

Perceptions of Hospital Food in Elderly Dysphagia Patients
Perception of elderly people with swallowing disorders on food served in hospital: an exploratory study using eye tracker and emotional face reader methodology to identify challenges and opportunities
R. Baixauli¹, A. Tarrega¹, M. Bolivar-Prados²˒³, Marta Cera²˒³, P. Clavé²˒³, L. Laguna¹*
- Institute of Agrochemistry and Food Technology (IATA, CSIC), Paterna, Valencia (Spain)
- Gastrointestinal Physiology Laboratory, Hospital de Mataró, Universitat Autònoma de Barcelona
- Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (Ciberehd), Barcelona, Spain
OPEN ACCESS
PUBLISHED 31 August 2025
CITATION Baixauli, R., et al., 2025. Perception of elderly people with swallowing disorders on food served in hospital: an exploratory study using eye tracker and emotional face reader methodology to identify challenges and opportunities Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6793
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6793
ISSN 2375-1924
ABSTRACT
Background: Individuals afflicted with dysphagia must modify the consistency of their diet, as there is no other viable option. The patient’s acceptance of the diet may not have been given enough attention. This study examined the use of an implicit method to ascertain the perceptions of consumers with dysphagia regarding diets that vary in consistency (pureed or minced and moist) and adaptation (adapted for enhanced sensory experience or base diet).
Methods: A total of 14 participants diagnosed with dysphagia (n = 14) were presented with eight slides of hospital food trays and were asked to indicate whether they liked the food on display by responding yes or no. Participants gaze behavior was recorded using an eye-tracking technique. Subsequently, the participants viewed 16 individual dishes, indicating their level of liking, intention to consume food, and whether they believed it to be safe (answering yes or no). The participants’ facial expressions were recorded throughout the experiment and the researchers assessed six discrete emotions.
Results: Regarding gaze behavior, the results indicated that the number of fixations, time to first fixation, and duration of first fixation were higher when participants responded in the negative than when they responded affirmatively to the question regarding their liking of the full tray. This discrepancy is likely because of the difficulty in recognizing food items. Pupil size was the primary factor influencing liking response when a classification tree was used. Regarding facial emotions, negative emotions associated with the adapted presentation of dishes were less prevalent than those observed in the base versions.
Conclusions: This study represents a preliminary investigation into implicit methods with participants with dysphagia in a hospital setting, aiming to elucidate the relationship between food liking and unconscious food liking.
Keywords: Swallowing disorders, eye-tracking, face reader, liking
1. Introduction
For various medical reasons, medical professionals may prescribe diets that include different food restrictions. Previous studies have focused on examining the adequacy of nutritional requirements in relation to actual food intake. However, the hedonic aspect has not yet been overlooked. In individuals with dysphagia, it is essential to modify food texture to ensure safe swallowing. The recommended diet includes pureed foods, jellies, mousses, porridge, and soft foods of varying consistencies.
There is a paucity of studies investigating the preferences of patients with swallowing disorders. Furthermore, most studies have concentrated on developing strategies for improvement rather than on an in-depth examination of the current situation. For example, Okkels et al. inquired about food preferences between meals to gain insight into the design of snack food for the elderly. In another study, Pouyet et al. proposed flavor enhancement as a strategy for improving liking. Other studies have concentrated on the manner of serving food or have attempted to alter the form or shape of the food. Ultimately, the perceptions of patients with dysphagia regarding the food they receive remain unclear. However, older adults with dysphagia may encounter difficulties verbally expressing their preferences. The reported preferences and opinions on food do not accurately reflect the actual preferences and opinions of this age group.
Another issue is the constant risk of food aspiration in individuals with dysphagia. To achieve this, it would be optimal to use only visual stimuli for an initial sensory assessment, eliminating the potential for risk. Eye-tracking has been used to examine the relationship between food selection and consumer attention. This observational technique allows the study of where and how an individual is looking. It is a noninvasive method that provides greater insight into consumer behavior. In addition, food can evoke emotional responses that influence an individual’s eating behavior, including food choice and intake. Baranda et al. used both explicit (questionnaire-like) and implicit methods (face reader) to investigate the influence of food shape on elderly consumers. Their findings revealed that despite no significant differences in liking, the products elicited disparate emotional responses, underscoring the necessity to consider these factors.
