

Opioid Policy’s Impact on Pain Management in Georgia
Influence of unbalanced opioid policy on pain management and home-based palliative care services in Republic of Georgia
Pati Dzotsenidze – MD, PhD¹ and Tamriko Bulia – MD, PhD student (researcher)²
- Associated professor – Georgian National University (SEU), Faculty of Medicine (research and Healthcare) Tbilisi, Georgia
- School of Health Sciences; University of Georgia (UG), Tbilisi, Georgia
OPEN ACCESS
PUBLISHED:31 May 2025
CITATION: Dzotsenidze, P. and Bulia, T., 2025. Influence of unbalanced opioid policy on pain management and home-based palliative care services in Republic of Georgia. Medical Research Archives, [online] 13(5).
https://doi.org/10.18103/mra.v13i5.6581
COPYRIGHT:© 2025 European Society of Medicine. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6581
ISSN 2375-1924
ABSTRACT
Introduction: Most patients with incurable diseases prefer to spend their treasured time in home settings. As pain is the most frequent symptom, often requiring opioid analgesics, it is essential that outpatient medical services are supported by policies that allow managing patients’ conditions at home. This paper aims to show how over-restrictive regulations/policies can impact patients’ ability to access pain management and hamper the development of home-based palliative care services.
Methods: To evaluate the influence of strict regulations on pain management and their impact on home-based palliative care services, on one hand the opioid legislation and policy documents were reviewed and on the other opioid consumption reports, data on mortality and provided palliative care services, and data from the patient survey were analyzed.
Results: The palliative care program states that only incurable patients who are at the end of their lives and need home-based support can benefit from the program. Additionally, the physician must be convinced that the diagnosis is correct and that the estimated life expectancy is no more than 3–6 months (duration of benefiting from the program). Consequently, fearing the penalties, physicians mostly include patients in the program, when apparent signs of death are present. Therefore, patients have to be hospitalized, to receive care. As a result, the number of provided home based services has decreased more than half and its’ ratio to inpatient services is 1:4.
Simultaneously, the legislation allows prescribing opioids only to terminally ill patients, for whom no other treatment options are available. Before being prescribed morphine, about 94% of the terminal patients experienced moderate to severe pain. 75% experienced severe pain for 1 month and more. Yet, opioids were prescribed with substantial delay in most cases (61–70%). In 45%, morphine was first prescribed by palliative care physicians available only at inpatient units.
Conclusion: Strict opioid policies negatively impact pain management in palliative care patients. Even being incurable, most patients cannot receive appropriate pain treatment, until they reach the “end-of-life” stage, or receive such treatment in inpatient settings. Such an approach ignores the possibility of improving the quality of life for patients in their home setting.
Introduction
Table 1. Estimated need for palliative care, based on mortality data and provided palliative care services in the frame of the state PC program in Georgia (2017-22)
| Year | Patients in need of palliative care | Total % of served patients by state PC program |
|---|---|---|
| 2017 | 47 822 | 17 885 (37%) |
| 2018 | 48 524 | 28 101 (58%) |
| 2019 | 46 559 | 22 886 (17.2%) |
| 2020 | 50 537 | 19 800 (22.7%) |
| 2021 | 59 906 | 22 405 (19.7%) |
| 2022 | 71 198 | 23 651 (22.8%) |
The above table shows that a maximum of 17% of patients in need of palliative care can receive such services. Moreover, during 2017–2022, not only did the number of patients who benefited from home-based services decrease significantly (twice more), but also the ratio between outpatient and inpatient services changed in favor of inpatient services (1:4).
The paper aims to discuss the main regulatory / policy barriers to opioid use that impede pain treatment in incurable patients and to evaluate their impact on accessibility of strong pain medications and the availability of home-based palliative care services.
