

Peer Navigator Employment Training for Health Care Transition
Peer Navigator Employment Training Program: A Health Care Transition Service-Training Model
Christine Bottrell Mirzaian, MD, MPH, 1; Rowan Smith, MPH 2; Courtney Porter, MPH 3; George M. de la Loza, MA, MS 4; Cecily L. Betz, PhD, RN, FAAN 5
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: MIRZAIAN, Christine Bottrell et al. Peer Navigator Employment Training Program: A Health Care Transition Service-Training Model. Medical Research Archives, [S.l.], v. 13, n. 3, mar. 2025. Available at: <https://esmed.org/MRA/mra/article/view/6446>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i3.6446
ISSN 2375-1924
Abstract
Background: Health care transition (HCT) service disparities are evident for youth and young adults with intellectual and/or developmental disabilities when compared to other populations of youth and young adults with chronic conditions, resulting in service discontinuities in accessing adult-focused care and acquisition of developmental milestones associated with adulthood. Models of care to address their unique needs for services have been reported to advance acquisition of HCT outcomes.
Methodology: An innovative HCT service model, Peer Navigator Employment Training Program (PNETP) is described in this paper. The PNETP is a service-training model focused on providing HCT services to youth and young adults and concomitantly training individuals with intellectual and/or developmental disabilities to serve as HCT peer navigators. The PNETP training program features a unique partnership among intellectual and/or developmental disability service and employment agencies and a regional pediatric medical center.
Preliminary Findings. A description of the PNETP is presented together with pilot data describing the PNETP implementation. Integral to the development of this model are the ongoing efforts to gather data from potential and actual users. Parental input was elicited for programmatic development. Descriptive data obtained with the initiation of PNETP is presented.
Conclusions. Preliminary PNETP implementation and programmatic pilot data suggest promise for its dual purpose of facilitating employment opportunities for individuals with intellectual and/or developmental disabilities as peer navigators in healthcare and social service settings and services for transition-aged youth and young adults. This specialty community health worker role shows not only promise for HCT navigation but for other specialty care services that would benefit from peer navigation support.
Keywords
Peer Navigator, Employment Training, Health Care Transition, Intellectual Disabilities, Developmental Disabilities
1. Introduction
This paper will describe the Peer Navigator Employment Training Program (PNETP) developed and implemented at Children’s Hospital Los Angeles University Center for Excellence in Developmental Disabilities (CHLA UCEDD). PNETP has the dual purpose of providing training to individuals with intellectual and/or developmental disabilities (IDD) to acquire knowledge and learn the skills to provide health care transition (HCT) services as peer navigators to youth and young adults with IDD (YYA with IDD) that assist them to facilitate their transfer of care to adult-focused providers and transition to adulthood. This innovative HCT service model is unique among the HCT models published in the literature that features a new HCT model of care as it addresses service needs of the underserved population of YYA with IDD while fostering the development of a heretofore untapped source of workforce providers that offer new opportunities for employment for the IDD population. As will be presented in this paper, PNETP interns acquire competencies comparable to the roles of community health workers (CHWs) in the healthcare system. PNETP builds upon and expands the benefits, value and potential of peer support/navigation for those with childhood acquired conditions including those with IDD to enable peers who are IDD self-advocates to serve as direct service providers. Relevant to the development of PNETP, we conducted a survey with 11 parents of sons and daughters with IDD who had been through the transition process. The research team gathered descriptive data to improve understanding of the HCT issues the YYA with IDD and their parents experienced with the transfer of care to adult-focused providers and interagency service systems to facilitate the transition to adulthood. The purpose of this paper is to describe the planning process of PNETP and its implementation.
2. Program Development Components
The PNETP draws upon several areas of HCT service needs and adult-focused employment outcomes identified in the IDD populations. This background section will provide an overview of the following programmatic and practice areas integral to the development and implementation of PNETP. Background content includes the following: a) HCT and YYA with IDD; b) IDD and Postsecondary Education; c) IDD and Employment; d) Peer Navigation; e) Community Health Workers; f) Assessment of Need for Peer Navigator Services from a Community Perspective; and g) Early PNETP Beginnings.
2.1. HEALTH CARE TRANSITION FOR YOUTH AND YOUNG ADULTS WITH INTELLECTUAL AND/OR DEVELOPMENTAL DISABILITIES.
The provision of HCT services involves an array of services and supports to facilitate the transfer of care and transition to adulthood. As has been asserted, “HCT has been described as a compendium of provider-oriented activities and outcomes that include the development of an individualized and asset-oriented transition plan …; parental support to cope with the adolescent’s role changes; transfer processing between pediatric- and adult-focused providers; an identified transition services coordinator; self-management training and referrals to transition and adult-focused services”. It has been widely acknowledged that HCT service disparities exist for YYA with IDD when compared to other diagnostic groups of YYA with childhood acquired conditions. Although reports of the numbers of youth with childhood acquired chronic conditions who enter adulthood are widely reported, with estimates cited of approximately one million, comparable data on the IDD population is not definitively known. Reported estimates indicate that 1 in 6 youth have a developmental disability (DD). As recent national surveys report, the DD and ID prevalence rates are on the rise. The 2021 prevalence rate of DD in children and youth ages, 3 to 17 years is 8.56%, higher than reported prevalence 7.40% in 2019; intellectual disability (ID) in youth ages 13 to 17 years is 2.35%, higher than the reported prevalence in children ages 3 to 12 years and ID prevalence (1.41%) for 13 to 17 years, 2009 to 2017. As the prevalence data indicates, there will be growing demands for HCT services as the number of YYA with IDD entering adulthood increases. Adverse outcomes related to HCT disparities have been reported in HCT planning that includes disengagement from services, fewer HCT services and limited information about health care resources. Several published reports have highlighted YYA with IDD have more unmet needs for HCT planning services given their lifelong challenges for supports for learning, self-management, and accessing services for primary care and specialty adult-focused providers who feel comfortable and clinically competent to provide care.
2.2. INTELLECTUAL AND/OR DEVELOPMENTAL DISABILITIES AND POSTSECONDARY EDUCATION.
In the largest national survey conducted exploring postsecondary outcomes of students with disabilities, the National Longitudinal Transition Study-2 (NLTS2) findings revealed disparate outcomes for those with ID as compared to other groups of students with disabilities. Young adults with ID have the lowest rates of postsecondary education enrollment (29%) compared to those with multiple disabilities (33%), autism (44%), and deaf blindness (57%). Examination of post-secondary education enrollment patterns found young adults with ID were enrolled in the following programs in descending order: 2-year community college (18.9%), vocational, technical, or business school (16.4%) and 4-year college (6.7%). All enrollment percentages when compared to other groups of students with disabilities were lower, including those with autism and deaf blindness. Other findings reported young adults with ID were lowest compared to other disabilities groups related to college metrics of steady enrollment in school (44.5%) and full-time enrollment (45.5%). More recently, widespread efforts have been undertaken to create more inclusive opportunities for students with IDD in post-secondary settings. Federal and state leadership has promoted the needed investment and legislation to enable the creation of 340 higher education programs in 49 states and state level coordination of postsecondary options for students with ID. It is now estimated that over 6,000 students with ID are enrolled in higher education programs.