The objective of this study was to explore the use of implicit methodology to determine the opinions of dysphagia consumers regarding the food they receive in a hospital setting. This will be done by considering two types of diet for different degrees of dysphagia and two types of adaptation (base diet and triple adapted diet, as described by Costa et al.).
2. Material and methods
2.1. PARTICIPANTS
Fourteen participants were recruited from the Gastrointestinal Physiology Unit of the Hospital de Mataró (Catalonia, Spain). The inclusion criteria were: a diagnosis of swallowing disorders; an age of over 65 years; and current or past hospitalisation with a prescribed dysphagia diet. The participants were divided into two groups, with seven women and seven men in each group. The average age of participants was 82 years. Half of the participants were instructed to consume a thick-pureed diet (Texture C, according to the British Dietetic Association, BDA), while the remaining seven were provided with a fork-mashable diet (Texture E, according to the BDA). Outpatients from the hospital were invited to attend a 1-hour session. Inpatients from the hospital were invited to participate in the study during the hospitalization period. Participants and their accompanying individuals were provided with a comprehensive explanation of the study’s objectives and procedures. If they accepted, they were invited to sign the consent form (code 63/22, Ethics Committee of Consorci Sanitari del Maresme). All participants were patients at Mataró Hospital. The principal inclusion criteria were as follows: the subject must be aged 65 or above, have demonstrated swallowing impairments as determined by the Volume-Viscosity Test, possess the cognitive capacity to respond to the questions posed, and accept participation by signing the informed consent form. The Ethics Committee of Consorci Sanitari del Maresme (code 63/22) approved the study protocol and informed consent forms.
2.2. STIMULI (FOOD TRAYS) AND PRESENTATION
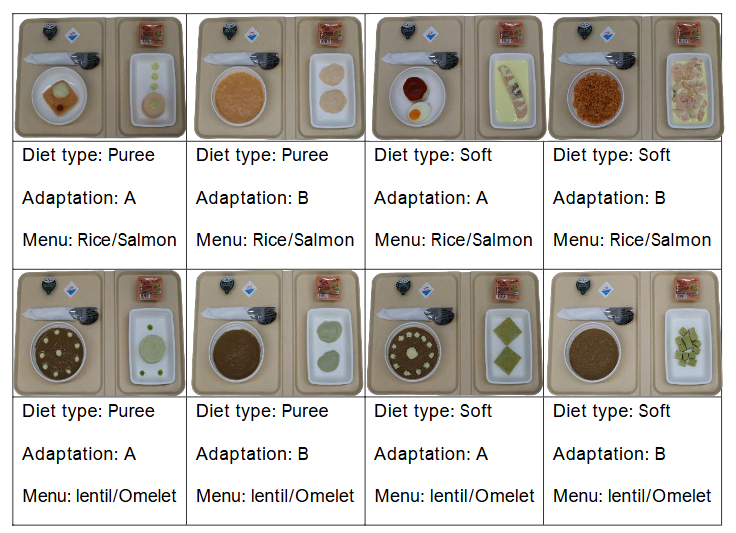
Two dietary regimens were used: a pureed diet (Texture C) and a soft fork-mashable diet (Texture E). One of the two types was adapted (marked with the letter A) in accordance with prior research findings on sensory appeal and safety. The other was maintained in its current form, as served in the hospital (marked with the letter B). Two menus were presented for consideration: one featuring rice and salmon, and the other featuring a lentil and courgette omelet. Eight complete trays (comprising the first course, main course, and dessert) from the hospital were presented to the participants, as illustrated in Figure 1.
2.3. PROCEDURE
Participants were positioned in front of a computer screen. The initial presentation on the screen depicted a hospital tray completed in two dishes: dessert, cutlery, and seasoning. The accompanying text read, Do you think you will like it? and included two button options, labeled YES and NO, immediately below the question. Subsequently, the starter was displayed on three consecutive screens, accompanied by the question, Do you think you will like it? and Do you think you will eat it? In addition, participants were asked whether they believed the starter was safe for consumption. The response was indicated via two buttons below the question YES and NO. Subsequently, the same set of questions was posed regarding the main dish. Eight full trays and sixteen individual dishes (comprising eight starters and eight mains) were evaluated. In total, 56 images were presented in eight blocks, with seven images per block and a randomized presentation between blocks among the participants. The images were presented, and the answers were recorded using Tobii Pro Fusion software.
