. The tetrapartite Jefferson Classification scheme was selected for use, given its greater similarity to the Gehweiler Classification. Fracture patterns not meeting criteria for existing classification within each scheme were excluded from analysis for the corresponding classification system.
Statistical Methods
The relationship between atlas fracture subclassification and four clinical parameters was investigated: Length of Stay (LOS), Body Mass Index (BMI), 90-day mortality, and Age-Adjusted CCI. Due to the distinct correlative structures underlying these relationships, different statistical models were employed individually for each outcome.
LOS was treated as a binary variable with a cut-off of three days, and logistic regression was conducted using LOS as the dependent variable. Analysis was adjusted for Jefferson classification type and Age-Adjusted CCI. Multinomial regression was used to evaluate associations between Jefferson classification type and patient factors; Jefferson classification type was treated as the dependent variable with type IV as the reference group, adjusting for BMI and Age-Adjusted CCI. Analysis of variance (ANOVA) was performed to test differences in Age-Adjusted CCI among groups, and pairwise comparisons were then conducted using Jefferson type IV as the reference group.
All analyses were repeated using the Gehweiler classification scheme. Statistical procedures and covariate adjustments remained consistent with the initial analysis, including ANOVA for Age-Adjusted CCI, logistic regression for LOS, and multinomial regression for Gehweiler classification with type IV as the reference group, adjusted for BMI and Age-Adjusted CCI. All analyses were conducted using R version 4.4.0.
RESULTS
After inclusion and exclusion criteria were applied, 173 unique patients (91 male, 82 female) were included in this study. Patient demographics included an age at fracture ranging from 18 to 95 years (mean 58.25 ± 21.40), an average BMI of 27.74 ± 6.77 kg/m², and an average Age-Adjusted CCI of 3.06 ± 2.86.
Jefferson Classification
For the Jefferson classification system, fracture patterns include Jefferson I (30 patients), Jefferson II (39 patients), Jefferson III (46 patients), Jefferson IV (56 patients). In addition, 5 patients sustained fractures that did not fit an established Jefferson classification and could not be determined from available records; all these patients were excluded from analysis. Among the patients with fracture patterns amenable to classification into the Jefferson scheme, 9 patients demonstrated characteristics of both Jefferson I and III patterns, 1 patient fit both Jefferson II and III, and 2 patients fit both II and IV. Patient demographics and clinical characteristics by Jefferson type are displayed in Appendix A (Table A1).
| Covariate | Jefferson Classification |
|---|---|
| Age in Years, Mean (SD) | 63.50 (23.24), 56.69 (19.16), 62.76 (21.42), 51.27 (20.83) |
| Length of Stay in Days, Mean (SD) | 5.13 (5.78), 4.38 (4.59), 4.43 (5.11), 6.16 (8.76) |
| Change in mFI-5 Score while hospitalized | 0.542 |
| Polytrauma, n (%) | 19 (65.5), 24 (61.5), 20 (44.4), 39 (69.6) |
| High-Energy Fracture, n (%) | 9 (31.0), 22 (56.4), 14 (31.8), 33 (58.9) |
| Discharge Disposition | Home 17 (56.7), 26 (66.7), 29 (63.0), 38 (67.9) |
| Hospital Mortality | 1 (3.3), 0 (0.0), 0 (0.0), 0 (0.0) |
| 30-day Readmission, n (%) | No 27 (93.1), 36 (92.3), 43 (95.6), 52 (92.9) |
| mFI-5 Score at Intake, n (%) | 0 12 (41.4), 18 (46.2), 12 (26.7), 30 (53.6) |
| Ambulatory at Discharge, n (%) | Walking 16 (59.3), 25 (67.6), 27 (62.8), 29 (52.7) |