2.3. INTELLECTUAL AND/OR DEVELOPMENTAL DISABILITIES AND EMPLOYMENT.
Employment rates for individuals with IDD vary depending on the diagnostic category. Individuals with ID have the lowest reported rates of employment compared to other disability groups. Individuals with ID continue to lag behind the metrics associated with employment and rates of poverty. In 2022, the employment rate of individuals with ID was nearly half of those without intellectual disabilities (44.5% vs. 78.9%). Rates of poverty for individuals with ID are considerably higher (25.9%) as compared to individuals without ID (11.5%) – nearly three times higher. An earlier survey sponsored by Special Olympics exploring employment profiles of adults with ID provided disappointing findings. The Special Olympics survey reported a lower percentage of adults with IDD, ages 21 to 64 employed; of whom nearly 50% work in sheltered workshops. It is estimated that 28% of adults with ID have never been employed. All were underemployed. In addition, there is a demand from individuals with disabilities for employment. According to the 2020/2021 National Core Indicators Survey conducted by the California Department of Developmental Services, 62% of individuals with developmental disabilities who are unemployed would like to have employment and 27% have job-related training. This demonstrates a need for more employment opportunities for individuals with DD and the creation of new employment pathways. As the employment data on individuals with IDD continues to reveal, employment rates remain persistently low despite widespread efforts to foster employment training options for the IDD community.
2.4. PEER NAVIGATION.
Variations of navigation models have been described as an adjunct model of care to assist patients with accessing needed resources and obtaining additional educational materials. Navigation services feature in-depth assistance with locating resources that may be difficult for recipients to access being unfamiliar with the where, how and what of services and supports that are available. Navigators are focused on providing one-to-one guidance using a person-centered approach that includes responsiveness to recipient questions that arise as they learn to navigate systems of care for which they have no prior experience. Navigators are informational resources that provide recipients’ in-depth understanding of types of referrals services and supports made that extend beyond information typically shared by health care providers. Peer navigators can provide recipients with basic information about agencies/organizations services and assist with analyzing service options that are optimal for recipients. Models of peer navigation have been reported as an intervention approach with a myriad of populations across the lifespan, often focused on vulnerable and underserved populations. The preponderance of research has been conducted with adult populations; few studies have been directed to youth with IDD. The unique focus of the peer navigation model is the shared lived experience between the support provider and the service recipient that enhances the perceived value of service interactions.
2.5. COMMUNITY HEALTH WORKERS.
Community Health Workers (CHW) are non-licensed, trained health supports who provide informational resources, social support, navigation assistance, and service referrals to community-based programs and serve as liaisons between clients and health care team members. Peer navigators could be considered a specialized type of community health worker. According to the American Public Health Association, a community health worker is a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served. This trusting relationship enables the worker to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery. A community health worker also builds individual and community capacity by increasing health knowledge and self-sufficiency through a range of activities such as outreach, community education, informal counseling, social support and advocacy. Their approach to care is holistic and is based upon a broad and inclusive concept of health that incorporates biopsychosocial, developmental and environmental domains that focuses on the health-related social needs and barriers, much like those identified by World Health Organization (WHO) such as financial resources for food, housing and basic necessities. Currently there are 63,400 community health workers. CHWs work in hospital and community-based health settings. This service model was originally adopted in low-resources countries to address the health-related needs of unserved and underserved populations. The CHW model was first introduced thirty years ago in the US; renewed interest has sparked its application in diverse settings and populations within the U.S. health care system. To date, there is not a widely accepted definition of a peer navigator; however, there are role characteristics, functions and responsibilities that share CHW commonalities pertaining to the scope of practice regardless of patient group across the lifespan and settings. These role responsibilities include:
- Provide resource information on health-related needs and community resources
- Facilitate access to health-related and community-based programs
- Serve as a liaison between the care recipients and members of the health care team
- Serve as an advocate
- Assist care recipients with navigating services and programs
- Assist with identifying and eliminating barriers to services.
2.6 ASSESSMENT OF NEED FOR PEER NAVIGATOR SERVICES FROM A COMMUNITY PERSPECTIVE
As part of a larger study, eleven parents/legal guardians were interviewed as to their perceptions of the transition experience as we embarked with the development and implementation of the peer navigation training program.
2.6.1. Parent Interviews
After IRB approval was obtained, data were gathered from 11 parents/guardians. Parents for this study were recruited by distributing flyers and information sheets via email to community-based parent support and disability advocacy groups who have been members of the CHLA UCEDD community partner network. Parent interviews were conducted via phone, which lasted approximately 30 minutes. These interviews were audio-recorded and transcribed. The interview guide contained 11 questions, three of which queried parental interest in having their son or daughter receive peer navigator services, the feasibility of their children being trained as a peer navigator and the potential benefits of a peer navigator program. Gift cards ($50) were distributed to parents following interviews.
2.6.2. Data Analysis.
Data were collected anonymously; therefore, limited demographic data were available to report. The Framework Method for Qualitative Analysis was used to guide the data analysis. Initially three research team members (C.M., R.S., C.B.) independently coded three interviews. After coding these interviews, the team met to compare and contrast the coding performed amongst the three team members. This comprehensive review set the basis for subsequent reviews that were conducted by two team members, wherein any conflicts that arose were resolved during the coding process (C.M., C.B.). The final analysis resulted in the following three themes generated from the data as identified in Table 1, Theme 1: Parent Perspective: Peer Navigation Not Feasible; Theme 2: Parent Perspective: Child Could Be Peer Navigator; Theme 3: Parental Perspective: Peer Navigation Beneficial.
