

Norepinephrine vs. Dopamine in Hemodynamically Unstable Patients
Comparative Study of Using Norepinephrine Infusion versus Dopamine in Hemodynamically Unstable Patients at Surgical Intensive Care Unit
Muhammad Naeem 1, Muhammad Saleh Khashkeli 2, Rafia Tabassum 3, Nasreen Kazi 4, Ghulam Muhammad Phul 5, Ashique Ali Arain 6
- MBBS, DA, MS (Anaesthesiology), Department of Anaesthesiology, Surgical Intensive Care Unit and Pain Center, Peoples University of Medical and Health for Women, Shaheed Benazirabad, Sindh, Pakistan
- MBBS, FCPS (Anaesthesiology), Professor and HOD, Department of Anaesthesiology, Surgical Intensive Care Unit and Pain Center, Peoples University of Medical and Health for Women, Shaheed Benazirabad, Sindh, Pakistan
- MBBS, DA (Anaesthesiology), Department of Anaesthesiology, Surgical Intensive Care Unit and Pain Center, Peoples University of Medical and Health for Women, Shaheed Benazirabad, Sindh, Pakistan
- MBBS, M. Phil. (Pharmacology), Professor and Chair Person department of Pharmacology, Bilawal Medical College, Jamshoro, Sindh, Pakistan
- MBBS, Phi (Physiology) Associate Professor, Department of Physiology, Gambat Medical College, Khairpur Mirs, Sindh, Pakistan
- MBBS, MCPS (Family Medicine), M. Phil (Pharmacology), Consultant Family Physician and Associate Professor of Pharmacology, Liaquat Institute of Medical and Health Sciences, Thatta, Sindh Pakistan
OPEN ACCESS
PUBLISHED: 3 July 2025
CITATION Naeem, M., Khashkeli, MS., et al., 2025. Comparative Study of Using Norepinephrine Infusion versus Dopamine in Hemodynamically Unstable Patients at Surgical Intensive Care Unit.
Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6720
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6720
ISSN 2375-1924
Abstract
Objective: This study evaluated the efficacy and safety of norepinephrine infusion versus dopamine in managing hemodynamically unstable patients in the surgical intensive care unit.
Methodology: This retrospective cohort study was conducted on patients admitted during 2021 and 2022. It was conducted at Peoples Medical College Hospital, Shaheed Benzirabad, Pakistan. The study included patients with hemodynamic instability, hypotension, and impaired tissue perfusion. The standardized protocol guided the administration of norepinephrine and dopamine, with doses adjusted according to hemodynamic goals and patient response.
Results: Patient records of 399 met the study criteria after reviewing the records. Among non-operative cases, 12.28% (n=49) patients received norepinephrine, while 46.37% (n=185) received dopamine. In post-operative cases, 6.27% (n=25) patients were administered norepinephrine compared to 35.08% (n=140) who received dopamine. In norepinephrine patients, 14.01% (n=16) were on self-ventilation, and 3.26% (n=13) required mechanical ventilation post-operatively, whereas, in the dopamine group, 8.77% (n=35) patients were on self-ventilation and 26.31% (n=105) on mechanical ventilation. Non-operative norepinephrine patients showed 7.02% (n=28) self-ventilation and 4.26% (n=17) mechanical ventilation, while dopamine patients showed 23.81% (n=95) self-ventilation and 22.56% (n=90) mechanical ventilation. Antibiotic use was higher in the dopamine group (76.19%, n=304) compared to the norepinephrine group (17.29%, n=69). Mortality was lower with norepinephrine (64.89%, n=48) than with dopamine (75.1%, n=244).
Conclusion: These results suggest that norepinephrine may be more effective and safer than dopamine, supporting its use as a first-line vasopressor.
Keywords
Norepinephrine, dopamine, vasopressor therapy, mortality, mechanical ventilation, antimicrobials.
