

Optimizing Medication Turnaround Time in Hospitals
Optimizing Medication Turnaround Time in Hospital Pharmacies: A Systematic Review important, factors and Solutions
Mohammed Almeziny¹, Raghad Alkhodair¹, Nuha Aldawsari², Salem Almeziny³, Abdullah Almeziny⁴, Majdoly Alkhodair⁵
- Prince Sultan Military Medical City
- King Saud Bin Abdulaziz University for Health Sciences, College of Public Health and Health Informatics
- Almaarefa University, College of Medicine
- Imam Mohammad Ibn Saud Islamic University, College of Medicine
- King Saud University, College of Medicine
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Almeziny, M., Alkhodair., R., Aldawsari, N., et al. Optimizing Medication Turnaround Time in Hospital Pharmacies: A Systematic Review important, factors and solutions. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6942
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6942
ISSN 2375-1924
ABSTRACT
Background: Medication turnaround time (TAT) is a critical metric for evaluating the efficiency and safety of hospital pharmacy operations. Optimizing TAT is essential to ensure patient safety, reduce medication errors, enhance workflow efficiency, enhance resource utilization and enhance both the continuity of care and patient satisfaction.
Aim: To discuss the important of TAT, factors influencing medication TAT and provide evidence-based recommendations to optimize medication delivery thereby improve patient care.
Methods: A comprehensive search of PubMed, Google Scholar, and ScienceDirect was conducted up to June 15, 2025. Eligible studies included if they were conducted in inpatient settings and reported medication TAT as outcome. Outpatient studies and those without relevant data were excluded. Data on study characteristics, interventions, and outcomes were extracted and summarized narratively; no meta-analysis was performed due to the heterogeneity of the studies.
Results: Analysis identified several determinants of prolonged TAT included inefficient health IT systems, inadequate communication, staffing limitations, and inconsistent workflows. Effective interventions encompassed automation, workflow redesign, staff role optimization, and process standardization. These strategies consistently reduced TAT, with reported improvements of 10% to over 50%.
Conclusion: TAT is a fundamental indicator to measure hospital pharmacy performance and improve patient outcomes. Addressing the barriers through evidence-based strategies can significantly streamline the medication use process. Optimizing medication TAT requires a multifaceted approach that integrates technology, standardized workflows, and improve human factors. Evidence suggests these approaches not only enhance operational efficiency but also reduce errors, strengthen regulatory compliance, and ultimately improve patient safety as well as satisfaction.
Keywords
Medication Turnaround Time, Hospital Pharmacy, Systematic Review, Healthcare Efficiency, Medication Use Process
Introduction
Rationale
The primary expectation of the hospital pharmacy department is to ensure that the correct medication is available at the appropriate time. Monitoring medication turnaround time (TAT) in inpatient settings enables institutions to assess the efficiency of patient care delivery. Evaluating time definitions within clinical processes can support the analysis of workflows in the Medication Use Process (MUP) and help identify potential vulnerabilities e.g., bottlenecks. Given the rising costs and growing demands on healthcare systems, enhancing the efficiency of clinical workflows has become increasingly important. When examining process times, it is essential to recognize the various definitions applied to different time intervals. Agency for Health Research and Quality (AHRQ) define TAT as “the interval from the time a medication order is written (manually or electronically) to the time the medication was administered”. TAT measure falls under the category of workflow impact and relates to the quality domain of efficiency.¹
Medication turnaround time is one of the most commonly used metrics for evaluating pharmacy, laboratory, or pathology services. Since the 1980s, it has been widely applied to objectively quantify the time required to complete laboratory tests.² Furthermore, TAT can be divided into two main phases: the interval from when the order is entered to when the pharmacy verifies it, and the period from pharmacy verification to the delivery of the medication.³
The earliest reference, dating back to 1971, defined TAT as the interval between the printing of an electrocardiogram and the placement of the resulting printout into the patient’s medical chart.⁴ In the laboratory workflow TAT is an important indicator of performance and is even seen as a necessary condition for trust between patient and physician.⁵,⁶ TAT in healthcare systems has been the focus of extensive research and publications on examples for publications reported TAT in radiology workflow,⁷ TAT for processing medication orders¹ or patient cycle time⁸ demonstrate that these process indicators are not limited to pharmacy, pathology or laboratory services. These parameters can be used for all clinical processes monitoring and benchmarking.
Delays can have devastating consequences, posing serious risks to patient safety. Improving medication TAT can help providers adhere more effectively to evidence-based guidelines, particularly in situations where timely medication administration is critical to patient care. For instance, in antimicrobial therapy, the “golden hour” is a term adapted from emergency medicine that refers to the critical first hour after recognition of severe infection, particularly sepsis or septic shock, during which the prompt administration of appropriate antimicrobial therapy is associated with significantly improved survival outcomes. Research shows that delays in administering effective antibiotics beyond this “golden hour” can dramatically increase mortality rates in patients with septic shock and severe bacterial infections.⁹–¹¹
According to the Institute for Safe Medication Practices (ISMP) and the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP),¹² medication errors can be classified into omission errors and commission errors. Omission errors refer to the failure to perform a necessary action for example, when a patient does not receive a scheduled antibiotic dose or a pharmacist fails to dispense an ordered medication. In contrast, commission errors involve performing an incorrect action, such as administering the wrong drug, the wrong dose, or delivering it via the incorrect route. As a result, prolonged TAT may lead to omission errors.