Methods
To evaluate the influence of strict regulations on patients’ ability to access opioid medications for pain treatment and their impact on home-based palliative care services, the legislation and policy documents regulating opioid prescription and accessibility of palliative care services were summarized. To identify the influence of the policy on patients in need, the following data were used: statistical data on opioid consumption from INCB annual reports, data on mortality/morbidity and provided services, and data from the patient survey performed in the frame of the PhD study – Evaluating Barriers to Chronic Pain Management and their Impact on the Quality of the Health Service by Pati Dzotsenidze, author of the current paper¹⁶. The following sources were analyzed:
• Policy
To assess the main regulatory and policy barriers, the well-established European Society for Medical Oncology’s (ESMO) policy framework regarding accessibility of opioid medications was used. These indicators were applied by ESMO and the European Association for Palliative Care (EAPC) in a large-scale survey in 41 European countries¹⁷,¹⁸. The same validated indicators were used by Global Opioid Policy Initiative (GOPI) project in countries in Latin America, Africa, Asia, India, and the Middle East¹⁹.
• To review the adequacy of pain treatment and palliative care services in Georgia, the following data were used: a. Statistical data reflecting opioid consumption from INCB annual reports²⁰. One of the most objective indicators of the adequacy of pain management is the rate of opioid consumption for the same purpose in a given country²¹–²⁴. b. Statistical data on provided actual palliative care services to check their compliance with the need for such services based on the WPCA recommendation²⁴ (for the period of 2017–2022 years). The WPCA
Table 2. Barriers to opioid accessibility
| Prescription-related barriers | Dispensing-related barriers |
|---|---|
| Authority to prescribe opioids | Pharmacy reluctance to dispense opioids |
| Special prescription form availability | Administrative barriers |
| Patient eligibility | Cost-related factors |
In the joint report WHO & WPCA estimate that 37.4% of all deaths from all causes need palliative care. The same report estimates the number of people in need of palliative care based on the prevalence of pain by disease. Data from the results of the patient survey performed in the frame of the authors’ PhD study clearly describe the problems which incurable patients in pain face in Georgia. The data collected in 2017 allows for a clear observation of the effect of further changes over the following years resulting in a decreased number of home-based palliative care services.
Results
GEORGIA – REGULATIONS / POLICY
Opioid policy for medical use in patients suffering from pain remains an unresolved issue in Georgia. According to regulations in Georgia opioids can only be prescribed to incurable patients in terminal stages of their diseases, when no any other treatment option is left for cure. However, opioids are not always prescribed even to incurable patients to relieve pain and suffering.
To make the issue clear, it is important to review two different points of the policy:
-
Legislation – regulating rules for opioid prescription²⁶ and
-
The palliative care state program through which it is possible to have access to the PC services or to opioids (https://matsne.gov.ge/ka/document/download/6375605/0/ge/pdf).
REGULATIONS
In Georgia opioids prescription and dispensing rules are regulated by the order N32/c-N102 (joint decree 32-102 MOH and MIA 2000). Though some updates were done, due to ambiguity and inconsistence of those updates²⁸ the older version of the regulation still dominates²⁹.
BARRIERS TO OPIOIDS ACCESSIBILITY –
for better categorization of the barriers the ESMO³⁰ barriers to opioid analgesic accessibility were used.
PRESCRIPTION-RELATED BARRIERS
• Authority to Prescribe Opioids:
In Georgia, only general practitioners, family/village doctors from authorized primary health care facilities serving patients according to residence place can prescribe opioids to outpatients. However, this can be prescribed only with a special permit.
• Special Permit:
The decision on assigning opioids is made by a special commission consisting of three members. After verifying the diagnoses, the commission decides
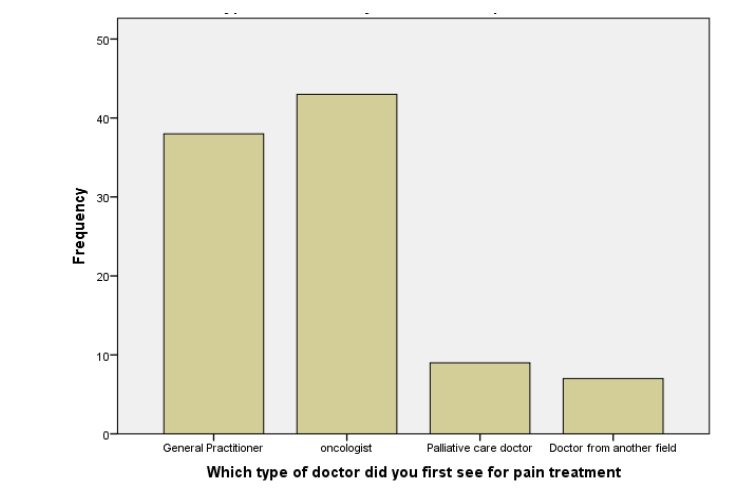
After their first contact with the physician for uncontrollable pain, opioids were prescribed only to 45% of patients in total. Out of the general practitioners that were addressed for pain treatment by incurable patients, only 39% prescribed morphine; among oncologists, only 41% did so.
