

Noninvasive Skin Cancer Classification via VOCT and OCT
Clinical Use of Vibrational Coherence Tomography and Optical Coherence Tomography to Noninvasively Classify Skin Cancers: A New Telemedicine Technique
Frederick H. Silver¹,², Tanmay Deshmukh², Kelly Ritter³ and Hari Nadiminti³
- Department of Pathology and Laboratory Medicine, Robert Wood Johnson Medical School, Rutgers, the State University of New Jersey, Piscataway, NJ 08854
- Optovibronex, LLC, Bethlehem, PA 18104, USA
- Dermatology, Summit Health, Berkeley Heights NJ 07922
OPEN ACCESS
PUBLISHED:31 October 2025
CITATION: Silver F, et al., 2025. Clinical Use of Vibrational Coherence Tomography and Optical Coherence Tomography to Noninvasively Classify Skin Cancers: A New Telemedicine Technique. Medical Research Archives, [online] 13(10).
https://doi.org/10.18103/mra.v13i10.6959
COPYRIGHT:© 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI:https://doi.org/10.18103/mra.v13i10.6959
ISSN 2375-1924
Abstract
Background: Vibrational optical coherence tomography (VOCT) is a new digital technique that identifies cancerous cells, small friable blood vessels, and fibrotic tissues that are the hallmarks of epithelial cell derived skin cancers. This technique uses infrared light and acoustic sound to characterize the components of skin and skin lesions and the differences that occur during cancer. Initial studies focused on understanding the physiological changes that occur that are the basis for noninvasive classification of skin cancers.
Objective: To collect additional clinical optical coherence tomography (OCT) images of cancerous lesions to develop convolutional neural network models of basal cell carcinomas (BCCs), squamous cell carcinomas (SCCs), and melanomas with high sensitivities and specificities. The goal of this research is to produce digital images and AI models that can be used with telemedicine for remote classification of skin cancers.
Methods: OCT images of cancerous lesions were collected using the OptoScope and compared to images of normal skin using a convolutional neural network. The models are developed by comparing the intensity distribution and location of pixels contained in the OCT images.
Results: Gray scale and color-coded OCT images of normal skin, BCCs, SCCs and melanomas were evaluated using convolutional neural network models. The models predicted the type of lesions with sensitivity and specificity greater than 90%. These models were able to predict the correct classifications of BCC, SCC, and melanomas consistent with the diagnoses based on lesion histopathology conducted by board certified dermatopathologists.
Conclusions: Results of OCT studies indicate that CNN models can classify different skin cancers in several minutes based on OCT images of BCC, SCC, and melanomas. Noninvasive use of the OptoScope provides digital information about skin cancers that can be used to classify skin cancers as part of an evaluation of patient lesions via telemedicine. This is particularly useful in areas where Dermatologists are in short supply and patient waiting times are prolonged. Evaluation using new digital techniques and the availability of approved topical treatments for these cancers will provide an effective manner to treat patients in rural areas where Dermatology visits are not readily available.
Keywords
basal cell carcinoma, squamous cell carcinoma, melanoma, vibrational OCT, OCT, cancer associated fibroblasts, thin blood vessels, fibrotic tissue, noninvasive testing, skin cancer, telemedicine
Introduction
Skin cancer is one of the fastest growing cancers worldwide. The incidence of nonmelanoma and melanoma skin cancers rank 5th and 17th, respectively among all cancers worldwide and is growing rapidly. In 2022 the estimated number of skin cancers was 20M and is expected to grow to 32.6M by 2045. There are approximately 5.4M basal cell (BCC) and squamous cell carcinomas (SCC) diagnosed each year in the US with 8 out of 10 of these cancers being BCCs. Of these, 60 to 80% of BCCs are nodular. One report suggests that nodular BCC of the face can be successfully treated topically with ingenol mebutate gel. BCC topical treatments with 5% imiquimod cream, 5 fluorouracil, and diclofenac gel have also been reported suggesting that some of these BCCs can be treated topically avoiding the trauma and skin loss associated with excisional therapy.
SCC makes up about 20% of all skin cancers in the US with the most prominent form being superficial cutaneous squamous carcinoma. Topical treatments for superficial SCC include 5 fluorouracil and imiquimod cream. The remaining skin cancers include melanoma which is projected to involve 105,000 new cases in 2025 in the US. Topical treatment of melanoma in situ with imiquimod cream, 5 fluorouracil, and other immunotherapies have been reported. The gold standard of skin cancer treatment is a biopsy followed by a complete excision after identification of clear lesion edges based on histopathology. While excision is the primary method used for skin cancer treatment in the US, a recent study of early SCC (Bowen’s disease) indicated that treatment with 5 fluorouracil was not inferior to surgical excision and led to good or better cosmetic outcomes as compared to excisional therapy.