| Interview Themes | Parent’s responses |
|---|---|
| Theme 1; Parent Perspective: Peer Navigation Not Feasible | Yeah. Like I said, I don’t know that a person with disability would have helped [Son J] but the families, they were helpful. You know, the families that have been raising their child with Down syndrome, they were the ones that were helpful. But the child with Down syndrome, I don’t know that [Son J] would have benefited from that. It’s an interesting idea though (Parent 7) |
| No, it’s not feasible because his disability is just too big. So he could not do it. What we do actually, a lot of moms, is that we share information and we exchange information between us. (Parent 4) | |
| For her specifically, peer to peer, I don’t know if my daughter would have the capacity to comprehend that information. (Parent 1) | |
| I mean she pretty much has a hard time just, yeah, no. My husband and I we pretty much manage all of the agency related interactions, decisions and the school-based ones (Parent 1) | |
| Well, my son is nonverbal. He doesn’t have a lot [specific?] behaviors or anything like that. But you know the nonverbal part can be difficult and like I said, he requires a lot of one-to-one assistance. So sometimes being more independent is problematic. So that’s why I’m saying that that would probably be a barrier for him. (Parent 3) | |
| Theme 2: Parent Perspective: Child Could Be Peer Navigator | I’m sure everybody’s trainable but he would need a lot of supports and services. Even now, we have the technology, so you could, you know, teach him, he would be able to type out that thing, because, you know, verbalizing is still difficult. But if he received the right kind of training [INDISTINCT] now because he’s an adult, it would take longer time than had it been done when he was younger, because, you know, younger brains are a little bit easier now they say. But yes. (Parent 10) |
| Yeah. I am a believer of any person, no matter his abilities, his medical condition, can have the opportunity to train and to work, with the support of someone (Parent 11) | |
| Heck, yeah. [LAUGHTER] Obviously, in [daughter L.]’s case, it would be a partnership. [LAUGHS] You’d get two for the [bang?] over here. I guess I would be the job coach person or whatever. Because while she, you ask her a question, the answer is in her head. We’ve just got to get it out. [LAUGHS] As to whether it’s a dry erase board, or a device, or something. So, it would need to be that. (Parent 9) | |
| Theme 3: Parental Perspective: Peer Navigation Beneficial | Oh yeah, for sure. (Parent 8) |
| Absolutely. (Parent 10) | |
| Oh. Of course. That’s for us parent we all get lost. We get lost especially on the medical area. But if you want to make a change, it is essential to create a database with doctors where we can go. (Parent 11) | |
| Oh yeah. I mean, and twofold. One, obviously, He closer that that person or that family fit who it is they’re helping, the better. Because they’re going to have experience with the same, or at least similar kinds of issues, that the new family, be it ourselves or whomever, would have. But also, back to the whole friendship thing. [LAUGHS] Maybe it becomes a friendship type of thing. (Parent 9) | |
| Yeah, I think so. I mean that’s always helpful. (Parent 6) | |
| Yeah, it would be a good thing, someone to know the system. But also, I would like to point out that navigating through the system, it’s really very, very much stressing, and it’s very much [exasperating?]. You know, for me, it would be a good thing, a coordination between the different services that they have, you know, pediatricians and, you know, the different needs that he has, you know, to they coordinated and to do the transition correctly. (Parent 4) | |
| I absolutely do believe that. I absolutely do (Parent 5) | |
| Oh sure, yeah (Parent 1) | |
| Yeah, potentially. (Parent 3) |
2.6.3. Survey Findings
Eleven parents all of whom were mothers participated in this study. Two were parents of daughters. One interview was conducted in Spanish.
As presented in Table 1, Theme 1: Parent Perspective: Peer Navigation Not Feasible, five parents felt becoming a peer navigator would not be a feasible employment option for their children. These reasons were predicted on the level of involvement of their children’s disability. One of the parents mentioned that their child’s “disability is just too big” (Parent 4); another parent noted her son is nonverbal. Remaining parents believed becoming a peer navigator would be a feasible employment option for their children; however, some expressed caution as exemplified by this parent’s response, “I’m sure everybody’s trainable but he would need a lot of supports and services” (Parent 10). Theme 2, Parent Perspective: Child Could Be Peer Navigator. Several parents acknowledged their children could be peer navigators. As presented in Theme 3, Parental Perspective: Peer Navigation Beneficial, parents comments included positive affirmations such as, “I absolutely do believe that. I absolutely do” (Parent 5). Another parent remarked the benefits could be attributed to the following circumstances “…because they’re going to have experience with the same, or at least similar issues” (Parent 9).
2.6.4. Survey Discussion.
These comments provided the team with additional insights and understanding about parents’ perspectives about the peer navigator training program that guided our training efforts. As these findings indicate, these parents expressed a mixture of perspectives about the proposed peer navigator program. Parents whose son or daughter have more severe levels of IDD involvement shared that the peer navigator program would not be feasible as either a service recipient or peer navigator. Other parents regardless of their son’s or daughter’s level of involvement expressed aspirational remarks about the potential of their children engaging as a peer navigator. There was widespread agreement that training individuals with IDD to become peer navigators would be helpful as parents expressed that assistance with the challenges with accessing transition and adult-focused services would be beneficial. The findings of this descriptive study provided the study team with informed insights with the early development of the peer navigator program. Their input was integrated into the training framework as peer navigator training modules and outreach strategies were developed as described in this paper.
2.7. EARLY BEGINNINGS.
Starting in 2022, our transition team at the CHLA UCEDD was initially awarded one-year funding from the California Department of Developmental Services to develop a peer navigator program, focused on HCT then called the Innovative Peer Navigator Employment Program in partnership with a local regional center. Two Peer Navigators who received training during that funding period provided HCT services to 21 YYA with developmental disabilities. This program, now known as the Peer Navigator Employment Training Program (PNETP) received funding in April, 2024 for two years from the Mitsubishi Electric America Foundation (MEAF) to expand and extend the program to train a larger number of individuals with developmental disabilities as peer navigators and provide health care transition services to more YYA with IDD.
3. Peer Navigator Employment Training Program Partnership.
The PNETP is a paid internship program for individuals with IDD aimed to provide marketable work skills in an integrated setting that can lead to inclusive and paid employment in healthcare and social service settings. PNETP combines partnership activities between two divergent service systems designed for dissimilar missions and goals yet integrates them into an innovative training program to achieve its dual training and service purposes.
3.1. COMMUNITY-BASED ORGANIZATIONS.
The Paid Internship Program (PIP) is an employment initiative of the California Department of Developmental Services. The aim of PIP is to foster employment opportunities for individuals with IDD who receive services through statewide regional centers, non-profit agencies whose organizational purpose is to develop, purchase, and coordinate services for individuals with IDD. This is accomplished through paid internships, wherein interns are paid at least minimum wage or more up to 1040 hours per year to learn vocational skills in a training program. The goal of these training programs is to provide needed job skills for interns to be hired in a competitive integrated employment setting. Since its inception, PNETP has established PIP partnerships with several RCs and job training agencies that have enabled the recruitment of eligible applicants into the PNETP with PIP funding, which includes provision of a job coach who focuses on professional development behaviors of interns such as abiding by institutional workplace practices and policies.
3.2. THE CHLA UCEDD TRANSITION TEAM.
The training staff (CB, CM, RS) developed and implemented the Peer Navigation training program. This program is a product of the transition team’s extensive experience and expertise in health care transition, navigation model development, and provision of services and supports and community-based programmatic efforts for the IDD population. The CHLA UCEDD partnership provides an instructional and clinically based training program enabling interns to provide HCT services to transition aged youth/young adults who receive services at CHLA. The CHLA instructional team and PIP job coaches work collaboratively as a training team with the enrolled interns.
5. Peer Navigator Employment Training Program Framework
The PNETP Framework is an integration of several conceptual approaches that have guided the development of the curriculum. The Health Care Transition Research Consortium HCT model embraces a lifespan ranging from early adolescence to emerging adulthood that is comprehensive in it approach addressing four domains of the lived experience -Individual, Family/Social Support, Environment, and the Health Care System during the transition period.

Some of the underlying assumptions of the model include the following:
- Health planning embodies a lifespan approach wherein children are supported throughout their development to achieve their highest level of functioning while learning to self-manage their condition; thereby enabling them to achieve their goals more easily for adulthood pertaining to the Individual, Family/Support, Environmental and Health Care System Domains.
- Health care transition care starts with an adolescent/family centered framework and migrates to an adolescent-centered framework and throughout adolescence and emerging adulthood that depends on providing services that are evidence based and appropriate for the biopsychosocial developmental stage of the adolescents and emerging adults with special health care needs and his or her family/social and environmental supports.
