





PCOS in Adolescents: Hormonal Profiles & Treatment Insights
Revisiting Hormonal profile in PCOS in Adolescents and Young Women
Ananya Bera, Bishista Bagchi, Siddhartha Chatterjee
Abstract
Background: Polycystic ovarian Syndrome (PCOS) is a prevalent endocrine condition affecting women of reproductive age. The fundamental reason for the daily rise in the incidence of PCOS in adolescence is inappropriate lifestyle choices. Diagnosing PCOS in adolescent (aged 13-19 years, post 2 years of menarche) and young women (aged 20-25 years) might be difficult due to the rapid physiological and anatomical changes accompanying puberty. It’s critical to be aware of the physiological quirks of puberty, which frequently resemble PCOS symptoms. There is a clustering of cardiovascular risk factors in women with PCOS, including hypertension, dyslipidaemia, obesity, and impaired glucose tolerance (IGT). The objective of the present study was to identify the most prevalent hormone in patients with single or multiple hormone disorders related to PCOS in adolescent and young women; after diagnosing them using the Rotterdam criteria. This may help to evaluate the associated risks and to plan the treatment protocol.
Methods: In the last few years from October 2022 to October 2024, a total of 6,006 gynecological patients attended Calcutta Fertility Mission, 21 Bondel Road, Kolkata, West Bengal, India. Of these, 2,492 were adolescent and young women; 250 of them were diagnosed with PCOS using Rotterdam Criteria. Standardized methods were used to collect anthropometric measures, including weight and height. Serum insulin, Testosterone, Dehydroepiandrosterone (DHEA), Thyroid Stimulating Hormone (TSH), Prolactin (PRL) and Homocysteine (HCY) were measured. Participants with menstrual disorders or any biochemical abnormalities were invited for ultrasonography (USG) examination. The ovarian volume and follicular size were evaluated transabdominally. Follicle stimulating Hormone (FSH), Leutinising Hormone (LH) and Anti Mullerian Hormone (AMH) were not estimated as their dysfunction is well understood. The hormones investigated influences the planning of treatment.
Results: Hyperhomocysteinemia was detected in 52.8% of cases of 250 PCOS patients whereas hyperadrenalism (4.8% in 250 PCOS patients) and hyperprolactinemia with hypothyroidism (4.8% in 250 PCOS patients) were detected in less number of patients.
Conclusion: Complications can be avoided with early detection of adolescent PCO. Early diagnosis and treatment facilitate the easy and successful stabilization of the condition for a longer duration.
Keywords
Adolescent, Polycystic Ovarian Syndrome (PCOS), Diagnosis, Prevalence, Body Mass Index (BMI)
Introduction
Polycystic ovarian Syndrome (PCOS) is becoming more common in adolescence, with improper lifestyle being the leading cause. The World Health Organisation (WHO) defines adolescence as the stage of life between 10 and 19 years old that is marked by major and crucial changes in puberty, growth, and development. There are four axes to the pubertal endocrine alterations linked to adolescents PCOS- a) Gonadotropic axis, b) Adrenocorticotropic axis, c) Somatotropic axis and d) Intrinsic axis. Polycystic ovarian syndrome (PCOS), which has been found to afflict 6–18% of adolescent girls, may have an impact on the hypothalamo-pituitary-ovarian (HPO) axis. It is a functional endocrine issue, hence the appearance of the ovary is not of concern. In reality, parents are more concerned about their adolescent daughters’ appearance, weight gain, somewhat masculine features like excessive hair growth and irregular menstruation. In addition, opinions made by acquaintances and neighbours as well as incorrect medical advice given by few professionals exacerbate the situation. The prevalence of PCOS in adolescents has now reached a peak. About 30% of women show polycystic changes in the ovaries, of these, 10-15% may progress to develop polycystic ovary syndrome (PCOS), mainly due to three factors such as stress, obesity, and unhealthy lifestyle. This conversion of PCOS to PCO is influenced by controlling these factors, and if we can reverse 10% of them. In adolescents, hyperandrogenism and menstruation disruption are the most common manifestations of PCOS. It is associated with abnormalities in ovulatory function, relative gonadotropin ratio, insulin secretion and function, androgen synthesis and function, genetic factors as well as the balance of pro- and antioxidant systems. It is thought that homocysteine hinders implantation of embryo by disrupting the vascular integrity and blood flow of the endometrium, which may lead to an early miscarriage as well. Developing precise diagnostic criteria for adolescent PCOS has been difficult due to its prevalence and hence diagnosis in this group is challenging due to the rapid physiological and anatomical changes that occur throughout puberty. The lack of strong evidence exacerbates over-diagnosis, General practitioners and allied health professionals use inconsistent, non-evidence-based methods for PCOS diagnosis and management. In adolescents, the number of years since menarche, which is vital to understand the progression of typical physiological changes associated with puberty, which can stay up to 2 years following menarche, after which they subside. There is a need for high-quality, evidence-based guidelines because pertinent consensus statements are frequently not tailored to adolescents and/or are not supported by strong, high-level evidence and/or rigorous procedures. This paper specifically focuses the prevalence of PCOS in adolescents (aged 13–19 years with post 2 years of menarche) and young women (aged 20–25 years) using the Rotterdam criteria, as well as the risk factors that are linked to the condition. The hormonal profile examination may be helpful to chalk out treatment planning and particularly to plan treatment in preventing immediate and remote complications.
Materials and Methods
SUBJECTS
In the last few years from October 2022 to October 2024, a total of 6006 gynecological patients attended the Calcutta Fertility Mission, 21 Bondel Road, Kolkata, West Bengal, India. Of these, 2492 were adolescent (13-19 years; post 2 years of menarche) and young patients (13-25 years); 250 of them were diagnosed with PCOS using Rotterdam Criteria. Among those 250 patients, 112 were adolescents and 138 were young women.