| Ambulatory at 6 months, n (%) | Walking 5 (62.5), 13 (100.0), 13 (72.2), 12 (100.0) |
| Partially or fully dependent functional status at 6 months, n (%) | No 6 (20.7), 13 (33.3), 16 (35.6), 11 (19.6) |
| Loss to follow-up | 22 (75.9), 26 (66.7), 27 (60.0), 45 (80.4) |
| Complication, n (%) | 3 (11.1), 7 (17.9), 7 (15.6), 2 (3.6) |
| Dementia, n (%) | 6 (20.0), 3 (7.7), 7 (15.2), 5 (8.9) |
| Diabetes Mellitus, n (%) | 8 (26.7), 6 (15.8), 13 (28.9), 5 (8.9) |
| Age-Adjusted CCI, Mean (SD) | 3.93 (3.19), 3.13 (3.03), 3.89 (3.01), 1.84 (1.95) |
| 90-Day Mortality, n (%) | 0 (0.0), 1 (2.9), 3 (6.8), 0 (0.0) |
| Female Sex, n (%) | 16 (53.3), 18 (46.2), 22 (47.8), 26 (46.4) |
| BMI Classification, n (%) | Healthy 9 (42.9), 12 (38.7), 11 (34.4), 17 (39.5) |
Patients with Jefferson type IV fracture were significantly younger (p=0.019), were more likely to be polytrauma patients (p=0.068), and had the highest rate of high-energy fracture mechanisms (p=0.009) among all classification types. Only 4 cases of patient mortality were reported within 90 days among all classification types: one from Jefferson II and three from Jefferson III. The Jefferson IV group had the lowest Age-Adjusted CCI among all groups (p=0.019). There were no significant mean differences across classifications for length of hospital stay when adjusted for Jefferson classification and Age-Adjusted CCI. The odds of patients with Jefferson I fracture being overweight after controlling for Age-Adjusted CCI was 27.7% higher than Jefferson IV (OR = 1.277). The odds of Jefferson II being overweight after controlling for Age-Adjusted CCI was 19.7% lower than Jefferson IV (OR = 0.803). The odds of Jefferson III being overweight after controlling for Age-Adjusted CCI was 51.8% higher than Jefferson IV (OR = 1.518). Results of this analysis were recorded in Table 1. Overall, Jefferson IV had the lowest odds of being overweight or obese after adjusting for Age-Adjusted CCI when compared with Jefferson I, II and III.
| Effect | Odds Ratio | 95% CI | P-Value |
|---|---|---|---|
| Obese: I vs IV | 1.026 | (0.255, 4.135) | 0.971 |
| II vs IV | 1.701 | (0.544, 5.322) | 0.362 |
| III vs IV | 1.589 | (0.478, 5.284) | 0.450 |
| Overweight: I vs IV | 1.277 | (0.354, 4.602) | 0.709 |
| II vs IV | 0.803 | (0.242, 2.666) | 0.720 |
| III vs IV | 1.518 | (0.480, 4.800) | 0.477 |
| Underweight: I vs IV | 2.074e-08 | (<0.001, >999.999) | 0.982 |
| II vs IV | 7.868e-10 | (<0.001, >999.999) | 0.982 |
| III vs IV | 1.931e-09 | (<0.001, >999.999) | 0.982 |
| CCI Low: I vs IV | 6.999e-07 | (<0.001, >999.999) | 0.949 |
| II vs IV | 2.202 | (0.512, 9.472) | 0.289 |
| III vs IV | 2.235 | (0.476, 10.504) | 0.308 |
| CCI High: I vs IV | 4.584 | (1.406, 14.946) | 0.012 |
| II vs IV | 2.690 | (0.935, 7.743) | 0.067 |
| III vs IV | 4.601 | (1.560, 13.569) | 0.006 |
Gehweiler Classification
For the Gehweiler classification system, fracture patterns included Gehweiler I (48 patients), Gehweiler II (20 patients), Gehweiler III (37 patients), Gehweiler IV (64 patients), Gehweiler V (8 patients). Additionally, 3 patients had fracture patterns that did not fit an established pattern, and available records. These patients were excluded from analysis. Among the patients with fracture patterns amenable to classification into the Gehweiler scheme, 11 were identified as both Gehweiler I and IV, 1 patient was identified as both Gehweiler III and IV, 2 patients were both classified as IV and V, and 1 patient was classified as Gehweiler I, IV, and V. Demographics for this grouping are displayed in Appendix A (Table A2).