Concepts associated with patient navigation have been integrated and adapted to this service model that have been previously described. Additionally, our PNETP team member (CM) initiated a parent navigator model six years ago composed of four parent navigators who have provided services to over 6,000 families. Drawing upon this experience, the parent navigator model experience has been an invaluable asset with the development and implementation of the PNETP.
6. Peer Navigator Employment Training Program Training Program
The PNETP is a 6-month training program. For the first two to three months of the program, the focus is on the acquisition of knowledge and skills needed to function as a peer navigator. These skills involve case management, ethics and boundary setting, person-centered thinking, and communication. The PNETP training program consists of the following curricular elements: a) instructional modules; b) group instruction; c) 1 to 1 coaching; d) job shadowing; e) clinical practice; f) conferencing as presented in Box 1 that are described in detail below.

Box 1: The Peer Navigator Employment Training Program Overview
The didactic portion (instructional modules, group instruction, 1 to 1 coaching) is followed by three months of supervised job training (1 to 1 coaching, job shadowing, clinical practice with providing peer navigation services to transition-aged YYA with IDD and their families. Peer Navigators learn office behavior, resource development, case management and service referral skills. Peer Navigators will learn information on how to make referrals to adult-focused primary and specialty health care providers and the community-based services for employment, postsecondary education, community living, and social, recreational, and leisure activities.
6.1. PEER NAVIGATOR EMPLOYMENT TRAINING PROGRAM INSTRUCTIONAL MODULES.
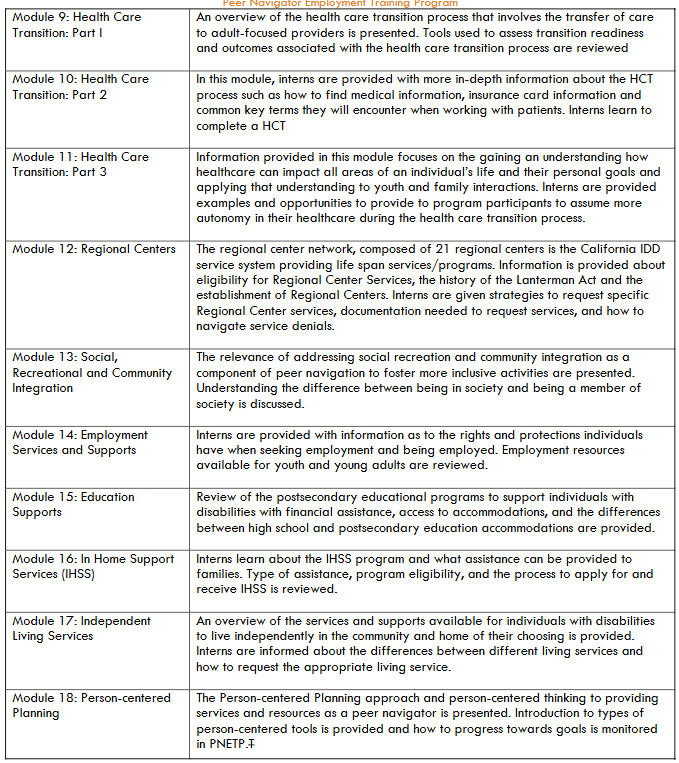
The PNETP consists of 18 modules designed to provide interns with comprehensive subject matter to learn content needed to function as a peer navigator. The instructional modules cover content on the knowledge and skills needed to learn about the role responsibilities of a peer navigator and the provision of HCT services and supports. PNETP curriculum provides interns with detailed information about the components of the transfer of care to adult-focused providers that include locating primary and specialty providers in their communities of choice, enrollment in health insurance plans, and coordination with CHLA inhouse pediatric providers. Interns learn about the extensive array of community-based transition and adult-focused resources based upon individualized needs. These resource referrals are typically for postsecondary educational programs, job development and placement and recreational interests. Each of the modules contains learning objectives, informational content, videos, links to resource websites and practice reviews. Completion time for the modules will vary depending upon the learning needs and pace of progression for interns; generally, interns’ immersion in modules takes four to six weeks. The description of modules is presented in Box 2.
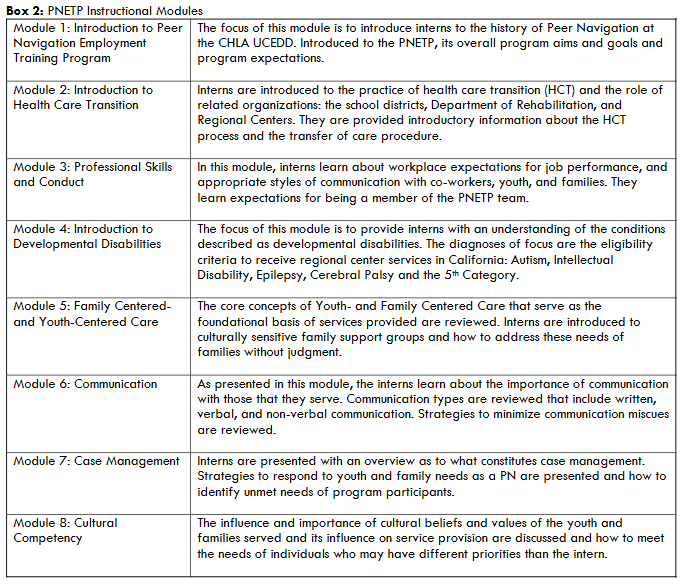
Module 1: Introduction to Peer Navigation Employment Training Program
The focus of this module is to introduce interns to the history of Peer Navigation at the CHLA UCEDD. Introduced to the PNETP, its overall program aims and goals and program expectations.
Module 2: Introduction to Health Care Transition
Interns are introduced to the practice of health care transition (HCT) and the role of related organizations: the school districts, Department of Rehabilitation, and Regional Centers. They are provided introductory information about the HCT process and the transfer of care procedure.
Module 3: Professional Skills and Conduct
In this module, interns learn about workplace expectations for job performance, and appropriate styles of communication with co-workers, youth, and families. They learn expectations for being a member of the PNETP team.
Module 4: Introduction to Developmental Disabilities
The focus of this module is to provide interns with an understanding of the conditions described as developmental disabilities. The diagnoses of focus are the eligibility criteria to receive regional center services in California: Autism, Intellectual Disability, Epilepsy, Cerebral Palsy and the 5th Category.
Module 5: Family Centered-and Youth-Centered Care
The core concepts of Youth- and Family Centered Care that serve as the foundational basis of services provided are reviewed. Interns are introduced to culturally sensitive family support groups and how to address these needs of families without judgment.
Module 6: Communication
As presented in this module, the interns learn about the importance of communication with those that they serve. Communication types are reviewed that include written, verbal, and non-verbal communication. Strategies to minimize communication miscues are reviewed.
Module 7: Case Management
Interns are presented with an overview as to what constitutes case management. Strategies to respond to youth and family needs as a PN are presented and how to identify unmet needs of program participants.
Module 8: Cultural Competency
The influence and importance of cultural beliefs and values of the youth and families served and its influence on service provision are discussed and how to meet the needs of individuals who may have different priorities than the intern.