INCLUSION CRITERIA
All voluntarily consenting participants who are adolescents past 2 years of menarche and young adults. Informed consent was obtained from the patient as well as their guardians.
EXCLUSION CRITERIA
Lack of consent to undergo longitudinal monitoring, presence of any chronic infection, type I diabetes, addiction to tobacco and alcohol were excluded from the study. Participants undergoing treatment for other clinically diagnosed conditions or using any prescribed medications for PCOS within the past 12 months will be excluded for participation in the study.
ANTHROPOMETRY AND BIOCHEMICAL PARAMETERS
Standardized methods were used to collect anthropometric measures, including weight and height. The formula for calculating BMI is weight (kg) divided by height (m2). Participants were grouped as based on BMI range: Mild thinness BMI (17-18.5 kg/m2), Normal BMI (18.5-25 kg/m2), Overweight BMI (25-30 kg/m2), Obese Class I (BMI – 30-35 kg/m2), Obese Class II (BMI -35-40 kg/m2) and Obese Class III (BMI >40 kg/m2). Serum insulin, Testosterone, Dehydroepiandrosterone, Thyroid Stimulating Hormone, Prolactin and Homocysteine were measured using an autoanalyzer (Cobas Integra 400 plus, Roche). 5ml of venous blood was collected from each individual in the morning preferably in empty stomach from antecubital vein of left arm. Serum was separated in room temperature and stored at 4 degrees centigrade.
USG EXAMINATION OF THE ABDOMEN
For a USG examination, participants with any biochemical abnormalities or menstrual problems were recruited. A 3.5-5 MHz curvilinear probe (Siemens Healthineers Acuson Juniper) was used transabdominally to measure ovarian volume and follicular size. In our study, participants were categorized as having PCOS or not based on USG findings according to the Rotterdam criteria.
DIAGNOSIS OF PCOS
According to the 1990 National Institutes of Health (NIH) criteria, PCOS is indicated by the presence of oligo-ovulation symptoms and androgen excess (clinical or biochemical) with modification in 2003, the European Society of Human Reproduction and Embryology and American Society of Reproductive Medicine (ESHRE/ASRM) jointly suggested the diagnosis of PCOS as satisfying any two of the following: hyperandrogenism, oligo/anovulation, and PCOM, known as the Rotterdam criteria. The 2006 publication of the Androgen Excess and PCOS Society (AE–PCOS) Position Statement stated that hyperandrogenism must coexist with indications of ovarian dysfunction, such as ovulatory dysfunction and/or PCOM. With significant restrictions, the Rotterdam criteria were recommended for use in the 2018 International Evidence-Based Guideline