Objective
The primary objective of this systematic review is to examine the cultural and organizational significance of medication TAT, identify factors that influence TAT within hospital pharmacy settings, and propose evidence-based recommendations to reduce it.
Methods
Eligibility Criteria
Inclusion criteria
Study design: Quantitative, qualitative, or mixed-methods studies.
Population: Inpatient care settings, including hospital wards, emergency departments, and Intensive Care Units.
Interventions: Any intervention aimed at influencing or improving medication TAT time, regardless of its nature or complexity.
Outcomes: Studies had to report medication TAT as a primary or secondary outcome.
Exclusion Criteria:
Studies conducted in outpatient settings.
Studies that did not report TAT.
Information Sources and Search Strategy
A comprehensive search was performed in PubMed, Google Scholar, and ScienceDirect. The final search was completed on June 15 2025. The following core terms were combined with Boolean operators (AND/OR) and adapted for each database: “turnaround time,” “medication process,” “inpatient pharmacy,” “dispensing efficiency,” “pharmacy automation,” “medication errors,” “pharmacy redesign,” and “standardization.”
Study Selection
In order to simplify the search process, members of the review team conducted independent searches in one assigned database using standardized keywords. The retrieved citations were imported into EndNote reference management software, where duplicate records were identified and removed. Titles and abstracts were then screened according to predefined inclusion and exclusion criteria for relevance. Following this, full texts of potentially eligible studies were retrieved and reviewed in detail. Studies that failed to meet the eligibility criteria were excluded.
Data Extraction
A structured data extraction form was used by a single reviewer to extract data. In each study reviewed in this review, the following variables were collected:
-
Author(s)
-
Year of publication
-
Study design
-
Sample size
-
Type of intervention(s)
-
TAT outcome
-
Key findings
Quality Assessment
Given that the objective of the review was to systematically map the existing evidence across a variety of study types without limiting inclusion based on quality appraisal criteria, methodological quality or bias was not formally assessed in the studies included in the review.
Data Synthesis
Data synthesis were not conducted; nor were statistical pooling or meta-analysis, as feasible. The findings from included studies were summarised in a table format to provide a comprehensive summary of key characteristics, types of interventions, and reported impacts on medication TAT. Given the variability in study design, type of intervention, and measures of outcomes, no quantitative synthesis or formal thematic analysis was generated.
Result
Study Selection
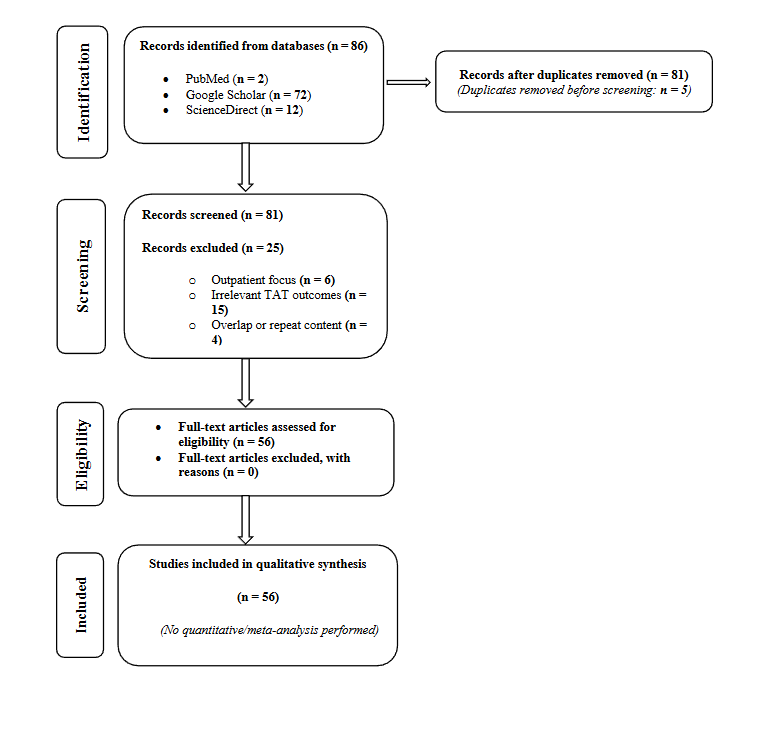
Following database searching, 86 studies were identified, including 2 from PubMed, 72 from Google Scholar, and 12 ScienceDirect. After deduplication there were 81 records that were selected for screening of titles and abstracts. Of these, 25 were excluded for not meeting the inclusion criteria for the review. The studies were excluded at this stage were predominantly; outpatient (n = 6), no relevant TAT outcomes (n = 15), and overlap or repeat content between documents (n = 4). Thus, there were 56 studies in the final synthesis. The study selection is shown in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow chart.”
Study Characteristics
The studies selected spanned publications from 1971 to 2025 in diverse health care systems. The studies were conducted in a variety of hospital inpatient environments including tertiary hospitals, teaching hospitals, emergency departments, and intensive care units. The studies took the form of observational studies, quality improvement, case studies, and systems focused evaluations.
Interventions to Improve Medication Turnaround Time
Five prominent forms of intervention were applied across the studies at different stages of the MUP:
Automation and Health Information Technology:
There was widespread use in hospitals of automated dispensing cabinets (ADCs), barcoding systems and closed-loop electronic medication management with varying effectiveness. Overall, these advancements led to quicker access to medication and engagement with workflow tracking.
Redesign and Workflow Methods:
An organized process used redesign and workflow improvement strategies to eliminate waste in workflows to improve efficiency. These strategies were able to be implemented and were able to achieve a significant reduction in TAT and overall process performance improvements.
