





Nurses’ Use of Learning Principles in Parent Education
Nurses perceptions and parents experiences of learning principles used within health education practice – an action research study
Dr Deryn Thompson PhD, MN, BN PC Allergy Nursing¹, Professor Jenny Fereday PhD², Dr Colleen Smith PhD (retired). Professor Esther May PhD³
ABSTRACT
Background: Patient/parent/family education (PPFE) commonly involves children’s nurses. They help parents to learn ─ interactively encode information, link new and existing knowledge, construct meaning and transform information to usable knowledge, building the skills to manage their children’s health/wellbeing. Ways nurses facilitate learning using Learning Principles (subjective/invisible practice aspects promoting deep thinking/metacognition) and which ones are important to parents learning are un-explained in nursing. Three action research cycles explored and mapped nurses use of Learning Principles within PPFE. This paper reports Cycles two and three ─ cycle one is published elsewhere.
Method: In Cycle two, Stringer’s Look, Think, Act approach within focus groups, involved nurses (n= 23) and parents (n= 8) from one Australian health network. Participants explored their perceptions and practice through interactive discussions and feedback ─ Look(ed). Look shifted to Think, as participants sorted their ideas, tested them against those of others, posed new questions, uncovered using and experiencing Learning Principles. Act involved stimulating nurses to draw up their tacit knowledge.
In a collaborative workshop (Cycle three), participants brainstormed, used creative, critical thinking and a decision-making matrix to determine the content and format to communicate those key Learning Principles used/experienced in PPFE to others.
Results: Cycle two’s thematic analysis coded Learning Principles nurses used/parents experienced to five themes. Shifting from automatic behaviours and knowing what would work, nurses made sense of theory/practice connections and ways they used Learning Principles important to parents needs. Mapped Learning Principles aligned with the Dimensions of Learning framework from educational psychology, a framework rarely integrated into nursing’s PPFE.
In Cycle three’s data synthesis, participants and the researcher identified ways to integrate the Learning Principles into a parent-education resource using the Dimensions of Learning framework. Cues guide nurses in ways cognitive and adult Learning Principles promote learners thinking (metacognition) in PPFE.
Conclusion: Mapping, describing and creating of a resource now shows how nurses use and parents experience Learning Principles in PPFE. Further research can determine the resource’s value in communicating the role of Learning Principles in the learning process ─ importantly, the information transformation process to usable, meaningful knowledge vital for self-management.
Keywords
Patient education, nursing practice, learning principles, health literacy, action research
INTRODUCTION
Patient or parent/family education (PPFE) is a responsibility of Paediatric nurses (PNs) and Child Health Nurses (CHNs). With no agreed universal definition, in this study, PPFE is: a shared learning process of collaborative, interactive teaching and learning opportunities that improve peoples’ health literacy and knowledge, build life-skills and support behaviour changes to enable parents to improve their families health and self-care.
Health-related information is conveyed in various modes, methods and styles, ideally at suitable health literacy levels for patients/parents of children needing care or support for health and well-being. Information provided by PNs and CHNs (hereinafter termed nurses, unless necessary to differentiate their roles), includes risk minimisation, care, treatments, management, and with the rising prevalence of chronic conditions, learning to gain long-term control. However, nurses must do more than provide information ─ the supportive PPFE process must encompass clinical reasoning and educative approaches that enable parents/families to use the information meaningfully. This involves them transforming information to usable knowledge needed to care for their children.
To use information meaningfully, educational psychology emphasises that learners are guided by facilitators (e.g., nurses) to enable the learning process, using a range of Learning Principles. Learning Principles (LPs) are the basic precepts comprising the foundations for people’s belief systems, behaviours and processes of reasoning, arising from research on theories of learning and knowledge. These Learning Principles involve cognition (thinking) and building knowledge, planning, reasoning, problem-solving and monitoring skills, which help learners to make appropriate decisions in their life situations. People make sense of their experiences, build their health literacy, and potentiate behaviour changes. Yet, for decades, healthcare directed nurses to use Knowles adult Learning Principles.
| Cognitive Learning Principles | Adult Learning Principles |
|---|---|
| contiguity (sequence) | the learner’s need to know |
| repetition, practice skills to retain and improve capability, helps the other learning stay alive | the self-concept or self-directedness of the learner |
| reinforcement, satisfaction upon improvement | prior experience of the learners |
| socio-cultural process of constructing meaning | readiness to learn |
| orientation to learning (meaningfulness) | active participation with the learner engaging motivation |
| relevance |
Knowles six principles are based upon adult learning or andragogy, as Knowles emphasised adults learn differently from children, and require different approaches. Yet, Knowles adult Learning Principles do not encompass the learner’s holistic world, their thinking (cognition), reasoning and problem-solving capacities, vital to transforming information to knowledge they can use long-term.
A literature review revealed health professionals descriptions of using Learning Principles were mostly implicit, disorganised, divergent in meaning, listed but did not explain using adult Learning Principles, and assumed learning took place. Interchangeability of terms teaching and learning, despite having different meanings, clouded clarity about how people learn within PPFE. Teaching describes the strategies/plans used by a person or group of people to influence others to learn. Learning, however, involves building a person’s thinking capabilities and behaviour changes. People interpret, reshape, rearrange information, transforming it to facts and usable knowledge. Old and new knowledge are linked, people become confident to adapt knowledge and skills when needed, as understanding builds critical and creative thinking capacities. Yet, ways nurses use Learning Principles to facilitate parents learning in PPFE present a gap in nursing literature, that this study sought to address.
RESEARCH AIMS AND OBJECTIVES:
A qualitative action research study aimed to identify, explore further and determine how nurses perceive, use and communicate their use of Learning Principles within PPFE. Objectives:
- to facilitate nurses to explore and describe how they use Learning Principles in PPFE.
- to facilitate parent exploration and descriptions of their learning experiences.
- collaboratively (researcher, nurses, parents) generate a resource to communicate how Learning Principles can be used in PPFE.
THE RESEARCH QUESTIONS:
- How are nurses using Learning Principles in PPFE?
- What is the evidence that nurses use Learning Principles in PPFE?
- What are parents experiences of learning during PPFE encounters?
- How can the use of Learning Principles be communicated to nurses and parents, to potentiate a practice change process?
A three cycle qualitative action research study collected data from May 2017 – August 2018. In Cycle 1, published elsewhere, observation of PNs, CHNs practice and parents learning experiences with a nurse revealed these nurses used various cognitive and adult Learning Principles aligning with those in Table 1. Yet, despite nurses knowing their PPFE practice worked, their individual interviews conducted one week after observations, revealed they struggled to explain what they did, or how they did it, believing their knowledge/skills were automatic or innate. Results aligned with Benner, who showed experienced nurses struggled to explain to newer nurses what they did in practice, as it was automatic. Benner argued nurses proficient, intuitive practice skills were based on deep background (tacit) knowledge and understanding, not automatic behaviours. Gustavsen highlighted deep knowledge and proficiency often go unnoticed, especially by health professionals, themselves, but ways of drawing up tacit knowledge posed unresolved challenges. Our results suggested that these nurses PPFE knowledge was subconscious (tacit), embedded within a shared understanding and clinical experience, but unexplainable to others. To encourage these nurses articulation of Learning Principles, they were asked to examine the member checking summary, in which participants checked for data interpretation accuracy. Importantly, this was also used to stimulate nurses deeper reflection on their PPFE practice. Nurses drew to their conscious thinking buried (tacit) Learning Principles, unarticulated in their interviews. Nurses brought their ideas to Cycle 2.
This paper reports on study Cycles two and three. In Cycle two, focus groups deeply explored, identified and mapped ways nurses used Learning Principles and those Learning Principles important to parents learning. In Cycle three, participants collaborated in a workshop to determine a resource content and format, capable of communicating to others those Learning Principles used in PPFE.
METHODS
THEORETICAL APPROACH
The interpretivist and social constructivism paradigms underpinned this study. Interpretivism involves researching in the natural setting of participants. The researcher (DT) was immersed in participants individual and group interactions (PPFE), seeing how they made meaning of their beliefs, lived experiences, social context and how experiences played out. Data interpretations are seen in the context of the environment in which they are formed, including the mind of the learner, as a nurse or parent.
Social constructivism’s premise is that a person’s mind initially creates reality and knowledge by making sense of their experiences within the world around them. When ideas create conflict, cognitive dissonance forces learners to resolve this conflict and gain knowledge. Learners build knowledge; their interactions enable them to test their ideas against those of others. The process of raising further questions promotes learning and knowledge building in both themselves, and those around them.
Stringer’s practical action research design:
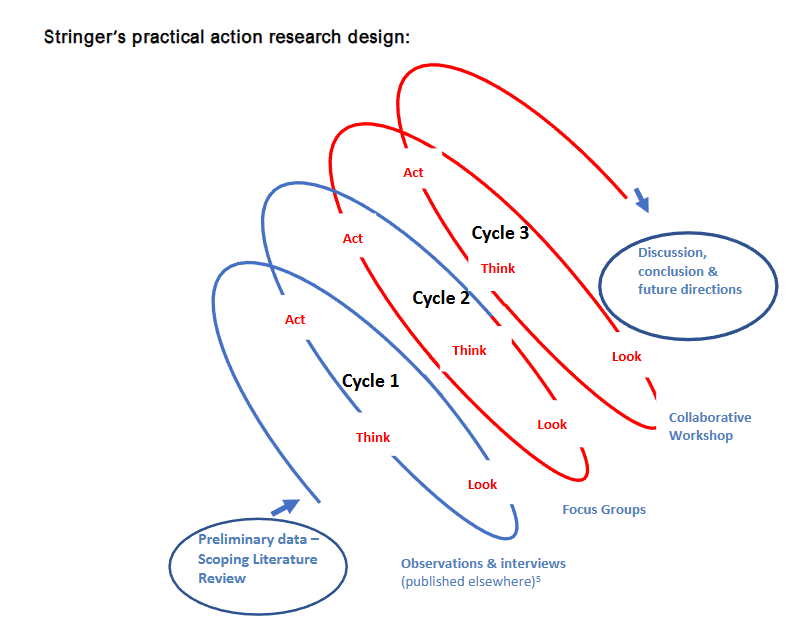
In Stringer’s model, Look involves collecting data about what one is seeing and hearing in situational contexts under investigation, to describe what is happening. Think is analysing the data collected in Look. Look and Think inform the Act implementing, assessing and reporting of the process of each cycle. Cycles of Look, Think and Act involved the researcher (DT) and participants revising, revisiting and reinterpreting findings, as they gained awareness and enlightenment during the research journey.
Cycles two and three suited this design and theoretical underpinning, for these reasons:
- Firstly, the divergent understanding and explanations of Learning Principles within the literature meant it was important that nurse and parent participants reflected deeply on their personal experiences with PPFE. Subjective and objective aspects of their knowledge could be brought to their conscious thinking. Reflective thinking pushed participants to question their existing knowledge boundaries, test their ideas against those of others, thereby building new understanding, including taken-for-granted or assumed aspects.
- Actively involving a community of people, engaged with PPFE, to each reflect upon and explore their lived experiences provides fresh opportunities for new perspectives, thus developing meaning and conscious awareness. Participants continue building knowledge, meaning and understanding from their discoveries in each cycle, working toward potentiating a change process.
ETHICAL ISSUES
Human Research Ethics approval was granted (HREC/17/WCHN/41) by the healthcare network. Approval was also granted from the healthcare network’s Research Governance body (SSA/17/WCH/045). All aspects of the study: recruitment, confidentiality, rigor, data collection, analysis and storage adhered to appropriate ethical approvals and human research codes, responsibilities and behaviours.
SETTING
The research was set in one major South Australian healthcare network, providing inpatient, outpatient (ambulatory) care and community services for women and for children (0-18 years) and their families. Two divisions of the healthcare network were involved:
- one where PNs provide inpatient/outpatient care services for children (0-18 years), with acute and chronic health conditions, and their families.
- the second, where CHNs provide community-based health promotional/parenting skills optimisation services for children 0-5 years, and their parents/carers.