2.4. EYE-TRACKER RECORDINGS
The eye-tracking procedure was conducted with the aid of an eye-tracker bar (Tobii Pro Fusion) at the base of a 24-inch display screen. Before commencing the test, a calibration procedure was performed to ascertain the position of the pupils. The gaze was recorded at a frequency of 250 Hz. The data obtained from the eye tracker were subsequently analyzed using the Tobii Pro Lab. In analyzing the eye-tracker data for the full tray, the eye movement data were analyzed based on the defined areas of interest (AOI), which included the first dish, the second dish, and the remaining elements. For each AOI image, the number of fixations, total fixation duration, time to first fixation, fixation duration, and duration of first fixation were recorded.
2.5. FACE READER RECORDINGS
The procedure was recorded using a high-definition 1080p LifeCam Studio webcam (Microsoft) and Face Reader v.09 software (Noldus Information Technology, Wageningen, Netherlands). Upon arrival, the participants were instructed to gaze at a square on a white background screen for facial calibration. Six basic emotions (happy, angry, surprise, sadness, fear, and disgust) and a neutral state were coded on a scale from 0 (not present at all) to 1 (maximum intensity of the fitted model).
2.6. DATA ANALYSIS
To investigate the impact of affirmative and negative responses (YES/NO) to the question if they would like to eat the food of the tray observed on eye-tracker parameters, a t-test was used. A classification tree analysis was used to develop a model that could explain the participants’ decisions about the trays (i.e., whether they liked them or not) based on eye-tracker parameters. The dataset used in this analysis comprised 112 cases. A three-way ANOVA was used to investigate the influence of patient, question (i.e., whether the subject believed they would like, eat, or find the starter safe) and election (i.e., whether the subject answered YES or NO) on the maximum values of the facial expression patterns (happy, angry, surprised, sad, afraid, or disgusted). All analyses were conducted using XLSTAT 2019.3.2 (Addinsoft, Paris, France).
3. Results
3.1. VISUAL RESPONSE TO FULL TRAY (TWO DISHES) OF THE DIFFERENT DIETS
The initial elements that capture attention in the tray are listed in Table 1. As can be observed, the gaze was nearly equally distributed between the two dishes, with a slight predominance for the starter dish on the left side of the tray. This can be attributed to the influence of reading and writing directions (left to right).
| Starter | Main |
|---|---|
| Puree A Rice/Salmon | 7 |
| Puree B Rice/Salmon | 7 |
| Soft A Rice/Salmon | 9 |
| Soft B Rice/Salmon | 8 |
| Puree A Lentil/Omelet | 9 |
| Puree B Lentil/Omelet | 6 |
| Soft A Lentil/Omelet | 8 |
| Soft B Lentil/Omelet | 8 |
Participants gaze differed depending on whether they answered YES or NO to whether they would like the tray. As illustrated in Table 2, when the participants responded negatively, the mean number of fixations, mean time to first fixation, and mean duration of first fixation were significantly higher than when they responded affirmatively. The duration of fixation and pupil diameter exhibited slight decreases when participants responded negatively, although these differences were not statistically significant.