The responses to the question – which type of physician finally prescribed morphine to them for intensive pain relief, show that (Figure N2):
• To 8% morphine was prescribed by the general practitioner
• To 25% by the oncologist
• And to 67% by the palliative care doctor.
Figure N2: Percentage of patients prescribed morphine
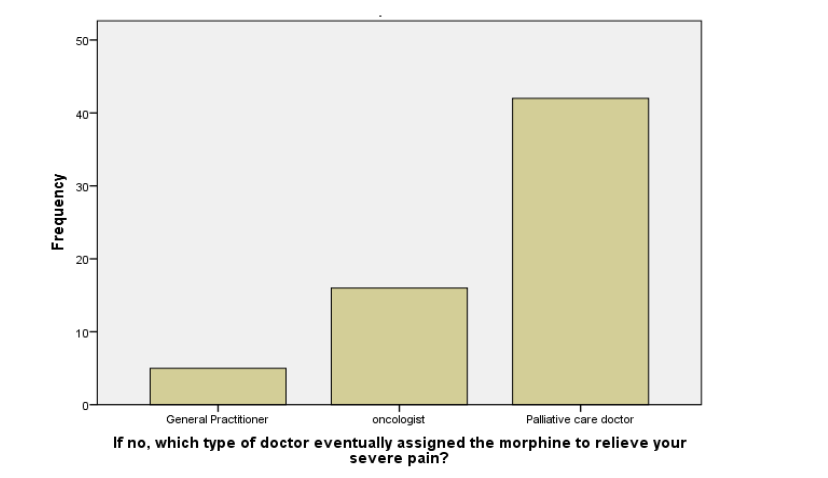
Finally in total, based on crosstabulation of the data, morphine was prescribed in 19% by GPs, in 31% by oncologists, and in 45% by the palliative care physicians. If we take into account that by that time palliative care physicians were only available in inpatient settings, it becomes clear that in order to receive adequate pain treatment, patients had to be placed in hospitals or palliative care units (the latter are also mostly located in hospitals).
It is noteworthy that although the Health Care State Programs’ component – “Palliative care for incurable patients” – in Georgia still covers home-based services, its proportion dramatically decreases each year and in 5 years dropped from 47% to 20%. Thus, the ratio of home-based and inpatient services becomes 1:4 (Table N1).
As regards the level of consumption of morphine (the only opioid for outpatients), defined daily doses for statistical purposes per million inhabitants per day – S-DDD, in 2022 it was 66 S-DDD. This level falls in a very low consumption category (1–100 S-DDD) indicating that the majority of patients did not have access to pain medication at all¹².
Discussion
The most restrictive negative provision in regulations is that opioids are discussed as a treatment of last resort. In order to prescribe opioids to patients, they must be terminally ill in Clinical Group IV – the incurable stage of disease when no other treatment options are available. Pain severity and its duration, or history of previous pain treatment effectiveness, with its possible accompanying complications, aren’t considered. The main requirement to start pain treatment is a verified incurable diagnosis. If we take into account the tendency of increasing deaths with unverified causes (since 2020, unverified deaths have increased from 6,471 to 10,603 in 2023, whereas in the same period the number of deaths due to cancer decreased by about 3,500)¹⁴, we can conclude that all undiagnosed and non-hospitalized patients die suffering, without receiving any relevant pain treatment.