Module 9: Health Care Transition: Part I
An overview of the health care transition process that involves the transfer of care to adult-focused providers is presented. Tools used to assess transition readiness and outcomes associated with the health care transition process are reviewed.
Module 10: Health Care Transition: Part 2
In this module, interns are provided with more in-depth information about the HCT process such as how to find medical information, insurance card information and common key terms they will encounter when working with patients. Interns learn to complete a HCT.
Module 11: Health Care Transition: Part 3
Information provided in this module focuses on the gaining an understanding how healthcare can impact all areas of an individual’s life and their personal goals and applying that understanding to youth and family interactions. Interns are provided examples and opportunities to provide to program participants to assume more autonomy in their healthcare during the health care transition process.
Module 12: Regional Centers
The regional center network, composed of 21 regional centers is the California IDD service system providing life span services/programs. Information is provided about eligibility for Regional Center Services, the history of the Lanterman Act and the establishment of Regional Centers. Interns are given strategies to request specific Regional Center services, documentation needed to request services, and how to navigate service denials.
Module 13: Social, Recreational and Community Integration
The relevance of addressing social recreation and community integration as a component of peer navigation to foster more inclusive activities are presented. Understanding the difference between being in society and being a member of society is discussed.
Module 14: Employment Services and Supports
Interns are provided with information as to the rights and protections individuals have when seeking employment and being employed. Employment resources available for youth and young adults are reviewed.
Module 15: Education Supports
Review of the postsecondary educational programs to support individuals with disabilities with financial assistance, access to accommodations, and the differences between high school and postsecondary education accommodations are provided.
Module 16: In Home Support Services (IHSS)
Interns learn about the IHSS program and what assistance can be provided to families. Type of assistance, program eligibility, and the process to apply for and receive IHSS is reviewed.
Module 17: Independent Living Services
An overview of the services and supports available for individuals with disabilities to live independently in the community and home of their choosing is provided. Interns are informed about the differences between different living services and how to request the appropriate living service.
Module 18: Person-centered Planning
The Person-centered Planning approach and person-centered thinking to providing services and resources as a peer navigator is presented. Introduction to types of person-centered tools is provided and how to progress towards goals is monitored in PNETP.
6.2. GROUP INSTRUCTION.
The scheduling format for training PNETP interns incorporates group instruction. Group instruction involves the interns getting together with the peer navigator training instructor and often the job coach. It is during these sessions; discussion is held to facilitate exchange between the interns about what they are learning based upon the person-centered plans that they are developing and implementing with the YYA with IDD in their caseloads as each will be characteristically different based upon the PCP individualized needs. During these “check-ins” interns meet in a small group and will provide a quick summary of what they are working on for each of their cases (without sharing private health information [PHI] and when they intend to follow up with their program participant. If an intern puzzled by a case, the group can brainstorm together how to overcome a barrier. Depending on the community of choice of YYA with IDD served, the local resources will differ, yet it is an opportunity for each of the interns to learn about other available resources in the community. Additionally, the HCT needs of the interns’ YYA with IDD caseloads will have variation pertaining to an array of different community-based resources (i.e. job training and placement agencies, recreational and social groups) that provide other opportunities for learning new information to enhance peer navigation knowledge and skills. Group instruction provides opportunities for development of the “soft skills” associated with workplace behaviors. These soft skills include respectfully listening to the intern’s discussion about their caseload, supportive and encouraging comments as discussion ensues and thoughtful recommendations are shared.
6.3. 1 TO 1 COACHING.
Both the job coach and PNETP training coordinator meet individually with the peer navigator interns to provide 1 to 1 coaching, although each trainer’s coaching will have a different focus. In 1 to 1 sessions with interns, the job coach provides feedback on workplace conduct such as communication with co-workers and supervisors as working in a health care setting is a new experience for the interns. The job coach assists interns in acclimating to a new work environment as it pertains to policies and job expectations such as dress code and providing guidance with online employee orientation program. As well, the job coach will coordinate feedback in 1 to 1 sessions based upon conferring with the PNETP training coordinator about the job coach’s observations noted during the PNETP training.
6.4. JOB SHADOWING.
Job shadowing has been a long-standing practice that has been used to assist individuals with IDD to obtain the skills and knowledge to learn necessary role responsibilities of an employment position. The job shadowing experiences are scheduled at least once during their PNETP training. Interns shadow CHLA employees involved with providing navigation, including parent navigators and health care transition services. It is during these experiences they observe the demonstration of services by a provider that they will eventually learn to do. Job shadowing enables the interns to observe provider role modeling as it pertains to communicating with YYA with IDD/chronic conditions and their families and contextualize what they learned in the modules in practice. Interns are encouraged to ask questions of those that they shadow.
6.5. CLINICAL PRACTICE.
Once the didactic portion has been completed, interns apply what has been learned to YYA with IDD and families referred to PNETP. Their initial contact begins with a review of the reasons for the referral, whether it is from the Center for Healthy Adolescent Transition (CHAT) program or primary care clinic. The CHLA CHAT program is a hospital-wide HCT program that prepares patients for transition and referrals for adult-focused care for specialty care centers without transition-specific programs. The PNETP intake involves a comprehensive assessment of HCT needs that serves as the basis for the person-centered plan as demonstrated by these areas of assessment: a) patient information pertaining to diagnosis, demographics, regional center enrollment; b) health care information including current primary and specialty care providers, insurance plan, medications, daily condition management tasks; c) educational information related to type of educational program that the YYA is currently enrolled in, access to IEP/504 Plan, provision of accommodations, academic aspirations; d) employment data that includes access to Department of Rehabilitation, current/previous employment, needs for accommodation, transportation use; e) independent living situation related to current and desired living arrangements, status of independent living skills, previous living skills training; and f) social recreational information consisting of interests and hobbies, social network, extracurricular activities. This initial intake provides the basis for development of the Person-centered Plan (PCP). The Person-centered Plan, generated in consultation with YYA with IDD and family members is formulated using different PCP templates as it applies to each area of HCT needs and the best options for the program participant to plan their future goals. After goals are defined, next steps, and resources needed, interns track progress towards transfer of care and transition to adulthood with a summary sheet and cross off steps as they are completed. Goals are identified together with the actions needed to achieve goals. The PCP process is continuous with ongoing contact with YYA with IDD and family typically on a weekly basis that may involve several contacts during the week. During the PCP’s implementation, new needs may be identified requiring revisions of the original PCP. Cases are closed once the PCP goals are obtained or the family and participant are confident in transfer of their services and transition options.
6.6. Conferencing.
Each week conference time is scheduled for one hour for each with the clinical faculty members of the project (C.B., C.M.) to review the status of their service activities with the assigned youths of their caseload. To effect optimal supervision, interns present their cases using a structured presentation outline. These experiences enable interns to consult with PNETP staff for additional input and insights designed to generate other options/recommendations for the PCP. For example, project staff may provide specific recommendations for the transfer of care to adult-focused providers given previous experiences with providers’ referrals. Conferencing template provides interns with a guide for sharing information about the youths they are presenting that includes the following items for presentation: current diagnoses, medications, YYA with IDD identified-needs, barriers to achieving PCP goals, and conferencing recommendations.