| N. | Fixation | Total Duration fixation (mseg) | Time to first fixation (mseg) | Duration of fixations (mseg) | Duration of first fixation (mseg) | Pupil diameter (mm) |
|---|---|---|---|---|---|---|
| NO | 49.3 | 10,363.7 | 933.1 | 211.1 | 230.3 | 2.41 |
| YES | 37.5 | 8,137.4 | 797.9 | 211.6 | 165.8 | 2.44 |
p-value* 0.023 0.013 0.003 0.492 0.919 0.547
*p-values in bold indicate significance
3.2. LIKING DECISION IN RELATION TO GAZE BEHAVIOR BY CLASSIFICATION TREES
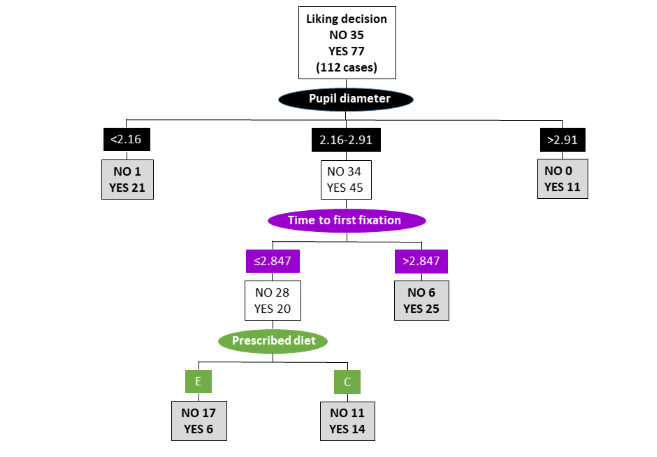
A classification tree with a four-level structure was obtained when the entire dataset (comprising eight menus) was considered. The main parameters that explained the liking decision were pupil diameter, time to first fixation, and the prescribed diet. The initial split was based on the measurement of pupil diameter, with a cut-off point of 2.16 mm. For cases in which the pupil diameter was below this threshold and above 2.91 mm, most participants indicated a positive liking response. Where the pupil diameter was intermediate (2.16-2.91 mm), the decision was contingent upon the time to first fixation exceeding 2.847 mm. In such cases, the liking decision was affirmative. Where the time to first fixation was minimal (i.e., the subjects observed the plate) and the prescribed diet comprised soft food (E), most of the subjects exhibited a negative liking response. The decision paths differed depending on the menu presented (rice/salmon vs. lentil/omelet).
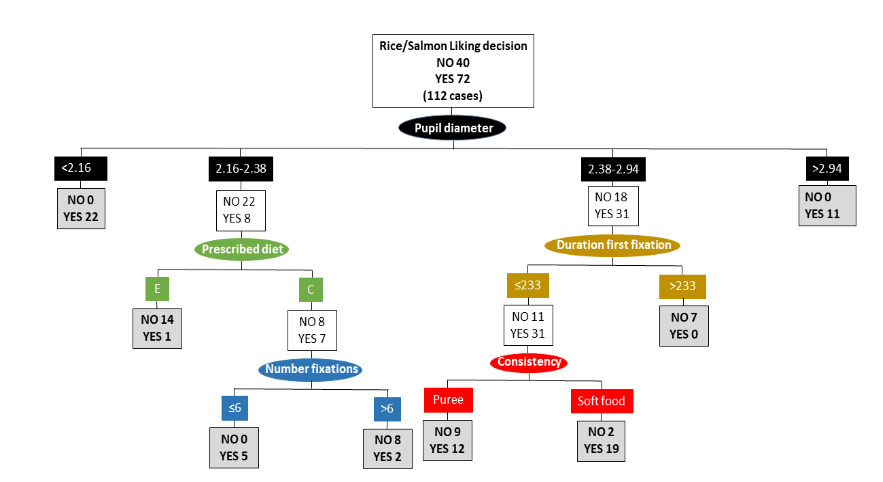
The classification tree for the lentil/omelet tray was more straightforward than that for the rice/salmon trays. Pupil dilation was the only parameter that explained the liking decision. A positive liking decision was indicated when the pupil diameter was below 2.25 mm and above 2.41 mm.