PARTICIPANTS
A purposive sample of nurses and parents involved with the health network (inclusion and exclusion criteria) provided the rich data needed to gain a deeper understanding to build the meaning required to answer the research questions and meet research aims. Data richness and depth were important to this project, not generalisability.
| Paediatric (PN) & Child Health (CHN) nurses inclusion criteria | Parent inclusion criteria | Exclusion criteria |
|---|---|---|
| PNs working in the designated healthcare network, in either the hospital or community-based setting, providing education to parents of children in the ambulatory care setting, diagnosed with a health condition | CHN providing education to parents of children 5 years, using the community-based health promotional/care services | parents who needed the services of an interpreter in PPFE |
| 18 years of age | parents receiving education in the primary researcher’s nurse-directed eczema education clinic | |
| have command of English language and not require interpreter services | ||
| receiving education from a PN or CHN about caring for their children, aged 0 – 5 years, in the hospital or community setting |
RECRUITMENT
Information about the study was circulated in health network nurse online newsletters (with contact details to obtain nurse participant information sheets and consent forms), seminars (where hard copies were also available) and snowballing technique. For parents, flyers were displayed in the health network hospital and community clinics and circulated in patient newsletters, outlining the study and how to obtain further information and consent forms. Information sheets reassured parents their involvement or any decision to withdraw from the study would be unquestioned, would not compromise care or impact upon them as health network services users.
DATA COLLECTION
Data collection for Cycles two and three occurred via two different methods to aid triangulation: focus groups and a collaborative workshop. Data from Cycle two significantly informed Cycle three.
CYCLE 2: FOCUS GROUPS DATA COLLECTION
Five focus groups were held March-April 2018. Consensus, rather than universal agreement, suggests focus groups comprise between three and eight participants for manageability, while generating rich discussion.
| Participant PNs (N= 10) | Participant CHNs (N= 13) | Participant parents (N= 8) |
|---|---|---|
| Focus Group 1 PNs n= 7 | Focus Group 1 CHNs n= 3 | Focus Group 1: HBPas n=3 CBPas n= 5 |
| Focus Group 2 PNs n= 3 | Focus Group 2 CHNs n= 10 |
Nurses had a common professional understanding of PPFE and their practice within their health network, while parents had commonalities in understanding of parents PPFE encounters with nurses. Homogenous participants interactive discussions, questioning of themselves and others, aimed to unlock their interpretations and distinct knowledge about Learning Principles they did not realise they had and had struggled to describe in Cycle one. Participants needed to build new understanding and meanings. The focus groups occurred on different days to accommodate the nurses shift work and to optimise the clarity and accuracy of data collection and researcher reflexivity documentations. The semi-structured interview guide, which was piloted prior to the study, facilitated discussions.
| Participants semi-structured focus group interview guide a) Nurses | Participants semi-structured focus group interview guide b) Parents |
|---|---|
| 1. What are the tricks of the trade you use in practice to help parents understand and learn what they have to do, to care for their child? | 1. Please tell me about your experiences of how the nurse helped you to learn when I sat in with you in the encounter. |
| 2. How do you describe ways you build on parents knowledge & understanding using LPs? | 2. If there was a resource to help facilitate your learning from a nurse, what do you think it should contain or what it may look like? |
| 3. How do you recognise or evaluate parents understanding of what they learned? | |
| 4. Please describe any words you use when trying to explain to another nurse how you establish information provided to parents when you use LPs? | |
| 5. What is your particular trick for teasing out parents understanding? | |
| 6. How important are follow up appointments to establish parents understanding? | |
| 7. What are the key things (LPs) that facilitate the changes you just mentioned [in parents behaviours in caring for their child]? | |
| 8. You said some parents are more task-orientated in their learning. Can you tell me more about that? | |
| 9. You’re all describing similar skill sets for using LPs, although you use different words and descriptions. Has anyone seen a resource that would help describe these practice skills? | |
| 10. What are your ideas for a core /starting point for nurses to create a guide explaining innate parts of using LPs in your PPFE? | |
| 11. Did you have any more thoughts to share about LPs in PPFE? |
The primary researcher’s moderation and group communication skills (e.g., listening and body language observation) helped minimise the risk of individual group members domination or non-contribution to conversation and optimised participants focus on the topic. Focus groups risk that participants may not reveal certain but relevant information or divulge truthful accounts when with colleagues with whom they may not wish to share information. To reduce these issues a comfortable relationship between the participants themselves and between participants and the researcher was established. Participants were welcomed and the presence of a research team member (CS) explained ─ to take field notes on the group’s nuances, interactions/body language that DT may miss during the facilitation. Field notes can also confirm participants intent in their statements and improve data richness. The participant information sheet contents, the study purpose, audio-recording, data use, creating of a pseudonym for confidentiality and accurate linkage of comment/nuance data to the correct participant, study rigour, and participants right to withdraw from the study or leave the room at any time without repercussion were highlighted.
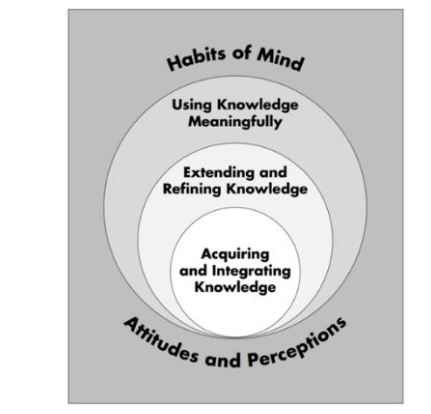
Initially, participants discussions, shared ideas and questioning comprised Look (explore). As discussions evolved, participants tried to sort their ideas, questioned further, reflected deeply and identified how key Learning Principles linked to their PPFE practice. They shifted continuously between Look and Think, deconstructing and reconstructing their knowledge and reshaping their ideas. When asked question 9 in the first CHN focus group, silence ensued. The CHNs knew of no resources explaining how to use Learning Principles. They could not suggest a possible starting point for creating a resource. This created a hurdle, as such data was needed for Cycle 3. Participants were then shown the Dimensions of Learning framework diagram. This framework helped clarify clarity Learning Principle descriptions in the literature review. The primary researcher asked the CHNs one extra question. What are your thoughts about this diagram? Lively conversations restarted, stimulating participants further Thinking. During the subsequent nurse focus groups, participants were also silent at Question 9. Figure 2 was shown, the question above asked. Lively discussions erupted.
When each focus group concluded, the date, time and location for the workshop, Cycle 3, were provided. An email would be sent to participants three weeks before the workshop. A member-checking summary, created as an infographic (which became the principle researcher’s Act for Cycle two), would be attached. Participants were asked to scrutinise the infographic to determine if data interpretation was true to participants intended meaning, and to stimulate further ideas on using Learning Principles and the content and format of a resource, possibly still innate knowledge. Infographics are logical, visual representations of information designed to engage those reading them. Infographics have successfully stimulated nurses deeper thinking and commonly aid understanding of complex healthcare information, through words and pictures.
RESEARCHER’S ACT FOR CYCLE TWO
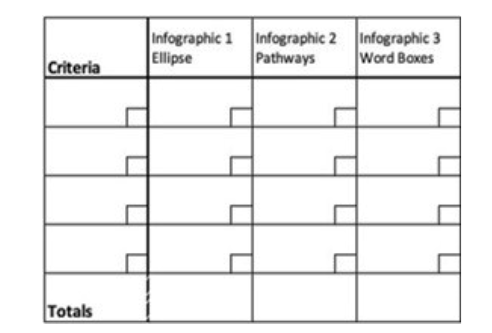
Three infographic formats to accommodate participants different learning styles: 1) an ellipse, 2) a learning pathway and 3) word box format (example shown in Figure 3) were created. Participants were asked to check the infographic for accuracy of data interpretation and participants intended meaning. While engaged, participants were also asked to think deeply (use metacognition) about their use and experiences of Learning Principles to stimulate (draw up actively) any ideas for creating a resource capable of communicating ways of using Learning Principles to other people. By involving participants, Thompson subconscious knowledge to their conscious thinking. The aim was for participants to link their retrieved knowledge to the collective focus group knowledge of the infographics.
CYCLE THREE: WORKSHOP DATA COLLECTION
A workshop involving nurses and parents working collaboratively, was held in August 2018 and comprised Cycle three. Workshops in healthcare can provide platforms whereby groups of homogenous adult learners can interactively gain and process new information, create knowledge, brainstorm, engage with problem-solving activities, create new ways of understanding and apply learning. Meaningful outcomes are achieved. The workshop used each of Stringer’s stages of Look, Think and Act enabling nurses and parents to collaboratively use different ways of thinking to generate ideas and contribute to resource content. The resource aimed to communicate what Learning Principles were and how to use them in PPFE.
Participants (n= 18: 6 PNs; 6 CHNs; 6 parents) were welcomed to the three hour workshop. No participants formally withdrew from the study. Data collection involved two stages. Stage 1 was based upon a rotating, interactive group engagement strategy ─ Jigsaw. This process facilitates diverse people within a collaborative learning environment to explore (Look), analyse, evaluate, discuss critically and appraise ideas created from significant volumes of information (Think), and then document the outcomes (Act). Participants formed teams of six [2 PNs, 2 CHNs, 2 Parents] at one of three worktables. Each member contributed their ideas on using and communicating key Learning Principles through a resource. On each worktable were the infographics, a Dimensions of Learning framework placed centrally on the large paper sheet (760 x 510mm/30 x 20 inches), felt tipped pens, A4 blank paper and sticky notes. Participants spent 20 minutes at each table, discussing and documenting ideas, writing their ideas on sticky notes and placing them adjacent to each of the Dimensions of Learning headings. After 20 minutes, five of the six people on the table rotated to the next worktable. One person remained as a spokesperson to explain the teams work, so far, to the five new people, who then explored, discussed, analysed, appraised further and documented their ideas. This rotation approach was repeated after 20 minutes, ensuring the first spokesperson moved to a new worktable. Each person’s information fits together like a jigsaw puzzle, with the rotating of people stimulating new ideas to create a more comprehensive picture of using and communicating Learning Principles in PPFE. The technique has been used in nursing studies, where collaborative learning processes built and shaped new knowledge. Hard copy materials, comprising the output of these activities/participants ideas, were photographed at the workshop’s completion and uploaded to NVivo 12, ready for data synthesis.
| Marzano et al. Dimensions of Learning framework |
|---|
| 1. Attitudes and perceptions: readiness, a positive attitude to learn, influenced by internal situations (e.g. emotions), safe learning environment, learners see value, relevance of the learning, clearly defined learning goals, motivation. |
| 2. Acquire and integrate knowledge: understand strategies for linking new knowledge to existing knowledge, organising, processing, storing knowledge for later retrieval and use – declarative knowledge (facts) and procedural (practical) knowledge, shape, internalise skills to use later. |
| 3. Extend and refine knowledge: strategies include: comparing, classifying, making inductions, deductions, analyse perspective, correct errors, apply reasoning, gain perspectives; use analogies. These processes help learners deconstruct and reconstruct knowledge. They can think of their new knowledge and skills in new and unusual ways. |
| 4. Apply the knowledge meaningfully: strategies include: decision-making, problem solving, analysis. |
| 5. Habits of mind: thinking and learned skills become part of everyday life; learners master critical, creative, self-regulated thinking, operate autonomously. |
The second stage of workshop data collection engaged participants in Think and Act, with each participant undertaking a decision-making matrix exercise, where participants were required to deconstruct their knowledge and reconstruct it using their thinking skills, by rating each infographic according to the criteria they had decided were most important to learning within PPFE. No prescriptive options on the matrix ensured data were participants ideas. Each participant ranked their criteria in order of their importance to the participant, numbering them accordingly, down the left side of the matrix sheet. For example, if participants identified five criteria, they were ranked 1-5, with the most important ranking 5. Across the top of the matrix were the names of the three infographics described above. Participants then rated each of the three infographics against each of their recorded criteria, with 3 being the one that satisfied that criterion best.
Disadvantages of workshops to collect data are that interactions may create power-relations, imbalances between participants or their non-engagement. Potential power imbalances were recognised and mitigated through clear explanations, creating relationships over the study between the principal researcher and participants, and actively engaging participants in activities.