These results suggest that new noninvasive digital technologies for skin lesion classification may lead to more extensive use of topical treatments for lesions identified as small skin cancers. Dermoscopy and visual inspection are the most widely used methods to detect skin cancers. However, more advanced noninvasive diagnostic techniques are needed and are being developed, including reflectance confocal microscopy, elastography, optical coherence tomography (OCT), and vibrational optical coherence tomography. Some of these methods can be employed remotely and data transferred over the internet. The aim of these methods is to provide fast, noninvasive screening of cancerous lesions to facilitate patient evaluation and treatment since the waiting times to see dermatologists are deemed to be excessive. This has led to new developments in the digital biopsy market that is projected to grow at a rate of 16.87% CAFR between 2025 and 2032. The demand for non-invasive techniques is growing rapidly to reduce the large number of biopsies on benign lesions conducted by Dermatologists which has been reported to be 55.5% of all skin biopsies conducted in the US. Rapid noninvasive methods are also needed to improve the quality of patient skin checks that can be achieved in part through improving the quality of teledermatology.
Teledermatology has been used remotely by analyzing camera photos or live video conferences of skin problems along with associated clinical histories. In the past teledermatology has been considered a supplement to a patient’s total care and not a replacement for in-person doctor’s visits. Much of the diagnostic criteria for patient evaluation by a Dermatologist is qualitative and not quantitative. The surface image of a lesion seen by dermoscopy often lacks subsurface details. New techniques such as optical coherence tomography, elastic scattering, Raman Spectroscopy, high frequency ultrasound, electrical impedance spectroscopy, and reflectance confocal microscopy may provide more information on subsurface structure. Advances in these technologies for the diagnosis of skin cancer are needed to optimize individual patient treatments.
One limiting factor in receiving dermatological care is the barriers to receiving access in underserved populations. The barriers include lack of health insurance, residence location, and being under federal poverty level. The goal of these new technologies is to create rapid noninvasive techniques to classify skin lesions by a variety of healthcare professionals that can be used along with telemedicine. The purpose of this paper is to describe a new technique termed vibrational optical coherence tomography (VOCT) that uses light and acoustic vibrations to characterize skin lesions based on the resonant frequency of skin components of both normal and cancerous lesions. The technique can differentiate between normal and cancerous cells, cancer associated fibroblasts, new thin and normal blood vessels, and fibrotic tissue characteristic of skin cancers. This paper will first describe the basic science studies conducted on normal skin and skin cancers that have led to the development of a clinical test. The clinical test can be conducted noninvasively to rapidly classify lesions using artificial intelligence (AI) and telemedicine as well as to evaluate the lesion base after the cancer is removed.
Methods
This study involved two separate parts. The first part of this study involves the use of both sound to result in a mechanical deflection of the samples and infrared light reflection during examination by the Vibrational OptoScope to define changes observed in cancerous lesion physical properties that are different from those observed in normal skin (VOCT). The second part is the development of a rapid clinical test based only on OCT images that requires only about 1 minute to collect raw OCT images noninvasively generating digital information that can be used along with AI and telemedicine to provide lesion classification in remote areas.
VOCT MEASUREMENTS
Skin Component Physical Property Identification The Vibrational OptoScope consists of a modified Lumedica OQ 2.0 OCT (Lumedica Inc, Durham, NC) equipped with a small 2.0-inch speaker as described previously operating at a wavelength of 840 nm collecting 13,000 frames per second. The device is modified with special software that is used to evaluate the displacement of the tissue under different acoustic frequency deformations. The measurements were made in vivo on intact control skin and on human cancerous lesions. All images were collected as part of IRB approved clinical studies on skin at Summit Health (Berkeley Heights, NJ) and Rutgers Center for Dermatology (Somerset, NJ). Clinical diagnoses were made by board certified dermatopathologists after H&E staining and review of the tissue sections as part of routine clinical skin excisional protocols. Measurements were made on OCT images of control skin (N=200), BCCs (N=99), SCCs (N=47), and melanomas (N=106).