Role Optimization and Staff Reassignment:
Several strategies that sped up the number of medications delivered included the use of pharmacy runners, embedding pharmacists on ward, and improved communication within pharmacy and clinical teams.
Digital Tracking and Communication:
Team members effectively tracked orders in real-time or informed their workload regarding monitoring orders and addressing delays with installed digital dashboards, automated alerts, and tracking capabilities.
Standardized Medication Processes:
Standard work processes were employed to reduce variability by protocol for stat doses, ICU medications, and high-risk drugs were created and implemented, thereby, reducing response time.
Intervention Outcomes
The majority of studies concluded that interventions had significant reductions in medication TAT, from 10% to over 50%. The most effective occurred in environments combining technology with standard work processes and optimal management of staffing. A few studies were at first restricted by resistance from managers to adopt new processes or limited infrastructure, and later overcame the barriers to full implementation. No study reported worsening TAT post interventions. The studies show that regimented structured and collaborative strategies can reduce medication delivery timelines for medications provided through hospitals.
Discussion
The significance of turnaround time in hospital pharmacies:
Patient Safety and Prevention of Medication Error
Late delivery of medications can have an enormous impact on patient safety. TAT and medication errors have a well-documented relationship. An optimized TAT can ensure medications are processed and delivered without delay to reduce possibilities for errors related to mistakes manual processes, and rush workflows if delays occur. A prolonged TAT can result in work arounds, manually overriding, or verbal orders are used to speed up the delivery, as these factors can increase the risk for medication errors. Administering medications at the appropriate time can protect patients from the harmful consequences associated with prolonged TAT.¹³–¹⁵
Operational Efficiency
When it comes to pharmacy operations, TAT is considered a key performance indicator (KPI) for pharmacy performance. Medication TAT: a metric that gives insight into the operational efficiency of a healthcare system’s mainly MPU. An optimized
TAT equals workflow efficiency, less bottlenecks, maximizing resources from prescription to administration. Long TAT is a sign of inefficiency such as duplicated work, manual processes, miscommunication, staffing issues that leads to wasted time and resources, these resources could be better spent on patient care. By evaluating TAT, healthcare systems can identify workflow inefficiencies, eliminate waste, utilize their staff appropriately, and deliver services in a more efficient manner.¹⁶,¹⁷
Cost Management
Inefficiencies TAT can cause longer stays and higher labor expenses. An optimized TAT is not a direct cost measure but it shows that processes are working effectively and efficiently, reducing waste, and eliminating unnecessary costs due to increase labor costs as result of staff spending too much time inquiring about delayed medication, double checking many times, or dealing with complaints from patients about waiting for medication. In addition to medication delays prolonging stays for inpatients, especially for those patients who have been discharged but are waiting for medications, that delays bed utilization, and leads to longer stays that increase inpatient costs.¹⁸
Continuity of Care
Medication turnaround time significantly influences continuity of care and is an important factor to determine the effectiveness and safety of clinical interventions. Ontime delivery of medications, in a healthcare setting, ensure patients receive their medication therapy as intended, and on time delivery is important to be maintained with minimal or no interruptions in treatment to preserve the effectiveness of the medication, to prevent worsening of chronic illnesses, or to address acute medical episodes.¹⁹ A delay in TAT can lead to gaps in treatment and ultimately may lead to poor patient outcomes, suffering, longer hospitalization, and an increased risk of complications or adverse events.²⁰,²¹ The consideration of continuity is also important during transfers of care (e.g., patient admission to a hospital, patient transfer from level of care to another, or patient discharge). Continued and on time access to medications will provide more effective continuity of care.²²
Patient Satisfaction
How fast and accurately the medication is delivered can influence a patient’s perception of the quality of care he/she is receiving, an always short TAT results in better patient and provider satisfaction, reinforces trust in the healthcare system, and better patient adherence toward their therapy.²³–²⁵ Liew et al²⁶ demonstrated that reorganizing the pharmacy workflow in Malaysia significantly reduced patient waiting times and medication near misses, leading to improved patient satisfaction. In the same way, Yulia et al²⁵ demonstrated that waiting time is determined. Therefore, performance monitoring was advocated as a feedback loop for enhancing pharmacy services and increase patient satisfaction.
Regulatory Compliance
Medication turnaround time is critical for regulatory compliance in an inpatient pharmacy environment. Regulatory compliance with regard to the management of medication within the unit, by various accreditation bodies (e.g., The Joint Commission (TJC)), and governmental agencies is inherently related to the safe and timely provision of medication.²¹,²⁷ Institutional compliance with evidence-based standards and guidelines from organizations like TJC may require timely medication initiation but may not provide a specific TAT numerical target for all medications. Instead, compliance may require facilities to have sufficient systems in place to ensure that all medications, and in particular non-formulary, urgent, and time-critical medication, be prepared and delivered within clinically appropriate time frames.²⁸,²⁹ TAT delays can be categorized as systems failures which can contribute to non-compliance findings in surveys. Many of these accreditations require hospitals to establish
policies and procedures related to TAT acceptable for different medication groups, and to continuously monitor these measures for improvement.³⁰ By not achieving the internal or industry benchmarks or with frequent medication delays, may signify a breakdown in the management of medication administration and may compromise patient safety during medication management in the inpatient pharmacy, and can lead to negative accreditation findings, fines, and even loss of license. Therefore, medication TAT directly is a reflection of an inpatient pharmacy’s effectiveness related to regulatory compliance and safety in patient care.