In Georgia, only general practitioners, family/village doctors from authorized primary health care facilities such as polyclinics, which serve patients according to residence place, can prescribe opioids to outpatients. However, it should be considered that the place of residence should be an official registration of living place. So, if the patient needs to move to another district, e.g., to a family member in order to get care, they have to go through a lot of procedures to change the place of registration, which is also time-consuming. However, that is not all that requires time. The physician (with the intention to prescribe, which is not always the case)³¹ has to obtain a special permit in order to prescribe opioids. The decision on assigning opioids is made by a commission consisting of three members, including the physician (GP or family doctor), oncologist or relevant field specialist, and specially authorized representative from the administration. The commission verifies the diagnosis and makes a decision whether or not to prescribe morphine, including the initial dosage and possible increase. The commission is available only one or two days a week. Once the decision is taken and opioids are prescribed to a patient, the patient or mostly the patient’s caregiver (as most of the patients are unable to do so) have to rush the same day to the pharmacies with special dispensing points for opioids located in police stations. As those dispensing points are not regular pharmacies, they work and dispense opioids only once a week on a specially designated day for dispensing, when a representative from the authorized pharmacy goes to the police station to dispense opioids. Moreover, such dispensing points are few, just five in Tbilisi, the capital of Georgia, so caregivers, after obtaining prescriptions, must hurry up to reach them and take place in a long queue. The patients or caregivers have to repeat that ritual every week as the special prescription form can cover only a 7-day supply of morphine and one can’t refill the supply with the same prescription.
A special prescription form is available only within the National Health State Palliative Care for Incurables’ program and just for those physicians who serve in
polyclinic-type facilities serving patients according to living registration place. Based on the evaluation of palliative care services in Georgia (2021), only about 50% of the home-based palliative care service providers (in total seven) have access to opioids, while only 25% prescribe them³². However, it cannot be excluded that the remaining providers just avoid prescribing opioids due to strict requirements and procedures²⁹.
Thus, over-restrictive regulations and policy not only have a negative impact on patients suffering from severe pain, but they also impede the normal functioning of home-based palliative care services and their integration into primary health care in Georgia.
According to the requirements of the state program on palliative care for incurable patients, physicians must be convinced that patients will not live longer and will die within 6 months. Otherwise, they have to stop treatment because the program states that the treatment can be delivered for no more than six months. The physicians must be convinced of the “inexpediency of any further treatment attempts (taking into account the specialists’ firm belief that the diagnosis is correct)” (https://matsne.gov.ge/ka/document/download/6375605/0/ge/pdf). However, most of the physicians, especially those working in outpatient facilities, lack the knowledge to make a prognosis or do not wish to take responsibility for a “firm belief that the diagnosis is correct”. Under the circumstances, it is not always possible to make a clear prognosis, particularly “in favor of” patients. Moreover, fear of sanctions can prevent the physicians from including the patient in the program or offering palliative care services timely, as they wait for apparent “end-of-life” signs to appear.
The restrictions since 2013 and lawsuits linked to patients living longer than six months resulted in stopping the functioning of professional home-based services that had operated for one decade in Georgia. Hence, it is not surprising that, though the Health Care State Program component – “Palliative care for incurable patients” – in Georgia also covers home-based services, its proportion dramatically decreases each year (Table N1) and the ratio of home-based services to inpatients is currently 1:4.
Thus, a physician’s decision-making is based on the life prognosis of a patient and it doesn’t consider severity of the symptoms or their influence on quality of life of the patients, because a physician has to wait until the patient reaches “end of life” and will have clearly verified diagnosis to be eligible for the program. Though the program’s inclusion criteria – limitation of the service up to six months and reaching the end of life stage mentioned above are meant for outpatient services and do not directly apply to opioids assignment, yet in most cases the same criteria are applied to opioid prescription, because likewise, in order to prescribe opioids, a physician must be sure that no other treatment option is left and the patient is in the terminal stage of the disease²⁸.