for PCOS. Adolescents with hyperandrogenism and irregular menstrual periods do not need an ultrasound to be diagnosed. They should be monitored for irregular cycles for at least two years following menarche. After ruling out secondary causes, the requirements for adults need the presence of two of the following three characteristics: androgen excess, ovulatory dysfunction, or polycystic ovarian morphology (Table 1). Participants in our research were categorised as having PCOS or not based on USG findings according to the Rotterdam criteria.
STATISTICAL ANALYSIS
Categorical variables are expressed as Number of patients and percentage of patients and compared across the groups using Pearson’s Chi Square test for Independence of Attributes. The statistical software SPSS version 25 has been used for the analysis. An alpha level of 5% has been taken, i.e. if any p value is less than 0.05 it has been considered as significant.
ETHICAL CONSIDERATION
The Ethical Committee of Calcutta Fertility Mission has given clearance for the retrospective study. Every individual who took part in the study gave written informed consent.
Results
In the present study, 45.2% cases had family history of PCOS, 52.4% cases had family history of menstrual abnormality, 9.6% cases had family history of hypertension on both side (maternal & paternal), 24% cases had family history of hypertension on paternal side, 33.2% cases had family history of hypertension on maternal side, 9.6% cases had family history of diabetes on paternal side and 4.8% cases had family history of maternal side (Figure 1).
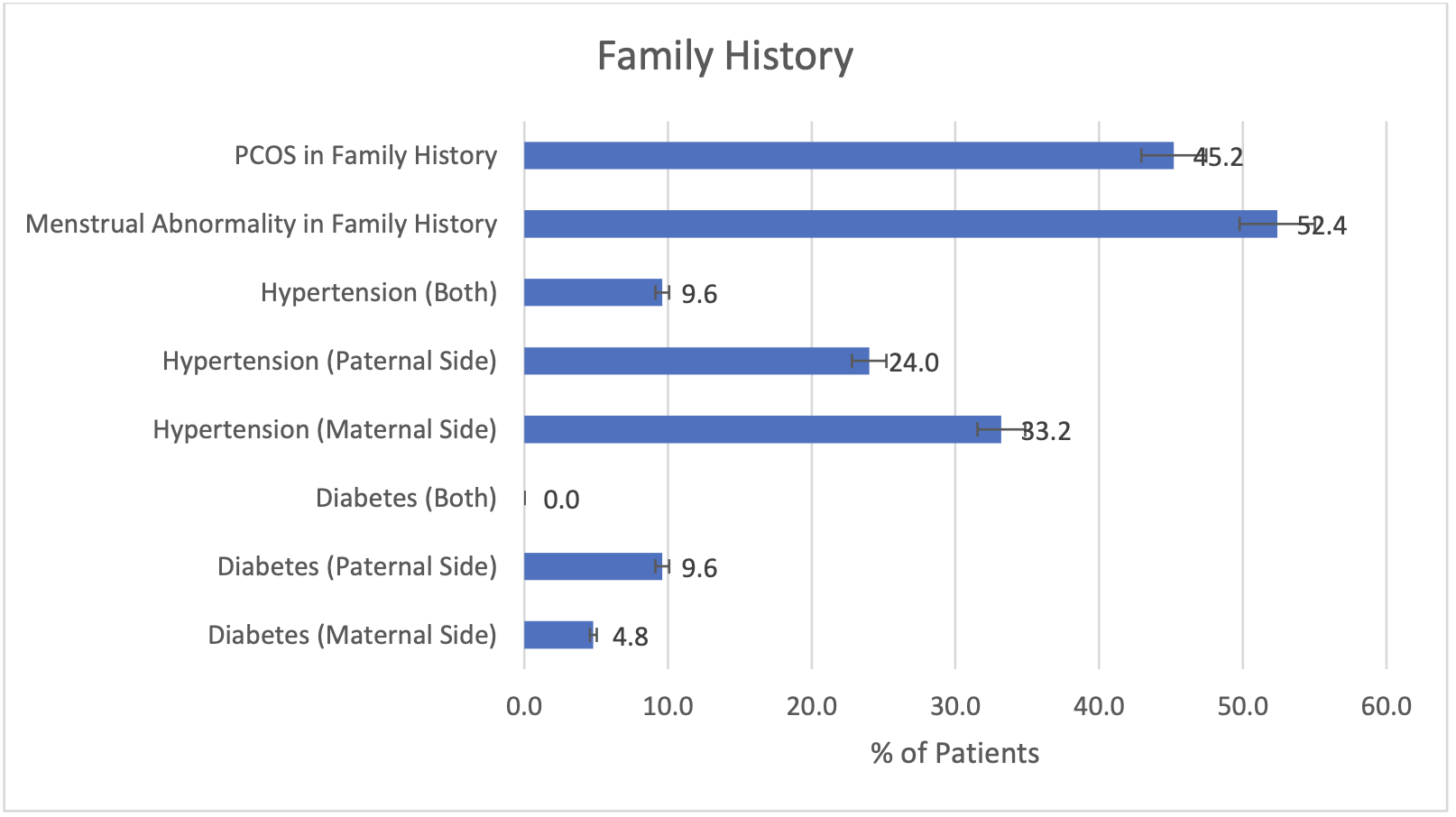
Figure 2 represents the greatest frequency of hyperhomocysteinemia, which was detected in 52.8% of 250 PCOS patients. We found the highest prevalence of hyperprolactinemia (44.64% in 112 patients) and hyperhomocysteinemia (44.64% in 112 patients) in adolescents (13-19 years, post 2 years menarche). Additionally, the highest prevalence of hyperhomocysteinemia (62.31% in 138 patients) was observed in young women (20-25 years).
Insulin resistance is exacerbated in PCOS-afflicted women who are often obese, with a noticeable central or abdominal obesity. These women have a higher chance of developing metabolic syndrome, cardiovascular disease, hypertension, dyslipidemia, impaired glucose tolerance (IGT), and type 2 diabetes later in life. Our study detected only a minimal number of cases, specifically 1 or 2 cases of detectable hyperinsulinemia, which can be considered negligible.
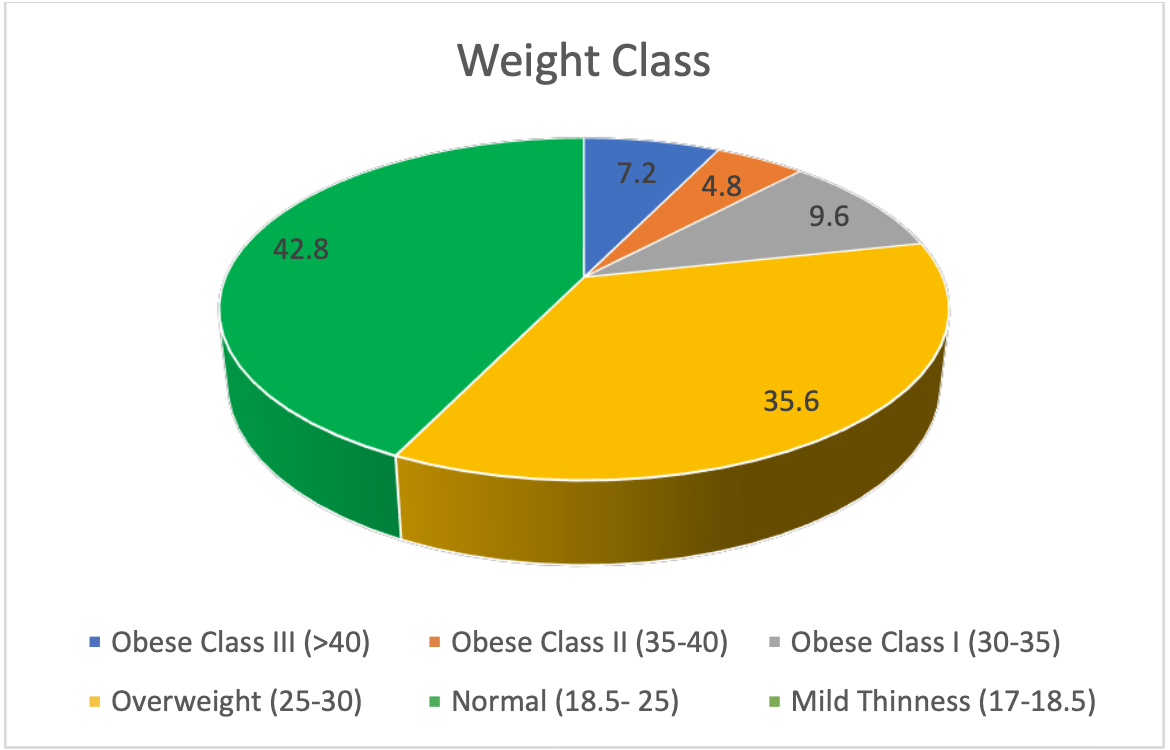
Figure 3 illustrates the graphical representation of distribution of cases according to weight class.
