





Optimizing Elderly Trauma Care in Emergency Medicine
The Role of Emergency Department Physicians in Optimizing the Care and Management of the Elderly Trauma Patients
Tarik Wasfie, MD FACS¹, Hussein Mazloum MD FACS², Hope Welter OMS-IV³, Steven Vance MD⁴
- Clinical Professor of Surgery Michigan State University-COM and Clinical Professor of Surgery Central Michigan University Medical School
- Director of Trauma Corewell Health – Trenton Hospital – Trenton, Michigan
- Kirksville College of Osteopathic Medicine, A.T. Still University, Kirksville, Missouri USA
- Associate Dean of Student Affairs Central Michigan University Medical School, Emergency Department Physician
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: Wastie, T., et al., 2025. The Role of Emergency Department Physicians in Optimizing the Care and Management of the Elderly Trauma Patients: a 10-year Community Hospital Experience. Medical Research Archives, [online] 13(5).
https://doi.org/10.18103/mra.v13i5.6556
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6556
ISSN 2375-1924
ABSTRACT
INTRODUCTION:
Emergency department (ED) physicians are positions at a critical place in the management of the elderly trauma patient, however their contribution can reach far beyond the ED room. We reviewed here the results of guidelines and recommendations utilized to care for our elderly trauma patients.
METHODS:
A retrospective analysis of patients seen in the ED between 2012-2022. In addition to geographical data collected are length of stay, morbidity, mortality, medications used, comorbid conditions. Statistical analysis using students t-test, chi square and regression analysis with a significant “p” value at less than 0.05. Internal Review Board approval was obtained prior to the studies.
RESULTS:
Of 375 elderly patients with fragility fracture seen in the ED, those who referred to the fracture liaison service (FLS) showed significant reduction in the refracture rate (p < 0.01) compared to those before establishment of the FLS. Those elderly patients with traumatic brain injury (TBI) who sustained less than 4 mm bleed and were not on anti-coagulation therapy can safely be observed in the ED for less than 23 hours and don’t need a repeat CT scan or neurosurgery consult. The presence of skull fracture is an ominous sign and should raise the ED physician’s suspicion for worse things to come.
CONCLUSIONS:
Emergency department physicians’ role in the care of the elderly trauma patients can reach far beyond the immediate ED room treatment. When these recommendations and guidelines are implemented, it will have a positive long-term influence on the elderly trauma patient.
Keywords
Emergency department, elderly trauma patients, patient care, management
INTRODUCTION
Emergency department (ED) physicians carry by far the highest responsibility in the immediate patient’s care and ultimately outcomes as they are positioned at the forefront of emergency medical situations patients encounter, including the trauma and disastrous response. However, the credit given to the ED physician is vastly underappreciated and undervalued, and considered by many as a referral station. This false perception and the attitude by many in the ED that the sooner a patient is transferred to inpatient care, the better, so as to vacate another room for another patient which enforces the existing perception. Nonetheless, present-day ED physicians increasingly contribute to optimizing patient care and making their decision based on improving patient outcome for the foreseeable future. Elderly patients are a unique group of patients whom we increasingly see now in the ED following traumas. As the United States and the world population expand and with the great advances in healthcare in the last decade, the average age of longevity increased for both male and female, and so as the cost of taking care of them. A higher number of elderly trauma patients visited the ED annually and the care of them becoming more complicated and of higher magnitude¹,³, as they arrive with multiple comorbid conditions and array of medications which may need to be adjusted as circumstances dictate. On the other hand, ED physicians have to utilize the available resources efficiently and to the best of the patient wellbeing, and with that, the steps taken by the ED physician will go very far in improving future wellbeing of the patients. The aim and scope of this article is to discuss the resources and guidelines available to the ED physician to utilize as adjunct to the immediate critical care provided to the elderly trauma patient as well as to review the benefits gained when they are implemented in a timely fashion.
Methods
The enclosed studies are a retrospective analysis of patients seen between 2012-2022 in the emergency department of a community hospital. Data collected (in addition to geographical data) are length of stay (hospital and intensive care unit), readmission rate, morbidity and mortality, comorbid conditions, and medications used including anti-coagulation and beta-blockers.