7. Peer Navigators Process and Progress to Date.
Currently, two Peer Navigators have completed PNETP; three are enrolled in PNTEP and four are scheduled to begin in early 2025. The goal of PNETP is to enroll 16 Peer Navigators over the next two years having provided services to approximately 160 YYA with IDD. An important outcome of PNETP is to facilitate the employment of Peer Navigators in health or social services settings as well as provide transition support for transition-aged YYA to facilitate their transfer of care to adult-focused health care providers and assist with the transition to adulthood.
7.1. RECRUITMENT AND SCREENING PROCESS.
Peer navigator interns have been recruited from the following agencies/organizations: regional centers (6), school districts (3), and job training agencies (8) in our catchment area wherein CHLA UCEDD is located. Box 3 contains the Peer Navigator Expectations included in the recruitment mailers sent to the network. Eligible candidates are referred to PNETP by affiliating agencies for team review. For example, the regional centers will perform an initial screening to review expectations and details about the PIP portion of the PNETP program. If needed, a transportation plan will be made to facilitate access to PNETP. PNETP screening process involves a phone screening interview with the applicant to determine their interest and skill set (i.e., computer skills that include use of software programs and accessing the internet). Following initial screening, applicants are then scheduled for a formal interview with the project team. Applicants are also asked to provide references for additional screening review. For applicants who are accepted into the program, the onboarding process begins.
Box 3: Expectations of Peer Navigator Interns
- Have employment goal(s) related to working in Health Care/Social Services
- Receives Adult Services from their Regional Center and eligible for the Paid Internship Program (PIP)
- Able to transport self to and from a physical work location as needed.
- Able to safely navigate an office building after an orientation with minimal supervision.
- Have an understanding of office etiquette.
- Work professionally with others on a team.
- Complete assignments.
- Familiar with technological applications such as Microsoft office and email.
- Desire to perform well and complete work in a timely manner.
- Maintain a caseload of at least 10 individuals at any one time.
- Work for at least 20 hours per week consistently.
7.2. TRAINING COMPETENCIES
Each of the training modules contains behavioral objectives that interns are expected to achieve. These competences include learning to provide resource information, service coordination and referrals as it pertains to the following transition and adult-focused areas of service need:
- Transfer of care from pediatric to adult-focused health care
- Postsecondary education and training
- Employment resources for job training and placement
- Community-based resources for independent living and community integration
These competencies are achieved through the training program instructional units previously described. Examples of the guided learning activities that enable interns’ acquisition of training competencies are presented in Box 4.
Box 4: Interns Performance Activities as Peer Navigators
- Attending an Individual Program Plan (IPP) meeting with an individual and their Service Coordinator to advocate for Services needed to attain IPP goals.
- Assisting an individual with filling out a job application, writing, and submitting a resume and cover letter.
- Brainstorm with an individual different steps to take to achieve a career goal, such as educational requirements and application process and then completing smaller steps towards the goal with the Program Participant.
- Following up with Program Participants weekly to check in, offer next steps, and receive a status report.
7.3. PEER NAVIGATOR EMPLOYMENT TRAINING PROGRAM EVALUATION.
Evaluation of PNETP involves several different strategies. All PNETP interns are administered the PNETP pre and posttests. These tests are administered at the beginning and at the conclusion of PNETP to assess the acquisition of learning that has been achieved in the training program. These items are based upon the behavioral objectives of each of the modules. Throughout PNETP, interns are provided ongoing feedback about their acquisition of knowledge and skills to become a peer navigator. Additionally, the PNETP team meets on a weekly basis to review the training status of PNETP interns in terms of progress with acquiring competencies and possible needs for remediation. Our team is in the process of conducting a qualitative study with recipients of PNETP to explore their satisfaction with services received and their own identified HCT outcomes. We will be conducting virtual/in person interviews to gather the following data: a) analyze if there is potential to facilitate the transition process, reduce the amount of discontinued services with the IPNEP and PNETP; b) explore the experience and satisfaction with the peer navigator services received by transition-aged young adults with IDD; and c) gather information on the peer navigator services received by transition-aged young adults with IDD. Eventually, it is our intent to use more robust methods to examine the effectiveness of this program as it pertains to employment and HCT outcomes.
8. Discussion
As has been presented in this paper, the PNETP is an employment pathway program designed to train individuals with IDD to learn the skills and knowledge to function as a peer navigator in healthcare or social services agencies/organizations. PNETP is both an educational and service innovation designed to achieve two separate but interrelated outcomes: a) develop and implement employment opportunities in competitive employment settings for individuals with IDD; and b) provide HCT services to underserved YYA with IDD and their families.
8.1. EDUCATIONAL ADJUSTMENTS AND IMPLICATIONS.
Since this program was first initiated in 2023, the training modules have undergone ongoing revisions as our program progresses forward with our dual aims of training interns to become Peer Navigators and provision of HCT services to transition-aged youth and young adults. Revisions with the modules are generated based upon the training input of the interns who share with the training team their requests for additional information and/or clarification of content presented. Other revision recommendations have been generated by members of the PNETP Advisory Committee. As a result, other modules have been added as a means of enriching the content provided to interns. As an example, modules on conservatorship and alternatives to conservatorship, including supportive decision making were added to the modules given the repeated intern encounters with families and youth who needed information on these topics. The content of the PNETP has focused on the following areas of emphasis that included communication skills, service coordination/case management, referrals to transition/adult-focused community-based agencies involved with adult-focused health care, education, employment and community living, similar in part or in full to other types of peer navigation programs reported. Some studies have been published focused on the provision of navigation services for transition-aged youth. For example, a recently reported peer navigator project focused on the provision of transition services to youth with sickle cell disease using CHW; another project reported about peer navigators’ (social workers) provision of HCT services to YYA with chronic conditions. Researchers recently reported perspectives offered by divergent groups of consumers, parents and providers about mental health services provided by peer navigators for transition aged youth. The PNETP is unique as it is a service-training HCT model addressing both the service and training needs of the IDD community. The PNETP is composed of similar training elements as reported in other peer navigator programs; the PNETP is approximately 500 hours in length, considerably longer than has been noted in other peer navigation programs, which have been reported from a few hours in length to several weeks. Another feature of PNETP, which is distinctly different from other reported navigation programs is the recruitment of individuals with the IDD lived experience and with limited to no previous experience in health care. The PNETP implementation was made possible with the innovative use of the PIP program funded by the California Department of Developmental Services and partnership with the regional center.
8.2. PRACTICE ADJUSTMENTS AND IMPLICATIONS.
This project introduces an innovative service-training model in health care and characteristically different than the typical employment options for the IDD population that have been focused on environmental services, grounds cleaning and maintenance occupations and administrative support. Unlike other employment pathways reported in healthcare settings, this training program is focused on the provision of direct services and supports to YYA with IDD and their families. Although, the service focus of PNETP is on the provision of health care transition services, this training-service model could be adapted for other populations in need for peer navigation services such as families whose children have complex health care needs, parents whose infants and toddlers receive early intervention services and older age groups who have ongoing needs for services such as the elderly. Peer Navigator programs have shown promising success with a variety of people, such as those with mental health conditions, reintegrating into the community after a jail sentence, HIV health outcomes, and community living outcomes for people with disabilities. The PNETP model is based upon the community health worker model and has the potential of being adapted in health care and social service settings as a more economically feasible model of care for health care transition planning.