Introduction
Hemodynamically unstable patients experience refractory, organ dysfunction, hypotension, and increased mortality rates. So, it is essential to select an appropriate vasopressor therapy to manage their condition. The death rate in patients with septic shock is 60-85% despite advances in basic care. Even though training boundaries exist, the ideal initial vasopressor for a patient in septic shock remains controversial. Various studies involving patients with vasodilatory septic shock suggest that the organization of fixed-dose vasopressin might be a viable salvage therapy with conventional catecholamines if the reaction to the agents is inadequate.
Septic shock is related to dangerous hypotension that doesn’t answer enough to fluid revival. Organ perfusion becomes compromised, prompting multi-organ dysfunction. Vasopressors are essential in reestablishing circulatory strain and keeping up with imperative organ capability. There are two widely used agents: norepinephrine and dopamine. It has been found that these vasopressors are used in the context of septic shock and other critical conditions. However, the optimal choice between these agents remains a topic of debate. Norepinephrine is a potent agonist consisting of alpha-1 and beta-1 receptors. It is frequently used in septic shock. It enhances systemic vascular resistance and blood pressure and increases tissue perfusion. However, norepinephrine’s effects on oxygen consumption and metabolic factors permit further study. Dopamine, another extensively used agent, acts on numerous receptors, including alpha-1, beta-1, and dopamine. Its hemodynamic effects are dose-dependent, with low doses primarily stimulating dopamine receptors and higher doses affecting alpha-1 and beta-1 receptors. However, concerns exist regarding tachyarrhythmias and adverse effects. This retrospective study compared the efficacy and safety of norepinephrine infusion and dopamine in managing hemodynamically unstable patients in the surgical intensive care unit (SICU).
Methodology
This retrospective cohort study was conducted on hemodynamically unstable patients admitted to the SICU at Peoples Medical College Hospital, Shaheed Benazirabad, Pakistan. The study’s ethical approval was received from the Institutional Bioethics Committee of the University of Sindh, Jamshoro, Pakistan (Reference No. ORIC/SU#122). Because this was a retrospective study, informed consent was not required. Data confidentiality was maintained throughout the study, and data was used only for research purposes.
The study included patients with hemodynamic instability, hypotension, and impaired tissue perfusion admitted to PMCH’s SICU. At the same time, subjects with contraindications to norepinephrine or dopamine, severe hypertension, severe cardiac arrhythmias, or those enrolled in other concurrent clinical trials were excluded from this study. A non-probability purposive sampling technique was used for the collection of patients admitted to SICU during 2021 and 2022. A predesigned study instrument was used to collect data from patient medical records. Variables in the questionnaire included the use of vasoactive therapy (norepinephrine or dopamine), patient status (non-operative and post-operative), antibiotics prescribed, ventilator support, type of discharge, and medical outcome (dead or alive). The standardized protocol guided the administration of norepinephrine and dopamine, with doses adjusted according to hemodynamic goals and patient response. This incorporates clinical qualities, hemodynamic parameters, blood pressure, and cardiac output. The primary outcomes included mortality rate, while secondary outcomes included ventilator support and antibiotics used. The collected data was tabulated in Microsoft Excel, coded, and exported to IBM SPSS Version 24. The categorical variables were presented as frequencies and percentages.
Results
The study results are presented in the form of tables and figures and discussed below.
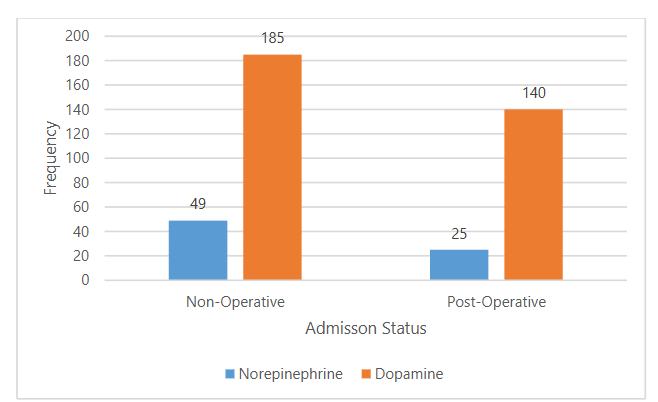
The distribution of patients according to their admission status (operative or non-operative) and the type of vasoactive therapy administered is shown in Figure 1. Among non-operative cases, 12.28% (n=49) patients received norepinephrine, while 46.37% (n=185) received dopamine. In post-operative cases, 6.27% (n=25) of patients were administered norepinephrine compared to 35.08% (n=140) who received dopamine.