Statistical analysis using students t-test, chi-square test, Pearson-fisher and multivariate regression analysis when indicated. A p value of less than 0.05 were considered statistically significant. Internal Board Review approval was obtained before conducting the studies.
Osteoporosis & Fragility Fracture / Fracture Liaison Service Program
Osteoporosis is defined as the loss of bone mineral density due to multiple factors such as advancing age and decreasing sex hormones⁴. Over 200 million people worldwide and 10.2 million in the United States⁵ are estimated to carry this diagnosis, with 70% of those over 50 years old being affected. This state of a weakened bone structure predisposes these patients to fractures and refracture, with increased risk found in those of female gender, history of prior fracture, and advanced age³.
One out of every two women over the age of 50 years old will have a fragility fracture at some point in their life⁶,⁷. The World Health Organization (WHO) defines a fragility fracture as a fracture of any bone in the body (except for the skull, feet and hand bones) caused by an injury that would not fracture a normal bone, such as a fall from standing⁸. Previous studies in the United States, Canada and Europe have found that women underestimate the risk of osteoporosis⁹. Common fragility fractures involve those of the hip, ribs and vertebrae in the geriatric osteoporotic population¹⁰. With an expected three-fold increase in the geriatric population expected in the next 30 years worldwide¹,³, there is an obvious concern for the economic and healthcare burden that will come with the surgical treatment of fragility fractures in this growing group of patients.
One solution to overcome this burden was introduced in the 1990s, the Fracture Liaison Service (FLS) program which aims to improve patient bone health and reduce refracture rates and readmission rates thus reducing rising expenditures in the geriatric population⁷,¹¹,¹². At our institution, an FLS program began in 2015 to follow up on vertebral compression fractures that required vertebroplasty or kyphoplasty. The goal was to help mitigate risk of a future fracture by reducing personal and hormonal risk factors which has shown to reduce fragility refracture rates⁷,¹¹–¹³.
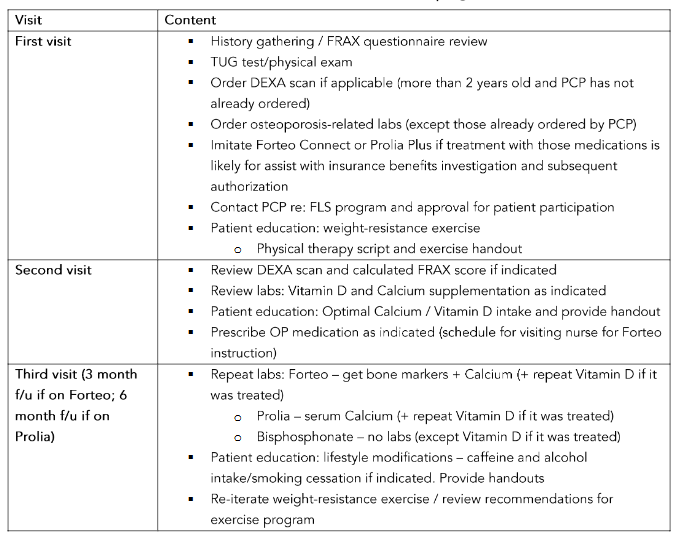
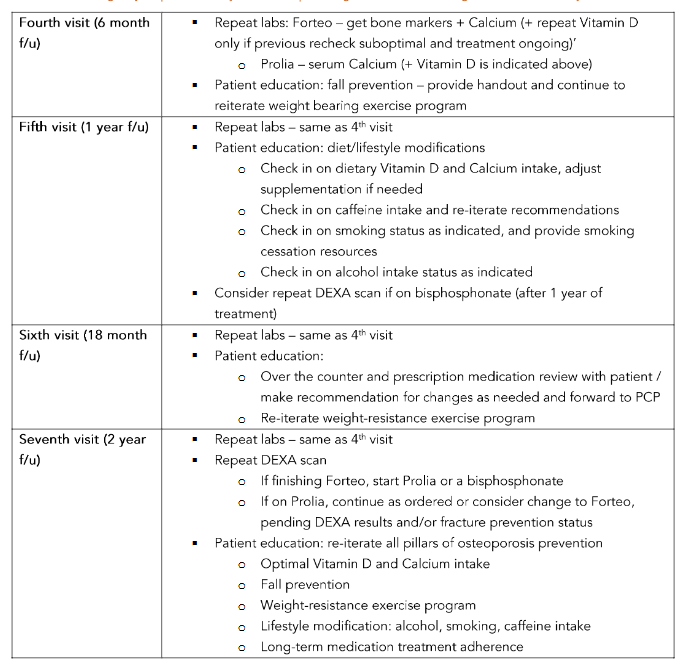
Figure 1: Fracture Risk Assessment
Trauma Brain Injury
The most common method of traumatic injury in the elderly patient is a fall from standing, with increased risk of bleed particularly in those with the pre-usage of anti-coagulation therapy¹²–¹⁴. Currently we adapted the following guidelines for brain injury management (Table 2)¹⁵.