8.3. RESEARCH ADJUSTMENTS AND IMPLICATIONS.
Scant research exists pertaining to the use of the Peer Navigation model with YYA with IDD and their families and indeed with any population of YYA with childhood acquired chronic conditions. Most papers published examining peer navigator programs have been descriptive studies; few quantitative papers have been published. Additionally, few peer navigator-focused studies have been conducted with pediatric/adolescent populations. To date, few navigation studies have been reported focused on adolescents/young adults. As reported, when this project was initiated, qualitative data were gathered from 11 parents as to their perspectives about the utility of this project. To date, parents’ input on the feasibility of and benefits accrued from receiving HCT peer navigation services for the YYA with IDD has not been reported.
Currently several research efforts are underway and planned. Follow-up data are currently being collected from YYA who have received PN services. Interview data will be collected as to their satisfaction with services received, helpfulness of services received, and outcomes of services received. Other planned investigations include analysis of type of referrals made and employment outcomes of peer navigators.
8.4 PEER NAVIGATORS PROGRESS AND OUTCOMES TO DATE.
Currently, two PNs have completed PNETP; three are enrolled in PNTEP and four are scheduled to begin in early 2025. The goal of PNETP is to enroll 16 Peer Navigators over the next two years having provided services to approximately 160 YYA with IDD. An important outcome of PNETP is to facilitate the employment of Peer Navigators in health or social services settings as well as provide support for transition-aged YYA to facilitate their transfer of care to adult-focused health care providers and assist with the transition to adulthood. At this time, one of our PNs from the first cohort had obtained full-time employment in social services, working with transition-aged youth.
9. Conclusion.
A service-training model, the PNETP has been developed and implemented to create an employment pathway for individuals with IDD in health care and social services settings and provide HCT to YYA with IDD to facilitate their transfer of care to adult-focused providers and transition to adulthood. This innovative model of care is unique both as a navigation and HCT model that has potential effect new opportunities for employment and services for the IDD community.
References
- American Public Health Association. Community Health Worker Definition. Accessed on December 1, 2024 at https://apha.org/apha-communities/member-sections/community-health-workers#:~:text=A%20community%20health%20worker%20is,understanding%20of%20the%20community%20served.
- Betz CL, Ferris ME, Woodward JF, Okumura MJ, Jan S, Wood DL. The health care transition research consortium health care transition model: a framework for research and practice. J Pediatr Rehabil Med. 2014;7(1):3-15. doi:10.3233/PRM-140277
- Cromwell EA, Ostrenga JS, Todd JV, et al. Cystic fibrosis prevalence in the United States and participation in the Cystic Fibrosis Foundation Patient Registry in 2020. J Cyst Fibros. 2023;22(3):436–442.
- National Heart,Lung and Blood Disease What Is Sickle Cell Disease? Accessed June 3, 2024 from: <https://www.nhlbi.nih.gov/health/sickle-cell-disease#:~:text=The%20condition%20affects%20more%20than,born%20with%20sickle%20cell%20trait. April 22, 2024.
- Cheak-Zamora NC, Farmer JE, Mayfield WA, et al. Health care transition services for youth with autism spectrum disorders. Rehabil Psychol. 2014;59(3):340–348. https://doi.org/10.1037/a0036725.
- Cheak-Zamora NC, Yang X, Farmer JE, Clark M. Disparities in transition planning for youth with autism spectrum disorder. Pediatrics. 2013;131(3):447–454. https://doi.org/10.1542/peds.2012-1572.
- Zablotsky Benjamin, et al. Health care transition planning among youth with ASD and other mental, behavioral, and developmental disorders. Matern Child Health J. 2020;24:796–804. https://doi.org/10.1016/j.jcf.2023.02.009.
- Zablotsky B, Black LI, Maenner MJ, et al. Prevalence and Trends of Developmental Disabilities among Children in the United States: 2009-2017. Pediatrics. 2019;144(4):e20190811. doi:10.1542/peds.2019-0811
- Zablotsky B, Ng AE, Black LI, Blumberg SJ. Diagnosed Developmental Disabilities in Children Aged 3–17 Years: United States, 2019–2021. NCHS Data Brief, no 473. Hyattsville, MD: National Center for Health Statistics.; 2023. https://doi.org/10.15620/cdc:129520.
- Leeb RT, Danielson ML, Bitsko RH, et al. Support for Transition from Adolescent to Adult Health Care Among Adolescents With and Without Mental, Behavioral, and Developmental Disorders – United States, 2016-2017 [published correction appears in MMWR Morb Mortal Wkly Rep. 2020 Oct 30;69(43):1611. doi: 10.15585/mmwr.mm6943a6]. MMWR Morb Mortal Wkly Rep. 2020;69(34):1156-1160. Published 2020 Aug 28. doi:10.15585/mmwr.mm6934a2
- Walsh C, Jones B, Schonwald A. Health Care Transition planning among adolescents with autism spectrum disorder. J Autism Dev Disord. 2017;47(4):980–991. https://doi.org/10.1007/s10803-016-3020-1. PMID: 28078534.
- Child and Adolescent Health Measurement Initiative. NPM 12: Transition to adult health care, CSHCN age 12-17 years, 2020-2021 National Child Health Survey, Data Resource Center for Child and Adolescent Health supported by the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB). Retrieved [02/20/2023] from []
- Newman L, Wagner M, Knokey AM, Marder C, Nagle K, Shaver D, Wei X, Cameto R, Contreras E, Ferguson K, Greene S, Schwarting M. The Post-High School Outcomes of Young Adults with Disabilities up to 8 Years After High School. A Report from the National Longitudinal Transition Study-2 (NLTS2) (NCSER 2011-3005). 2011; Menlo Park, CA: SRI International.
- Oakes, L R, Nichols TR, Schleien SJ, Strack RW, & Milroy JJ Exploring Inclusion of College Students with IDD in Campus Recreation Through the Lens of Recreation Departments’ Organizational Level Stakeholders. Recreational Sports Journal. 2021; 45(1), 34-51. https://doi.org/10.1177/1558866120982594
- Grigal M, Dukes LL III, Walker Z. Advancing Access to Higher Education for Students with Intellectual Disability in the United States. Disabilities. 2021; 1(4):438-449. https://doi.org/10.3390/disabilities1040030
- Erickson, W., Lee, C., & von Schrader, S. 2018 Disability Status Report: United States. 2020. Ithaca, NY: Cornell University Yang-Tan Institute on Employment and Disability (YTI).