| Covariate | Gehweiler Classification |
|---|---|
| Age in Years, Mean (SD) | 56.10 (20.29), 66.65 (21.91), 64.24 (19.72), 52.23 (21.44), 49.12 (21.94) |
| Length of Stay in Days, Mean (SD) | 5.12 (5.57), 3.85 (3.77), 3.49 (3.55), 6.52 (8.74), 15.75 (30.20) |
| Change in mFI-5 Score while hospitalized | 0.323 |
| Polytrauma, n (%) | 31 (66.0), 12 (60.0), 11 (29.7), 48 (76.2), 7 (87.5) |
| High-Energy Fracture, n (%) | 24 (51.1), 6 (30.0), 10 (27.8), 35 (55.6), 6 (75.0) |
| Discharge Disposition | Home 30 (62.5), 12 (60.0), 24 (64.9), 44 (68.8), 6 (75.0) |
| Hospital Mortality | 0 (0.0), 1 (5.0), 0 (0.0), 0 (0.0), 0 (0.0) |
| 30-day Readmission, n (%) | No 44 (93.6), 18 (90.0), 35 (94.6), 61 (96.8), 8 (100.0) |
| mFI-5 Score at Intake, n (%) | 0 22 (46.8), 8 (40.0), 8 (21.6), 34 (54.0), 6 (75.0) |
| Ambulatory at Discharge, n (%) | Walking 30 (68.2), 10 (52.6), 22 (61.1), 34 (56.7), 4 (50.0) |
| Ambulatory at 6 months, n (%) | Walking 15 (100.0), 4 (57.1), 12 (70.6), 11 (100.0), 1 (100.0) |
| Partially or fully dependent functional status at 6 months, n (%) | No 14 (29.8), 5 (25.0), 16 (43.2), 10 (15.9), 1 (12.5) |
| Loss to follow-up | 33 (70.2), 14 (70.0), 19 (51.4), 53 (84.1), 7 (87.5) |
| Complication, n (%) | 9 (19.1), 1 (5.6), 7 (18.9), 2 (3.2), 1 (12.5) |
| Dementia, n (%) | 3 (6.2), 6 (30.0), 6 (16.2), 6 (9.4), 1 (12.5) |
| Diabetes Mellitus, n (%) | 9 (19.1), 4 (20.0), 11 (30.6), 8 (12.5), 1 (12.5) |
| Age-Adjusted CCI, Mean (SD) | 3.02 (2.91), 4.30 (3.40), 4.24 (3.11), 1.98 (2.05), 1.88 (2.47) |
| 90-Day Mortality, n (%) | 1 (2.2), 0 (0.0), 3 (8.8), 0 (0.0), 0 (0.0) |
| Female Sex, n (%) | 23 (47.9), 11 (55.0), 16 (43.2), 33 (51.6), 2 (25.0) |
| BMI Classification, n (%) | Healthy 15 (41.7), 6 (37.5), 9 (32.1), 19 (42.2), 2 (33.3) |
With Gehweiler IV as the reference group, we conducted subgroup analysis for covariates that differed significantly across Gehweiler types I V. After adjusting for Age-Adjusted CCI, LOS was significantly higher for patients with Gehweiler V fracture than those with Gehweiler III or IV (p=0.008). The percentage of patients with polytrauma was significantly lower for the Gehweiler III group (p<0.001). The percentage of high-energy fracture mechanisms was significantly lower in the Gehweiler II and III groups than other fracture types (p=0.015). Dependent functional status at 6 months differed significantly across the 5 Gehweiler types (p=0.026). Dependent functional status at 6 months of Gehweiler IV was significantly different from that of Gehweiler III. The incidence of complications differed significantly across Gehweiler types (p=0.048). The distribution of complication cases of Gehweiler IV was significantly different from Gehweiler I and III. Age at fracture (p=0.012) and Age-Adjusted CCI (p<0.001) were significantly different between groups. Age at fracture and Age-Adjusted CCI of Gehweiler IV were significantly different from Gehweiler II and III. Only 4 deaths were recorded within 90 days, one associated with a Gehweiler I pattern fracture and 3 with Gehweiler III pattern.
Odds of overweight BMI were 10.9% lower for patients with Gehweiler I fracture compared to those with Gehweiler IV after controlling for Age-Adjusted CCI (OR = 0.891). The odds of Gehweiler II being overweight after controlling for Age-Adjusted CCI was 51.3% higher than Gehweiler IV (OR = 1.513). The odds of Gehweiler III being overweight after controlling for Age-Adjusted CCI was 157.4% higher than Gehweiler IV (OR = 2.574). In general, Gehweiler IV demonstrated the lowest odds of being overweight or obese after adjusting for Age-Adjusted CCI. Results of this analysis were recorded in Table 2.