| Vasoactive therapy | Type of Admission | Type of Ventilation | Frequency | Percentage |
|---|---|---|---|---|
| Norepinephrine | Post-operative | Self | 16 | 4.01 |
| Norepinephrine | Post-operative | Mechanical | 13 | 3.26 |
| Norepinephrine | Non Operative | Self | 28 | 7.02 |
| Norepinephrine | Non Operative | Mechanical | 17 | 4.26 |
| Dopamine | Post-operative | Self | 35 | 8.77 |
| Dopamine | Post-operative | Mechanical | 105 | 26.31 |
| Dopamine | Non Operative | Self | 95 | 23.81 |
| Dopamine | Non Operative | Mechanical | 90 | 22.56 |
Table 1 shows the frequencies and percentages of self-ventilation to mechanical ventilation cases among patients receiving norepinephrine and dopamine therapies in the SICU. For patients receiving norepinephrine, post-operative cases required self-ventilation in 14.01% (n=16) cases, while 3.26% (n=13) required mechanical ventilation. In non-operative norepinephrine-administered cases, 7.02% (n=28) required self-ventilation and 4.26% (n=17) mechanical ventilation, totaling 74 cases. In contrast, for patients administered dopamine, among post-operative cases, 8.77% (n=35) of patients required self-ventilation compared to 26.31% (n=105) requiring mechanical ventilation. While in non-operative dopamine administer cases, 23.81% (n=95) required self-ventilation, while 22.57% (n=90) necessitated mechanical ventilation, totaling 325 cases.
| Antimicrobial use | Norepinephrine | Dopamine |
|---|---|---|
| No | 5 (1.25) | 21 (5.27) |
| Yes | 69 (17.29) | 304 (76.19) |
| Ceftriaxone | 42 (10.53) | 227 (74.7) |
| Piperacillin + Tazobactam | 12 (3.01) | 41 (10.28) |
| Amoxicillin | 01 (0.25) | 10 (2.51) |
| Metronidazole (Flagyl) | 07 (1.75) | 09 (2.26) |
| Meropenem | 08 (2.01) | 08 (2.01) |
| Augmentin | 01 (0.25) | 03 (0.75) |
| Moxifloxacin | 02 (0.50) | 02 (20.50) |
| Cefixime | 01 (0.25) | 01 (0.25) |
| Cefuroxime | 0 (0) | 01 (0.25) |
| Penicillin | 0 (0) | 01 (0.25) |
| Vancomycin | 0 (0) | 01 (0.25) |
| Cefoperazone | 01 (0.25) | 0 (00) |
Table 2 shows the need for antimicrobial therapy among the patients receiving norepinephrine and dopamine therapies; for patients receiving norepinephrine, 17.29% (n=69) were administered antibiotics, while 5 (1.25%) did not require antibiotic. Among the antibiotics used in the norepinephrine group, Ceftriaxone was the most prevalent (42 cases), followed by Piperacillin + Tazobactam (12 cases). In the dopamine group, 304 patients (76.19%) were administered antibiotics, while 21 (5.27%) did not require antimicrobial therapy. Among the administered antibiotics, Ceftriaxone was again the most commonly prescribed (227 cases), followed by Piperacillin + Tazobactam (41 cases).
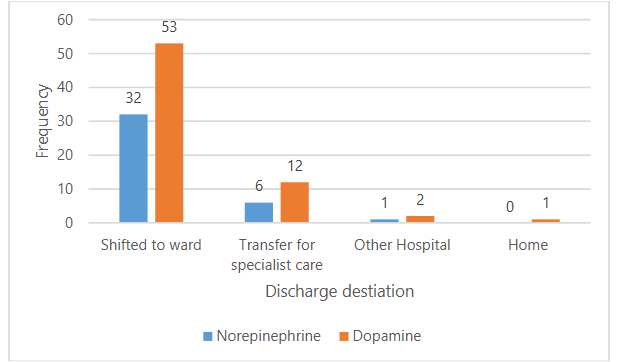
Figure 2 shows the discharge destinations of 107 patients who were discharged alive from the SICU. Among patients who were administered norepinephrine, 8.02% (n=32) were shifted to the ward among. Conversely, 13.28% (n=53) were moved to the ward for patients receiving dopamine.