DATA ANALYSIS
CYCLE 2
The audio-recordings were transcribed verbatim, capturing nuances, sounds or gaps in conversation that may indicate participants deep thinking, reflection or struggles to articulate their thoughts/knowledge on Learning Principles. Braun & Clarke’s six step thematic analysis approach guided data analysis.
| Six steps of thematic analysis |
|---|
| 1. familiarizing themselves with their data |
| 2. generating the codes systematically across the data set, collating data to each code |
| 3. searching for themes from the collated data and collating data to those potential themes |
| 4. reviewing the themes, checking that data relevant to each theme is coded |
| 5. defining and naming the themes, and determining their story |
| 6. writing communicating findings, weaving together narrative and data contextualising analysis to existing literature and the research questions |
Transcriptions and the field notes were read in full by the principal researcher while simultaneously listening to the audio-recordings, for clarity and greater context. Words identifying participants were removed, transcriber mis-interpretations corrected, missed or unclear comments clarified or documented as [unclear: time], amended where possible or noted as [inaudible: time]. Such corrections are possible when the same person collects and analyses the data. Data were then exported to computer-assisted qualitative data analysis software, NVivo version 12, to assist with data management. NVivo software enables engagement with and building knowledge by categorising (coding) the data, searching, shaping, modelling and looking at relationships between data. NVivo enables each participant to be a unit of analysis ─ a case was created for each participant and data linked accordingly.
Throughout the analysis process, the primary researcher created a continuous memo, recording notes on any ideas forming and the interpretation stages of the study. During the data familiarisation phase, memos and entries in a reflexive diary helped the researcher and the supervisory team to recognise any preconceived ideas about Learning Principles and PPFE, assisting study rigour. Cycle 2 data were divided into categories soon after collection, codes generated complete coding, enabling data to build meaning as the study gained momentum and incoming data were analysed. Data were stored as nodes in the quest to describe how the participating nurses used Learning Principles and ways parents experienced learning with a nurse in PPFE. Each node was named. A brief description outlining the node’s subject matter helped add clarity to the supervisors checking of the researcher’s data interpretation and node naming at different timepoints during thematic analysis, creating transparency in the process. Data not fitting into nodes early in the analysis or seeming unclear, were coded to a spare node, should they develop relevance as the analysis progressed.
Throughout the analysis and as understanding developed, initial codes were revisited, modified or amalgamated when similarities were noticed, and newer data fitted into existing nodes. Hierarchical or parent nodes contained sub-headings where appropriate, helping to elucidate deeper information and meaning, relevant to the initial node. After the coding, patterns in the data guided theme development, reflecting core and reoccurring concepts identified through the analysis. For clarity in thematic analysis comment attribution, parent abbreviations in this paper are: Community-based Parents (CBPa) and Hospital Based parents (HBPa).
DATA ANALYSIS CYCLE THREE
Hard-copy data of workshop’s group work written on paper sheets and the field notes were transcribed on the day of the workshop for accuracy, with worktables data read in full. Photos, scanned copies of matrices, field notes and data summaries from each worktable were entered into NVivo 12, safeguarding data accuracy. The Dimensions of Learning Framework, that aligned significantly with the Learning Principles nurses used and were desired by parents in Cycle 2, formed the framework against which the workshop responses were coded. Each dimension became a node. This approach also created clarity on the meaning of each node, aiding the supervisory team to cross-check and discuss and reach consensus on any ambiguities of synthesised data. Synthesised data reflected the ways nurses used Learning Principles and those parents believed were vital for effective learning. These data informed the content and format for a resource to communicate ways Learning Principles were used to other people.
RESULTS
CYCLE 2 FOCUS GROUPS
Five themes were formulated: 1) establishing parents understanding; 2) barriers and enablers to using Learning Principles; 3) assumptions ─ expectations of nurses knowledge about learning; 4) practice paradoxes and 5) using Learning Principles – knowingly connecting to practice.
THEME 1: ESTABLISHING PARENTS UNDERSTANDING
Building parents understanding represented LP use and was a goal of nurses PPFE and desired by parents. However, this was complex.
Nurses descriptions Initially CHNs (3/13; 23%) and PNs (3/10; 30%) stated their use of Learning Principles was innate with an informal evaluation of parents learning/understanding, via verbal feedback: Yes, that is a good question. I think we do it without analysing it… (CHN 47).. Discussions shifted when PN (57) described their ordered approach: teaching using a [specific device] involves demonstration, show the video, explain more, then set each parent a scenario. Ask the parent…What are you going to do? A second scenario will show their real understanding. The parent is feeding back to me that they have understood (PN 57).
Mention of scenarios led nurses to then question whether the Teach-back protocol (parents rephrasing what was said) really did establish understanding. There seems a belief that all nurses interpret/execute Teach-back consistently. However, establishing understanding, as a subjective PPFE aspect, like learning, was very unclear and interpretations inconsistent: that’s the thing, it’s never proven. You write all these good things about learning, but when compared to a randomised control trial [practice] doesn’t capture all the fuzzy stuff (PN 69).
Deeper reflections also raised concerns about tick-box documentation of parent understanding of what care they must perform, e.g. on a discharge list, did not show understanding: they may have understood while you’re in front of them but do they understand it in a week’s time? (PN 58). Each nurse would also have a different interpretation of tick-box meaning. Yet, parent understanding could be still lacking, impacting parents subsequent care of their children: she presented the child too late to hospital there was much guilt. When she talked to me, she did not even know the different medication devices the child was with the specialist for three years but they never got the nurse to help (PN 69).
Tick-boxes potentially limited newer/inexperienced nurses PPFE skills development, with them potentially not revisiting parent understanding at each encounter. Even experienced nurses clinical judgement skills could be eroded if relying on tick-boxes: tick-boxes should be conversation starters, not something that closes communication loops, once ticked. The tool is only as good as the person using it…you’ve got to have the knowledge and experience to interpret stuff (PN 707). what happens is the people that used to think, no longer need to. are we really helping ourselves and our patients long-term?… with tick-boxes (PN 53).
PARENTS DESCRIPTIONS
Parents of children with complex issues also found nurses use of tick-boxes unsatisfactory: the nurse checked everything off in the questionnaire, asked me questions all tick-boxes. Often, they don’t need to be more complicated than a tick-box, I know he’s doing well. But I wasn’t mentally. I needed some help. I needed a strategy (CBPa 84).
THEME 2: BARRIERS AND ENABLERS TO USING LEARNING PRINCIPLES
Barriers and enablers within PPFE practice and parents experiences also reflected the nurses use of Learning Principles.
BARRIERS
Nurses descriptions Documenting and listening to parents simultaneously challenged nurses Learning Principles use. Parents psychosocial issues meant nurses drew on different Learning Principles for each situation: If I’ve got a distressed mother, the face is telling me something different from what the lips are telling me. So, it’s flexibility. Having that understanding that it’s not okay now to sit documenting for 20 minutes. While she’s talking, I miss what she’s saying (CHN 76).
The time taken to build/establish parents knowledge, skills and understanding took longer time than just exchanging information. Follow-up appointments were essential, but the health network’s unrealistic patient consultation target expectations discouraged follow-up. When parents previously received incomplete/incorrect information from other health professionals, their children’s treatments or wellbeing were compromised. Unsatisfactory PPFE meant nurses must help parents to rebuild confidence in themselves: I get them to go through what happened, ask if they had any education before, has anyone taught them about these things ask the parent to go through what happened what did they learn from that situation? You can assess what level of understanding they have for what happens in my specialty then you can then start (PN 69).
Parents who felt vulnerable were overwhelmed if nurses provided too much information: You often have to wade through the emotional side of things before you can actually get down to the nitty gritty (PN 53).
PARENTS DESCRIPTIONS
Incomplete/incorrect education in previous PPFE encounters, nurses not identifying parents existing knowledge, not listening, providing too little/too complex information and no explanations or practical demonstrations of what to do affected their learning: their assumptions that you know something, because you’re in the system. You may have missed that step, or no one told you that step because, you see different people along the way (HBPa 96).
ENABLERS
Enablers represented the activities/aspects of nurses practice that supported learning. Descriptions implicitly expanded upon ways nurses used Learning Principles.
NURSES DESCRIPTIONS
Nurses who listened aided learning some [parents] have said they know who will listen to them, and [they] come back because somebody would listen and took time (CHN 91). CHNs valued interdisciplinary collaboration. Acquired information and skills from colleagues helped professional development, and implicitly broadened skills use of Learning Principles: the input we have from psychologists, social workers much more trained in mental health and relationships. That’s invaluable Without them we would not be as knowledgeable and able to work successfully with our clients (CHN 97).
PARENTS DESCRIPTIONS
Parents valued a positive learning environment, trusting nurse/parent relationships, seeing the same nurse each time to build confidence, especially if they were vulnerable: that relationship that’s developed her openness for me to be vulnerable, has led to a better education experience for me (CBPa 81).
Detailed, but straightforward explanations of health conditions, demonstrations of skills needed, given in small steps were vital to parents, and confirmed nurses Learning Principles use: if you are talking about creams, they quantify the information. How much I need to put on, what direction I apply, what other brand I use if this one doesn’t work the next best option? How do I bath him? It’s really specific to start with. If this plan does not work, I know I’ve tried it…I can evolve to a new one They give you ideas relax you (CBPa 85).
Care plans nurses created, which are a series of cues, supplemented by verbal explanation and support, helped parents grasp what to do: If I don’t understand something, or if something else comes up I can text her. In some ways, like the written information if something is fallen out of your head afterwards, you know you can double check things (CBPa 81).
More frequent clinics were preferred, where parents received less information, but could better understand and use what transpired. Once their learning made sense to them and skills became automatic, parents felt capable and ready for discharge.
THEME 3: ASSUMPTIONS ─ EXPECTATIONS OF NURSES KNOWLEDGE ABOUT LEARNING
The nurses recognised some PPFE aspects and Learning Principles use were based upon assumptions, rather than evidence. Sub-themes were 1) organisational assumptions, and 2) expectations of knowing.
3.1 ORGANISATIONAL ASSUMPTIONS
The nurses realised their health network assumed nurses had pre-existing PPFE skills and prior training, especially those with post-graduate qualifications: we’re just expected to know it and do it (PN 54). No nurses recalled dedicated Learning Principles training opportunities. Multiple annual mandatory training requirements were barriers to nurses attending non-mandated courses. Dedicated training was absent and a resource for using Learning Principles was overdue. Field notes showed other group members nodded in agreement: If you can’t explain it to someone else, you don’t understand it enough (PN 707); If minimal professional development is undertaken, practice becomes stale (CHN 98).
3.2 NURSES OWN ASSUMPTIONS ABOUT LEARNING
Participating nurses could not recall how they built their professional knowledge/skills in using Learning Principles. Nurses assumptions, made about their own Learning Principles and PPFE skills being innate/automatic, shifted to being a lack of conscious awareness: I don’t think there’s a gap that we’re not doing it the gap is we don’t acknowledge we’re doing it we do it every single day. We’re actually not aware that we’re doing it or thinking of it in that context (CHN 79).
THEME 4: PRACTICE PARADOXES
Contradictions arose between what nurses believed was expected of them in PPFE and what they carried out. Theme 4, Practice paradoxes comprised two subthemes 1) the nurse cannot be the expert, 2) parents choice versus nurses opinion.
4.1 THE NURSE CANNOT BE THE EXPERT
Nurses revealed a dilemma about not being seen as experts by parents. The expert label implied power imbalances conflicting with the person-and-family-centred care and partnership approaches required by the health network. Situations whereby nurses looked in power or parents felt disempowered were avoided: you are not in a position of power, you, drop lower than them, so the patient has a position of power. I drop my voice too… (PN 53).
One nurse mooted a way to consider conflicted feelings: I think it’s important that they see us as an expert so they can trust us in that way, but we need to be approachable experts (CHN 56).
4.2 PARENTS CHOICE VERSUS NURSES OPINION
Contrastingly, participating parents wanted nurses to have extensive knowledge/expertise to help them learn to do things correctly to build confidence and capability to care for their children. Another paradox was when nurses encouraged parents to become decision-makers as they learned in a partnership. Open-ended questioning created simple, practical ways of encouraging parents to take on their share of learning and decision-making and represented implicit use of Learning Principles in practice. Despite nurses encouraging shared partnerships, parents often wanted specific directions: if that was what the client wanted this is acceptable (CHN 76). Also, a psycho-socio-cultural situation of parents required nurses sometimes to provide direct advice to optimise children’s care and safety, with situations reassessed next visit.