Factors affecting medication turnaround time in hospital Pharmacies:
Usability Issues and Workarounds
By definition, health information technologies such as computerized physician order entry (CPOE) and clinical decision support systems (CDSS) when designed properly, should improve efficiency, however, at least two studies have shown that to be inadequate goal that to limit by usability or system design that aligned poorly with clinical workflow.³¹,³² Khajouei et al³¹ identified that the non-intuitive order sets, and complex user interfaces contributed to longer order entry leading to longer medication processing times.³¹ It is also important to note that both studies found that users were abandoning safety checks or safety alerts or modifying standard workflows, resulting in variation to medication preparation and checking process and ultimately taking longer. Similarly, Niazkhani et al³² found significant workaround behaviors of physicians and nurses because of insufficient flexibility of the system. It was concluded that a number of workaround behaviors, including entering verbal orders outside of the CPOE system or skipping mandatory documentation requirements, were acts of omission that compromised the safety of the system and contributed to delays, and possibly risks in the medication-use process.
Poor Communication and Information Gaps
Breakdowns in interdisciplinary communication between prescribers, pharmacists, and nursing staff represent a significant factor that affect medication delivery time. Chapman et al³³ found in a neonatal intensive care units that when transitioning to CPOE, delays in order verification and medication preparation due to poor communication and lack of real-time feedback loops were greatest during off hours and when the medication orders needed further clarification. Delays can also occur when uncertainty exists related to medication orders, incomplete patient information, and missing communications between prescribing clinicians, final dispensing pharmacists, and nursing staff as these factors also result in clarification calls, reviews of charts, or repeated follow-up calls that typically delay convert time into TAT.³⁴
Staffing Limitations and Role Confusion
Insufficient human resources, especially in pharmacy departments, is a significant contributor to delays in medication processes. Lorimer et al³⁵ reported a lack of specification of responsibilities between pharmacists, technicians and nurses in acute-care hospital environment led to repetitive tasks or confusion for all departments who would own a particular task, resulting in workflow interruption and delays in medication preparation. In addition, Hwang et al¹⁹ found shortage of pharmacy staff during high-demand periods prolonged delivery times and exacerbated patient discomfort related to delay of medication administration in pain management situation.
Lack of Workflow Consistency
Lack of workflow consistency and standardized operating procedures is identified to be a cause of TAT variability between departments. Raghuvanshi and Choudhary³⁶ found departments without a structured medication ordering process had inconsistent processing times for similar medications and emphasized the importance of standardizing workflows to ensure timely delivery. Similarly, Naylor et al²⁸ found that without a common definition of TAT, it was difficult to benchmark performance or implement quality improvements.
Factors Related to pharmacy location and Logistical Infrastructure
Limitations associated with infrastructure such as physical separation between hospitals and pharmacy units, slow or absent transportation systems, and manual delivery can all hinder TAT. Almalki et al¹⁴ noticed the significant logistical challenge created by the distance between centralized hospital pharmacies and inpatient care units. The proximity of the pharmacy to patient care units is a key determinant of TAT, particularly in large or multi-storied hospitals. When the pharmacy is remote from clinical units and handling a high volume of orders, the medication dispensing process is significantly hindered, increasing the risk of delays and potential errors. An underperforming or antiquated system used to deliver care, whether defined as long distances to travel, or manual delivery, will always delay TAT, which in turn delays patient care.³⁸
Resistance to Change and Insufficient Training
Successful implementation of new technology requires infrastructure and user buy-in. Many studies noted that poor training when launching systems were barriers to adoption and using the systems successfully. For instance, Cordero et al³⁹ noted that during the early implementation of CPOE in a neonatal intensive care unit, clinicians expressed confusion and frustration due to inadequate training which promoted increased reliance on paper-based and verbal orders to communicate that delayed medication processing. Furthermore, Cunningham et al⁴⁰ supported this finding, stating resistance from healthcare providers was largely due to their lack of engagement and the failure to integrate end-user feedback in the system design stage of a project.
Absence of Priority Mechanisms for Urgent Medications
Another contributing item seen in many articles was the absence of protocols or rules for prioritizing time-sensitive or emergent medication orders. Gabriel et al⁴¹ found that specialty pharmacies frequently experienced medication delays due to the lack of prioritization systems, where urgent orders were processed alongside routine ones without differentiation. The study concluded that the use of flags or automated prioritization algorithms that could direct preparation and delivery of urgent or critical medications, should be a standard practice in emergency and critical care units. The study indicated that visual flags or automated prioritization algorithms to direct the preparation and delivery of urgent or critical medications, should be a standard process in emergency and intensive care units.
Proposed solutions to reduce medication turnaround time
Classifying prescriptions
Classifying prescriptions enables pharmacists to prioritize the most time-sensitive prescriptions to STAT, As Soon As Possible (ASAP) and routine.⁴²,²⁸ This structured prioritization helps to reduce TAT for critical medications and ensure timely therapy initiation. In addition, American Society of Health-System Pharmacists (ASHP) guidelines emphasize the value of classifying medication orders to optimize operations and ensure resources are used effectively. By focusing attention where it is most needed, pharmacy teams can manage their workload more effectively.