Therefore, considering the above, the results of the patients’ survey must be no surprise. The patient survey revealed that before opioid prescription, out of the 90% of the patients who were regularly receiving non-opioid treatment, 94% were still in pain (from moderate to severe pain). Although the legislation allows assigning opioids to incurable patients, most of the patients weren’t able to receive adequate pain management or receive such treatment timely from the primary health care physicians responsible for prescribing opioids. Pain duration prior to opioid prescription exceeded one month among 88% of the patients with severe pain and 76% of the patients with moderate pain. Though all the patients were at the incurable stage of the disease, it took from 1 week to 1 month in 33% and more than 1 month in 40% of them to find a physician who prescribed morphine to them. To summarize, in 59% of the patients, morphine wasn’t prescribed by the physicians responsible for doing so. Finally in total, based on crosstabulation of the data, morphine was prescribed in 19% by GPs, in 31% by oncologists, and in 45% by the palliative care physicians available only at inpatient units¹⁶. In most of the cases opioids were prescribed with delay, making patients wait and suffer until they reach “end-of-life” stage with apparent death signs, when most of them already needed hospitalization due to uncontrolled symptoms.
This explains why the number of patients benefiting from the home-based services as well as the share of home-based services intensively declines annually. Unsurprisingly, that morphine consumption for pain control determined as statistical – defined daily doses by INCB report is in the range of 60–66 S-DDD¹² and falls in a very low classification (1–100 S-DDD), very inadequate to control pain in most of the patients in need.
The table N1 reveals that a maximum of 17% of patients in need of palliative care had access to the services. Similar data is shown by The Lancet Commission on global access to palliative care and pain relief, according to which the distributed opioid morphine-equivalent (DOME) for Georgia is 17%³³. Though in their report, the Lancet Commission states that “the difference between DOME and total need for pain relief medicine is a minimum measure of unmet need” as the availability of morphine is not the same as “the amount dispensed or consumed by patients”³⁴.
Thus, based on the discussion above, the following suggestions are recommended:
Opioid Prescription and Dispensing Rules
• Opioid prescription practices should primarily be based on pain severity, previous pain treatment history, and its impact on the quality of life. Additionally, they should take into consideration the diagnosis and prognosis of the patients. They must follow WHO 3 step analgesic ladders’ recommendations³⁵,³⁶.
• The regulation must clearly state that the decision to prescribe opioids must be made by the physician caring for the patient, based on careful and regular assessment of the patient’s condition; Although a provision supporting this approach already exists, it is often ignored by most physicians and their administration due to ambiguity and conflicting norms²⁹. More clarity can automatically change the practice of prescribing morphine (issuing prescriptions) only once a week, on the day of dispensing opioids from the authorized ‘pharmacies’ located in police stations.
• The Government must seek solutions to reintegrate opioid dispensing practices back into regular pharmacies. This will eliminate the need to wait several days to obtain opioid medications for pain relief and spare valuable time for patients and caregivers, who will no longer have to travel long distances to police stations.
NATIONAL PALLIATIVE CARE PROGRAM FOR INCURABLE PATIENTS
The program should not restrict the eligibility of outpatients to the “end of life” stage or limit service duration strictly to a 3–6-month period. In addition, it is advisable to increase funding to transition from purely medical care to a more holistic model of palliative care.
Conclusions
Strict opioid regulations and restrictive policy of palliative care programs have a negative impact on pain management in palliative care patients. Even being incurable, mostly they can’t receive appropriate pain treatment, if at all, until they become the “end-of-life” patients, or receive such treatment already in inpatient settings. Such an approach totally ignores the possibility of improving the quality of life of the patients in their home setting and does not allow them to pass their last period of life in dignity and without suffering and isolation.
Thus, it is strongly recommended that all groundless limitations and impediments be removed. Opioid Prescription Rules must be based on medical indications for pain treatment and must follow WHO 3 step analgesic ladders’ recommendations³⁵,³⁶. The regulations must use clear language to avoid ambiguity. National Palliative Care Program for Incurable Patients should not restrict the eligibility of outpatients to the “end of life” and service duration strictly to the 3–6-month period. The focus must shift from incurable diagnosis to quality of life and functional assessment of the patients.
Amendments to regulations and elimination of needless restrictions can also increase the role of the Primary Health Care Sector to ensure maximal access to pain relief and quality palliative care for outpatients.
Conflicts of Interest
The author has no conflicts of interest to declare.