THEME 5: EVOLVING LEARNING PRINCIPLES
Discussions revealed these nurses were using many Learning Principles within PPFE before seeing clear links to the Dimensions of Learning framework on sighting the diagram.
5.1 USING KEY LEARNING PRINCIPLES KNOWINGLY CONNECTING TO PRACTICE
Dialogue and nurses body expressions (e.g. raised eyebrows; smiles), documented in the field notes, reflected nurses increasing awareness that they used a vast array of Learning Principles in practice: it makes more sense (CHN 69). Nurses all recognised parents brought existing knowledge to each educational encounter, influencing parents linking of their new and existing knowledge: It’s identifying what people know then building on that (CHN 47).
Parents felt valued and willing to learn in interactive learning partnerships. Parent-education practice, straightforward language, was likened to unpacking the box of what people know, do not know and need to know and learn: demonstration really helps to see what capabilities are there, what can be achieved, if it needs to be changed, and following up in a week or two (CHN 88).
Key Learning Principles with cues for parents to recognise changes in their child were vital: I will go from top to toe; what parents need to look for in [condition] what their [child’s] voice might sound like…where you look to see if their breathing is getting worse, lift clothing up. I give a visual description to parent what’s improving what makes me feel worried…things parents can identify with…I explain with a rationale, why I got the child to count to 10 quickly, what it did to their breathing. That way parents learn what is normal and what’s a worry…what signs make me think their child is getting worse, e.g., getting very tired, or sleepy (PN 53).
Nurses frequently used cues to stimulate learning throughout all encounters. These were greatly valued by parents (e.g. in care plans, nurses explaining how to use the plans, having parents explain back what they learned through a scenario, answering open-ended questions nurses posed, and using analogies to explain/clarify information, gauging parents understanding of what was learned) represented Learning Principles these nurses used to build parents knowledge, skills and confidence to provide care at home: I get clients I see frequently to write a list of questions at the end of each visit. I evaluate next visit, by going back to the questions. Have they answered them all? achieved them? It’s just a framework to start them talking, really focusing on what they really want and need… (CHN 84).
