






Patient-Based Medicine: Redefining Patient Care Focus
Patient-Based Medicine – A Novel Framework to Restore Focus on the Patient
Richard Evan Steele1, Johannes G. Schmidt2
- Owner and doctor, Klinikken Livet,
https://www.klinikken-livet.dk and
https://www.realnetdoc.com - Chairman, PBM Foundation.
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: Steele, R., E., Schmidt, J., G., Patient-Based Medicine – A Novel Framework to Restore Focus on the Patient. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6790
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6790
ISSN 2375-1924
ABSTRACT
Patient-Based Medicine (PBM) proposes a bold reformation of modern medicine – one that places the patient, not the disease, as the primary object of care. Rooted in the traditions of epidemiology, ancient Chinese medicine, and pragmatic clinical reasoning, PBM advocates a shift away from pathology markers and disease-based protocols toward outcomes that truly matter to patients: quality of life or back to work, resiliency, and total morbidity and mortality.
Keywords: Patient-Based Medicine, patient-centered care, resiliency, morbidity, mortality, clinical outcomes, epidemiology, ancient Chinese medicine.
Introduction
Traditional modern western medicine can be likened to an express train barreling down the tracks to a destination that no one has defined, and no one has any idea of the who what when where how and why of this behemoth. There are those among us that propound a paradigm shift that will place the patient at the center of our deliberations rather than the current focus on improving parameters that we have defined without regard to issues that are meaningful to the patient, which is improvements in quality of life and/or back to work as the dependent variable.
The reorientation of clinical research towards the questions of treatment benefit (beyond the question of treatment efficacy) and of whether clinical trials represent actual practice (external validity) is the timely path to clinical research questions of real interest and importance. Postmodern anything goes makes it possible to also consider hitherto dismissed effects, such as placebo, as valuable. However, that would require a precise documentation of the external validity of such effects. Not disease as such, but the disease context, not therapy as such, but the therapeutic context, not the patient as such, but the patient context, not a test as such, but the test situation has become an important focus of clinical research.
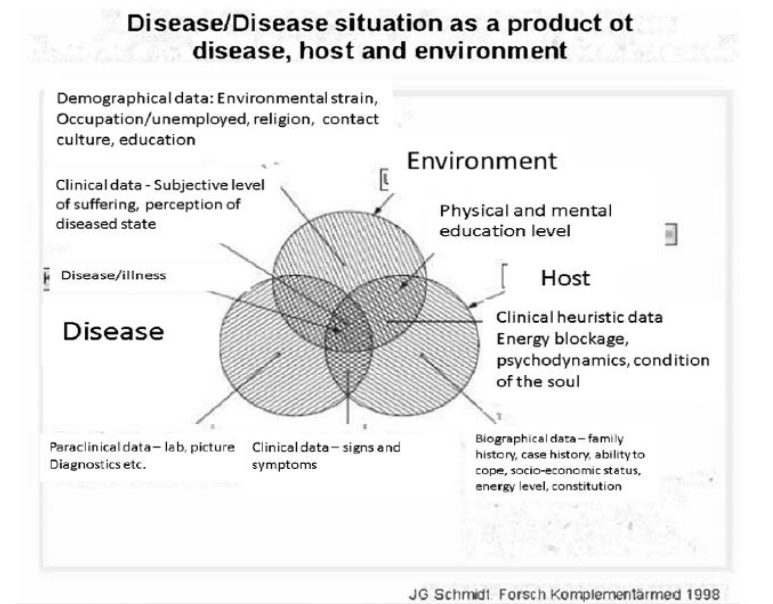
In respect to test results, current medicine can and should recognize its preoccupation with allegedly objective and hard data. The patient context can determine whether an efficacious therapy is beneficial or harmful. It is thus the proper definition of the patient context which makes medicine documentable, no matter how objective or subjective the effect of therapy is. The consideration of the therapeutic context leads to the important distinction between efficacy and effectiveness (or benefit), and this makes it clear that the randomized controlled trial in its traditional design as the placebo controlled double-blind trial (DBRCT) is limited to the evaluation of drug theory. The evaluation of treatment effectiveness requires more pragmatic trials which study treatment operations and not isolated components and which may also compare entire treatment strategies. Pragmatic clinical trials, in future, will not only allow the study of pathogenesis blockers, but also the study of salutogenic interventions working with the host constitution. The following illustration gives a good picture of this way of thinking and its importance for individuals receiving treatment. It is clear we have paid too little attention to the importance of environment and host resiliency in our modern paradigms that have been more or less ubiquitous in our research. The illustration below provides a graphic of this way of thinking, and the importance of taking the patient and the environment into account in the patient encounter. The illustration provides a backdrop for the development of a holistic approach to the patient which is key to the development of patient-based medicine. This would be a significant departure from current practice that has received scathing criticism from JS Norell.