| Weight Class | Number | Percent |
|---|---|---|
| Obese Class III (>40) | 18 | 7.2 |
| Obese Class II (35-40) | 12 | 4.8 |
| Obese Class I (30-35) | 24 | 9.6 |
| Overweight (25-30) | 89 | 35.6 |
| Normal (18.5- 25) | 107 | 42.8 |
| Mild Thinness (17-18.5) | 0 | 0.0 |
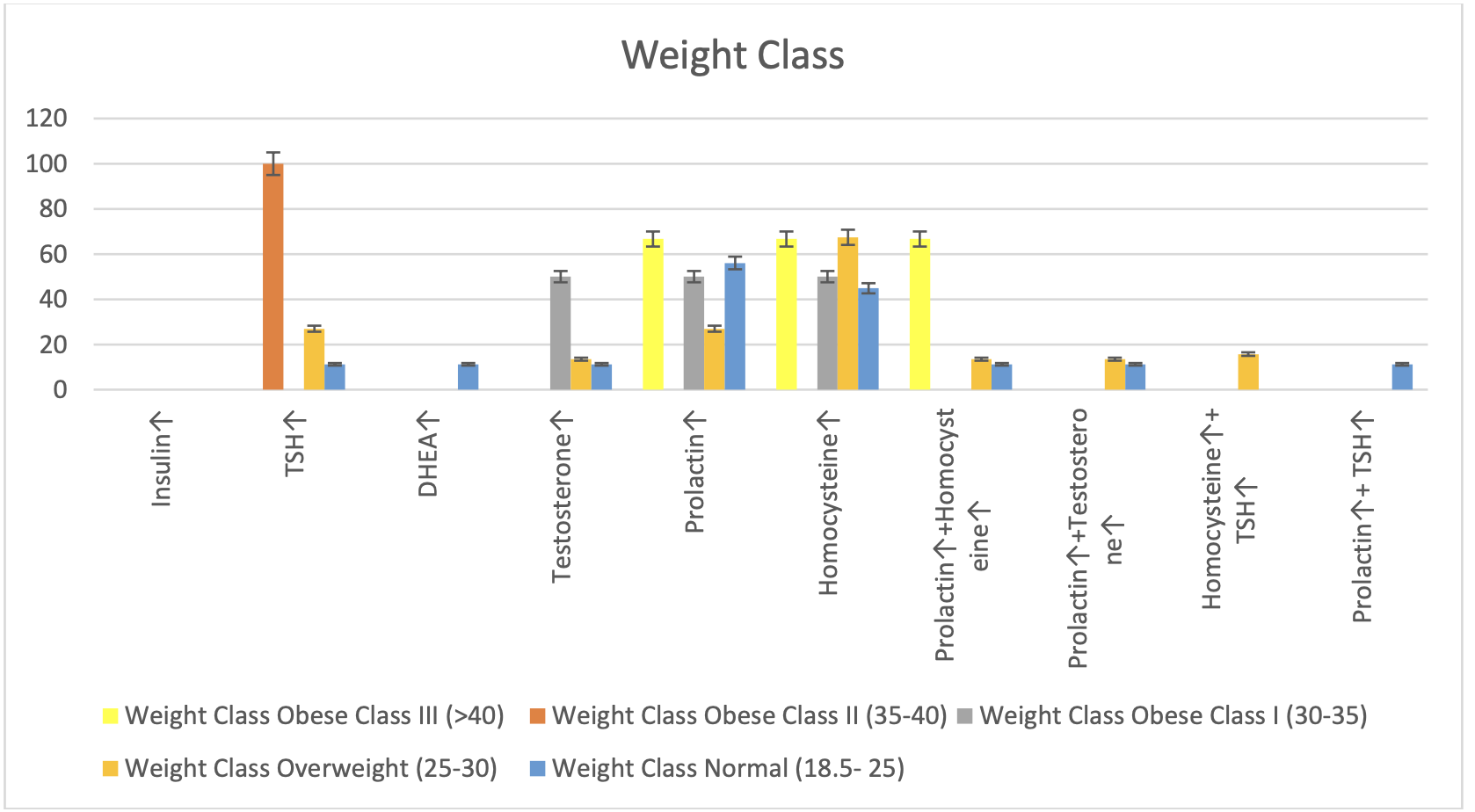
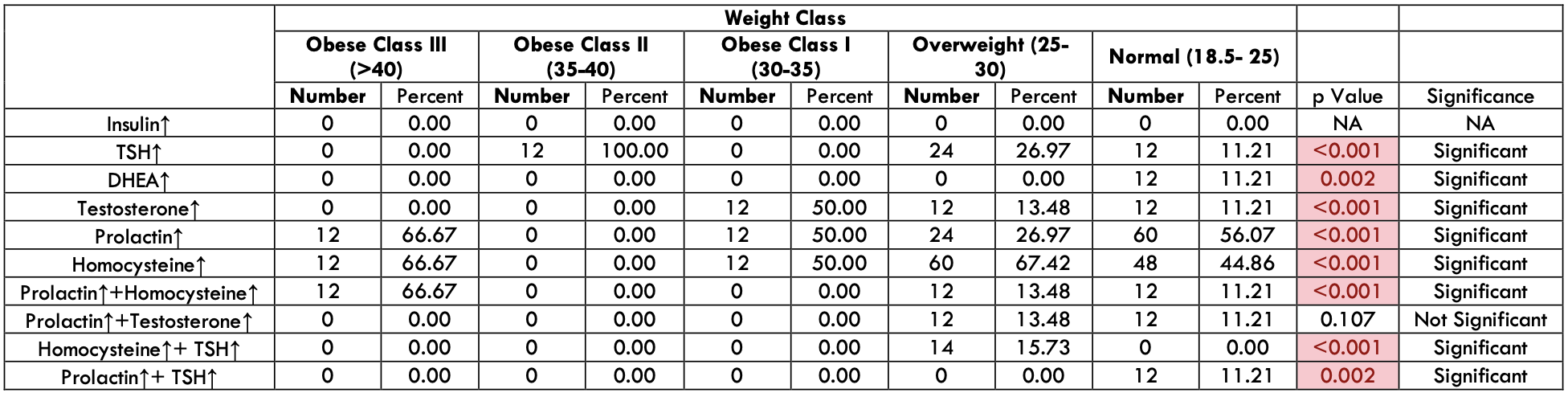
We are comparing the increase in hormone levels across different weight classes (Table- 3). Hypothyroidism was observed in 100% of cases among 12 patients with PCOS in the Obese Class II, in 26.97% of cases among 89 patients with PCOS in the Overweight category, and in 11.21% of cases among 107 patients with PCOS with normal BMI. Hyperandrogenism was observed in 11.21% of cases among 107 patients with PCOS in the normal BMI category, in 50% of cases among 24 patients with PCOS in the Obese Class I and in 13.48% of cases among 89 overweight patients. Hyperprolactinemia was observed in 66.67% of cases among 18 patients with PCOS in the Obese Class III, in 50% of cases among 24 Obese Class I patients, in 26.97% of cases among 89 patients who were overweight and in 56.07% of cases among 107 patients with PCOS with normal BMI. Hyperhomocysteinemia was observed in 66.67% of cases among 18 patients with PCOS in the Obese Class III category, in 50% of cases among 24 patients with PCOS in the Obese Class I category, in 67.42% of cases among 89 patients with PCOS in the Overweight category, and in 44.86% of cases among 107 patients with PCOS in the Normal BMI.