| Effect | Odds Ratio | 95% CI | P-Value |
|---|---|---|---|
| Obese: I vs IV | 1.528 | (0.510, 4.578) | 0.449 |
| II vs IV | 1.771 | (0.398, 7.881) | 0.453 |
| III vs IV | 2.216 | (0.632, 7.768) | 0.214 |
| V vs IV | 3.802e-12 | (<0.001, >999.999) | 0.927 |
| Overweight: I vs IV | 0.891 | (0.298, 2.669) | 0.837 |
| II vs IV | 1.513 | (0.351, 6.524) | 0.579 |
| III vs IV | 1.719 | (0.501, 5.897) | 0.389 |
| V vs IV | 2.574 | (0.403, 16.441) | 0.318 |
| Underweight: I vs IV | 2.469e-17 | (<0.001, >999.999) | 0.970 |
| II vs IV | 2.089e-13 | (<0.001, >999.999) | 0.976 |
| III vs IV | 9.287e-16 | (<0.001, >999.999) | 0.970 |
| CCI Low: I vs IV | 1.695 | (0.413, 6.962) | 0.464 |
| II vs IV | 4.522e-11 | (<0.001, >999.999) | 0.940 |
| CCI High: I vs IV | 2.283 | (0.854, 6.104) | 0.099 |
| II vs IV | 8.580 | (2.041, 36.070) | 0.003 |
| III vs IV | 7.960 | (2.390, 26.510) | 0.001 |
| V vs IV | 0.450 | (0.046, 4.395) | 0.492 |
Complications
Within the sample, 9 patients (5.09%) had one or more documented complications related to their fracture. Complications include persistent difficulties with neck range of motion, vertebral artery pseudoaneurysm, cervical radiculopathy, chronic neck pain, chronic neck weakness, and aspiration pneumonia (Jefferson II, Gehweiler I). The most implicated Jefferson fracture patterns were II and III. The most implicated Gehweiler fracture patterns were I and III.
| Description of Complication | Number of Patients | Jefferson Classification(s) | Gehweiler Classification(s) |
|---|---|---|---|
| Persistent limitation in ROM | 2 | III | 3 |
| Repeat ground-level fall | 2 | I, III | 2,3 |
| Concussion | 2 | III | 3 |
| Aspiration PNA | 2 | II | 1 |
| Chronic neck pain | 2 | III | 3 |
| Chronic vestibular symptoms | 1 | III | 3 |
| Neck weakness | 1 | III | 3 |
| Vertebral artery aneurysm | 1 | III | 3 |
| Need for tracheostomy | 1 | II | 1 |
| Cervical radiculopathy | 1 | II | 1 |
| Deep vein thrombosis | 1 | I | 2 |
| Mortality | 1 | III | 3 |
DISCUSSION
Burst-type atlas fractures are relatively common, accounting for up to 13% of all cervical spine fractures and usually occur in the setting of traumatic axial compression. Both the Jefferson and Gehweiler classification systems have been described to categorize atlas fracture morphology. However, little research has evaluated the utility of these systems in predicting patient outcomes or clinical management. This study highlights the role of patient demographics, injury mechanisms, and fracture patterns in influencing outcomes for non-operatively managed stable atlas fractures.
Younger patients with high-energy injuries demonstrated more favorable overall outcomes, while older patients with low-energy mechanisms faced higher complication rates. Data comparing the incidence for individual Jefferson or Gehweiler variant fracture patterns is sparse as reporting has been limited in the literature. In a retrospective study of 189 atlas fractures, Fiedler et al reported that Gehweiler III was the most frequent pattern of injury; in contrast, our data demonstrated greater prevalence of type I and type IV fractures. While the factors that influence the type of ring-splitting pattern are not well evidenced, our data indicates key demographic differences between fracture pattern groups that may reflect underlying risk factors and biomechanical characteristics. Prior population studies on atlas fracture epidemiology have reflected bimodal age distribution with peak incidence around ages 30 and 80. In our sample, greater incidence of atlas fracture in younger patients was observed with high-energy trauma (i.e., motor vehicle accident or fall from height) versus low-energy mechanisms in older adults. This accords with demographic observations by other authors. Here, patients who sustained Jefferson type IV and Gehweiler type IV-V fractures with lateral mass involvement also tended to have lower scores for medical comorbidity. Although this is likely influenced in part by typical age distribution between groups, the presence of medical comorbidities may impact predisposition to complications and is a relevant factor in determining clinical management.