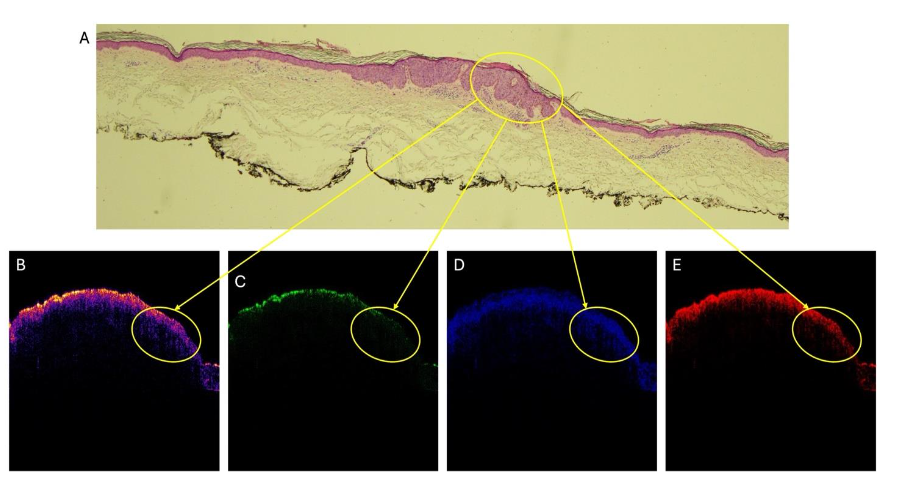
The OptoScope included a 2 inch-diameter speaker placed about 2.0 inches from the tissue to be vibrated in the VOCT studies. The speaker creates a sinusoidal sound wave at 55 dB using an app supplied by the I5 computer that is part of the OptoScope. Both the sound wave and the light were applied to the tissue surface along the axis of the light beam at increasing sound frequencies between 30 and 300Hz. The deflection of the surface vertically along the direction of the path of the light beam was measured. The weighted displacement was measured by determining the tissue displacement in the presence of the sound divided by the displacement of the speaker in the absence of a sample. All OCT images were created by scanning the skin of cancerous lesion cross sections. The gray scale scans were color coded using image J as reported previously. The OCT gray scale pixel images were also broken into green, blue, and red subchannel images using a lookup table. By breaking up the pixel intensity distribution at each point into low (green), medium (blue), and high (red) intensities, it is possible to examine differences in reflection of the different layers of skin and skin lesions. The VOCT analysis of skin cancers requires about 15 minutes to collect all the required data and an additional 10 to 20 minutes to process the data. Therefore, the development of a rapid classification method that was more suitable for use in the clinic was undertaken based on the collected OCT images once the contributions of each skin component was understood based on the VOCT study results.
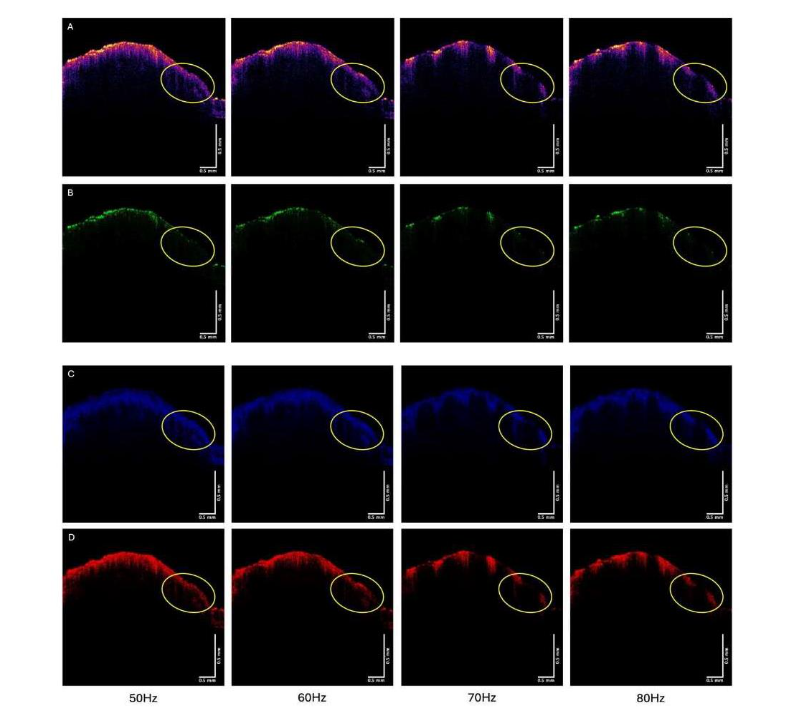
VOCT data collected on the lesions were compared to H&E-stained tissue sections of the cancerous lesions. All diagnoses were made by board certified Dermatopathologists after review of each lesion. OCT images were also collected on intact skin lesions and tissue biopsies vibrated at frequencies between 50 and 80 Hz. OCT gray scale images were color-coded using image J. Green, blue, and red subchannel OCT images were prepared using a RGB look-up table.