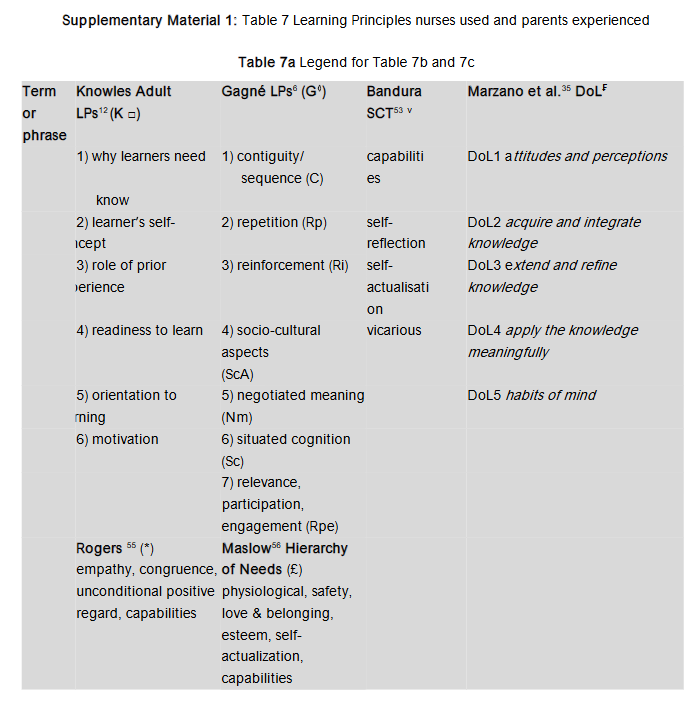
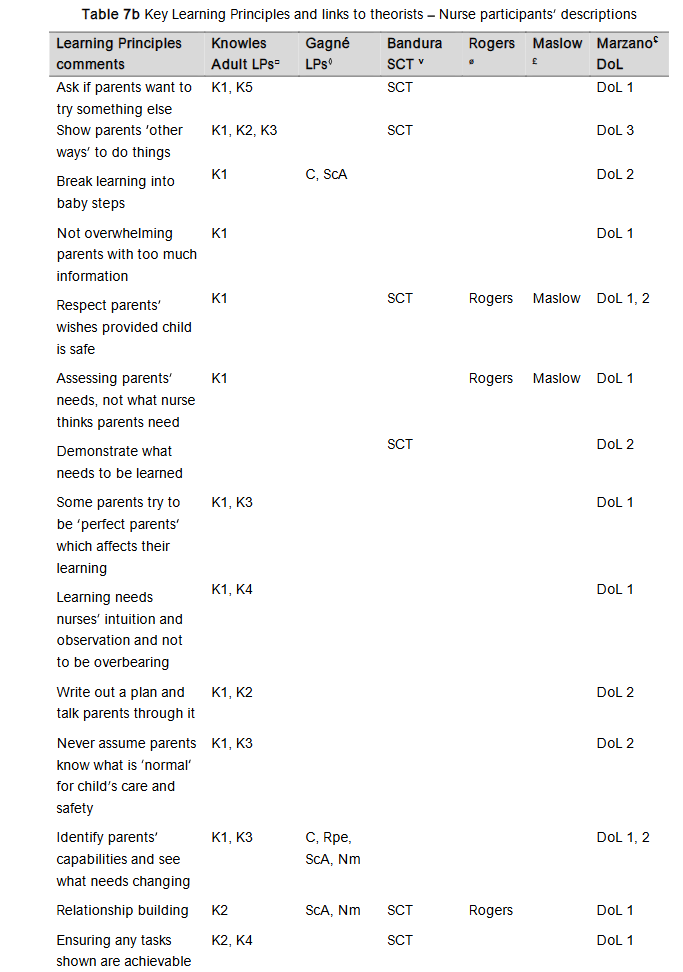
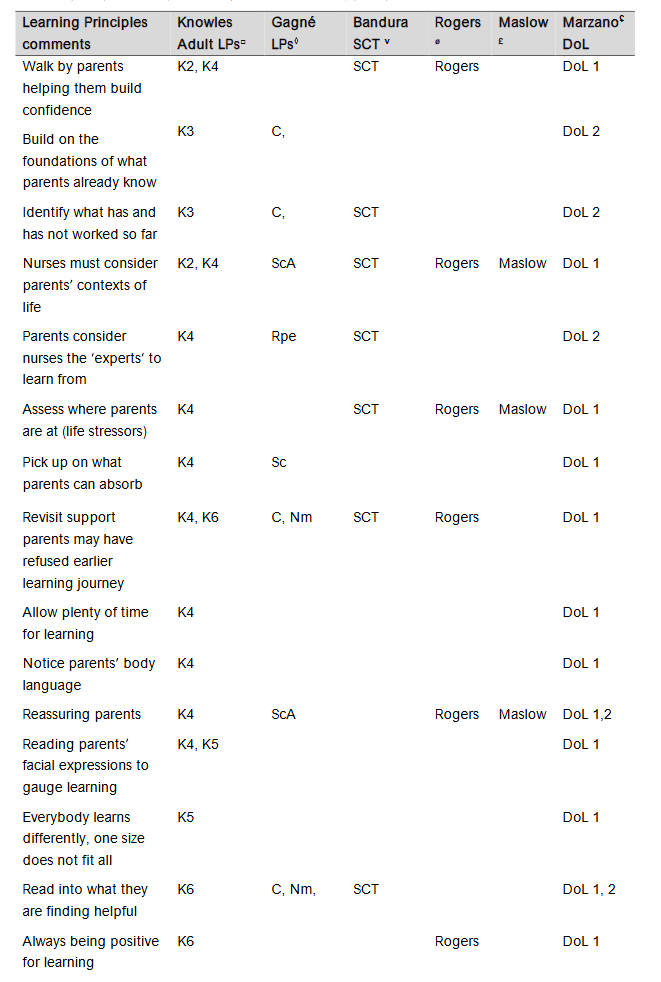
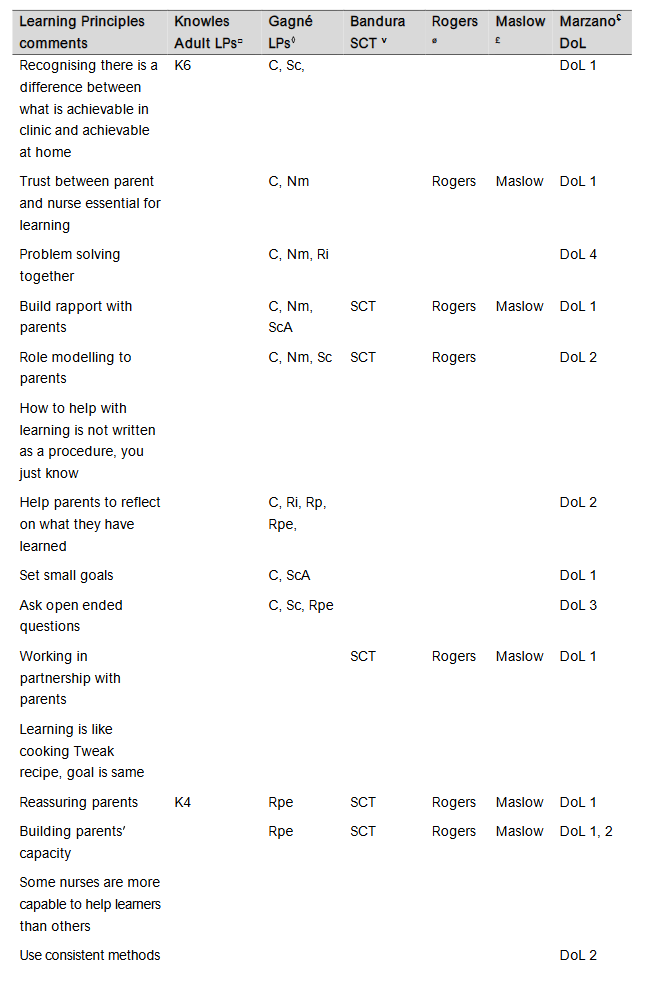
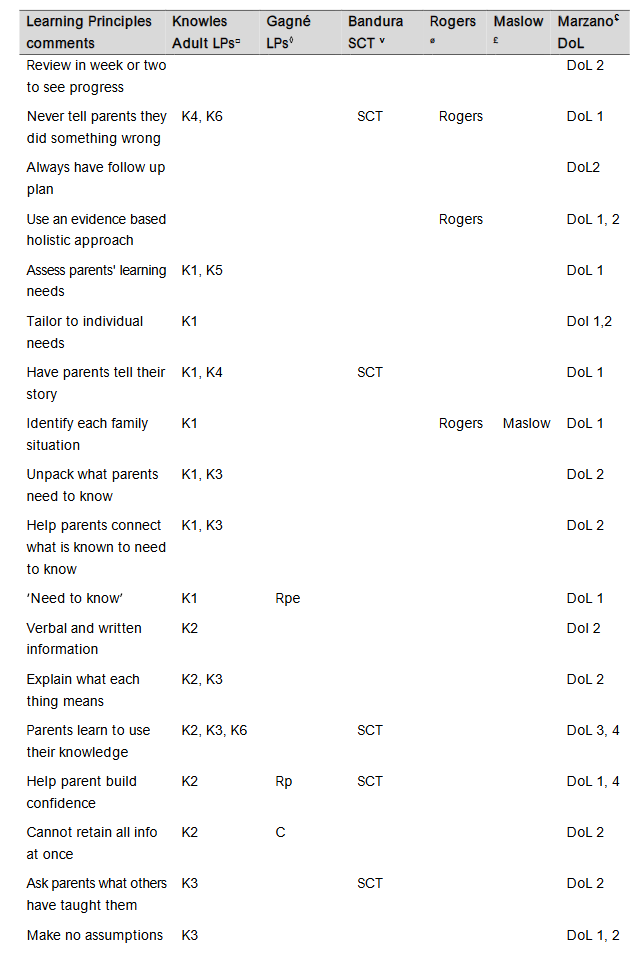
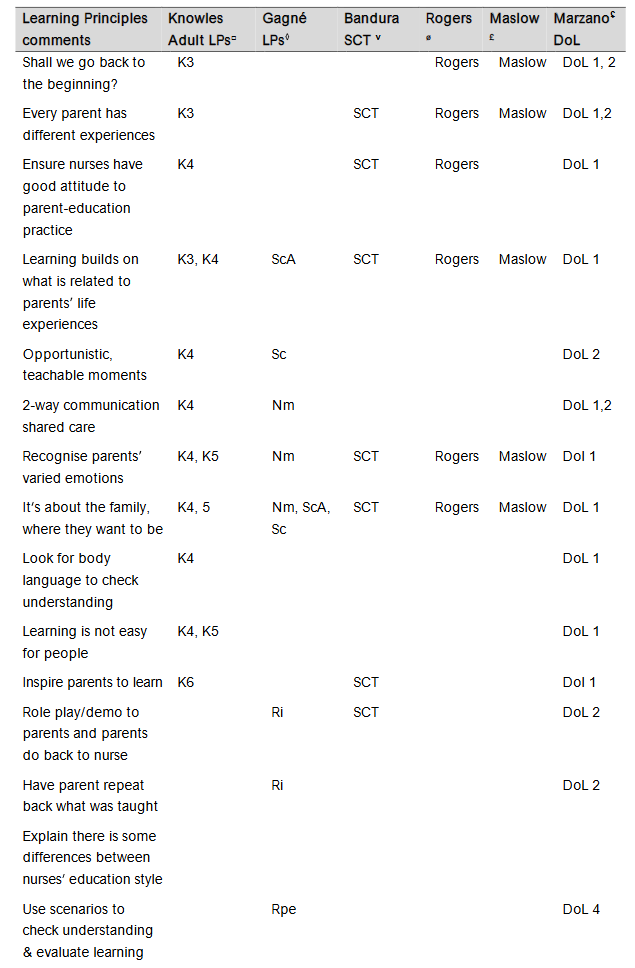
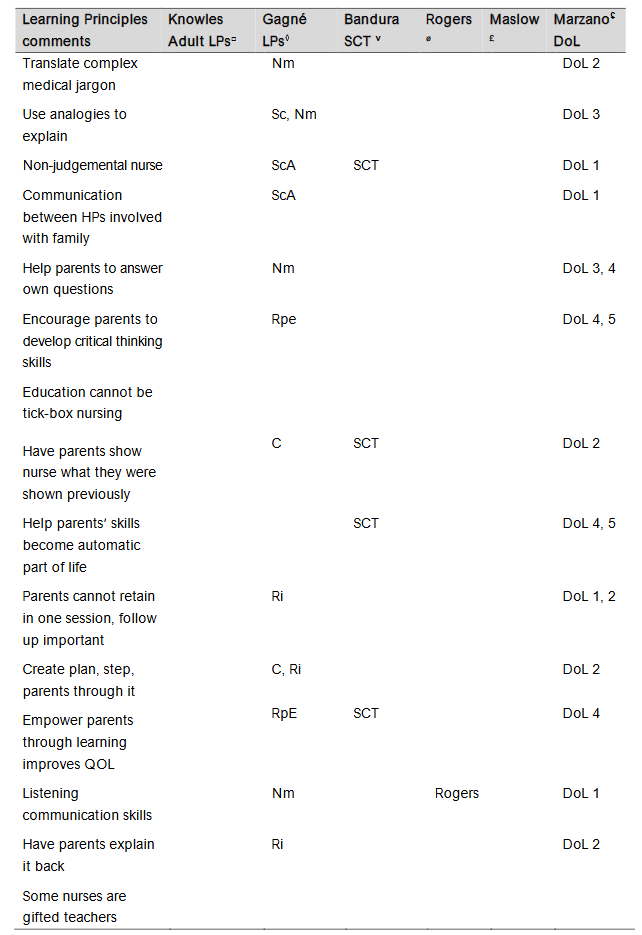
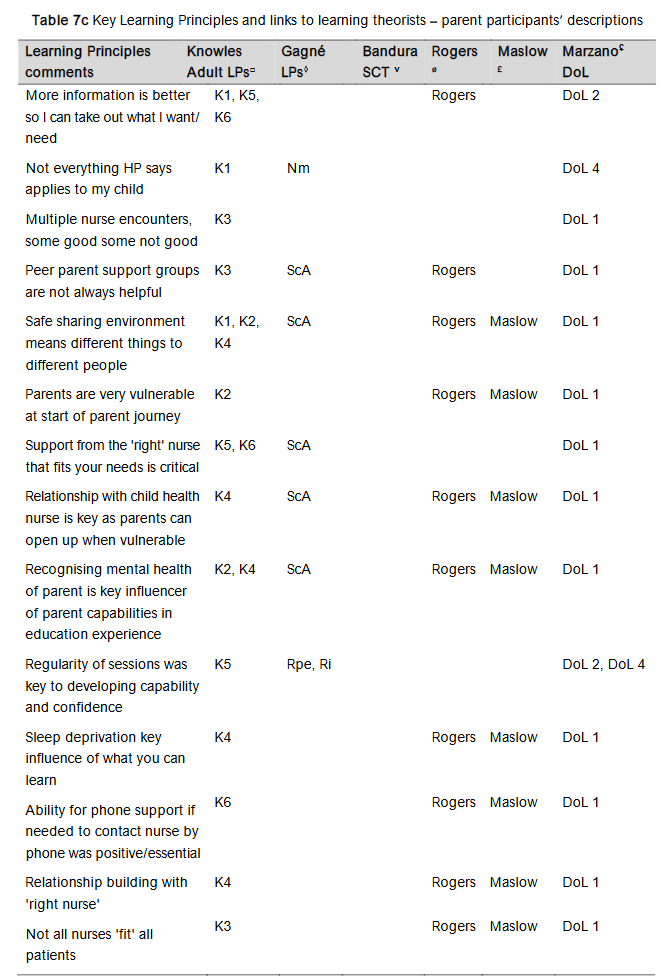
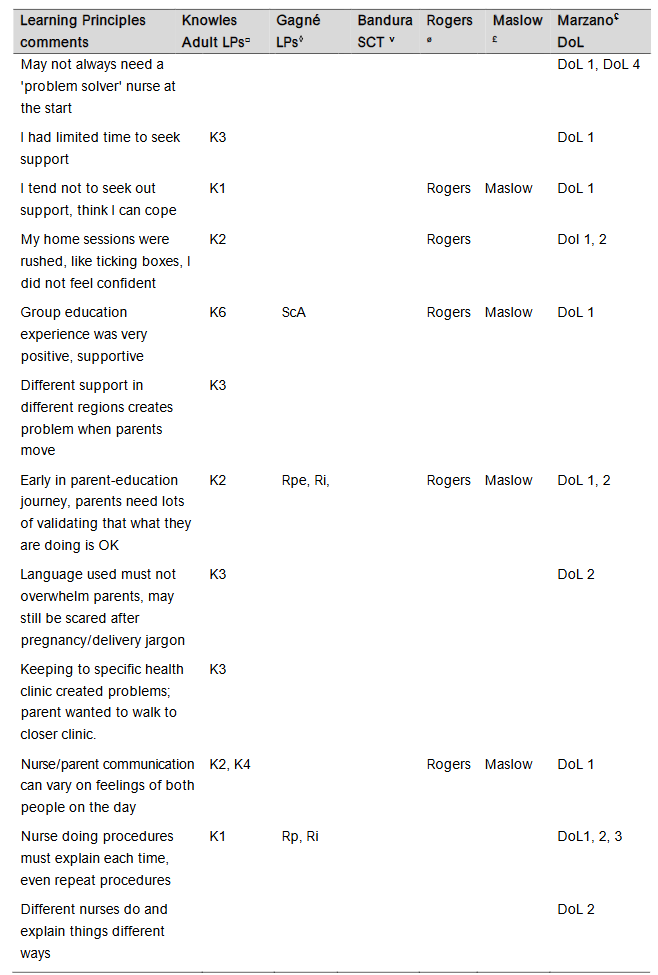
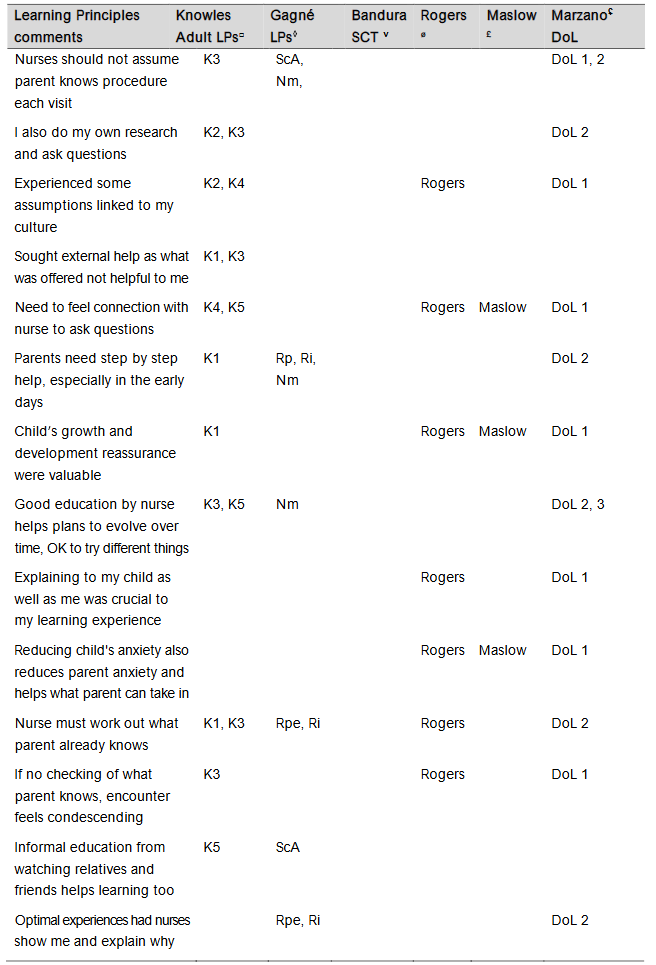
The comprehensive array of Learning Principles nurses described plus parents descriptions of key aspects of nurses PPFE are mapped and codified to theorists in Table 7, (Supplementary Material 1).
| Key Learning Principles and links to theorists Nurse participants descriptions |
|---|
| Ask if parents want to try something else |
| Show parents other ways to do things |
| Break learning into baby steps |
| Not overwhelming parents with too much information |
| Respect parents wishes provided child is safe |
| Assessing parents needs, not what nurse thinks parents need |
| Demonstrate what needs to be learned |
| Some parents try to be perfect parents which affects their learning |
| Learning needs nurses intuition and observation and not to be overbearing |
| Write out a plan and talk parents through it |
| Never assume parents know what is normal for child’s care and safety |
| Identify parents capabilities and see what needs changing |
| Relationship building |
| Ensuring any tasks shown are achievable |
5.2 DIMENSIONS OF LEARNING
Nurses lamented there was no formal resource or formal teaching about Learning Principles to explain how nurses use Learning Principles in practice: learning’s a grey area of practice, not black and white. With no formal teaching as such, on how to do it You just kind of do it (CHN 76). No consistent terms/professional language impacted effective communication between nurses themselves to build skills in using Learning Principles: we have been given much information over the years, but nothing that put it all together (CHN 47) and it was time a resource was developed (CHN 94).
The enthusiasm nurses showed when seeing the Dimensions of Learning framework diagram, plus the framework’s alignment to the Learning Principles nurses used suggested the framework resonated, significantly, with their deeper reflections on ways they used Learning Principles it’s what nurses do in practice… (PN 98).