| Weight Class | Insulin↑ | TSH↑ | DHEA↑ | Testosterone↑ | Prolactin↑ | Homocysteine↑ | Prolactin↑+Homocysteine↑ | Prolactin↑+Testosterone↑ | Homocysteine↑+ TSH↑ | Prolactin↑+ TSH↑ |
|---|---|---|---|---|---|---|---|---|---|---|
| Obese Class III (>40) | 0 | 0.00 | 0 | 0 | 12 | 66.67 | 12 | 0 | 0 | 0 |
| Obese Class II (35-40) | 0 | 100.00 | 0 | 0 | 0 | 0.00 | 0 | 0 | 0 | 0 |
| Obese Class I (30-35) | 0 | 0.00 | 0 | 12 | 12 | 50.00 | 0 | 0 | 0 | 0 |
| Overweight (25-30) | 0 | 26.97 | 0 | 12 | 24 | 67.42 | 12 | 12 | 14 | 0 |
| Normal (18.5- 25) | 0 | 11.21 | 12 | 12 | 60 | 44.86 | 12 | 12 | 0 | 0 |
Figure 4 shows the graphical representation of prevalence of single or multiple hormone disorders across different weight classes.
Discussion
PCOS is a multifactorial disease and is found to have association with those who have family history of PCOS, menstrual abnormality, hypertension and type 2 diabetes mellitus. Women with PCO, are at increased risk for gestational diabetes mellitus (GDM) as well. It has been demonstrated that certain gene-gene interactions, and gene-environment interactions influence the development of PCOS, a X-linked polygenic condition, in around 30% of women. In this study, 45.2% of cases reported a family history of PCOS, while 52.4% had a family history of menstrual abnormalities. 9.6% of these women had a family history of hypertension and paternal history of diabetes, 4.8% reported a maternal family history of diabetes. The unopposed action of estrogen leads to endometrial hyperplasia, resulting in a normal menstrual cycle, regular cycles with menorrhagia, oligomenorrhea, or amenorrhea followed by menorrhagia, spotting episodes depending on estrogen levels in the body. In our present study, menstrual abnormalities were most common not only in PCOS patients but also in 52.4% of cases with a family history of menstrual abnormalities. Other investigations have reported that PCOS patients frequently exhibit signs of obesity, hyperandrogenism, and hyperinsulinemia. In our previous study, hypothyroidism, hyperinsulinemia, and hyperandrogenism were found in the maximum number of cases (35%), while hyperinsulinemia alone was present in 25% of cases. Hyperprolactinemia with hyperadrenalism was observed in the minimum number of cases (5%). In our current investigation, hyperhomocysteinemia was detected in the greatest number of cases (52.8%), whereas hyperadrenalism (4.8%) and hyperprolactinemia with hypothyroidism (4.8%) were detected in the smaller number of women. The highest prevalence of hyperprolactinemia (44.64% among 112 patients) and hyperhomocysteinemia (44.64% among 112 patients) was observed in adolescents. Young women showed the highest prevalence of hyperhomocysteinemia (62.31% among 138 patients). We found only 1 or 2 cases of hyperinsulinemia, which can be considered negligible. This is a noteworthy finding, indicating a changing trend in the presentation of PCOS among adolescent and young women. In women with PCOS, elevated homocysteine levels and reduced antioxidant capacity may be associated with a higher risk of cardiovascular disease, recurrent coronary events and myocardial infarction also. The activation of apoptosis, production of oxidative stress, increased expression of inflammatory cytokines, and aberrant methylation are among the molecular pathways of homocysteine-induced cellular dysfunction. Atherogenic and prothrombotic characteristics of Homocysteine like increased fibrinopeptide A and prothrombin fragments 1 and 2, decreased endothelial antithrombotic activity because of thrombomodulin function changes, and activation of factor VIIa and V, contribute to cardiovascular morbidity and mortality. Hyperhomocysteinemia in PCOS women has been linked to increased pregnancy loss and diminished ovulation. In PCOS women undergoing assisted reproduction, elevated follicular homocysteine levels are a strong predictor of the oocyte, embryo quality, and fertilization rate. Women with hyperhomocysteinemia had greater risks of miscarriage and combining aspirin and LMWH therapy may help prevent RPL in hyperhomocysteinemia.