Clinical Classification Test Based on OCT Images
A clinical test was developed using OCT images without vibrational data to provide a rapid classification for cancerous skin lesions. In the clinical test, OCT images were collected on skin lesions and compared to images of normal skin using a convolutional neural network (CNN). The sensitivity, specificity, and area under the operating curve (AUOC) were calculated for CNN models developed for each cancer type. In this study, a transfer learning-based Convolutional Neural Network (CNN) using the ResNet18 architecture was implemented to classify OCT images of normal skin versus BCC, SCC, and melanoma. The grayscale images were converted into three-channel inputs to match the ResNet18 requirements, and data augmentation techniques such as random horizontal flipping, rotation, and resizing were applied to enhance generalization, while normalization followed ImageNet standards. Using a 5-fold cross-validation strategy, to ensure robust performance evaluation, and the final classification layer of ResNet18 was modified to output a single node for binary classification. The network was trained using the Adam optimizer with Binary Cross-Entropy loss over multiple epochs, with the best-performing model saved based on validation accuracy. To provide interpretability, Gradient-weighted Class Activation Mapping (Grad-CAM) was employed to highlight the discriminative regions used by the model when distinguishing skin lesions from normal skin. Finally, model performance was assessed through test accuracy, confusion matrices, sensitivity, specificity, and ROC-AUC analysis, offering both predictive power and clinical relevance.
Results
BASIC VOCT STUDIES OF SKIN CANCER
The first part of these studies was directed to compare the resonant frequency of the different components of normal skin and cancerous skin lesions. As summarized in Table 1, normal skin has major resonant frequency peaks at 50, 100, and 150Hz while cancerous skin lesions have additional peaks at 80, 130, and 250-260Hz.
| Resonant Frequency (Hz) | Component |
|---|---|
| 50-60 | Normal Epithelial Cells |
| 80 | Cancer Associated Fibroblasts |
| 100 | Papillary Collagen |
| 130 | Cancerous Thin Blood Vessels |
| 150 | Normal Blood Vessels |
| 250-260 | Fibrous Tissue Surrounding Cancers |
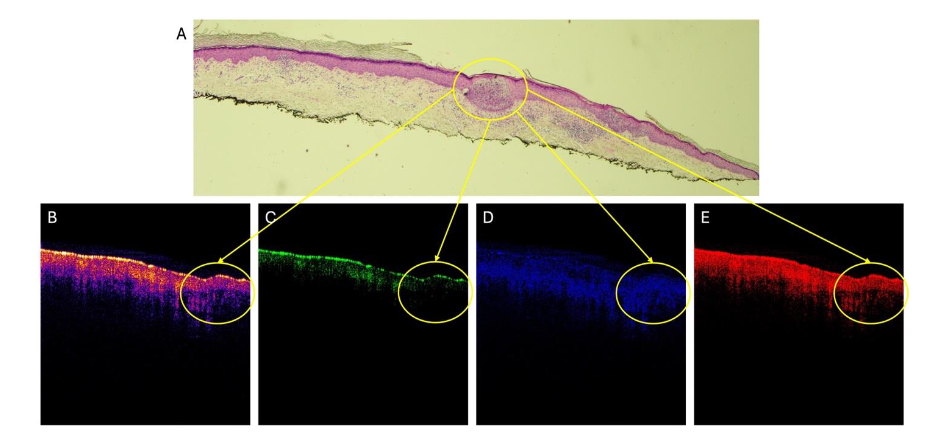
Figure 2 compares the color-coded OCT image (2A) and green (2B), blue (2C), and red (2D) subchannel images of a basal cell carcinoma vibrated at 50, 60, and 70 Hz.