RESULTS
CYCLE 3 THE WORKSHOP
Cycle 3’s data confirmed those Learning Principles uncovered in Cycles 1 and 2. Predominantly, data aligned with Dimensions of Learning headings 1-3. Fewer terms aligned with Dimensions of Learning 4 (applying the knowledge meaningfully) and 5 (habits of mind). Commentary heard during the workshop and captured in field notes reflected collaboration, questioning, deep reflection and learning: It is so useful to hear points on learning from both perspectives [parents; nurses]… (PN 58). Nurses were stimulated to reflect deeply on their overall PPFE nursing practice:… I have realised so many things are assumed … (PN 57). The significant criteria outlined by nurses and parents in the Matrix are outlined in Table 9.
| Parent and nurse infographic criteria | |
|---|---|
| Top 3 criteria for each parent participant | Top 3 Criteria for each nurse participant |
| Clear steps to follow | Cultural understanding |
| Key points in plain language | Individual nursing approach to client |
| Translates to ESL easily | Listening skills |
| Empathy/cultural | Relatable/adaptable |
| Easy to interpret | Approachable, compassionate |
| Minimal text | Empathy & listening |
| Visual appeal | Cues from group members |
| Clear Flow | Adaptable for client |
| Easy to follow | Empathy |
| Clarity of language | Individualised/adaptable |
| Information provided | Clear information |
| Simple layout not busy | Easy to understand |
| Succinct clear brief points | Easy Guide |
| Uses easy language | Examples are provided |
| Key points are clear | Clear communication |
| Summary of parent criteria | Clear |
| Simple, easy to follow, clear language | Logical flow |
| Easy to follow | Interpretation of language |
| Adaptability to practice | Visual |
| How clear is path communicated? | Effective language |
| Are diagrams effective? | Size of writing |
| Time allowed | Graphic friendly |
| Makes sense to the nurse | Ease of following |
| Learning style of parent | What tool needed to teach? |
| Understand and interpret content |
Participants ranked the infographics (5 being the most important) to identify a preferred format and content. Slight preference was for the Word-boxes infographic to Pathways Infographic. The result of the decision-making exercise, together with an understanding of the important criteria, guided the generation of a resource.
| Infographic decision table |
|---|
| Nurse/Parent Infographic 1 Ellipse Infographic 2 Pathway Infographic 3 Word-boxes |
| P1 2 2 3 |
| P3 3 2 1 |
| P11 3 2 3 |
| P12 1 2 3 |
| P13 1 3 2 |
| P18 incomplete |
| TOTAL PARENTS 10 11 12 |
| N2 incomplete |
| N4 1 3 2 |
| N5 2 1 3 |
| N6 2 1 3 |
| N7 1 2 3 |
| N8 2 3 1 |
| N9 2 3 1 |
| N10 1 3 2 |
| N14 incomplete |
| N15 1 2 3 |
| N16 3 1 2 |
| N17 3 2 1 |
| TOTAL NURSES 18 21 21 |
| OVERALL TOTAL 28 32 33 |
RESEARCHER’S ACT FOR CYCLE 3 Cues featured strongly in Cycles 1 and Cycle 2 of the study ─ they helped educators and learners make connections between the information provided and the knowledge (facts and the practical aspects) they needed to use, parents psycho-socio-cultural considerations, and their developing confidence and capability in their children’s care. The resource was created as Cycle 3 Act from participants data, their collective knowledge and wisdom. Cues, not prescriptive tasks, stimulate each educator’s (nurse’s) ideas to determine relevant points for facilitating each parent’s effective, meaningful learning within PPFE.
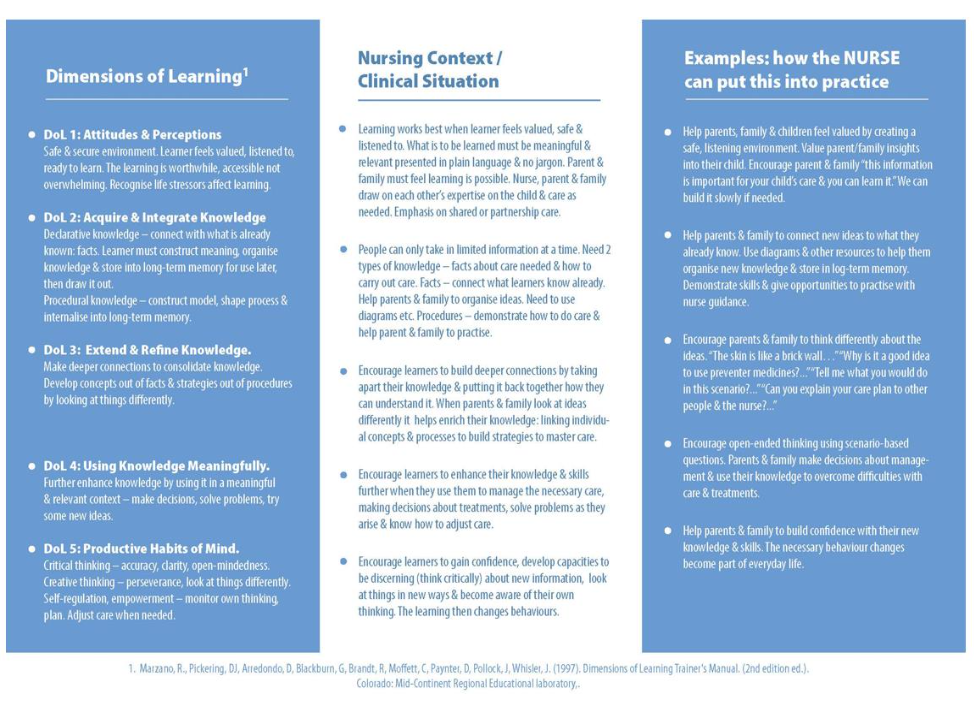
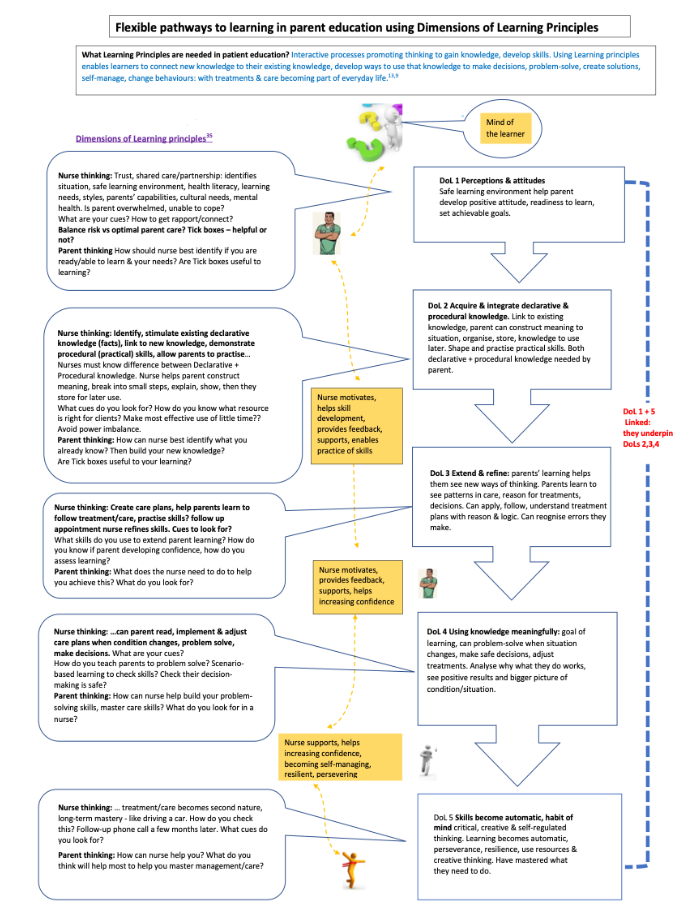
Side one of the resource, the nurses side, has three columns: 1) briefly outlines each Dimension of Learning, a consistent core framework explaining how thinking and learning take place in each dimension. Nurses can link this to current practice. 2) contains a representation of the learning process and a range of Learning Principles in the context of nurses practice and patients and families health. 3) provides cues (examples of nursing activities) to stimulate nurses to make connections between their knowledge, previous learning, Learning Principles and translating these factors into PPFE.
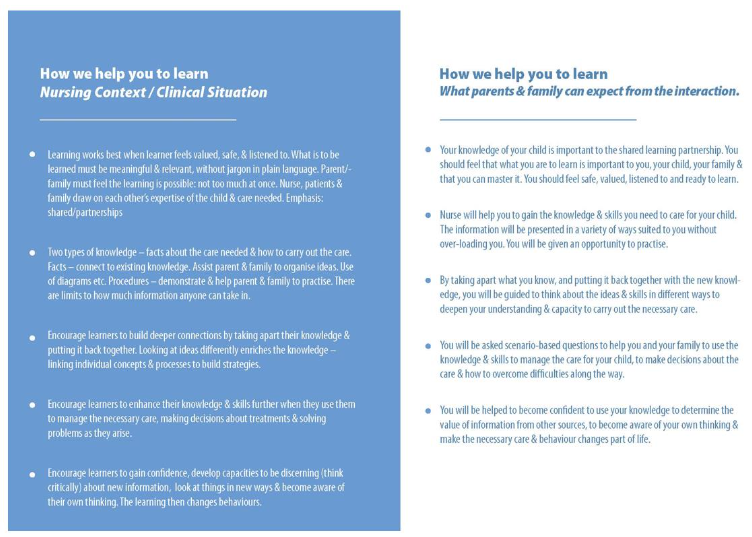
On the parents side, outlines to parents what nurses/health professionals should do to facilitate their thinking and learning process to transform information, build knowledge, skills and confidence. In How we help you to learn parents can see key Learning Principles nurses should engage with to optimise their PPFE learning experiences. Each Dimension of Learning section includes prompts to help parents connect to what they need to learn, open conversations with their nurse, and to address learning needs. The resource captures the philosophy of person-and family-centred care, partnerships, and consistency in information and learning, with nurses and parents using the same resource.
DISCUSSION
To our knowledge, this is the first study to explore, identify and describe the ways nurses use a range of cognitive and adult Learning Principles, previously not described in nursing’s PPFE literature. The alignment of participants descriptions of the ways they implemented a range of Learning Principles into their PPFE practice and what was important to parents experiences also add important, new understandings to how nurses facilitate the learning process, descriptions of which have previously been overlooked. These results and insights have implications for nursing practice.
MAPPING OF THE LEARNING PRINCIPLES
Previously, nursing’s dialogue surrounding the use of Learning Principles emphasised using adult Learning Principles of Knowles. However, multiple researchers recognised there was still a gap in effective learning outcomes when only adult principles were used, but did not offer solutions. Kaakinan and Atwood proposed that nurses overlook integrating the cognitive and social processes involved in adult learning, something Wolf et al. found also. However, the descriptions identified and mapped in Cycle 2 show these nurses did consider cognitive and social aspects of PPFE as vital, but were unlikely consciously aware of their actions, rather they worked. Our results have potential to help nurses begin to build awareness of what nursing actions need to be integrated into effective PPFE practice, including using metacognition to deeply reflect upon what they think are existing but innate practice/skills and consciously draw up what may be tacit knowledge to inform their PPFE. If nurses are to help parents to build the knowledge, skills, confidence and empowerment to care for their children, awareness of what underpins PPFE and using cognitive Learning Principles are vital. Using adult principles alone impacts the learning process, as cognitive Learning Principles are what help people to think, reason and problem-solve as they transform information to usable knowledge and build the skills to care for their children.
NURSES INTEGRATION OF THEORIES
Of significance were the Cycle two findings that nurses implemented various learning theories (Social cognitive theory and self-efficacy theory) and humanistic theories of Rogers and Maslow). This is contrary to a wide body of literature suggesting nurses avoid engaging with learning theories, which Merriam describes as a mosaic, hard to navigate. Interestingly, our study findings support Thompson et al.’s literature review on Learning Principle implementation by health professionals, that found the most successful educational interventions/encounters were those implementing or underpinned by Bandura’s theories. Our results suggest a possible starting point for further research to see whether nurses have tacit but unrecognised knowledge of using various learning and humanistic theories, already underpinning their practice. Our results pose two questions: 1) have these nurses ever been exposed to the theories or have they, through years of trial and error, refined their practice to align with the theories, but been unaware of them? And 2) could nurses familiarising themselves with the Dimensions of Learning framework and using metacognition, unlock tacit knowledge and possible connections to buried theoretical nursing knowledge?