- National Disability Institute Financial Inequality: Disability, Race and Poverty in America, Goodman N,,Morris M, Boston K Accessed on 12.10.2024 from: https://www.nationaldisabilityinstitute.org/wp-content/uploads/2019/02/disability-race-poverty-in-america.pdf
- Siperstein GN, Parker RC, Drascher M. National snapshot of adults with intellectual disabilities in the labor force. Journal of Vocational Rehabilitation. 2013;39(3):157-165. doi:10.3233/JVR-130658
- California Department of Developmental Services, National Core Indicators Accessed on December 10, 2024 from https://www.dds.ca.gov/rc/nci/
- Ahonkhai AA, Kuti KM, Hirschhorn LR, et al. Successful Implementation Strategies in iCARE Nigeria-A Pilot Intervention with Text Message Reminders and Peer Navigation for Youth Living with HIV. Trop Med Infect Dis. 2023;8(11):498. Published 2023 Nov 16. doi:10.3390/tropicalmed8110498
- Cunningham WE, Weiss RE, Nakazono T, et al. Effectiveness of a Peer Navigation Intervention to Sustain Viral Suppression Among HIV-Positive Men and Transgender Women Released From Jail: The LINK LA Randomized Clinical Trial. JAMA Intern Med. 2018;178(4):542-553. doi:10.1001/jamainternmed.2018.0150
- Freeman HP, Rodriguez RL. History and principles of patient navigation. Cancer. 2011;117(15 Suppl):3539-3542. doi:10.1002/cncr.26262
- Hailemariam M, Weinstock LM, Johnson JE. Peer navigation for individuals with serious mental illness leaving jail: a pilot randomized trial study protocol. Pilot Feasibility Stud. 2020;6:114. Published 2020 Aug 17. doi:10.1186/s40814-020-00659-1
- Kelly E, Fulginiti A, Pahwa R, Tallen L, Duan L, Brekke JS. A pilot test of a peer navigator intervention for improving the health of individuals with serious mental illness. Community Ment Health J. 2014;50(4):435-446. doi:10.1007/s10597-013-9616-4
- Marsack-Topolewski C, Milberger S, Janks E, Anderson N, Bray M, Samuel PS. Evaluation of peer-mediated systems navigation for ageing families of individuals with developmental disabilities. J Intellect Disabil Res. 2023;67(5):462-474. doi:10.1111/jir.13024
- Littlewood K, Cooper L, Rosenthal M, Averett P, Yelick A, Bennett R. Children’s Home Network’s Kinship Navigator Program: Connecting to Concrete Resources Through Peer-to-Peer Kinship Navigation Services. Families in Society, 2024;105(1), 139-151. https://doi.org/10.1177/10443894231196283
- Pagkas-Bather J, Jaramillo J, Henry J, et al. What’s PrEP?: peer navigator acceptability among minority MSM in Washington. BMC Public Health. 2020;20(1):248. Published 2020 Feb 18. doi:10.1186/s12889-020-8325-5
- Rocha-Jiménez T, Pitpitan EV, Cazares R, Smith LR. “He is the Same as Me”: Key Populations’ Acceptability and Experience of a Community-Based Peer Navigator Intervention to Support Engagement in HIV Care in Tijuana, Mexico. AIDS Patient Care STDS. 2021;35(11):449-456. doi:10.1089/apc.2021.0069
- Kangovi S, Mitra N, Norton L, et al. Effect of Community Health Worker Support on Clinical Outcomes of Low-Income Patients Across Primary Care Facilities: A Randomized Clinical Trial. JAMA Intern Med. 2018;178(12):1635-1643. doi:10.1001/jamainternmed.2018.4630
- World Health Organization. Constitution. Accessed October 25, 2024 from: https://www.who.int/about/governance/constitution
- Bureau of Labor Statistics, U.S. Department of Labor, Occupational Outlook Handbook, Community Health Workers, at https://www.bls.gov/ooh/community-and-social-service/community-health-workers.htm (visited December 15, 2024). Thursday, August 29, 2024
- Herman AA. Community Health Workers and Integrated Primary Health Care Teams in the 21st Century. Journal of Ambulatory Care Management. 2011; 34 (4): 354-361. doi: 10.1097/JAC.0b013e31822cbcd0.
- Carter N, Valaitis RK, Lam A, Feather J, Nicholl J, Cleghorn L. Navigation delivery models and roles of navigators in primary care: a scoping literature review. BMC Health Serv Res. 2018;18(1):96. Published 2018 Feb 8. doi:10.1186/s12913-018-2889-0
- Valaitis RK, Carter N, Lam A, Nicholl J, Feather J, Cleghorn L. Implementation and maintenance of patient navigation programs linking primary care with community-based health and social services: a scoping literature review. BMC Health Serv Res. 2017;17(1):116. Published 2017 Feb 6. doi:10.1186/s12913-017-2046-1
- Gale, N. K., Heath, G., Cameron, E., Rashid, S., & Redwood, S. (2013). Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC medical research methodology, 13, 117. https://doi.org/10.1186/1471-2288-13-117
- California Department of Developmental Services. Current initiatives and efforts to advance employment for Californians with intellectual/developmental disabilities (ID/DD). Paid Internship Programs.Accessed on December 10, 2024 from: https://www.dds.ca.gov/wp-content/uploads/2021/12/EmploymentWG_Handout_12132021.pdf
- Betz CL, Ferris ME, Woodward JF, Okumura MJ, Jan S, Wood DL. The health care transition research consortium health care transition model: a framework for research and practice. J Pediatr Rehabil Med. 2014;7(1):3-15. doi:10.3233/PRM-140277
- Mirzaian CB, Solomon O, Setaghiyan H, et al. Enhancing access to early intervention by including parent navigators with lived experience in a pediatric medical home. Fam Syst Health. 2024;42(3):405-416. doi:10.1037/fsh0000864
- Iverson E, Sayegh CS, Porter C, Tanaka D, Williams R, Reflections on developing a hospital-wide health care transition program, Health Care Transitions, 2025; 3, 100090, https://doi.org/10.1016/j.hctj.2024.100090.
- Patton M, San Martin-Feeney D, Allemang B, Punjwani Z, Samborn S, Pfister K, Ryan L, Mackie AS, Samuel S, Dimitropoulos G, What skills do adolescents and young adults desire as they prepare for adult health care?, Health Care Transitions, 2024; 2, 100049, https://doi.org/10.1016/j.hctj.2024.100049.
- Belton TD, Wu K, Steinway CM, Trachtenberg SW, Tchume-Johnson T, Shilly S, Austin T, Luma S, Smith K, Smith-Whitley K, Rubin D, Jan S, Training young adults as community health workers specializing in pediatric to adult health care transition to support emerging adults with sickle cell disease, Health Care Transitions, 2024; 2, 100050, https://doi.org/10.1016/j.hctj.2024.100050.
- Markoulakis R, Weingust S, Foot J, Levitt A, The family navigation project: An innovation in working with families to match mental health services with their youth’s needs. Can J Commun Ment Health, 2016; 35, 63-66. https://doi.org/10.7870/cjcmh-2016-026
- Markoulakis R, Cader H, Wong K, Kodeeswaran S, Addison T, Walsh C, Charles J, Cheung M, Sur D, Willis D, Levitt A, The role of navigation services in supporting mental health and addictions care transitions: A qualitative exploration of perspectives from transitional-aged youth, family, and service providers (part 2), Health Care Transitions; 2025, 3, 100082, https://doi.org/10.1016/j.hctj.2024.100082.