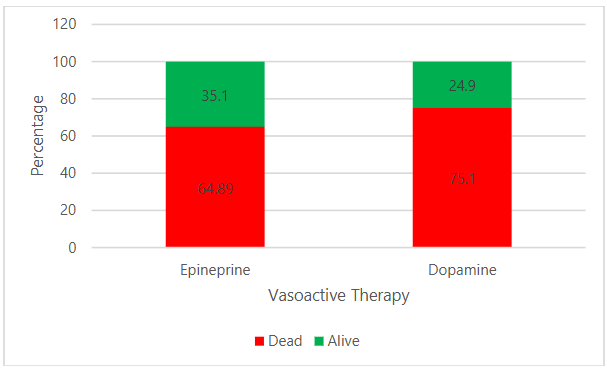
Figure 3 shows the primary outcomes based on dopamine and norepinephrine administration. Among patients administered norepinephrine, the majority (64.89%, n=48) were discharged as deceased, followed by 35.1% (n=26) discharged alive. Among patients administered dopamine, 75.1% (n=244) were discharged as deceased, followed by 24.9% (n=81) discharged alive.
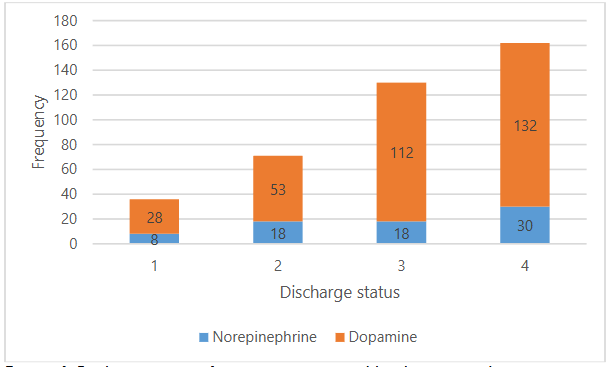
Figure 4 shows the discharge status of patients categorized by their surgical status (post-operative or non-operative) with the vasoactive therapy received (norepinephrine or dopamine). For patients receiving norepinephrine, among post-operative cases, 10.81% (n=8 cases) were discharged alive while 24.32% (n=18) were deceased, and among non-operative cases, 24.32% (n=18) were discharged alive while 40.54% (n=30) were deceased, totaling 74 cases. For patients administered dopamine, among post-operative cases, 8.61% (n=28) were discharged alive while 34.46% (n=112) were deceased, and among non-operative cases, 16.30% (n=53) were discharged alive while 40.16% (n=132) were deceased, totaling 325 cases.
Discussion
As such, the current study’s results help to inform our understanding of the relevance of vasoactive therapies in the identified hemodynamically unstable patients within the SICU. Analysis of norepinephrine and dopamine has exhibited differences concerning patient mortality, ventilator support, and antibiotic prescriptions.
In the current study, norepinephrine exhibited better outcomes than dopamine. While the application of dopamine at some time was considered noble considering its positive effects on renal perfusion, recent studies demonstrated that it is dangerous as it increases the incidence of arrhythmic events and mortality in some patient populations. The outcomes of the present study are in line with these concerns and recommend that norepinephrine may be safer; this is in line with the evolving clinical practice guideline that proposes the use of norepinephrine as a first-line vasopressor in septic shock patients.
A higher proportion of non-operated cases on dopamine than surgically operated cases indicates that dopamine therapy is more likely to be used in patients who are not operated. For this reason, dopamine is perceived as the first-line agent in treating hypotension and shock. Nonetheless, the reported higher mortality rates in patients in the dopamine group, especially in the non-operative subgroup, suggest that norepinephrine may be more effective than dopamine in the treatment of hemodynamic instability. These results conform to the evidence suggesting that dopamine may have unfavorable effects in cases of specific kinds of patients.