Historical Roots
Epidemiological training in Australia inspired Dr. Schmidt’s skepticism about breast cancer screening. His published analysis, later adopted by the Cochrane Collaboration and the Swiss Medical Board, argued that screenings often do more harm than good. This set the foundation for PBM’s emphasis on total patient outcomes over abstract risk reductions. PBM also draws from ancient Chinese medicine, particularly the idea of diagnosing and treating the “root deficiency” rather than superficial symptoms. Resilience is seen as a physiological, measurable state—a position supported by anecdotal successes in late-stage cancer recovery and reappraisal of metastases as potentially adaptive phenomena. This has led to a holistic approach that is illustrated in the graphic below:
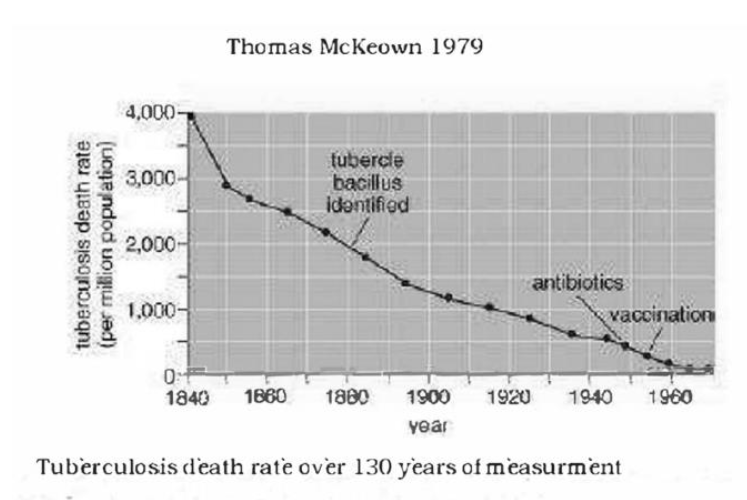
To the astute observer, our dependence on medicine and its effect on disease categories has been exaggerated extremely. Another graphic that demonstrates this clearly is pictured below. As the graph clearly shows, the advent of antibiotics and vaccinations has not altered the course of survival from tuberculosis, which has clearly been the result of improved resiliency among populations.
Illustrious leaders of medicine including Petr Skrabanek, James McCormick, Alvin Feinstein, Stephen Leeder to name just a few have admonished our systems for being insensitive, overly zealous and built upon many fallacies and follies. The worst side of this is what is called the surrogate fallacy, in which a perceived benefit if viewed from a holistic epidemiological point turns out to be the opposite. Two large scale and well acknowledged studies have shown this clearly. The first is the so-called CAST (coronary arrhythmia suppression trial) study, in which the given therapy suppressed the arrhythmias successfully, but the overall mortality increased significantly. In other words, the application of anti-arrhythmic therapy kills more patients than it saves. The surrogate here is reduction of arrhythmia which is viewed as beneficial. The fallacy is that the therapy kills more patients than it saves. The second is the RECORD (Rosiglitazone Evaluated for Cardiovascular Outcomes in Oral Agent Combination Therapy for Type 2 Diabetes) in which the target was reduction of HBa1C, which was clearly accomplished. But also here, the therapy increased overall mortality significantly among the study group from cardiovascular deaths and deaths due to trauma. The surrogate here is that the reduction of Hba1C was beneficial, but the fallacy is that the therapy kills more patients than it saves.
Evidence-based medicine often errs to the side of a surrogate and not paying attention to the fallacy. The lesson to be learned here is that epidemiological research needs to be brought forth. The thinking behind this is to reduce the number of surrogate fallacies. The thinking is akin to the phenomenon of environmental accounting, in which the sum total of everything involved in the consummation of the activity taken into account. An example is the automobile. It is common to view the cost of driving a car that it is the cost of fuel only. But environmental accounting takes into account the insurance, vehicle upkeep, cost of accidents, building of roads and bridges, cost of downtime while driving, cost of legislative bodies regulating the area, the production of rubber and making of tires, production and application of lubrication, development and utilization of sensors, electronics (including radios), production and installation of tempered glass, mining and production of metals, the production of smog and acid rain and their environmental ramifications, and maybe some elements that I have not thought of. The point is that without the clear picture of the true cost, we are in danger of entering the surrogate fallacy.