Conclusion
Numerous current or future complications can be avoided with early identification of PCOS in adolescence and young women. Early treatment initiation facilitates the easy and successful stability of the condition for a longer duration. In our recent investigation, increased homocysteine levels were detected in majority of women with PCOS. Since PCOS is linked to several factors such as insulin resistance, impaired glucose tolerance, hyperandrogenemia, obesity, oxidative stress and dyslipidemia, associated hyperhomocysteinemia, may add to the risk of vasculopathy and thromboembolism. Simple folic acid Vitamin B6 and Vitamin B12 replacement can control homocystein level in serum. Further research is needed to understand the function of homocysteine in human reproductive physiology, as well as it’ role among different hormones involved in development of PCOS. This may develop more effective PCOS treatments that can avoid the short and long-term complications.
Acknowledgement
There is no conflict of interest of any author. All authors have equal contributions. There is no external Funding. Funded by institution itself.
References
- Rosenfield RL. The Polycystic Ovary Morphology-Polycystic Ovary Syndrome Spectrum. J Pediatr Adolesc Gynecol. 2015; 28(6): 412-419. doi: 10.1016/j.jpag.2014.07.016.
- Peña AS, Witchel SF, Hoeger KM, Oberfield SE, Vogiatzi MG, Misso M, Garad R, Dabadghao P, Teede H. Adolescent polycystic ovary syndrome according to the international evidence-based guideline. BMC Med. 2020; 18(1): 1-16. doi: 10.1186/s12916-020-01516-x.
- Apter D. Endocrine and metabolic abnormalities in adolescents with a PCOS-like condition: consequences for adult reproduction. Trends Endocrinol Metab. 1998; 9(2): 58-61. doi: 10.1016/s1043-2760(98)00020-4.
- Apter D, Bützow T, Laughlin GA, Yen SS. Accelerated 24-hour luteinizing hormone pulsatile activity in adolescent girls with ovarian hyperandrogenism: relevance to the developmental phase of polycystic ovarian syndrome. J Clin Endocrinol Metab. 1994; 79(1): 119-125. doi: 10.1210/jcem.79.1.8027216.
- Moghetti P, Castello R, Negri C, Tosi F, Spiazzi GG, Brun E, Balducci R, Toscano V, Muggeo M. Insulin infusion amplifies 17 alpha-hydroxycorticosteroid intermediates response to adrenocorticotropin in hyperandrogenic women: apparent relative impairment of 17,20-lyase activity. J Clin Endocrinol Metab. 1996; 81(3): 881-886. doi: 10.1210/jcem.81.3.8772544.
- Wallach EE, Nobels F, Dewailly D. Puberty and polycystic ovarian syndrome: the insulin/insulin-like growth factor I hypothesis. Fertil Steril. 1992; 58(4): 655-666. doi: 10.1016/s0015-0282(16)55307-2.
- Ehrmann DA, Schneider DJ, Sobel BE, Cavaghan MK, Imperial J, Rosenfield RL, Polonsky KS. Troglitazone improves defects in insulin action, insulin secretion, ovarian steroidogenesis, and fibrinolysis in women with polycystic ovary syndrome. J Clin Endocrinol Metab. 1997; 82(7): 2108-2116. doi: 10.1210/jcem.82.7.4069.
- Diamanti-Kandarakis E, Kouli C, Tsianateli T, Bergiele A. Therapeutic effects of metformin on insulin resistance and hyperandrogenism in polycystic ovary syndrome. Eur J Endocrinol. 1998;138(3): 269-274. doi: 10.1530/eje.0.1380269.
- Haghollahi F, Heidary Z, Bagheri M, Masoumi M, Ghaemi M. Polycystic Ovary Syndrome in Adolescence: From the Cradle to the Grave. Fertil, Gynecol Androl. 2022; 2(1). doi: https://doi.org/10.5812/fga-129248.
- Rosenfield RL, Ehrmann DA. The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited. Endocr Rev. 2016; 37(5): 467-520. doi: 10.1210/er.2015-1104.
- Chatterjee S, Chowdhury RG, Ganguly D. Adolescent PCO-The Modern Approach. Journal of Krishna Institute of Medical Sciences (JKIMSU). 2014; 3(2): 160-164.
- Liu J, Wu Q, Hao Y, Jiao M, Wang X, Jiang S, Han L. Measuring the global disease burden of polycystic ovary syndrome in 194 countries: Global Burden of Disease Study 2017. Hum Reprod. 2021; 36(4): 1108-1119. doi: 10.1093/humrep/deaa371.
- Vink JM, Sadrzadeh S, Lambalk CB, Boomsma DI. Heritability of polycystic ovary syndrome in a Dutch twin-family study. J Clin Endocrinol Metab. 2006; 91(6): 2100-2104. doi: 10.1210/jc.2005-1494.
- Nelen WL, Blom HJ, Steegers EA, den Heijer M, Eskes TK. Hyperhomocysteinemia and recurrent early pregnancy loss: a meta-analysis. Fertil Steril. 2000; 74(6): 1196-1199. doi: 10.1016/s0015-0282(00)01595-8.
- Quéré I, Mercier E, Bellet H, Janbon C, Marès P, Gris JC. Vitamin supplementation and pregnancy outcome in women with recurrent early pregnancy loss and hyperhomocysteinemia. Fertil Steril. 2001; 75(4): 823-825. doi: 10.1016/s0015-0282(01)01678-8.
- Meczekalski B, Niwczyk O, Kostrzak A, Maciejewska-Jeske M, Bala G, Szeliga A. PCOS in Adolescents-Ongoing Riddles in Diagnosis and Treatment. J Clin Med. 2023; 12(3): 1221. doi: 10.3390/jcm12031221.