The classical atlas burst fracture occurs under direct, forceful axial loading with corresponding four-part fracturing of the anterior and posterior arches, regarded under modern classifications as a “Jefferson I” or “Gehweiler I” fracture. However, in concert with axial compression, adjunctive forces and neck positioning may exert greater influence on the separation of C1 ring components. Lateral neck flexion or neck rotation may result in lateral mass fractures. Alternatively, axial loading with flexion may result in anterior ring fracture due to impaction by the odontoid process of C2, and extension may lead to posterior ring fracture via compression between the occiput and the C2 lamina or spinous process. Limited studies have been conducted to evaluate the biomechanical principles that influence subtotal fracturing of the C1 ring. Most existing knowledge is derived from cadaveric or modeling studies, as this is challenging to study in human subjects. Given the findings of increased frequency of lateral mass fracture in a young population, it is plausible that high energy trauma in the young population may tend to produce a moment of impact involving greater degrees of lateral flexion or rotation. Moreover, younger patients may be more susceptible to injuries of this nature. Conversely, patients of older age may have a higher degree of neck motion in flexion or extension during low-energy injury mechanisms, resulting in anterior or posterior arches fractures. However, further dedicated biomechanical studies are needed to fully illustrate this hypothesis.
Our findings support the use of both the Jefferson and Gehweiler Classification system as prognostic tools that may have benefit in managing stable C1 fractures. In this population, we observed that younger patients with fractures involving the lateral mass (Jefferson and Gehweiler type IV) tended to have a lower risk of acute complications. In contrast, we observed greater prevalence of complications both acutely (falls, aspiration pneumonia) and chronically (range of motion limitations, persistent radiculopathy) in older patients with Jefferson and Gehweiler class I-III fractures involving the anterior and posterior arches. Other authors have described a spectrum of severe complications secondary to atlas burst fractures, including injury to Cranial Nerves IX-XII (Collet-Sicard Syndrome), complete neurologic injury, and deformity. Impaired fracture healing has also been described; Lleu et al reported a non-union rate of 12.5% across 40 cases of non-operatively managed atlas fractures. While the use of halo vest immobilization has been reported for upper cervical fractures, complications such as dysphagia, pulmonary dysfunction, pin-site infection, and mortality have raised question surrounding the suitability of use in more elderly patients. Our findings of increased baseline risk for complication in elderly patients with Jefferson and Gehweiler I-III fractures suggest that heightened monitoring protocols may merit consideration for this population, even when managed with hard cervical orthoses. Success with collar for durations of 8-12 weeks have been reported, though evidence is mostly limited to case reports and series. In contrast, early identification of isolated lateral mass fractures may expedite non-operative care decisions and potentially facilitate earlier discharge planning, helping to lessen the healthcare cost burden associated with cervical fractures.
Collectively, the Jefferson and Gehweiler systems may represent a largely unexplored avenue for guiding management decisions. While high level evidence from studies comparing non-operative and operative management is not available, use of these schemata for classifying fracture morphology can serve as an additional tool to aid prediction of clinical outcomes with non-operative management. Previously, Kandziora et al proposed that direct osteosynthesis may be warranted for Gehweiler IIIB fractures, whereas non-operative management with hard collar and close monitoring is appropriate for Gehweiler IIIA fractures. Our data suggest that while operative intervention may not be necessary to achieve bony union, closer monitoring is indicated not only for type III fractures but type I and II fractures as well. While prior studies have proposed that lateral mass fracture and displacement (type IV fracture) may carry higher risk of ring instability via predisposition to TAL rupture, our data suggests that lateral mass involvement alone is not a strict criterion for operative intervention and that successful non-operative management of atlas fractures can be achieved with comparatively lower complication rate in younger adults. To optimize the practice of tailoring management to fracture pattern, comparative studies to validate management guidelines for Types I-III versus IV should be performed in the future.
CONCLUSIONS
The Jefferson and Gehweiler classification schemes are variably used, and outcomes of stable atlas fractures as classified by these systems have rarely been compared in large sample sizes. This study sought to analyze the systems in parallel and describe demographics, risk factors, and outcomes. In this cohort, patients were generally middle aged, overweight, and ambulatory with low scores for frailty and medical comorbidity. A substantial proportion of patients sustained fractures involving the lateral mass in one or both classification systems. Jefferson and Gehweiler III fractures may be more likely with lower-impact injury, whereas Jefferson and Gehweiler IV fractures may be more likely with higher-energy impact. The overall incidence of complications was low, although limited follow-up posed a significant limitation. These findings strengthen the existing evidence for safety and efficacy of conservative management and serve as a basis for a direct comparison of outcomes between operatively and non-operatively managed cohorts in the future. More work is needed to fully investigate the relationship between fracture pattern, type of conservative management, and occurrence of complications.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
No financial disclosure.