Regarding the ventilation tactics, the results suggest that patients who received dopamine more often relied on mechanical ventilation for one reason or another. This could indicate a worse severity of the clinical condition at the onset of the disease or the cautiousness of the clinicians in the exclusive use of respiratory support. Deciding when to use self-ventilation or to turn to mechanical ventilation depends on several factors, including the patient’s respiratory index, oxygenation, and prognosis. It is also possible that the prevalence of mechanical ventilation among dopamine-receiving patients could be in line with increased disease severity, which warrants such an intervention. This finding is in concordance with the literature because as the severity of shock increases, patients are more prone to develop complications that warrant interventions like jet ventilation. This work showed the value of promptly assessing a patient’s respiratory manipulation requirement to boost efficiency.
Markers of antimicrobial usage varied significantly by the group; patients receiving dopamine had substantially greater antimicrobial utilization, potentially reflecting a higher prevalence of infection or more liberal policies of antimicrobial prophylaxis in patients undergoing noradrenergic blockade. The selection of antimicrobials – Ceftriaxone and Piperacillin + Tazobactam- is based on the guidelines for empirical antibiotic therapy used to treat infections that occur most frequently in intensive care unit (ICU) patients. A high frequency of antimicrobial treatment aggregate dispensing, especially in the dopamine cluster, asserts specific questions about antimicrobial stewardship. In essence, with antibiotics, the likelihood of developing resistance causes a higher threat in the ICU environment. This study emphasizes the importance of prudent use of antimicrobials, which should be recommended and used based on culture results and/or clinical indication.
The mortality in the patients in the dopaminergic group indirectly highlights the fact that the use of vasoactive agents in patients should be done carefully, considering their effect on the patient’s overall survival. However, the study does not prove a cause-and-effect relationship but points towards comparing more specific characteristics when choosing vasoactive therapy. These highlighted concerns, most notably the high mortality rate among the patients on discharge and particularly receiving dopamine, should warrant the interconnection as a constant reminder of the severity of the conditions managed in the ICU. Of course, it is essential to note the possibility of selection bias: by definition, index patients with a 1-year mortality of 57% are sicker and, thus, presumably more likely to have received dopamine without actually being so because of it, therefore confounding the observed effect. Future studies need to try and isolate these factors to establish the exact role that the choice of vasoactive therapy plays in patient morbidity and mortality.
These results help elucidate whether managing patients with hemodynamic instability using direct or indirect vasoactive agents is more efficient. This points to the need to apply randomized controlled trials to better understand the effectiveness of the two drugs. Further, the conclusions emphasize the need to consider the individual patient’s characteristics and prognosis when managing ICU patients; this means that the treatment should be as individual as possible since the response to the therapy varies from one patient to another.
Conclusion
In conclusion, the study unveils an understanding of the crosslinks between vasoactive therapies, patient management, and overall clinical results. These results suggest that norepinephrine may be more effective and safer than dopamine, supporting its use as a first-line vasopressor. This study underscores the importance of individualized patient management and careful consideration of vasoactive agent choice to improve outcomes in hemodynamically unstable patients.
Acknowledgment
We are thankful to the hospital management and staff for cooperating and facilitation the carrying out this research work.
Conflict of Interest
There no conflict of interest among the authors.
References:
- Gupta S, Agrawal G, Thakur S, Gupta A, Wazir S. The effect of norepinephrine on clinical and hemodynamic parameters in neonates with shock: a retrospective cohort study. European Journal of Pediatrics. 2022;181(6):2379-87.
- Abd el Fattah Shaban A, Elsayed RM, Mohamed SG. Comparative study between the effects of arginine-vasopressin, norepinephrine or both on hemodynamics in catecholamine resistant septic shock. 2022;41(2):219-226.
- Lazzeri C, Bonizzoli M, Guetti C, Fulceri GE, Peris A. Hemodynamic management in brain dead donors. World journal of transplantation. 2021;11(10):410.