It is imperative to adopt this way of thinking in clinical medicine. If we are to get better at helping patients improve their quality of life and/or getting him or her back to work after work disability, we must adopt a new paradigm which will allow us to think more holistically and see beyond our focus on laboratory and picture diagnostic results, and get back to our roots of promoting quality of life improvements and/or back to work criteria that will allow us to embrace whatever improves these things without prejudice or a “holier than thou” attitude. Many examples of how the prejudice and “holier than thou” attitudes are deleterious to a large proportion of our patient mass which our traditional systems are mostly powerless against exist. Typical examples of syndromes that are left out and told “learn to live with it” are whiplash syndrome, post-concussion syndrome, tension headache, lower back pain and pain stemming from untoward psychic phenomena (functional pain). These conditions are common, comprising on the order of 20% of the population. The author has likened it to an express train hurtling down the tracks to a destination no one knows where is. Meanwhile, the 20-30% still standing on the platform wonders at the departing train. The new paradigm we call Patient-based medicine includes the elements that are needed to address this. In our book, Patient-based medicine – treat the patient not his disease, Cambridge scholars 2023, the problem complex is clearly spelled out, and the way forward is laid out.
Key Innovations of PBM
PBM introduces five foundational innovations:
- Host-Centered Illness Understanding: PBM restores a classical epidemiological balance between disease and host, urging clinicians to prioritize treating the host—i.e., the patient—as the central determinant of health outcomes.
- Avoidance of Surrogate Fallacies: PBM warns against the use of laboratory and imaging markers as proxies for health, where early diagnosis often results in overtreatment without meaningful benefit. The emphasis should be on real-life metrics such as mortality and functional status, not disease-specific scores.
- Learning from COVID-19 Policy Failures: PBM critiques the medical community’s support of COVID-19 lockdowns, documenting that they caused excess mortality, especially from cardiovascular causes. Sweden, which avoided such measures, did not suffer the same mortality spike, according to WHO data.
- Therapeutic Resilience Building: The PBM model incorporates strategies to strengthen host resilience—an ancient practice revitalized through both traditional medicine and modern trials. The example of 19th-century tuberculosis recovery in Swiss sanatoria illustrates how resilience – not necessarily medical intervention – can reverse disease trajectories.
- Integration of Complementary Medicine: PBM offers a rational framework for integrating complementary therapies by focusing on patient benefit rather than conformity to molecular science. It calls for pragmatic clinical trials to evaluate such interventions.
A Call for Reform
PBM calls for a reassessment of Evidence-Based Medicine (EBM), which it sees as over-committed to pathophysiological reasoning and often blind to real life outcomes. Historical trials like CAST and RECORD are cited as cautionary tales, where control of biomarkers led to increased mortality. PBM urges a new synthesis, where empirical outcomes constitute therapeutic success.
Vision for Implementation
The PBM Foundation plans to institutionalize this paradigm through international symposia in Davos, Switzerland, starting in 2026. These events will explore topics such as resiliency measurement, integration of prayer and placebo research, the role of traditional diets, rehabilitative strategies and complementary treatments. PBM seeks to reduce the dominance of the medico-industrial complex and revive a clinical paradigm that serves patients. Patient-Based Medicine does not oppose scientific rigor – it demands a redirection of that rigor toward the patient, not his disease.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
No financial disclosure.
Acknowledgements:
No acknowledgements.
References:
- Schmidt JG, Steele RE. Patient based medicine – treat the patient, not his disease. Cambridge Scholars 2023, 107 pp
- Steele RE, de Leeuw E, Carpenter DO. A novel and effective treatment modality for medically unexplained symptoms. J Pain Management. 2009;1(4):401–12
- Weinstein MC. Clinimetrics. New Haven: Yale University Press; 1987
- Schmidt, J. G. (1990). The epidemiology of mass breast cancer screening—a plea for a valid measure of benefit. Journal of Clinical Epidemiology, 43(3), 215–225. doi: 10.1016/0895-4356(90)90002-7
- Steele RE, Low level laser therapy and myofascial pain. J Pain Management 2020, 13(1): 57-62
- Skrabanek P, McCormick J. Follies and Fallacies in Medicine. London (or Dublin): Tarragon Press; 1989
- Echt, D. S., Liebson, P. R., Mitchell, L. B., Peters, R. W., Obias-Manno, D., Barker, A. H., … & CAST Investigators. (1991). Mortality and Morbidity in Patients Receiving Encainide, Flecainide, or Placebo. New England Journal of Medicine, 48(7), 223–33. doi:10.1056/NEJM199108103250629
- Home, P. D., Pocock, S. J., Beck-Nielsen, H., Curtis, P. S., Gomis, R., Hanefeld, M., … RECORD Study Group. (2009). Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. Lancet, 373(9681), 2125–2135. doi:10.1016/S0140-6736(09)60953-3
- Norell JS, editor. Six Minutes for the Patient: Interactions in General Practice Consultation. London: Tavistock Press (reissued by Routledge); 1973.