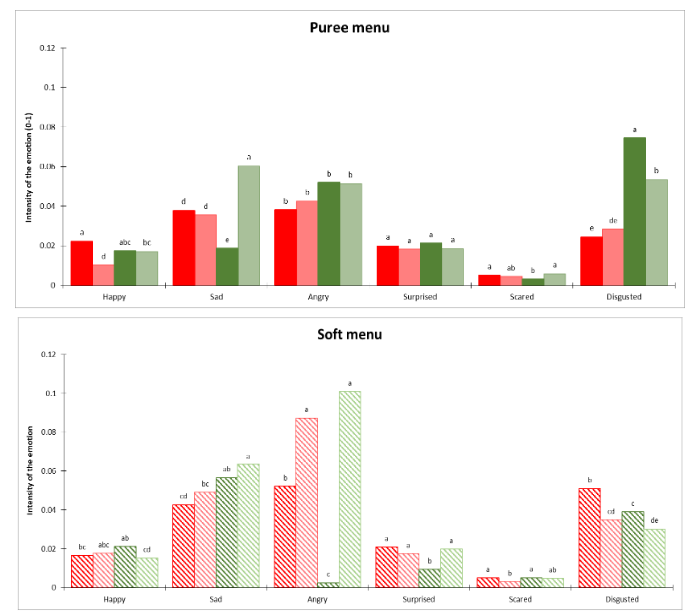
3.3. EMOTIONAL RESPONSE WHEN LOOKING AT THE FULL TRAY FOR DIFFERENT DIET TYPE (PUREE OR SOFT FOOD)

Overall, participants showed a greater propensity to express negative emotions (sad, angry and disgusted) than to express positive emotions (happy). Among the two types of diet, it was no significant differences.
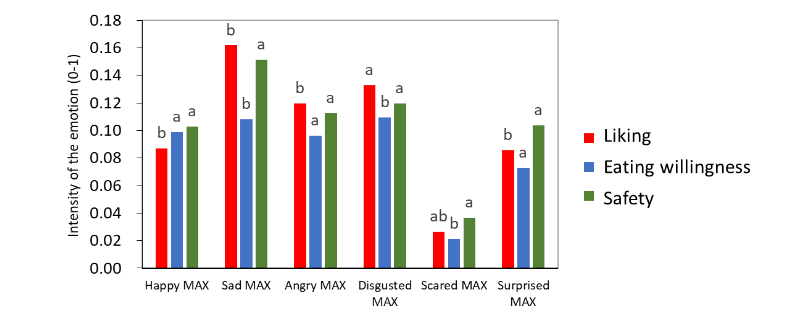
3.4. MAXIMUM EMOTIONAL RESPONSE WHEN LOOKING AT EACH DISH AND ANSWER DIFFERENT QUESTIONS
As demonstrated in Table 3, ANOVA revealed that the patient was a significant factor influencing the maximum level of emotional expression. In addition, the maximum facial expressions of sadness, surprise, and fear were influenced by the type of question, as shown in Table 3. Emotions did not show differences in the patients response (YES/NO) to the three questions (Do you think you will like it?, Do you think you will eat it? Do you think it is safe?) did not show differences in the recorded emotions.
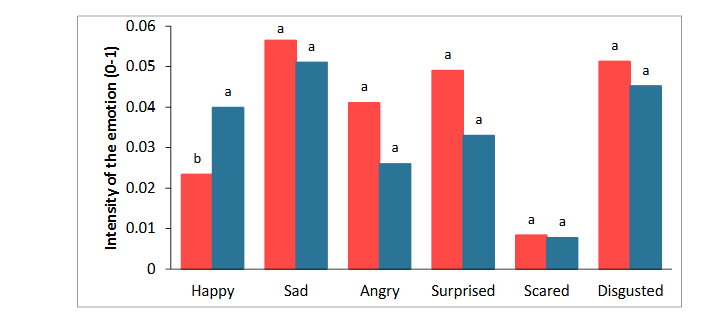
3.5. EMOTIONAL RESPONSE DEPENDING ON THE PRESENTED MENU (B: BASIC DIET; A: ADAPTED)
When participants were queried about the safety of the dishes, the negative emotional response to the adapted presentation of the dishes was lower than that observed for the base versions. Only for the emotion happy were there significant differences, with higher levels of happiness observed when the diet was adapted following the triple adapted diet recommendations.
Discussion
The purpose of this study was to investigate how consumers with dysphagia perceive the food they are served in a hospital context using implicit technique. In summary, gaze behavior results showed that when participants answered negatively to the question about whether they liked the entire tray, the number of fixations, time to first fixation, and duration of first fixation were higher than when they answered affirmatively. Eye tracker methodology, are a direct behavioral measure to understand human behavior, preference, attention, and cognitive processes. In this study, participants spent more time thinking (as reflected by the longer time they spent looking at the tray) before saying no. Previous research on gaze behaviour and emotional responses to non-food items (when looking at social media) has shown that people invest more time looking when they are experiencing negative emotions than positive ones. This is consistent with previous research which suggests that negative emotions lead to deeper information processing than positive emotions.