These guidelines were implemented between 2017 and 2021 at our institution, and a retrospective analysis of 542 elderly trauma patients with head injury seen in the ED were collected and studied to review the success of the BIG protocol. The use of two patient groups represented the period before and after BIG protocol administration, with Group 1 as the pre-BIG protocol group and the latter Group 2 as the BIG protocol group. From this study, we concluded that the BIG protocol guidelines and criteria were safe for management of major elderly trauma patients in a level II trauma center following the protocol in the outlined table (Table 2). Though an overall cost reduction was found by reducing length of stay, there was an added requirement of a 23-hour maximum holding in observation for the BIG 2 group. Due to the difficulty and practicality faced in holding for more than 6 hours in the ED,further studies should implement with a larger sample size for better generalizability¹⁶.
Table 2. Brain Injury Guidelines
LOC: loss of consciousness; CAMP: Coumadin, Aspirin, Plavix; SDH: subdural hemorrhage; SAH: subarachnoid hemorrhage; IVH: intraventricular hemorrhage; RHCT: repeat head CT; NSG: nonsurgical.
The Glasgow Coma Scale (GCS) is commonly used to prioritize patients and determine the need for neurosurgical intervention through grading traumatic brain injuries (TBI) as mild (GCS 13-15), moderate (GCS 9-12), or severe (GCS ≤ 8). Nonetheless, GCS scores in the elderly may not accurately predict prognosis due to the fact that the brain atrophy in the elderly leads to increased unoccupied intracranial space for bleeds. Along with this, the elderly face a higher risk for TBI and intracranial hemorrhage (ICH) following low velocity mechanisms (i.e. fall). Their risk is most often increased further due to
anticoagulation use resulting in a lower rate of timely neurosurgical intervention in those elderly patients with low injury severity scores (ISS) leading to increased morbidity and mortality¹⁷.
Studies have shown that early detection and treatment of TBI improve patient outcomes. We investigated TBI patients to identify the factors that influence outcomes in elderly patients with low ISS and high GCS. Mortality in TBI was higher in elderly patients, possibly due to multiple comorbid conditions that decrease physiologic reserve. Further, it was found that lower trauma activation levels, inappropriate triaging and delayed treatment increased intensive care unit (ICU) and hospital length of stay, leading to higher patient burden and morbidity that continued after discharge¹⁸. In conclusion, it is recommended that the ED physician considers triaging an elderly patient with minor trauma and a high GCS at a higher level.
In 30% of cases of epidural hematomas (EH), the clinical course is as follows: loss of consciousness, lucid interval, rapid deterioration of mental status due to rapid increase in the intracranial pressure with resultant of midbrain herniation and respiratory arrest¹⁹. Though the mainstay of treatment is surgery, nonsurgical conservative management has shown to be successful. Our retrospective analysis²⁰ aimed to study the management outcomes of elderly patients with acute traumatic EH, specifically looking for factors that lead to success and failure of conservative therapy in this population. At our level II trauma center, conservative management included a GCS score and head CT on arrival to the ED with subsequent follow up CT within 24 hours. These patients were admitted to the Neuro-Trauma intensive care unit for monitoring. We were able to conclude that in the elderly traumatic EH patient, select patients can be managed nonsurgically, as long as there is no significant progression of the hematoma with follow up CT and GCS. It is important to note that associated skull fractures were shown to be a potential threatening sign.
Post-discharge program: strength, eye care, environment, medication (S.E.E.M.)