- Gibson-Helm M, Teede H, Dunaif A, Dokras A. Delayed Diagnosis and a Lack of Information Associated With Dissatisfaction in Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2017; 102(2): 604-612. doi: 10.1210/jc.2016-2963.
- Bonny AE, Appelbaum H, Connor EL, Cromer B, DiVasta A, Gomez-Lobo V, Harel Z, Huppert J, Sucato G; NASPAG Research Committee. Clinical variability in approaches to polycystic ovary syndrome. J Pediatr Adolesc Gynecol. 2012; 25(4): 259-261. doi: 10.1016/j.jpag.2012.03.004.
- Auble B, Elder D, Gross A, Hillman JB. Differences in the management of adolescents with polycystic ovary syndrome across pediatric specialties. J Pediatr Adolesc Gynecol. 2013; 26(4): 234-238. doi: 10.1016/j.jpag.2013.03.007.
- Sebastian MR, Wiemann CM, Bacha F, Alston Taylor SJ. Diagnostic Evaluation, Comorbidity Screening, and Treatment of Polycystic Ovary Syndrome in Adolescents in 3 Specialty Clinics. J Pediatr Adolesc Gynecol. 2018; 31(4): 367-371. doi: 10.1016/j.jpag.2018.01.007.
- Peña AS, Metz M. What is adolescent polycystic ovary syndrome? J Paediatr Child Health. 2018; 54(4): 351-355. doi: 10.1111/jpc.13821.
- Witchel SF, Oberfield S, Rosenfield RL, Codner E, Bonny A, Ibáñez L, Pena A, Horikawa R, Gomez-Lobo V, Joel D, Tfayli H, Arslanian S, Dabadghao P, Garcia Rudaz C, Lee PA. The Diagnosis of Polycystic Ovary Syndrome during Adolescence. Horm Res Paediatr. 2015; 83 (6): 376-389. doi: 10.1159/000375530.
- ESHRE TR, ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil steril. 2004; 81(1): 19-25. doi: https://doi.org/10.1016/j.fertnstert.2003.10.004
- Ibáñez L, Oberfield SE, Witchel S, Auchus RJ, Chang RJ, Codner E, Dabadghao P, Darendeliler F, Elbarbary NS, Gambineri A, Garcia Rudaz C, Hoeger KM, López-Bermejo A, Ong K, Peña AS, Reinehr T, Stener-Victorin E. An International Consortium Update: Pathophysiology, Diagnosis, and Treatment of Polycystic Ovarian Syndrome in Adolescence. Horm Res Paediatr. 2017; 88(6): 371-395. doi: 10.1159/000479371.
- Zawadri J. Diagnostic criteria for polycystic ovary syndrome: towards a rational approach. Polycystic ovary syndrome. Current issues in endocrinology and metabolism. 1992.
- Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, Janssen OE, Legro RS, Norman RJ, Taylor AE, Witchel SF; Androgen Excess Society. Positions statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guideline. J Clin Endocrinol Metab. 2006; 91(11): 4237-4245. doi: 10.1210/jc.2006-0178.
- Teede HJ, Misso ML, Costello MF, Dokras A, Laven J, Moran L, Piltonen T, Norman RJ; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2018;110(3): 364-379. doi: 10.1016/j.fertnstert.2018.05.004.
- Teede H, Deeks A, Moran L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010; 8 (1): 41. doi: 10.1186/1741-7015-8-41.
- Dahlgren E, Janson PO, Johansson S, Lapidus L, Odén A. Polycystic ovary syndrome and risk for myocardial infarction. Evaluated from a risk factor model based on a prospective population study of women. Acta Obstet Gynecol Scand. 1992; 71(8): 599-604. doi: 10.3109/00016349209006227.
- Talbott E, Guzick D, Clerici A, Berga S, Detre K, Weimer K, Kuller L. Coronary heart disease risk factors in women with polycystic ovary syndrome. Arterioscler Thromb Vasc Biol. 1995; 15(7): 821-826. doi: 10.1161/01.atv.15.7.821.
- Wild RA. Obesity, lipids, cardiovascular risk, and androgen excess. Am J Med. 1995; 98(1A): 27S-32S. doi: 10.1016/s0002-9343(99)80056-4.
- Collaboration HS. Homocysteine and risk of ischemic heart disease and stroke. Jama. 2002; 288(16): 2015-2022. doi: 10.1001/jama.288.16.2015.
- Pierpoint T, McKeigue PM, Isaacs AJ, Wild SH, Jacobs HS. Mortality of women with polycystic ovary syndrome at long-term follow-up. J Clin Epidemiol. 1998; 51(7): 581-586. doi: 10.1016/s0895-4356(98)00035-3.
- Nagaria T, Mohapatra A, & Jaiswal J. Effect of Myoinositol and Metformin in combination on clinical and hormonal profile in patients of polycystic ovarian syndrome. Int J Reprod Contracept Obstet Gynecol, 2019; 8(2), 702. doi: https://doi.org/10.18203/2320-1770.ijrcog20190309.
- Chirania, K., Misra, S., & Behera, S. A randomised clinical trial comparing myoinositol and metformin in PCOS. Int J Reprod Contracept Obstet Gynecol. 2017;6(5), 1814-1820. doi: https://doi.org/10.18203/2320-1770.ijrcog20171563.
- Mor E, Zograbyan A, Saadat P, Bayrak A, Tourgeman DE, Zhang C, Stanczyk FZ, Paulson RJ. The insulin resistant subphenotype of polycystic ovary syndrome: clinical parameters and pathogenesis. Am J Obstet Gynecol. 2004; 190(6): 1654-1660. doi: 10.1016/j.ajog.2004.02.052.
- Mehreen, T. S., Ranjani, H., Kamalesh, R., Ram, U., Anjana, R. M., & Mohan, V. Prevalence of polycystic ovarian syndrome among adolescents and young women in India. Journal of Diabetology, 2021; 12(3), 319-325. doi: 10.4130/JOD.JOD_105_20.