USING METACOGNITION
In Cycle 2, nurses and parents questioned, discussed, debated and came to new realisations about the ways nurses use the invisible, but vital aspects of their PPFE. Nurses had fine-tuned their skills of using a range of Learning Principles heuristically over time, but the process of using metacognition helped nurses draw on their tacit knowledge, with participants becoming aware that their knowledge and skills were not innate or automatic. Deeper reflection using cues in the member-checking summaries helped nurses move beyond their assumed beliefs and knowledge boundaries, questioning not only their own practice, but organisational assumptions and protocols, such as the barriers of tick-box documentation for demonstrating patient understanding. Our findings about tick-boxes and their meanings being interpreted differently by nurses, even conveying inaccurate levels of patient understanding, corroborate findings of multiple researchers on tick-box use for discharge information, documentation and mis-interpretation. Systematic reviews determined that tick-boxes and checklists were commonly incomplete, failed to convey the context and negatively impacted effective nurse/nurse and nurse/patient communications and patient safety. Organisations need to revisit and reconsider recommendations of prescriptive tick-boxes, where one size fits all, and consider building nurses awareness of the Learning Principles needed to build patients/parents understanding and capabilities patient, so that PPFE learning experiences and even patient safety are optimised.
EMPOWERMENT AND LEARNING PRINCIPLES
Multiple nursing PPFE publications underscore empowering parents to optimise self-management care of their children, but provide minimal guidance to nurses to help them see ways to optimise the learning process. Our findings support this stance. Researchers commonly generate new tools to create consistent ways to meet patients learning needs and build empowerment within PPFE, but still overlook explaining to nurses how they enact the learning process for people to transform information provided into usable knowledge. Parents accounts in our results reinforced that the cognitive Learning Principles nurses used significantly helped them to connect new and existing knowledge, build problem-solving skills and practical capabilities to deliver and adjust care/treatments to their children confidently. This new perspective suggests that before new tools are created, researchers should seek to explore what Learning Principles their population samples are using, and explore ways they are using them, in a consistent professional language, so nurses can use such tools effectively.
PROFESSIONAL LANGUAGE
Nurses and parents in our study referred to a lack of a common professional language for the invisible aspects of nursing’s PPFE practice and using Learning Principles, as a key practice hurdle. Our findings support De Vries and Peddle et al.’s research into the need for a common language for many aspects of interprofessional health education. The mapping of the Learning Principles and their alignment to the Dimensions of Learning framework provides nurses, parents and healthcare organisations with guidance and a possible language to potentially recognise what subjective aspects of PPFE practice resonate with their current practice, as they build parents learning and empowerment. Further research is needed.
DIMENSIONS OF LEARNING FRAMEWORK
The Dimensions of Learning framework, and the resource based upon the framework, created after the Cycle three workshop, contains cues, rather than a prescriptive list of tasks. This outcome supports other research where nurses found using cues, rather than prescriptive tasks, vital to clinical reasoning decisions and building of tacit knowledge, that can only come from experience. Many nurses are already familiar with using cues to stimulate their thinking about their practice, with cues being integrated into nurse competency assessment processes. Therefore, it is unsurprising that participants descriptions resonated with the Dimensions of Learning framework. There is potential for further research to explore whether cues help other nurses outside the healthcare setting of the study, to recognise what they actually do in current PPFE practice, when implementing the adult learning principles so emphasised by nursing organisations protocols/guidelines.
That the Dimensions of Learning framework resonated with nurses it’s what nurses do and parents is an important finding. The mapping of the Learning Principles nurses used and parents experiences showed significant alignment with the various dimensions of the framework one to three, although there were fewer connections to dimensions four (problem solving) and five (where skills become part of everyday life). That said, the framework helped nurses connect to their practice of using Learning Principles in PPFE. Suter & Suter integrated the Dimensions of Learning, Gagne’s 6 and Knowles Learning Principles and Bandura’s theories into a home care nursing guide for chronic disease self-management, but connections between theory and practice were implicit. The resource created as a Cycle 3 outcome encourages parents problem-solving skill development, which Trento highlighted is important for patients and families when striving for long-term success in self-management/self-efficacy in PPFE. Yet, helping people with diverse learning needs to see the connections between theory, practice and skill development still poses challenges. We propose that problem-solving capabilities are often invisible, but can be recognised and tested when learners are presented with scenarios relevant to their condition/situation. Further research can determine if the resource can raise nurses conscious awareness of what Learning Principles they do use in PPFE practice with consistent language, integrating analogies and the role of using scenarios to check parent understanding, which align with dimensions four and five, rather than just using the teach-back approach. Nurses in our study recognised that teach-back alone is insufficient to ensure parents/patients understanding.
The study findings potentially extend further a framework created by Thompson & Thompson, explaining how learning takes place within PPFE and the role of the nurse as a conduit in the information to knowledge transformation process for eczema education. Their sound framework, based on learning theories and nursing practice, was too complex for busy clinical nurses. It also overlooked discussing how Learning Principles are used within PPFE practice. This gap may possibly be bridged by what we believe is the first resource guiding nurses to develop awareness surrounding use of various learning theories. While outlining in straightforward language ways Learning Principles can be used and how learning takes place, provide the guidance. Learning, like clinical reasoning, is difficult to teach and learn.
HEALTH LITERACY
The study findings also support Wolf et al.’s health learning capacity framework, proposed to strengthen health literacy. These authors created an algorithm to improve health professionals cognitive learning and psychosocial skills capabilities when building patients functional, interactive and critical health literacy. The algorithm has had limited uptake. Future research can explore if our resource, plus Wolf et al.’s algorithm opens new insights for nurses PPFE practice and building patients health literacy. Currently, global health literacy skills development is limited and insightful solutions are needed ─ simpler pictures and words (functional health literacy), favoured by most health networks, have yielded limited success and need further research.
Strengths, limitations
STRENGTHS
Strengths of the study included actively involving nurses and parents in the action research process to explore, capture and utilise their depth of knowledge, experience and perspectives on an invisible part of healthcare practice. The principal researcher’s insider status as an employee of the health network outpatient department helped to build relationships, rapport between participants, fostered trust and potentially engendered genuine responses. However, DT’s employment in the outpatient setting of the study had potential biases. Therefore, DT recorded her ideas, thoughts and potential biases prior to, during and after data collection and the analyses in a reflexive diary, assisting credibility and the audit trail. Multiple methods of data collection (focus groups, field notes and the workshop) helped augment credibility. Field notes by CS helped clarify data interpretation and were part of the audit trail. As field notes are influenced by the thoughts and beliefs of the person creating them by recording what is seen and heard, DT and CS discussed the field note contents after each focus group and the workshop. Conversations were documented in a reflexive diary.
Member checking summaries created from data analysis and sent to participants, enabling them to contact/discuss concerns with DT also enhanced rigour. Researcher/supervisor discussions and data analyses and synthesis scrutiny by supervisors until consensus was reached, throughout they study, assisted dependability and further mitigated risk of bias. The reimagining of Stringer’s Act, to have participants metacognition recognised as an activity, was supported by robust literature, and is a strength rather than a limitation.
LIMITATIONS
The purposive sample of PNs, CHNs and parents from one Australian health network in this qualitative study, means results are not generalisable to other nurse or parent groups or other settings. The exclusion of parents who needed interpreter services within PPFE limits findings, but there is a need to explore how Learning Principles are used with this population. The researcher’s interpretations, classifying and coding of Learning Principles cannot be free of personal beliefs and values, but the measures discussed in the paper attempted to mitigate these limitations. The researcher’s insider status as an employee of the healthcare network may have influenced those who volunteered to be involved in the research, and also their behaviours during data collection. Time constraints of PhD timelines prevented the resource being piloted in the healthcare setting or bringing participants back to deliberate and refine the resource. Further research using this initial tool is planned.
Implications for practice
Nursing research has been challenged on ways to make the learning process, in contrast to the teaching process, explicit and understandable to nurses and patients/parents/families. Using metacognition has potential to help people actively connect to what they may know already, but are unable to articulate or unlock about their LP use and learning facilitation.⁵¹,⁵² There is potential for the resource, based on The Dimensions of Learning framework, to help nurses better recognise what they do in PPFE practice, rethinking ‘accepted’ concepts of automatic/innate behaviours.²⁶
Mapping of Learning Principles important to parents’ learning, building of confidence and capability helped uncover the range of cognitive and adult Learning Principles nurses used.⁴,⁶–¹⁰ The resource created has potential to help parents see how learning should take place within PPFE, with nurses respecting and building on parents’ existing knowledge and skills. It is not a tick-box approach, moving beyond ‘identifying patients’ learning needs’.¹,⁶⁶ The resource shows nurses and parents what ‘to do’ to help learning take place. Cues were important to nurses’ PPFE and to parents to stimulate their learning and building of understanding. Further research can explore how cues impact a wider group of parents in PPFE, especially for thinking, reasoning and problem-solving skills development.
The research may help inform nursing professional development surrounding PPFE. Organisational assumptions about nurses’ PPFE capabilities, sole use of adult learning Principles and the nursing literature’s assumptions that in educational interventions learning always follows from teaching strategies, need overhauling.⁵ Examining how the Dimensions of Learning framework may help nurses
Conclusion
Cycles 2 and 3 of this action research study helped a group of experienced, proficient nurses unlock their tacit knowledge and assumptions, building awareness of their use of a range of cognitive and adult Learning Principles they heuristically developed over years of practice, but struggled to describe initially. Using metacognition, these nurses’ beliefs that their Learning Principles’ use was innate or automatic PPFE shifted from assumed and invisible, to visible and able to be recognised and described. Reimagining Stringer’s Act using metacognition created new insights to help nurses unlock knowledge they have, but cannot explain. ‘Action’ within action research should not be limited to objective, visible tasks.²⁷ These cognitive Learning Principles were vital for parents’ interactive optimal learning experiences: information to knowledge transformation, skills, capability and confidence building to manage their children’s care, long term.
The alignment of participants’ descriptions to the existing Dimensions of Learning framework from educational psychology has important potential to be explored in other nurse and parent PPFE populations.⁶–¹⁰ The framework provided a ‘conduit’ between nurses’ theory and practice and parents’ desired and necessary learning experiences. Nurses recognised the invisible nature of learning, through the framework.¹⁴ The resource potentially creates a means to communicate explicitly the ways Learning Principles are used in PPFE, to others. Future research can also determine whether the resource can help build health literacy/ health learning capacity for people with chronic conditions, which is still a challenge world-wide.²
Funding:
This paper received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Availability:
Access to the research data from this project may be discussed with the lead author. Data management has adhered to appropriate ethical approvals and requirements.
Acknowledgements:
We wish to acknowledge the participants who gave their valuable time to participate in the study and Associate Professor Matthew Leach for his valuable supervisory role in the PhD study.
Disclosures:
All authors report no conflicts of interest or financial interests in this work.
References
1. Bastable S, Gramet P. Overview of Education in Healthcare. In: Health Professional as Educator: Principles of Teaching and Learning. 2nd ed. Burlington, Massachusetts: Jones & Bartlett Learning:2020:32-98.
2. World Health Organisation. Therapeutic Patient Education: an introductory guide, Copenhagen: WHO Regional Office for Europe; (2023). Accessed November 1, 2025.
3. Grant J, Mitchell C, Cuthbertson, L. National Standards of Practice for Maternal, Child and Family Health Nursing Practice in Australia, Adelaide, Australia: Flinders Press; 2017.
4. Wolf M, Wilson E, Rapp D. et al. Literacy and learning in health care. Pediatrics. 2009; 24(3), suppl. 3:275–81. doi:10.1542/peds.2009-1162C
5. Thompson D, Leach M, Smith C, Fereday J, May E. How nurses and other health professionals use learning principles in parent education practice: a scoping review of the literature, Heliyon;6(3):1–24. doi: 10.1016/j.heliyon.2020.e03564
6. Gagné R. The conditions of learning and theory of instruction, 4th ed, Holt, Rinehart and Winston, New York; 1985.
7. Eberly Centre. Learning Principles. Carnegie Mellon University, Pittsburgh.
https://www.cmu.edu/teaching/principles/learnin.html. Published 2019. Accessed 16 October, 2025.