Acknowledgements
None
References
1. Munday D, Dale J, Murray S. Choice and place of death: individual preferences, uncertainty, and the availability of care. J R Soc Med. 2007; 100(5):211-215. doi:10.1177/014107680710000509
2. Higginson IJ, Sen-Gupta GJA. Place of Care in Advanced Cancer: A Qualitative Systematic Literature Review of Patient Preferences. https://home.liebertpub.com/jpm. 2005;3(3):287-300. doi:10.1089/JPM.2000.3.287
3. WHO, WPCA. Global Atlas of Palliative Care at the End of Life.; 2014. Accessed August 3, 2018. www.ehospice.com
4. World Health Organization. Strengthening of Palliative Care as a Component of Integrated Treatment throughout the Life Course. J Pain Palliat Care Pharmacother. 2014;28(2):130-134.
doi:10.3109/15360288.2014.911801
5. Palliative care. Accessed May 6, 2025. https://www.who.int/news-room/fact-sheets/detail/palliative-care
6. WHO. Astana Declaration. Published 2018. Accessed July 29, 2020.
https://www.who.int/primary-health/conference-phc/declaration
7. WHO. National cancer control programmes : policies and managerial guidelines. Published 2002. Accessed March 21, 2025. https://iris.who.int/handle/10665/42494
8. WHO. Integrating Palliative Care and Symptom Relief into Primary Health Care.; 2018. Accessed November 3, 2018. http://www.who.int/servicedeliverysafety/en
9. Gomes B, Calanzani N, Curiale V, Mccrone P, Higginson IJ. Effectiveness and cost-effectiveness of home palliative care services for adults with advanced illness and their caregivers. Cochrane Database Syst Rev. 2013;2016(3). doi:10.1002/14651858.CD007760.PUB2
10. Maresova P, Hruška J, Randlova K, Rezny L, Carrillo-de-la-Peña MT, Kuca K. Systematic Review of the Cost-Effectiveness of Home-Based Palliative Care Interventions in Patients with Cancer: A Critical Analysis. Cancer Manag Res. 2024;16:1155-1174. doi:10.2147/CMAR.S472649
11. Stjernswärd J, Foley KM, Ferris FD. The Public Health Strategy for Palliative Care. J Pain Symptom Manage. 2007;33(5):486-493. doi:10.1016/j.jpainsymman.2007.02.016
12. International Narcotics Control Board (INCB). Narcotic Drugs — Estimated World Requirements for 2024 — Statistics for 2022. Published online 2023. Accessed March 21, 2025. www.incb.org
13. Kiknadze N, Dzotsenidze P. Palliative Care Development in Georgia. J Pain Symptom Manage. 2018;55:S25-S29. doi:10.1016/j.jpainsymman.2017.03.021
14. Deaths – National Statistics Office of Georgia. Accessed April 15, 2025.
https://www.geostat.ge/en/modules/categories/320/deaths
15. ძოწენიძე ფატი, რუხაძე თამარი, აბესაძე იოსებ. “ქრონიკული ტკივილის მართვის.”; 2012. Accessed July 30, 2018. http://www.moh.gov.ge/uploads/guidelines/2017/06/02/9bdedb3c90dcec579e7f9a0f589eafaf.pdf
16. Pati Dzotsenidze T. ქრონიკული ტკივილის მართვაში არსებული ბარიერების შეფასება და მათი ზემოქმედება სამედიცინო მომსახურების ხარისხზე. ივანე ჯავახიშვილის სახელობის თბილისის სახელმწიფო უნივერსიტეტი.; 2019.