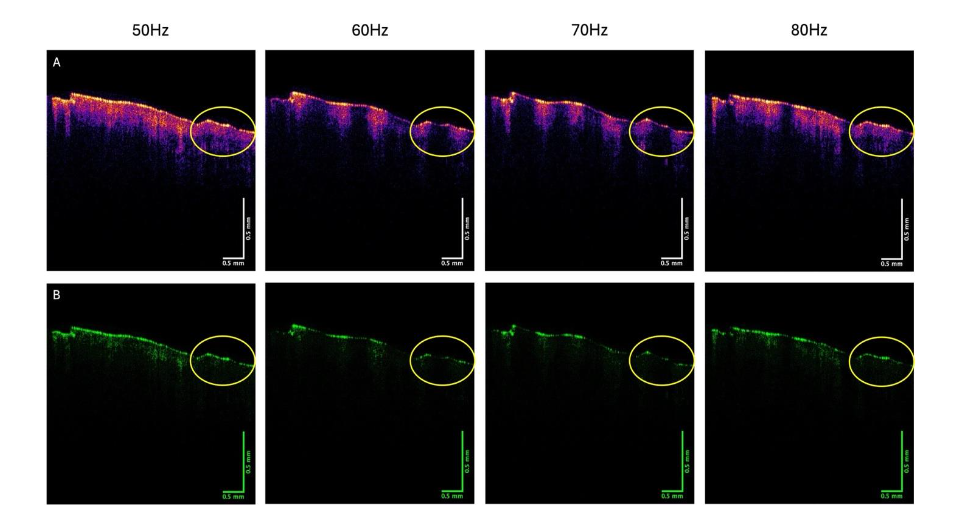
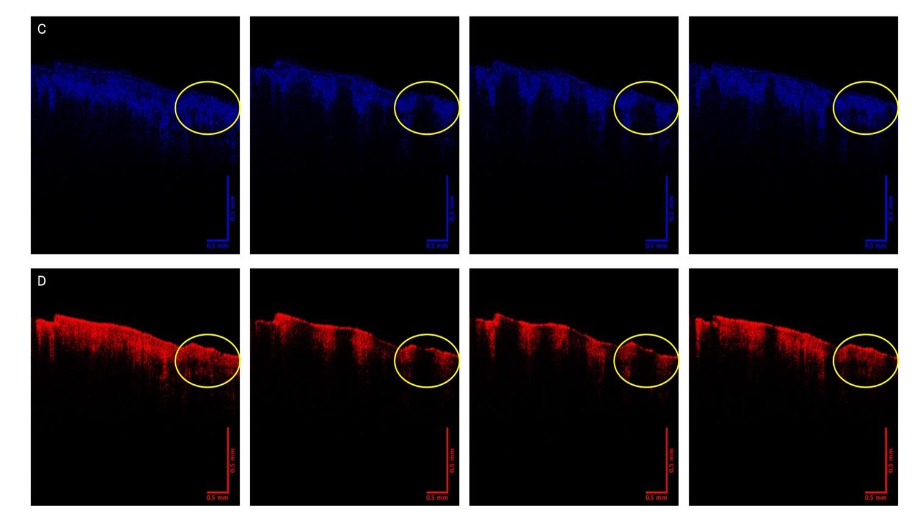
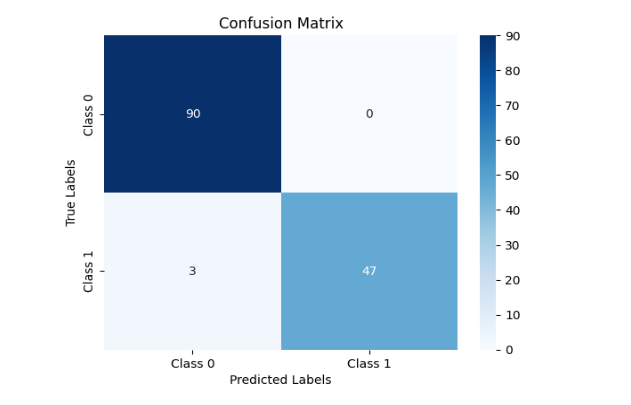
Table 2 lists the results of sensitivity and specificity calculations as well as the area under the operating curve (AUOC) predicted by the model.