Traumatic brain injury (TBI), particularly in the elderly patient, carries with it a high mortality and morbidity¹³. Furthermore, the readmission rate of those patients who suffered from TBI run around 30%, with either a secondary fall or sequela from chronicity of the original TBI²¹.
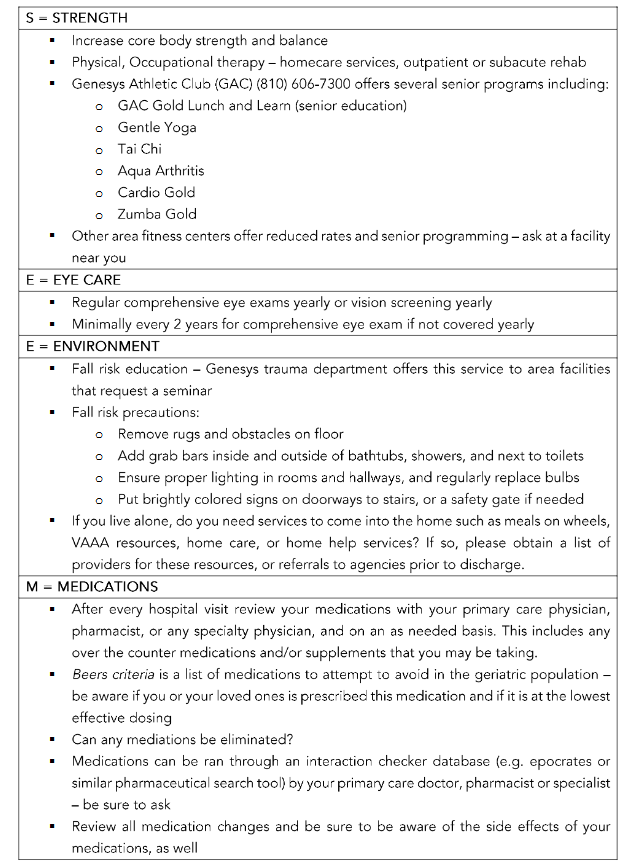
In order to improve outcomes of the elderly trauma patient population at our community hospital, we implemented the S.E.E.M discharge program to focus on prevention of re-injury and subsequent readmission. The S.E.E.M. program provides patient education on strength, eye care, environment, and medications. The strength section focuses on fitness education via programs at our athletic center and/or encouraging physical therapy/occupational therapy. In terms of eye care, patients are recommended to have eye exams yearly or as frequent as their insurance will allow. Environmentally, the program focuses on fall risk precautions and access to resources for those who live alone. Finally, the medications section prompts patients to see their primary care providers on a regular basis to review their medication lists to check for interactions, talk about possible eliminations, and learn about potential side effects so that the elderly population can be aware of the safety profile of their medications. In our center, elderly patients receive this educational instruction with their discharge instructions (Table 3). In the ED, physicians and providers can take part in this effort by providing patients with the same information as the S.E.E.M. program to promote wellness and better patient health beyond their current visit to the trauma center.
Conclusion
Emergency department physicians play a pivotal role in care of the elderly trauma patient. That role is not just limited to emergency room visits, but far beyond the current treatment and well into their future care and well-being.
S.E.E.M. Discharge Program
Conflict of Interest:
The authors declared no conflict of interest. No support was provided for this study.
Acknowledgment:
The authors acknowledge the assistance of Debbie Cicchini for her tireless effort in obtaining the references needed.
References
1. Vincent GK, Velkoff VA, U.S. Census Bureau. The next four decades: The older population in the United States: 2010-2050. US Census Bureau, Department of Commerce. Economics and Statistics; May 2010. p. 25-1138 Administration Report.
2. Evans DC, Gerlach AT, Christy JM, et al. Pre-injury polypharmacy as a predictor of outcomes in trauma patients. Int J Crit Illn Inj Sci. 2011;1(2): 104-109. doi: 10.4103/2229-5151.84793
3. Miller AN, Lake AF, Emory CL. Establishing a fracture liaison service: An orthopaedic approach. J Bone Joint Surg Am. 2015;97(7):675-681.