However, a study conducted to evaluate the appropriateness of STAT prescriptions in emergency department in a tertiary hospital in Saudi Arabia revealed that 49.34% of the STAT prescriptions were inappropriately prescribed. Therefore, it is recommended to provide education for prescribers, establish clear criteria for medications that qualify for STAT ordering, and implement close monitoring of STAT dose utilization. Additionally, further studies should be undertaken to assess the consequences of inappropriate STAT orders.⁴³
Enhancing pharmacy workflow
In terms of pharmacy workflow optimization, there are also some changes that can lead to decreased TAT, in terms of workflow and physical redesign of pharmacy, specify staff roles, standardization, etc.
Workflow redesign: lean principles to eliminate wasteful steps, improve layout help and identified bottlenecks.⁴⁴ Additionally, A systematic review evaluated Lean Six Sigma strategies to improve hospital pharmacy workflows and service quality, guided by PRISMA standards and analyzing 1,447 studies (73 included, 2009–2023). Quality improvement and workflow optimization dominated managerial tactics. The review highlights the importance of lean leadership, quality practices, and strategic approaches to optimize hospital pharmacy operations globally.⁴⁵
Task delegation and staff roles: Clearly defining roles of each staff including pharmacists, technicians, and support staff reduces duplication and ensures faster processing of medication orders.³⁵
Standardization in pharmacy practice covers numerous aspects including the development and application of standard operating procedures, standard preparation concentrations, unified units of measurements, and evidence-based guidelines. Standardization resulted in safe, high-quality, and high-efficient care, medication-related care in all healthcare setting.
Standardizing reduces variability in the entire prescribing, dispensing, and administration processes, which decreases the variation in preparation time and enhances predictability in the medications prepared for patient use and medications delivered to the patient units. Standardized protocols and order sets also help prescribers to identify appropriate therapies faster and reduce back-and-forth interaction with pharmacy staff that usually requires clarifications.⁴⁶
Research suggests that standardizing medications preparation and compounding—primarily the use of ready-to-use or pre-prepared medications (primarily IV compounding) minimized the preparation and medication verification time. In addition, ready-to-use or pre-prepared medications can be stored in ADCs. The medications stored in ADCs provides fewer variables to process and faster times in medication delivery.³⁰
Standardized formulations and protocols have also provided opportunities to integrate pharmacy automation (e.g., ADC, robotic compounding) into pharmacy workflows, which have also reduced the number of manual interventions and subsequently reduced TAT.²⁷
Standardization, when properly executed, significantly reduces prescribing and compounding errors, hence minimizing the need for rework, directly improving TAT reduction associated delays required to resolve errors.⁴⁷
In summary, optimizing pharmacy workflows reduces medication TAT both directly and indirectly by standardizing processes, which enhances efficiency, minimizes human error, and clearly defines staff responsibilities.
Technology integration
Computerized physician order entry offers numerous benefits beyond just reducing TAT; it also enhances the efficiency of patient care across the organization. In addition, it guarantees 100% compliance that the requested data are completed.²⁹
CDSS provide real-time alerts and guidance when entering orders, reducing clarifications and pharmacist interventions, which enhances workflow thereby lowers TAT.⁴⁸
ADCs decentralize dispensing and storage of medications, improving inventory and reducing costs as well as TAT for inpatient delivery of medication. A study has shown that ADCs decrease nurses’ wait times and improve immediate access to medications. Additionally, ADCs are associated with fewer medication delay incidents and increased staff satisfaction.¹⁴
Barcode Medication Administration (BCMA) supports four of the five rights of medication
administration—right patient, drug, route, and time—while the accuracy of the right dose can be further enhanced through the use of CDSS. BCMA may help reduce medication administration error and help to reduce TAT as result of eliminating the need for corrective action.²⁰
Carousel Dispensing Technology (CDT) has maximized efficiency and effectiveness throughout pharmacy dispensing processes. Through the use of CDT improved workflow occurred for ADC refills, first-dose dispensing, supplemental cart fills, as well as inpatient medication procurement.⁴⁹
After the deployment of CDT, mean TAT for STAT medication requests was improved, as well as accuracy for all medication requests.⁴⁹
Finally, the greatest improvement to medication safety observed was the minimization of workflow interruptions—a basically recognized factor to medication errors. The system also led to improved patient safety via enhanced proactive decision making, lower backlog processing.⁵⁰
The use of pneumatic tube systems in hospitals can greatly enhance the TAT⁵¹. However, there are several considerations and limitations to which the attention is needed to be paid that not all medications—cytotoxic, heat or fragile medications—can be transported by pneumatic tube systems.⁵²
Technology integration helps speed up TAT by improving efficiencies, increasing accuracy, and enhancing communications in MUPs. With tools such as CPOE, BCMA, automation, and analytics, institutions can provide pharmacy services that are ultimately faster, safer, and more reliable.
Improve communication across teams
Effective communication in healthcare is a critical component of patient safety, clinical efficiency, and interdisciplinary collaboration. Poor communication among healthcare professionals can lead to medical errors, compromised patient outcomes, and increased healthcare costs.²²
A research project conducted at a tertiary hospital examined the perception and satisfaction of physicians, nurses and pharmacists toward the Patient Care Area Pharmacist role. The results showed that having pharmacists work in these areas can foster interprofessional communication, reduce the workload of other health professionals, improve clinical and medication distribution delivery, and ultimately result in reducing TAT and cost savings.⁵³
Real-Time Dashboards and Analytics: The introduction of an integrated information system resulted in reducing telephone communications due to the ability to track prescriptions in real-time and prioritization based on urgency. The potential of the real-time dashboards truly improved the tracking of prescriptions through both pharmacy and nursing units, as the overall TAT was improved.⁵⁰
Moreover, the presence of satellite pharmacies enhances interdisciplinary collaboration among healthcare professionals, reinforcing the foundation of high quality, integrated patient care.⁵⁴
Proximity of pharmacy units
Satellite pharmacies are smaller, decentralized pharmacy units strategically located near patient care areas. First introduced in 1969, they were proposed as essential components of healthcare systems aimed at enhancing service delivery. By situating pharmacy services within specific hospital wards, satellite pharmacies can provide specialized, patient-centered support tailored to the unique needs of each area thus improving outcomes.