| Type | Sensitivity | Specificity | Area Under Curve (AUOC) |
|---|---|---|---|
| Normal Skin vs BCC | 93.4% | 100% | 0.97 |
| Normal Skin vs SCC | 94.0% | 100% | 0.97 |
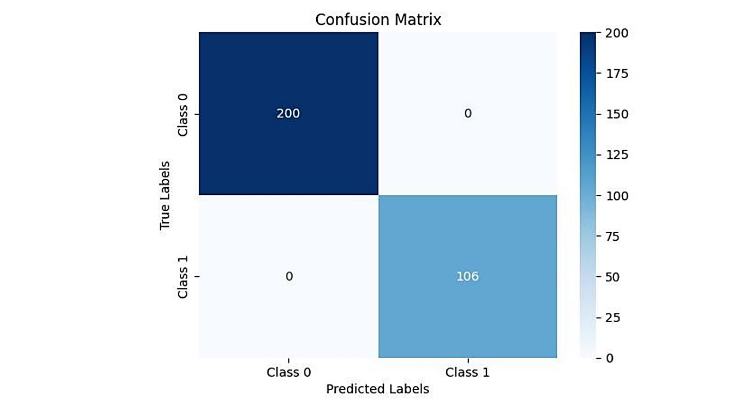
| Normal Skin vs Melanoma | 99.1% | 100% | 1.00 |
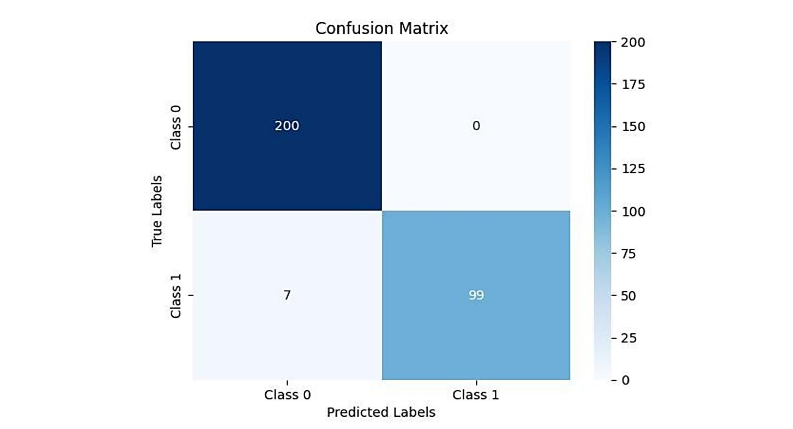
 L
LFigure 7. Convolutional neural network results developed to distinguish melanoma (1) from normal skin (0). Note the sensitivity of distinguishing melanoma from normal is 100% while specificity is 100%. Table 2 lists the results of sensitivity and specificity calculations as well the area under the operating curve (AUOC) predicted by the model.
RESULTS – CLINICAL SKIN CANCER
CLASSIFICATION TESTS
The clinical part of this study was focused on creating a rapid test to classify skin cancers using the OptoScope. While vibrational measurements are useful in defining the behavior of skin components, the 20 minutes required to collect the data was deemed excessive to be practical as a clinical test. Therefore, the use of gray scale images along with AI was adapted to classify skin cancers since the grayscale OCT images take only about 1 minute to collect and 2 minutes to run through the CNN models for different skin cancers. The resulting image is then automatically analyzed using the convolutional neural network model to obtain a probability of the lesion classification.
Figures 1 and 4 show OCT images of a BCC and a SCC, respectively. When we run these images through the CNN models, the following shown in Table 3 are obtained. The models correctly classify BCC and SCC images and indicate that they are not melanomas.
Once the model predicts the probability that the lesion is one of these classifications, the operator of the OptoScope presses the color-coding icon on the screen and the image is color-coded and broken into the green (low intensity pixels), blue (medium), and red (high intensity) pixels for visual review. This allows the physician to visually examine the lesion image and decide whether they can confirm the classification that lesion is a cancer based on the image loss in the green channel and a lack of a hyporeflective region in the blue channel. In this manner using both AI and the OptoScope image the operator can confirm the classification. In these cases the CNN model correctly classifies the images as BCC and SCC and gives a score of about 50% or lower for incorrect classification as a melanoma.
Table 3. Probability that the OCT images of Figures 1 and 4 are BCC and SCC based on the CNN Models
Image Type | BCC | SCC | Melanoma
BCC (Figure 1) | 98.5% | NA | 23.9%
SCC (Figure 4) | NA | 98.7% | 53.6%
Discussion
The growing numbers of skin cancers observed worldwide present a diagnostic problem for physicians already overwhelmed with identifying which skin lesions need to be treated immediately. Therefore, the need to develop alternative rapid technologies to facilitate lesion classification is an important technical problem. Many of these new technologies will involve digital imaging and the ability to transmit biopsy data over the internet. There are numerous advantages of developing new digital technologies that can be used with telemedicine in advancing dermatology practices. The long wait times, large number of biopsies conducted on benign lesions, the increased volume of patient lesions screened, and the inability to determine lesion depths noninvasively, has prompted the need for new technologies for skin lesion classification. The rapid growth of noninvasive digital technologies that can be used in conjunction with telemedicine offers increased sophistication, diagnostic speed, and accuracy. The ability to define the margins and depths of skin lesions noninvasively allows improved surgical efficiency and limits unexpected complications associated with margin uncertainties that prolong surgical times and require subsequent skin grafting procedures. The use of topical agents to treat superficial cancers in patients with head, neck, and scalp lesions will limit scarring and other complications and provide better satisfaction especially for patients who have had a negative experience in previous excisional surgeries.