17. Cherny NI, Baselga J, de Conno F, Radbruch L. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Europe: a report from the ESMO/EAPC Opioid Policy Initiative. Ann Oncol. 2010;21(3):615-626. doi:10.1093/annonc/mdp581
18. Cherny NI, Catane R, Kosmidis PA. Problems of opioid availability and accessibility across Europe: ESMO tackles the regulatory causes of intolerable and needless suffering. Ann Oncol. 2006;17(6):885-887. doi:10.1093/annonc/mdl073
19. Cherny NI, Cleary J, Scholten W, Radbruch L, Torode J. The Global Opioid Policy Initiative (GOPI) project to evaluate the availability and accessibility of opioids for the management of cancer pain in Africa, Asia, Latin America and the Caribbean, and the Middle East: introduction and methodology. Ann Oncol. 2013;24(SUPPLEMENT11): xi7-xi13. doi:10.1093/ANNONC/MDT498
20. International Narcotics control Board. Technical Reports. Narcotic Drugs – Technical Report. Published 2021. Accessed October 7, 2022. https://www.incb.org/incb/en/narcotic-drugs/Technical_Reports/narcotic_drugs_reports.html
21. UN, INCB. 2010 INTERNATIONAL NARCOTICS CONTROL BOARD Ensuring Adequate Access for Medical and Scientific Purposes UNITED NATIONS.; 2010. Accessed July 31, 2018. www.incb.org
22. Aaron Gilson, David Joranson, Karen Ryan, Jody Garthwaite JK. Achieving Balance In State Pain Policy, A Progress Report Card.; 2006. doi:10.1097/01.JTN.0000315778.97341.9a
23. PPSG APMG. Drug Control and Access to Medicines (DCAM).; 2009. Accessed July 30, 2018. http://apmglobalhealth.com/sites/apmglobalhealth.com/files/projects/docs/compendium.pdf
24. Connor SR. The global atlas of palliative care at the end of life: An advocacy tool. Eur J Palliat Care. Published online 2014. doi:10.1159/000440690
25. Worldwide Palliative Care Alliance. Accessed April 27, 2025.
https://repository.gheli.harvard.edu/repository/11295/
26. ნარკოტიკული ანალგეტიკებით სიმპტომურ მკურნალობაზე მყოფი კონტინგენტის საჭიროებისათვის ნარკოტიკული საშუალებების შენახვის, აღრიცხვის, დანიშვნის, გამოწერის, გაცემისა და გამოყენების დროებითი წესების დამტკიცების შესახებ | სსიპ ”საქართველოს საკანონმდებლო მაცნე”. Accessed April 22, 2021. https://matsne.gov.ge/ka/document/view/1065520?publication=0
27. ბრძანება32-102სშჯსსს, შსს2000. Joint Decree of MLHSA an MIA 32-102.pdf.
28. Dzotsenidze P, Abesadze I, Maurer MA, et al. Identifying barriers and contradictions in laws affecting pain management in Georgia. Transl Clin Med – Georg Med J. 2018;3(2):19-30. doi:10.29088/TCM-GMJ.2018-2.19
29. Dzotsenidze P, Lekashvili T, Chikhladze N, Jorbenadze M, Abesadze I, Kordzaia D. Impact of Ambiguous and Restrictive Regulations on Opioid-Prescribing Practice in Georgia. J Pain Symptom Manage. Published online March 2018. doi:10.1016/j.jpainsymman.2018.03.018
30. Cherny NI, Baselga J, de Conno F, Radbruch L. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Europe: A report from the ESMO/EAPC opioid policy initiative. Ann Oncol. Published online 2010. doi:10.1093/annonc/mdp581
31. SHAVDIA N, DZOTSENIDZE P, SHAVDIA N. CANCER PAIN AND ITS MANAGEMENT WITH OPIOIDS IN GEORGIA. Exp Clin Med Georg. 2022;(8). doi:10.52340/JECM.2022.08.17
32. OSGF. Assessment of Palliative Care Services – სამოქალაქო საზოგადოების ფონდი. Published 2021. Accessed March 22, 2025. https://csf.ge/en/assessment-of-palliative-care-services/
33. Global Data Platform to Calculate SHS and Palliative Care Need – IAHPC. Accessed March 22, 2025. https://iahpc.org/research/global-data-platform-to-calculate-shs-and-palliative-care-need/database/
34. Marie Knaul F, Farmer PE, Krakauer EL, et al. The Lancet Commissions Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: the Lancet Commission report. Lancet. 2018;391:1391-1454. doi:10.1016/S0140-6736(17)32513-8
35. Anekar AA, Hendrix JM, Cascella M. WHO Analgesic Ladder. J R Coll Physicians Edinb. 2023; 38(3):284. doi:10.1007/978-3-642-28753-4_102537
36. WHO, 1986. Cancer Pain Relief. Accessed July 29, 2018.
http://apps.who.int/iris/bitstream/handle/10665/43944/9241561009_eng.pdf