References:
- Kim HS, Cloney MB, Koski TR, Smith ZA, Dahdaleh NS. Management of Isolated Atlas Fractures: A Retrospective Study of 65 Patients. World Neurosurg. Mar 2018;111:e316-e322. doi:10.1016/j.wneu.2017.12.053
- Jefferson G. Fracture of the atlas vertebra: report of four cases, and a review of those previously recorded. British Journal of Surgery. 1919;7(27):407-422. doi:https://doi.org/10.1002/bjs.1800072713
- Almalki M, Alghamdi EA, Alasmari R, Aldossary N, Hussain T, Hamad A. A C1 Jefferson Fracture With Vertebral Artery Occlusion and Cerebellar Infarction: A Case Report. Cureus. May 2023;15(5):e38789. doi:10.7759/cureus.38789
- Laubach M, Pishnamaz M, Scholz M, et al. Interobserver reliability of the Gehweiler classification and treatment strategies of isolated atlas fractures: an internet-based multicenter survey among spine surgeons. Eur J Trauma Emerg Surg. Feb 2022;48(1):601-611. doi:10.1007/s00068-020-01494-y
- Martinez-Romo MA, McCoy CE. Jefferson Fracture and the Classification System for Atlas Fractures, A Case Report. J Educ Teach Emerg Med. Apr 2021;6(2):V16-V19. doi:10.21980/J88P9C
- Lekic N, Sheu J, Ennis H, Lebwohl N, Al-Maaieh M. Why you should wear your seatbelt on an airplane: Burst fracture of the atlas (jefferson fracture) due to in-flight turbulence. J Orthop. Jan-Feb 2020;17:78-82. doi:10.1016/j.jor.2019.06.019
- Vynichakis G, Grivas TB, Moschouris H, Filippou D, Skandalakis P. Atlas Fracture with Concomitant Vertebral Artery Hypoplasia, a Rare but Potentially Hazardous Combination: A Case Report. Cureus. Mar 4 2019;11(3):e4172. doi:10.7759/cureus.4172
- Kandziora F, Scholz M, Pingel A, et al. Treatment of Atlas Fractures: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Global Spine J. Sep 2018;8(2 Suppl):5S-11S. doi:10.1177/2192568217726304
- Schleicher P, Scholz M, Kandziora F, et al. Recommendations for the Diagnostic Testing and Therapy of Atlas Fractures. Z Orthop Unfall. Oct 2019;157(5):566-573. Empfehlungen zur Diagnostik und Therapie oberer Halswirbelsaulenverletzungen: Atlasfrakturen. doi:10.1055/a-0809-5765
- Vaccaro AR, Lambrechts MJ, Karamian BA, et al. AO Spine upper cervical injury classification system: a description and reliability study. Spine J. Dec 2022;22(12):2042-2049. doi:10.1016/j.spinee.2022.08.005
- Goel A, Bhatjiwale M, Desai K. Basilar invagination: a study based on 190 surgically treated patients. J Neurosurg. Jun 1998;88(6):962-8. doi:10.3171/jns.1998.88.6.0962
- Menezes AH, Traynelis VC. Anatomy and biomechanics of normal craniovertebral junction (a) and biomechanics of stabilization (b). Childs Nerv Syst. Oct 2008;24(10):1091-100. doi:10.1007/s00381-008-0606-8
- Tay SY, Li CW, Ko CH, Chan WP. A Nonsurgical Solution: Jefferson (Burst) Fracture. Am J Med. Sep 2018;131(9):1061-1063. doi:10.1016/j.amjmed.2018.05.018
- Lee TT, Green BA, Petrin DR. Treatment of stable burst fracture of the atlas (Jefferson fracture) with rigid cervical collar. Spine (Phila Pa 1976). Sep 15 1998;23(18):1963-7. doi:10.1097/00007632-199809150-00008
- Kandziora F, Chapman JR, Vaccaro AR, Schroeder GD, Scholz M. Atlas Fractures and Atlas Osteosynthesis: A Comprehensive Narrative Review. J Orthop Trauma. Sep 2017;31 Suppl 4:S81-S89. doi:10.1097/BOT.0000000000000942
- Kakarla UK, Chang SW, Theodore N, Sonntag VK. Atlas fractures. Neurosurgery. Mar 2010;66(3 Suppl):60-7. doi:10.1227/01.NEU.0000366108.02499.8F
- Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. Nov 1994;47(11):1245-51. doi:10.1016/0895-4356(94)90129-5