- Wang B, Mo X, Wu Z, Guan X. Systematic review and meta-analysis of the correlation between plasma homocysteine levels and coronary heart disease. J Thorac Dis. 2022;14(3): 646-653. doi: 10.21037/jtd-22-78.
- Maleedhu P, M V, S S B S, Kodumuri PK, Devi D V. Status of Homocysteine in Polycystic Ovary Syndrome (PCOS). J Clin Diagn Res. 2014; 8(2): 31-33. doi: 10.7860/JCDR/2014/7070.3999.
- Mohan SK, Priya VV. Lipid peroxidation, glutathione, ascorbic acid, vitamin E, antioxidant enzyme and serum homocysteine status in patients with polycystic ovary syndrome. Biology and Medicine. 2009; 1 (3): 44-49.
- Forges T, Monnier-Barbarino P, Alberto JM, Guéant-Rodriguez RM, Daval JL, Guéant JL. Impact of folate and homocysteine metabolism on human reproductive health. Hum Reprod Update. 2007; 13(3): 225-238. doi: 10.1093/humupd/dml063.
- Salehpour S, Manzor-Al-Ajdad O, Samani EN, Abadi A. Evaluation of homocysteine levels in patients with polycystic ovarian syndrome. Int J Fertil Steril. 2011; 4(4): 168-171.
- Chang H, Xie L, Ge H, Wu Q, Wen Y, Zhang D, Zhang Y, Ma H, Gao J, Wang CC, Stener-Victorin E, Ng EH, Wu X. Effects of hyperhomocysteinaemia and metabolic syndrome on reproduction in women with polycystic ovary syndrome: a secondary analysis. Reprod Biomed Online. 2019; 38(6): 990-998. doi: 10.1016/j.rbmo.2018.12.046.
- Berker B, Kaya C, Aytac R, Satiroglu H. Homocysteine concentrations in follicular fluid are associated with poor oocyte and embryo qualities in polycystic ovary syndrome patients undergoing assisted reproduction. Hum Reprod. 2009; 24(9): 2293-2302. doi: 10.1093/humrep/dep069.
- Chakraborty P, Banerjee S, Saha P, Nandi SS, Sharma S, Goswami SK, Chakravarty B, Kabir SN. Aspirin and low-molecular weight heparin combination therapy effectively prevents recurrent miscarriage in hyperhomocysteinemic women. PLoS One. 2013; 8(9): e74155. doi: 10.1371/journal.pone.0074155.
- Chakraborty P, Goswami SK, Rajani S, Sharma S, Kabir SN, Chakravarty B, Jana K. Recurrent pregnancy loss in polycystic ovary syndrome: role of hyperhomocysteinemia and insulin resistance. PLoS One. 2013; 8(5): e64446. doi: 10.1371/journal.pone.0064446.
- Yildiz BO, Bozdag G, Yapici Z, Esinler I, Yarali H. Prevalence, phenotype and cardiometabolic risk of polycystic ovary syndrome under different diagnostic criteria. Hum Reprod. 2012; 27(10): 3067-3073. doi: 10.1093/humrep/des232.
- Barber TM, McCarthy MI, Wass JA, Franks S. Obesity and polycystic ovary syndrome. Clin Endocrinol (Oxf). 2006; 65(2): 137-145. doi: 10.1111/j.1365-2265.2006.02587.x.
- Ollila MM, Piltonen T, Puukka K, Ruokonen A, Järvelin MR, Tapanainen JS, Franks S, Morin-Papunen L. Weight Gain and Dyslipidemia in Early Adulthood Associate With Polycystic Ovary Syndrome: Prospective Cohort Study. J Clin Endocrinol Metab. 2016; 101(2): 739-747. doi: 10.1210/jc.2015-3543.
- Barber TM, Hanson P, Weickert MO, Franks S. Obesity and Polycystic Ovary Syndrome: Implications for Pathogenesis and Novel Management Strategies. Clin Med Insights Reprod Health. 2019; 13: 1179558119874042. doi: 10.1177/1179558119874042.
- Glueck CJ, Goldenberg N. Characteristics of obesity in polycystic ovary syndrome: Etiology, treatment, and genetics. Metabolism. 2019; 92: 108-120. doi: https://doi.org/10.1016/j.metabol.2018.11.002.
- Goodarzi MO, Dumesic DA, Chazenbalk G, Azziz R. Polycystic ovary syndrome: etiology, pathogenesis and diagnosis. Nat Rev Endocrinol. 2011; 7(4): 219–231. doi: https://doi.org/10.1038/nrendo.2010.217.
- Ramezani Tehrani F, Amiri M. Polycystic Ovary Syndrome in Adolescents: Challenges in Diagnosis and Treatment. Int J Endocrinol Metab. 2019; 17(3): e91554. doi: 10.5812/ijem.91554.
- Kostopoulou E, Anagnostis P, Bosdou JK, Spiliotis BE, Goulis DG. Polycystic ovary Syndrome in Adolescents: Pitfalls in Diagnosis and Management. Curr Obes Rep. 2020; 9 (3), 193–203. doi: https://doi.org/10.1007/s13679-020-00388-9.
- Barber TM, Franks S. Adipocyte biology in polycystic ovary syndrome. Mol Cell Endocrinol. 2013; 373(1-2): 68-76. doi: 10.1016/j.mce.2012.10.010.
- Dumesic DA, Oberfield SE, Stener-Victorin E, Marshall JC, Laven JS, Legro RS. Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr Rev. 2015; 36(5): 487-525. doi: 10.1210/er.2015-1018.
- Manique MES, Ferreira AMAP. Polycystic Ovary Syndrome in Adolescence: Challenges in Diagnosis and Management. Rev Bras Ginecol Obstet. 2022; 44(4): 425-433. doi: 10.1055/s-0042-1742292.