In addition, Mohs surgeries can be facilitated by scanning the excised tissue from the patient while the frozen sections are being prepared for examination. Scanning the lesion base after the Mohs section is removed will provide an indication of any residual lesion without prolonging the surgical procedure. Once the lesion is judged free of cancer it can be debulked and sent out for dermatopathology to confirm the existence of clear edges. Vibrational optical cohesion is a new technique that provides basic biological information about the characteristic nature of skin cancers based on the proliferation of new normal cells with a resonant frequency (Rf) of 50Hz, new cancer associated fibroblasts (Rf=80Hz), new thin blood vessels (Rf=130 Hz), and fibrotic tissue (Rf=250-260 Hz). The Vibrational OptoScope studies provide basic information on the changes in the composition of the tumor stroma. This information is contained in the OCT images of cancers as changes in texture and physical arrangement of the lesion components. This information is contained in the gray scale OCT images and is indirectly extracted by the CNN model used to classify the lesion. The change in stroma organization as recognized by the CNN model leads to a high sensitivity and specificity with limited false negative predictions. The false positives observed are limited in number and do not lead to any missed classifications. Additional data collection will improve the sensitivity and specificity of the model’s predictions for all lesions including SCCs.
OptoScope images can be used as part of a telemedicine session. Gray scale OptoScope images can be collected by a trained assistant whose job is to correctly locate the lesion image. The instrument can then be run remotely over the internet by an expert who can correctly apply the CNN models to classify the lesion. Using this approach, large numbers of patients can be rapidly classified, especially in areas where Dermatologists are in short supply. The digital image is then available to be viewed by experts that can refer the patient for treatment. In cases where the scanning is done in a center where a trained nurse or physician’s assistant is employed, a shave biopsy can immediately be done and sent out for histopathology. Small superficial lesions that are identified as BCC or SCC can then be treated topically minimizing any delay between classification and treatment.
Conclusions
VOCT is a digital technique that identifies new cancerous cells, small friable blood vessels, and fibrotic tissues that are the hallmarks of epithelial cell derived skin cancers. Because of the length of time it takes to collect all the required vibrational data required for an in-depth analysis of BCC, SCC, and melanomas, a rapid AI based model of OCT grayscale images has been developed using a convolutional neural network. The grayscale image needed requires only about a minute to collect and then can be run through the CNN models to calculate a classification and the accuracy of the classification. The image can be collected and shared digitally for review by a trained physician and a referral for treatment can be made remotely or the lesion can be biopsied and treated topically. The results of this research suggest that digital images along with AI models can be used with telemedicine for remote classification of skin cancers facilitating treatment in areas where Dermatology visits are difficult to schedule.
Acknowledgements
The authors thank Professor Emrah Bayrak and the Capstone team at Lehigh University composed of Kendalin Flores, Max Tran, Ernesto Sanchez Lopez, Nico Babbio, and Julia Knox for their assistance in programming the convolutional neural network models. The authors would like to thank Drs Cindy Wassef, Gayathri Kollipara, and Amy Pappert for assistance collecting and reviewing the biopsies used in this study.
References
- Digital Biopsy Market Insights, accessed 8/23/2025.
- International Agency For Research on Cancer, accessed 8/22/2025.
- Key Statistics, accessed March 6, 2025.
- Negrutiu, M.; Danescu, S.; Popa, T.; Focsan, M.; Vesa, S.C.; Baican, A. Advancements in Basal Cell Carcinoma Diagnosis: Non-Invasive Imaging and Multimodal Approach. J. Clin. Med. 2024, 13, 39. doi.org/10.3390/jcm13010039
- Iannazzone SS, Ingordo V. Nodular basal cell carcinoma of the face successfully treated with ingenol mebutate 0.015% gel. Dermatol Pract Concept. 2018 Apr 30;8(2):129-131. doi: 10.5826/dpc.0802a12.
- Tan IJ, Pathak GN, Silver FH. Topical Treatments for Basal Cell Carcinoma and Actinic Keratosis in the United States. Cancers (Basel). 2023 Aug 2;15(15):3927. doi: 10.3390/cancers15153927.
- Fan Q, Cohen S, John B, Riker AI. Melanoma in Situ Treated with Topical Imiquimod for Management of Persistently Positive Margins: A Review of Treatment Methods. Ochsner J. 2015 Winter;15(4):443-7.
- Ahmady S, Nelemans PJ, Kelleners-Smeets NWJ, Arits AHMM, de Rooij MJM, Kessels JPHM, Essers BAB, Mosterd K. Surgical excision versus topical 5% 5-fluorouracil and photodynamic therapy in treatment of Bowen’s disease: A multicenter randomized controlled trial. J Am Acad Dermatol. 2024 Jan;90(1):58-65. doi: 10.1016/j.jaad.2023.09.001.