Satellite pharmacies contribute significantly to patient safety and operational efficiency by reducing medication errors, streamlining drug delivery processes. As a result, they help improve both patient outcomes and the performance of interdisciplinary care teams.
Beyond logistics and safety, satellite pharmacies also play a pivotal role in direct patient care
through services such as medication reconciliation and pharmacotherapy counseling.
However, despite their advantages, satellite pharmacies face several challenges. These include ensuring sufficient staffing levels, maintaining seamless coordination with the central pharmacy, and implementing efficient health information systems to monitor and manage medication-related transactions. In the absence of such infrastructure, there is a risk of service duplication and communication breakdowns, which can undermine the overall effectiveness of the satellite model.⁵⁴
Medication inventory management
Effective medication inventory management plays a pivotal role in optimizing TAT by ensuring drug availability as result, enhances the overall efficiency of pharmacy operations ultimately leading to shorter TAT.²¹ Poor inventory control leads to stockouts and negatively affecting patient care.
Effective inventory systems offer timely processing of medication when it is needed, thus eliminating the impact of the unavailability of medicines or misplaced items, so ultimately speeding up the dispense time, and assuring that TAT is optimized.
Automated inventory systems can limit human error, and improve medication retrieval times.⁵⁵
Here are some practical ways to improve the inventory systems:
-
Utilize intelligent inventory tools (e.g., Radio Frequency Identification (RFID); Artificial Intelligence (AI) driven demand forecasting)
-
Standardize inventory on stock amounts by using different methods of inventory assessments such as an Always Better Control (ABC) or Vital Essential Non-essential (VEN).
-
Better collaborations with suppliers to reduce lead times in procuring process.
-
Educate staff on best practice inventory management to reduce stock out or over stock.
-
Utilize both medication distribution system, centralized and decentralized system.
Feedback system
An effective feedback system is essential for any organization to adapt to evolving needs over time and to drive continuous improvement in hospital quality.⁵⁶ This is particularly critical for roles with substantial public interaction, as it provides a clear understanding of public sentiment.
A feedback system operates by collecting inputs, implementing necessary changes, and evaluating the impact through subsequent feedback. Direct patient feedback serves as a fundamental measure for assessing patient experience. An effective feedback system should function as a dynamic, interactive platform that actively connects all stakeholders and sustains their engagement through a seamless cycle of information exchange.²³
Hospitals are utilizing a variety of feedback collection methods—such as experience trackers, mobile devices, online platforms, telephone systems, and touchscreen kiosks—to gather real-time patient data and insights.²⁴ A combination of qualitative and quantitative approaches is necessary to strengthen the validity of the findings.⁵⁷
Conclusion
Medication turnaround time is an important measure that affects patient safety, quality of care, and efficient operations. The healthcare system can improve medication delivery and patient outcomes by addressing the factors that affect TAT, including workflow environments, interprofessional communication, technology integration issues (e.g., CPOE, ADCs, BCMA, robotics), employee training, inventory management and prioritization systems for prescribing.
Evidence from 56 studies suggests that to improve TAT, a multiple-approach strategy should be adopted: a distinctive combination of new technology and Lean-Six Sigma, standardizing protocols, and real-time data analytics. Critical success factors include end-user centered design, inter-professional collaboration, and feedback.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Acknowledgements:
No acknowledgements.
References
1. Agency for Healthcare Research and Quality. Medication turnaround time in the inpatient setting (AHRQ Publication No. 2009:09-0045). Agency for Healthcare Research and Quality. digital.ahrq.gov/sites/default/files/docs/page/medication-turnaround-time-quick-reference-guide.pdf
2. Bloch DM. Computer-generated management tools for the clinical pathology laboratory: I. Throughput Report. J Med Syst. 1980;4(3-4):367-380. doi:10.1007/BF02222846
3. Mekhjian HS, Kumar RR, Kuehn L, et al. Immediate benefits realized following implementation of physician order entry at an academic medical center. J Am Med Inform Assoc. 2002;9(5):529-539. doi:10.1197/jamia.m1038
4. Tell R, Hoffman I. The elimination of turnaround time in routine ECG processing. J Electrocardiol. 1971;4(3):279-281. doi:10.1016/s0022-0736(71)80042-0
5. Hawkins RC. Laboratory turnaround time. Clin Biochem Rev. 2007;28(4):179-194
6. Braddock CH 3rd, Snyder L. The doctor will see you shortly. The ethical significance of time for the patient-physician relationship. J Gen Intern Med. 2005;20(11):1057-1062. doi:10.1111/j.1525-1497.2005.00217.x
7. Hurlen P, Østbye T, Borthne A, Gulbrandsen P. Introducing PACS to the late majority. A longitudinal study. J Digit Imaging. 2010;23(1):87-94. doi:10.1007/s10278-008-9160-x
8. Samaan ZM, Klein MD, Mansour ME, DeWitt TG. The impact of the electronic health record on an academic pediatric primary care center. J Ambul Care Manage. 2009;32(3):180-187. doi:10.1097/JAC.0b013e3181ac9667
9. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287
10. Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304-377. doi:10.1007/s00134-017-4683-6.
11. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589-1596. doi:10.1097/01.CCM.0000217961.75225.E9
12. Institute for Safe Medication Practices (ISMP) and National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP), taxonomy of medication errors. NCC MERP 2001
13. Alharthi A, Alshagrawi S. The Impact of Standardization of Intravenous Medication on Patient Safety and Quality of Healthcare: A Systematic Review . Open Public Health J, 2024; 17: e18749445335795
14. Almalki A, Jambi A, Elbehiry B, Albuti H. Improving Inpatient Medication Dispensing with an Automated System. Glob J Qual Saf Healthc. 2023;6(4):117-125. Published 2023 Nov 24. doi:10.36401/JQSH-23-15
15. Beobide Telleria I, Ferro Uriguen A, Miró Isasi B, Martínez Arrechea S, Genua Goena MI. The impact of automation on the safety of drug dispensing in nursing homes. Impacto de la automatización en la seguridad de la dispensación de medicamentos a centros sociosanitarios. Farm Hosp. 2018;42(4):141-146. Published 2018 Jul 1. doi:10.7399/fh.10949
16. Borrelli EP, Telinoiu M, Nelkin H, Dumitru D, Lucaci JD. Appraising the clinical, operational, and economic impacts of automated medication dispensing cabinets in perioperative and surgical settings: A systematic literature review. J Am Pharm Assoc (2003). 2024;64(5):102143. doi:10.1016/j.japh.2024.102143
17. Capilli M, Enrico F, Federici M, Comandone T. Increasing pharmacy productivity and reducing medication turnaround times in an Italian comprehensive cancer center by implementing robotic chemotherapy drugs compounding. J Oncol Pharm Pract. 2022;28(2):353-361. doi:10.1177/1078155221992851
18. Bagattini ÂM, Borges JLA, Riera R, de Carvalho DCMF. Automation of a tertiary hospital pharmacy drug dispensing system in a lower-middle-income country: A case study and preliminary results. Explor Res Clin Soc Pharm. 2022;6:100151. Published 2022 Jun 9. doi:10.1016/j.rcsop.2022.100151.
19. Hwang J, Koo GK, De Palm SE, et al. Inpatient Pain Medication Administration: Understanding the Process and Its Delays. J Surg Res. 2018;232:49-55. doi:10.1016/j.jss.2018.05.080
20. Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med. 2010;362(18):1698-1707. doi:10.1056/NEJMsa0907115
21. Billstein-Leber M, Carrillo CJD, Cassano AT, Moline K, Robertson JJ. ASHP Guidelines on Preventing Medication Errors in Hospitals. Am J Health Syst Pharm. 2018;75(19):1493-1517. doi:10.2146/ajhp170811
22. World Health Organization (WHO). Communication During Patient Handovers 2013
23. Coulter A, Fitzpatrick R, & Cornwell J. Measures of patients’ experience in hospital: purpose, methods and uses. London: King’;s Fund: 2009:7-9
24. Brown H, Davidson D, Ellins J. Real-time patient feedback. Birmingham: University of Birmingham, Health Services Management Center: 2009.
25. Yulia R, Hartono R, Indrayanti M, Ayumuyas NP, Herawati F. Studying waiting time in pharmacy: A strategy for improving patient satisfaction. MethodsX. 2025;14:103282. Published 2025 Mar 25. doi:10.1016/j.mex.2025.103282
26. Liew JES, Chong Cheng Y, Tai NL, et al. A before-after study to evaluate the effect of pharmacy workflow redesign to improve pharmacy waiting time and reduce medication near misses in Malaysia. Int J Pharm Pract. 2024;32(1):83-90. doi:10.1093/ijpp/riad083
27. Cello, R., Conley, M., Cooley, T., De la Torre, C., Dorn, M., Ferer, D. S., … & Volpe, G. (2022). ASHP guidelines on the safe use of automated dispensing cabinets. American Journal of Health-System Pharmacy, 79(1), e71-e82.
28. Naylor H, Woloschuk DM, Fitch P, Miller S. Retrospective audit of medication order turnaround time after implementation of standardized definitions. Can J Hosp Pharm. 2011;64(5):346-353. doi:10.4212/cjhp.v64i5.1070
29. Jensen J. The effects of Computerized Provider Order Entry on medication turn-around time: a time-to-first dose study at the Providence Portland Medical Center. AMIA Annu Symp Proc. 2006;2006:384-388
30. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: Monitoring and patient education. Am J Health Syst Pharm. 2021;78(7):524–545.