4. Alswat KA. Gender disparities in osteoporosis. J Clin Med Res. 2017;9(5):382-387. doi: 10.14740/jocmr2970w
5. US Preventive Services Task Force, Curry SJ, Krist AH, et al. Screening for osteoporosis to prevent fractures: US preventive services task force recommendation statement. JAMA. 2018;319(24): 2521-2531. doi: 10.1001/jama.2018.7498
6. Brenneman SK, Barrett-Connor E, Sajjan S, Markson LE, Siris ES. Impact of recent fracture on health-related quality of life in postmenopausal women. J Bone Miner Res. 2006;21(6):809-816. doi: 10.1359/jbmr.060301
7. Jackson A , Wasfie T, Brock C, et al. Fragility Vertebral Compression Fractures in Postmenopausal Women: The Role of a Fracture Liaison Service Program. The American Surgeon 2020; 86(12) 1636-1639. Doi: 10.1177/0003134820933254
8. Kanis JA on behalf of the World Health Organization Scientific Group (2007). Assessment of osteoporosis at the primary health-care level. Technical Report. World Health Organization Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK. 2007:Printed by the University of Sheffield.
9. Singer A, Exuzides A, Spangler L, et al. Burden of Illness for osteoporotic fractures compared with other serious diseases among postmenopausal women in the United States. Mayo Clin Proc. 2015; 90(1):53-62. doi: 10.1016/j.mayocp.2014.09.011.
10. Lyritis GP, Mayasis B, Tsakalakos N, et al. The natural history of the osteoporotic vertebral fracture. Clin Rheumatol. 1989;8 Suppl 2:66-69. doi: 10.1007/BF02207237
11. Wasfie T, Jackson A, Brock C, et al. Does a fracture liaison service program minimize recurrent fragility fractures in the elderly with osteoporotic vertebral compression fractures? The American Journal of Surgery 2018.
http://doi.org/10.1016/j.amjsurg2018.09.027
12. Frontera JA, Egorova N, Moskowitz AJ. National trend in prevalence, cost, and discharge disposition after subdural hematoma from 199/2007. Crit Care Med. 2011;39(7):1619-1625.
13. Kalanithi P, Schubert RD, Lad SP, Harris OA, Boakye M. Hospital costs, incidence, and hospital mortality rates of traumatic subdural hematoma in the United States. J Neurosurg. 2011;115(5):1013-1018.
14. Canner JK, Giuliano K, Gani F, Schneider EB. Thirty-day re-admission after traumatic brain injury: Results from MarketScan. Brain Inj. 2016;30 (13-14):1570-1575.
15. Joseph B, Aziz H, Pandit V, et al. Prospective validation of the Brain Injury Guidelines: managing traumatic brain injury without neurosurgical consultation. J Trauma Acute Care Surg. 2014;77 (6): 984-988.
16. Wasfie T, Korbitz H, Odowd B, et al. Validation of Brain Injury Guidelines in the Elderly Trauma Patient Presenting at a Level Two Trauma Center. The American Surgeon. 2023; 0(0) 1-3. doi: 10.1177/0003134823161676
17. Kehoe A, Smith JE, Bouamra O, Edwards A, Yates D, Lecky F. Older patients with trauma brain injury present with a higher GCS score than younger patients for a given severity of injury. Emerg Med J 2016;33(6):381-5.
https://doi.org/10.1136/emermed-2015-205180
18. Bick H, Wasfie T, Labond V, et al. Traumatic brain injury in the elderly with high Glasgow coma scale and low injury severity scores: Factors influencing outcomes. American Journal of Emergency Medicine 2022; 51, 354-357.
19. Hamilton M, Wallace C. Nonoperative management of acute epidural hematoma diagnosed by CT: the neuroradiologist’s role. Am J Neuroradiol. 1992:13(3):853-859.
20. Wasfie T, Ho T, Shapiro B. Acute Traumatic Epidural Hematoma in the Elderly: A Community Hospital Experience. The American Surgeon 2020; 00(0) 1-2. doi: 10.1177/0003134820943117.
21. Zatzick DF, Rowhani-Rahbar A, Wang J, Russo J, Darnell D, Ingraham L, et al. The cumulative burden of psychiatric substance use and medical disorders and re-hospitalization and mortality after injury. Psychatr Serv. 2017 June 01:68(6):596-602