- Ferrante di Ruffano, L.; Dinnes, J.; Deeks, J.J.; Chuchu, N.; Bayliss, S.E.; Davenport, C.; Takwoingi, Y.; Godfrey, K.; O’Sullivan, C.; Matin, R.N.; et al. Optical coherence tomography for diagnosing skin cancer in adults. Cochrane Database Syst. Rev. 2018,12, CD013189.
- Silver, F.H.; Deshmukh, T.; Patel, A.; Dhillon, J.; Bobra, A.; Nadiminti, H. Rapid Noninvasive Skin Screening for Basal Cell Carcinomas using Vibrational Optical Coherence Tomography. Br. J. Cancer Res. 2025, 8, 747-755.
- Suneja T, Smith ED, Chen GJ, Zipperstein KJ, Fleischer AB Jr, Feldman SR. Waiting times to see a dermatologist are perceived as too long by dermatologists: implications for the dermatology workforce. Arch Dermatol. 2001 Oct;137(10):1303-7. doi: 10.1001/archderm.137.10.1303.
- Weinstein DA, Konda S, Coldiron BM. Use of Skin Biopsies Among Dermatologists. Dermatol Surg. 2017 Nov;43(11):1348-1357. doi: 10.1097/DSS.0000000000001188.
- Haleem A, Javaid M, Singh RP, Suman R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sens Int. 2021;2:100117. doi: 10.1016/j.sintl.2021.100117. Epub 2021 Jul 24.
- Reed M, Huang J, Somers M, Hsueh L, Graetz I, Millman A, Muelly E, Gopalan A. Telemedicine Versus In-Person Primary Care: Treatment and Follow-up Visits. Ann Intern Med. 2023 Oct;176(10):1349-1357. doi: 10.7326/M23-1335.
- Zhiyue Su, Chengquan Li, Haitian Fu, Liyang Wang, Meilong Wu, Xiaobin Feng, Development and prospect of telemedicine, Intelligent Medicine, Volume 4, Issue 1, 2024, Pages 1-9. doi.org/10.1016/j.imed.2022.10.004.
- Sud E, Anjankar A. Applications of Telemedicine in Dermatology. Cureus. 2022 Aug 7;14(8):e27740. doi: 10.7759/cureus.27740.
- Wolner ZJ, Yélamos O, Liopyris K, Rogers T, Marchetti MA, Marghoob AA. Enhancing Skin Cancer Diagnosis with Dermoscopy. Dermatol Clin. 2017 Oct;35(4):417-437. doi: 10.1016/j.det.2017.06.003.
- Jung JM, Cho JY, Lee WJ, Chang SE, Lee MW, Won CH. Emerging Minimally Invasive Technologies for the Detection of Skin Cancer. J Pers Med. 2021 Sep 24;11(10):951. doi: 10.3390/jpm11100951.
- Duniphin DD. Limited Access to Dermatology Specialty Care: Barriers and Teledermatology. Dermatol Pract Concept. 2023 Jan 1;13(1):e20230131. doi: 10.5826/dpc.1301a31.
- Silver, F.H.; Deshmukh, T.; Ryan, N.; Romm, A.; Nadiminti, H. Fingerprinting Benign and Cancerous Skin Lesions Using Vibrational Optical Coherence Tomography: Differentiation among Cancerous Lesion Types Based on the Presence of New Cells, Blood Vessels, and Fibrosis. Biomolecules 2022, 12, 1332. https://doi.org/10.3390/biom12101332
- Silver FH, Kelkar N, Deshmukh T, Horvath I, Shah RG. Mechano-Vibrational Spectroscopy of Tissues and Materials Using Vibrational Optical Coherence Tomography: A New Non-Invasive and Non-Destructive Technique. Recent Progress in Materials 2020; 2(2): 010; doi:10.21926/rpm.2002010.
- Silver, F.H.; Deshmukh, T.; Patel, A.; Nadiminti, H. Use of Optical Coherence Tomography Images to Differentiate Between Normal Skin, Skin Lesions, and Melanoma: A Pilot Study. J. Cancer Sci. Therapy 2024, 4, 1751.
- Silver FH, Deshmukh T, Nadiminti H, Wassef C, Pappert A, et al. Use of Optical Coherence Tomography images to Differentiate Between Normal Skin, Skin Lesions, and Melanoma: A Pilot Study. J Clin Med Img. 2024; V8(6): 1-11.