8. Brown A. The Advancement of Learning, Educ Res.1994;23(8):4-12.
9. Gagné R, Wager W, Golas K, Keller J. Principles of instructional design. 5th ed. Thomson Wadsworth Belmont, California; 2005.
10. Bastable S, Myers G, Binion, B. Health Literacy in Adult Population. In Health Professional as Educator: principles of teaching and learning. Burlington, Massachusetts: Jones & Bartlett Learning:2020; 497-616
11. Griffith B, Loveless D. eds. The interdependence of teaching and learning, Information Age Publishing, Charlotte, North Carolina; 2013.
12. Knowles MF, Holton E, Swanson R. The Adult Learner: The Definitive Classic in Adult Education and Human Resource Development. 8th ed. Oxon: Routledge, Taylor & Francis. Francis, Oxon; 2015.
13. Anderson J. Cognitive psychology and its implications. 6th ed, Worth Publishers, New York; 2005.
14. Thompson D, May E, Leach M, Smith C, Fereday J.The invisible nature of learning: patient education in nursing, Collegian. 2021; 28(3):341-345.
15. Kivunja C, Kuyini A. Understanding and applying research paradigms in educational contexts. Int J High Educ. 2017; 6(5):26-41.
doi: 10.5430/ijhe.v6n5p26
16. Ormston R, Spencer L, Barnard, M, Snape D. Foundations of Qualitative Research. In Ritchie J, Lewis J, McNaughton Nichols C, Ormiston R. eds. Qualitative Research Practice, 2nd ed. Sage Publication, Ltd. London;243-65.
17. Stringer E. Action Research. SAGE Publications Inc., Thousand Oaks, CA; 2007.
18. Thompson D, May E, Leach M, Smith C, Fereday J. Applying Learning Principles Within Parent Education: Exploring Nurse’ Practice and Parents’ Experiences. Patient Prefer Adherence. 2023; 17: 2949-2970, doi: 10.2147/PPA.S426043Â. https://pubmed.ncbi.nlm.nih.gov/38027081
19. Benner P. Taking a stand on experiential learning and good practice. Am J Crit Care. 2001;10(1):60-62. doi: 10.4037/ajcc2001.10.1.60
20. Gustavsen B. Theory and practice: the mediating discourse. In Reason P, Bradbury H, (eds), The handbook of Action Research, SAGE Publications Ltd, London. 2006;17-26
21. Hegney D, Francis K. Action research: changing nursing practice. Nurs Stand. 2015; 29(40): 36–41.
22. D’Eredita M, Barreto C. How does tacit knowledge proliferate? An episode-based perspective, Organ Stud. 2006; 27(12):1821–41. doi: 10.1177/0170840606067666
23. Navon E. The third debate revisited. Rev Int Stud. 2000; 27(4):611–25.
doi:10.1017/S0260210501006118
24. Thomas A, Menon A, Boruff J, Rodriguez A, Ahmed S. Applications of social constructivist learning theories in knowledge translation for healthcare professionals: a scoping review. Implement Sci. 2014; 9(1):54–74.
doi: 10.1186/1748-5908-9-54
25. Given, L. Constructivism. In Given L. ed. The Sage encyclopedia of qualitative research methods, SAGE Publications Inc., Thousand Oaks, 2008; 116–120.
26. Gaventa J, Cornwall A. Challenging the boundaries of the possible: participation, knowledge and power, IDS Bull. 2006; 37(6):122–28. doi: 0.1111/j.1759-5436.2006.tb00329.x
27. Holter I, Schwartz-Barcott D. Action Research: what is it? How has it been used and how can it be used in nursing? J Adv Nurs. 1993; 18(2):298–304. https://doi.org/10.1046/j.1365-2648.1993.18020298.x
28. Leitch R, Day C. Action Research and reflective practice: towards a holistic view. Educ Action Res. 2000; 8(1):179–93. doi: 10.1080/09650790000200108
29. National Health and Medical Research Council (NHMRC). Australian Code for the Responsible Conduct of Research, Australian Research Council and Universities Australia.
https://www.arc.gov.au/about-arc/program-policies/research-integrity/australian-code-responsible-conduct-research-2018
30. Polit, D, Beck C. Nursing research generating and assessing evidence for nursing practice. 10th ed. Wolters Kluwer, Philadelphia. 2017.
31. Liamputtong, P. Focus group methodology: principles and practice. SAGE Publications Ltd, London; 2017.
32. Lambert S, Loiselle C. Combining individual interviews and focus groups to enhance data richness. J Adv Nurs. 2008; s62(2):228–37. doi: 10.1111/j.1365-2648.2007.04559.x
33. Orngreen R, Levinsen K. Workshops as a research methodology, J Educ Elearn. 2017: 15 (1):70.
34. Braun V, Clarke V. Successful Qualitative Research: A Practical Guide for Beginners. London, England: SAGE Publications; 2013.
35. Marzano R, Pickering, D, Arredondo, D, et al. Dimensions of Learning Teacher’s Manual , 2nd ed, Mid-Continent Regional Educational laboratory, Colorado;1997.
36. Baillie L. Promoting and evaluating scientific rigour in qualitative research. Nurs Stand. 2015;29 (46):36-42. https://doi.org/10.7748/ns.29.46.36.e8830.
37. Scott H, Fawkner S, Oliver C, Murray A. Why healthcare professionals should know a little about infographics. Br J Sports Med. 2016; 50(18);1104–1105
38. Bradshaw MJ, Porter S. Infographics: A New Tool for the Nursing Classroom. Nurse Educ. 2017; 42:57–59.
39. Arcia A, Suero-Tejeda N, Bales M et al. Sometimes more is more: iterative participatory design of infographics for engagement of community members with varying levels of health literacy. J Am Med Inform Assoc. 2015; 23(1):174–183.
40. Shoghi M, Sajadi M, Oskuie F, Dehnad A, Borimnejad L. Strategies for bridging the theory-practice gap from the perspective of nursing experts. Heliyon. 2019; 5(9):e02503. 10.1016/j.heliyon.2019.e02503
41. Aronson E, Bridgeman D. Jigsaw groups and the desegregated classroom: In pursuit of communal goals. J Pers Soc Psychol. 1979;37(7):1309-1319. https://doi.org/10.1177/01461672790050040
42. Aronson E. The Jigsaw Classroom. Social Psychology Network. http://www.jigsaw.org. Published 2000. Accessed December 23, 2025
43. QSR International, NVivo 12, viewed 2 March 2018, https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
44. American Society of Quality [ASQ]. What is a matrix diagram? 2018; Accessed November 3, 2025. https://asq.org/quality-resources/matrix-diagram
45. Öberg J, Hernwall P. Participatory design with teachers: designing the workshops, in Designs for Learning. Proceedings of the 5th International Conference on Designs for Learning, 2016. Copenhagen; 269–282.
46. Bazeley P, Jackson K. Qualitative data analysis with NVivo. SAGE Publications Ltd, London; 2013.
47. Clapper T. Beyond Knowles: What those conducting simulation need to know about adult learning theory. Clin Simul Nurs; 2009; 6(1): pp. e7–e14. doi:10.1016/j.ecns.2009.07.003
48. Merriam S. Adult learning theory: evolution and future directions ‘, PAACE Journal of Lifelong Learning; 2017;26; 1–37.
49. Kaakinen J, Arwood E. Systematic review of nursing simulation literature for use of learning theory. Int J Nurs Educ Scholarsh, 2009. 6(16). https://doi.org/10.2202/1548-923X.1688
50. Kothari A, Rudman D, Dobbins M, et al. The use of tacit and explicit knowledge in public health: a qualitative study. Implement Sci. 2012; 7(1):20–32. doi: 10.1186/1748-5908-7-20
51. Kuiper R, Pesut D. 2004. Promoting cognitive and metacognitive reflective reasoning skills in nursing practice: self‐regulated learning theory. J Adv Nurs. 2004;45(4);381–91
52. Kosior K, Wall T, Ferrero S. The role of metacognition in teaching clinical reasoning: theory to practice. Educ Health Prof. 2019;2:108–14, doi: 10.4103/EHP.EHP_14_19
53. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall; 1986.
54. Bandura A. Self-Efficacy: The Exercise of Control. W.H. Freeman; 1997.
55. Rogers C. Freedom to learn for the 80s. Charles E. Merrill Publishing Company, Columbus, Ohio; 1983.
56. Maslow A. Motivation and Personality, Harper and Row, New York. 1970.
57. Bjork, R, Dunlosky, J & Kornell, N. 2013, Self-Regulated Learning: Beliefs, Techniques, and Illusions, Annu Rev Psychol. 64(1);417–444.
58. Culyer L, Jatulis L, Cannistraci P, Brownell C. 2018. Evidenced-based teaching strategies that facilitate transfer of knowledge between theory and practice: what are nursing faculty using? Teach Learn Nurs. 2018; 13(3):174–79. https://doi.org/10.1016/j.teln.2018.03.003
59. ten Cate O, Snell L, Mann K, Vermunt J. Orienting teaching toward the learning & process; Acad Med. 2004; 79(3):219–28.
60. Tanner K. Promoting student metacognition. CBE Life Sci Educ. 2012. 11(2):113–20.
https://doi.org/10.1187/cbe.12-03-0033
61. Fish D, De Cossart L. Thinking outside the (tick) box: rescuing professionalism and professional judgement’, Med Educ; 2006;40(5);403–404.
62. Rydenfält C, Ek Å, Larsson P. Safety checklist compliance and a false sense of safety: new directions for research. BMJ Qual Saf; 2014; 23(3):183–186.
63. Nightingale R, Wirz L, Cook W, Swallow V. Collaborating with parents of children with chronic conditions and professionals to design, develop and pre-pilot PLAnT (the Parent Learning Needs and Preferences Assessment Tool)’, J Pediatr Nurs, 2017; 35; 90–97, doi: 10.1016/j.pec.2015.05.002
64. Svavarsdottir H, Sigueoardottir A, Steinsbekk A. How to become an expert educator: a qualitative study on the view of health professionals with experience in patient education. BioMed Central; 2015; 15(1), 1-9.
65. Vries-ErichJ, Reuchlin K, de Maaijer P, van de Ridder M. Identifying facilitators and barriers for implementation of interprofessional education: Perspectives from medical educators in the Netherlands, J Interprof Care, 2017; 31:2; 170-174, doi: 10.1080/13561820.2016.1261099
66. Peddle M, Bearman M, Radomski N, Mckenna L, Nestel D. ‘What non-technical skills competencies are addressed by Australian standards documents for health professionals who work in secondary and tertiary clinical settings? A qualitative comparative analysis’, BMJ Open; 2018; 8(8); e020799–e020799.
67. Hoffman K, Aitkin L, Duffield C. (2009). A comparison of novice and expert nurses’ cue collection during clinical decision-making: Verbal protocol analysis. Int J Stud Nurs; 2009; 46(10): 1335-44. doi: 10.1016/j.ijnurstu.2009.04.001
68. Ingvarsson E, Verho J, Rosengren K. Managing Uncertainty in Nursing – Newly Graduated Nurses’ Experiences of Introduction to the Nursing Profession. Int Arch Nurs Health Care: 2019; 5:119. doi.org/10.23937/2469-5823/1510119.
69. ANSAT. ANSAT Resource Manual for RNs. ANSAT; 2018. Accessed December 23, 2025. https://www.ansat.com.au/home/resources
70. Trento M. 2019. The utopia of research: epistemology of patient education, Acta Diabetol. 2019; 56(2);145–150.
71. Suter P, Suter W. Patient education. Timeless principles of learning: a solid foundation for enhancing chronic disease self-management, Home Healthc Nurse. 2010; 6(2):82–8.
10.1097/01.NHH.0000311024.11023.09
72. Thompson D, Thompson M. Knowledge, instruction and behavioural change: building a framework for effective eczema education in clinical practice’, J Adv Nurs.70(11); 2483–2494. doi:10.1111/jan.1243.