31. Khajouei R, Peek N, Wierenga PC, Kersten MJ, Jaspers MW. Effect of predefined order sets and usability problems on efficiency of computerized medication ordering. Int J Med Inform. 2010;79(10):690-698. doi:10.1016/j.ijmedinf.2010.08.001
32. Niazkhani Z, Pirnejad H, van der Sijs H, Aarts J. Evaluating the medication process in the context of CPOE use: the significance of working around the system. Int J Med Inform. 2011;80(7):490-506. doi:10.1016/j.ijmedinf.2011.03.009
33. Chapman AK, Lehmann CU, Donohue PK, Aucott SW. Implementation of computerized provider order entry in a neonatal intensive care unit: Impact on admission workflow. Int J Med Inform. 2012;81(5):291-295. doi:10.1016/j.ijmedinf.2011.12.006
34. Moss J, Berner ES. Evaluating clinical decision support tools for medication administration safety in a simulated environment. Int J Med Inform. 2015;84(5):308-318. doi:10.1016/j.ijmedinf.2015.01.018
35. Lorimer HJ, Lalli SL, Spina SP. Redesign of the pharmacy practice model at a tertiary care teaching hospital. Can J Hosp Pharm. 2013;66(1):28-34. doi:10.4212/cjhp.v66i1.1209
36. Raghuvanshi, VP, Choudhary H. Medication Turnaround Time In Hospital Pharmacy Department. International Journal of Research and Development in Pharmacy and Life Sciences, 2013:2(5), 626-630
37. Kirschling TE, Rough SS, Ludwig BC. Determining the feasibility of robotic courier medication delivery in a hospital setting. Am J Health Syst Pharm. 2009;66(19):1754-1762. doi:10.2146/ajhp080184
38. Fernandes CM, Worster A, Eva K, Hill S, McCallum C. Pneumatic tube delivery system for blood samples reduces turnaround times without affecting sample quality. J Emerg Nurs. 2006;32(2):139-143. doi:10.1016/j.jen.2005.11.013
39. Cordero L, Kuehn L, Kumar RR, Mekhjian HS. Impact of computerized physician order entry on clinical practice in a newborn intensive care unit. J Perinatol. 2004;24(2):88-93. doi:10.1038/sj.jp.7211000
40. Cunningham TR, Geller ES, Clarke SW. Impact of electronic prescribing in a hospital setting: a process-focused evaluation. Int J Med Inform. 2008;77(8):546-554. doi:10.1016/j.ijmedinf.2007.10.008
41. Gabriel MH, Kotschevar CM, Tarver D, Mastrangelo V, Pezzullo L, Campbell PJ. Specialty pharmacy turnaround time impediments, facilitators, and good practices. J Manag Care Spec Pharm. 2022;28(11):1244-1251. doi:10.18553/jmcp.2022.28.11.1244
42. Barlow B, Barlow A, Hammond DA. Identifying the different types of professional relationships: Are you my mentor? [published correction appears in Am J Health Syst Pharm. 2022 Feb 18;79(5):402. doi: 10.1093/ajhp/zxaa368.]. Am J Health Syst Pharm. 2020;77(18):1463-1465. doi:10.1093/ajhp/zxaa134
43. Alosaimi M, Almeziny M. The Appropriateness of STAT Prescriptions in Emergency Department in a Tertiary Hospital in Saudi Arabia. Saudi Commission for Health Specialties (SCFHS) hosted a Pharmacy Resident Research Day, 2022.
44. Tsao NW, Lo C, Babich M, Bansback N. Applying Lean methodologies to improve workflow in hospital pharmacies: A systematic review. Eur J Hosp Pharm. 2022;29(1):3–10.
45. Sallam M. Enhancing Hospital Pharmacy Operations Through Lean and Six Sigma Strategies: A Systematic Review. Cureus. 2024;16(3):e57176. Published 2024 Mar 29. doi:10.7759/cureus.57176
46. Almeziny M., Tawakol H, et al,” Standardization as a strategy to reduce medication errors” ,2018 Midyear. Clinical Meeting and Exhibition, Anaheim, CA, United State of America.
47. Trbovich, P. (2014). Five ways to incorporate systems thinking into healthcare organizations. Biomedical instrumentation & technology, 48(s2), 31-36.
48. Berner ES. Clinical decision support systems: state of the art. AHRQ publication, 2009:90069, 1-26
49. Temple J, Ludwig B. Implementation and evaluation of carousel dispensing technology in a university medical center pharmacy. Am J Health Syst Pharm. 2010;67(10):821-829. doi:10.2146/ajhp090307
50. Binobaid S, Almeziny M, Fan IS. Using an integrated information system to reduce interruptions and the number of non-relevant contacts in the inpatient pharmacy at tertiary hospital. Saudi Pharm J. 2017;25(5):760-769. doi:10.1016/j.jsps.2016.11.005
51. Kok JHJ, Lam CWL, Lee MYJ. Reducing delivery times of emergency blood products through pneumatic tube systems. Asian J Transfus Sci. 2019;13(1):3-9. doi:10.4103/ajts.AJTS_52_18
52. Wang P, Nguyen L. Update to delivering medications via a pneumatic tube system. Am J Health Syst Pharm. 2017;74(19):1521-1522. doi:10.2146/ajhp150107
53. Almeziny, M., Khurshid, F. M., Alaneazi, N. L., Alotaibi, S. S., Alharbi, S. N., Almitwazi, A. A., … & Alsultan, M. S. (2020). Perception and satisfaction of stakeholders regarding the patient care area pharmacist initiative in a military hospital in Saudi Arabia. Tropical Journal of Pharmaceutical Research, 19(2), 401-409.
54. Sharifan A. The Strategic Roles of Satellite Pharmacies in Hospital Settings. Hosp Pharm. Published online September 13, 2024. doi:10.1177/00185787241279416
55. American Journal of Health-System Pharmacy. Impact of Automated Dispensing Cabinets on Medication Turnaround Time 2021
56. Murante AM, Vainieri M, Rojas D, Nuti S. Does feedback influence patient – professional communication? Empirical evidence from Italy. Health Policy. 2014;116(2-3):273-280. doi:10.1016/j.healthpol.2014.02.001
57. Gowda NR, Wankar A, Arya S., Vikas H, Narayanan NK, Linto CP. Feedback system in healthcare: the why, what and how. Int J Mark Stud. 2020:12(1), 1-52