- Sharma K, Charaniya R, Champaneri B, Bhatia S, Sharma V, Mansuri Z, Panakkal BJ, Thakkar H, Patel K. Assessing the hemodynamic impact of various inotropes combination in patients with cardiogenic shock with Non-ST elevation myocardial infarction–the ANAPHOR study. Indian Heart Journal. 2021;73(5):572-6.
- Ahmad S, Khurshid A, Maqsood I, Arshad MS. Comparison of efficacy of dopamine versus epinephrine infusion in fluid refractory septic shock in a tertiary care pediatric ICU. The Professional Medical Journal. 2023;30(11):1456-60.
- Jentzer JC, Hollenberg SM. Vasopressor and inotrope therapy in cardiac critical care. Journal of Intensive Care Medicine. 2021;36(8):843-56.
- Michelle L, Bitner BF, Pang JC, Berger MH, Haidar YM et al. Outcomes of perioperative vasopressor use for hemodynamic management of patients undergoing free flap surgery: A systematic review and meta-analysis. Head & neck. 2023;45(3):721-32.
- Russell JA, Gordon AC, Williams MD, Boyd JH, Walley KR, Kissoon N. Vasopressor therapy in the intensive care unit. In Seminars in respiratory and critical care medicine 2021;42(01): 059-077.
- Grand J, Møller JE, Hassager C, Schmidt H, Mølstrøm S, Boesgaard S, Meyer MA, Josiassen J, Højgaard HF, Frydland M, Dahl JS. Impact of blood pressure targets on central hemodynamics during intensive care after out-of-hospital cardiac arrest. Resuscitation. 2024;1;194:110094.
- Berends AM, Kerstens MN, Lenders JW, Timmers HJ. Approach to the patient: perioperative management of the patient with pheochromocytoma or sympathetic paraganglioma. The Journal of Clinical Endocrinology & Metabolism. 2020;105(9):3088-102.
- Fabick AC, Hawn JM, Barwick KW, Weeda ER, Goodwin AJ, Bell CM. Comparison of extravasation events related to the peripheral administration of vasopressors prior to and following implementation of an institutional protocol. Journal of the American College of Clinical Pharmacy. 2023;6(7):709-17.
- Fabick AC, Hawn JM, Barwick KW, Weeda ER, Goodwin AJ, Bell CM. Comparison of extravasation events related to the peripheral administration of vasopressors prior to and following implementation of an institutional protocol. Journal of the American College of Clinical Pharmacy. 2023;6(7):709-17.
- De Backer, D., Biston, P., Devriendt, J., et al. Comparison of dopamine and norepinephrine in the treatment of shock. New England Journal of Medicine, 2010;362(9): 779-789.
- Schmidt, G. A., Girard, T. D., Kress, J. P., et al. Official executive summary of an American Thoracic Society/American College of Chest Physicians clinical practice guideline: liberation from mechanical ventilation in critically ill adults. American Journal of Respiratory and Critical Care Medicine,2015;191(1): 10-20.
- Kollef, M. H., Sherman, G., Ward, S., et al. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest,2008; 133(2): 483-494.
- Holmes, C. L., & Walley, K. R. Bad medicine: low-dose dopamine in the ICU. Chest,2013; 143(5): 1145-1150.
- Rhodes, A., Evans, L. E., Alhazzani, W., et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Critical Care Medicine, 2016;45(3): 486-552.
- Vincent, J. L., De Backer, D., & Wiedermann, C. J. Fluid management in sepsis: The potential beneficial effects of albumin. Journal of Critical Care, 2018;43: 211-217.
- Bassetti, M., Poulakou, G., & Ruppe, E. Antimicrobial resistance in the next 30 years, humankind, bugs and drugs: A visionary approach. Intensive Care Medicine,2018; 44(10): 1464-1475.
- Peake, S. L., Delaney, A., Bailey, M., et al. Goal-directed resuscitation for patients with early septic shock. New England Journal of Medicine, 2014;371(16): 1496-1506.