Beyond the role of emotions when answering no, there have been another related study where time was higher but when food was preferred. Yasui et al. used eye-tracking to identify the food preferences of individuals with communication difficulties. They presented photographs of full-meal trays and attempted to correlate fixation time with preference. The number of fixations and fixation times was found to increase when food was preferred. In another study, Tichý et al. presented consumers with a series of food photographs and found that the images deemed most appealing by participants exhibited higher levels of gaze fixation and monitoring time, with one exception. Here, consumers require additional effort to identify food items. In this study, participants exhibited longer fixation durations when responding NO, which aligns with the findings of Tichý et al. In summary, considering both, those dishes that awake negative emotions and where difficult identifying the food items depicted in the photographs, necessitating additional time for decision-making. Consequently, as previously suggested by other researchers, it is crucial to present food items on the plate in a manner that facilitates identification, reducing the time required for decision-making.
Prior research has also demonstrated a negative perception of pureed foods, which were described as indistinguishable, lacking sensory appeal, and reminiscent of baby foods. Carrillo et al. investigated the impact of puréeing food on flavor recognition, finding it was perceived as less flavorful than the same food in its original state. This finding may explain the low intake of pureed foods. This lack of recognition reinforces the hypothesis that participants will look for longer and respond negatively. However, this fact, the lack of recognition does not explain the negative emotions associated with the soft puree diet. Therefore, only the fact of seeing the meals presented in a hospital tray might cause these emotions.
When using a classification tree, the main element determining like response was pupil size. Negative facial emotions related to the modified dish presentation were less common than those seen in the original versions. The results indicated pupil size was the primary factor influencing the response to liking. Both pupil dilation (large size) and constriction (small size) were associated with a positive liking response. This dichotomy has been identified in other studies. In contrast to the findings of Beukema et al., which indicated that unfamiliar objects elicited greater pupil dilation than familiar objects, other studies have reported that smaller pupils are associated with the perception of unfamiliar images and branded products. Here, it was observed that two participants with a dilated pupil measuring greater than 2.91 mm consistently responded affirmatively to all questions regarding liking. At the opposite end of the spectrum, three participants with a small pupil size (less than 2.16 mm) indicated a consistent affirmative response.
The results indicated that participants with the prescribed diet E (soft pieces of food) were more selective than patients with the prescribed diet C (pureed food). This was evidenced because they rejected more trays, particularly when they were presented with plates. These findings align with those of Ettinger et al., who examined the acceptance of pureed food by two consumer groups (pureed and non-pureed food consumers). The study found that puree consumers exhibited a greater preference for the appearance of purees than did non-puree consumers, potentially because of their familiarity with these products.
Limitations of this study and future perspective
The principal limitation of this study is the relatively small number of participants. It is also crucial to guarantee the stability of participants’ heads. For some, maintaining the stability of their heads throughout the test proved challenging, underscoring the necessity to identify a method for stabilizing their heads in a manner that is both effective and comfortable. It is also important to understand that participants only viewed an image and, for safety reasons, did not eat the food served, which might have produced different results.
Conclusions
This study represents a first effort to use implicit methodologies in patients with dysphagia within a hospital context. Analysis of eye-tracking parameters and participants’ preferences using regression trees demonstrated a correlation between verbal preference and pupil dilation. It has been proposed that pupil size can be used as an index to predict the preference for visual stimuli. Furthermore, the study confirmed that patient recognition of food is a crucial factor in improving their liking, as this is often challenging when food is presented in pureed form. The analysis of facial expressions indicated that sensory adaptation of the dishes served resulted in an improvement in the patients’ positive emotional state when viewing the diets. The emotions elicited differed depending on the question posed whether the respondents expressed a preference for the food, intended to eat it, or perceived it as safe. Thus, it can be posited that the manner of food presentation and the verbal instructions provided when presenting the food can act as drivers to improve dietary preference and acceptance. These findings suggest that the use of implicit methods can assist food service providers in selecting different menus that could enhance dining experiences and improve food intake for individuals with texture-modified diets. Further research with a larger sample size is needed.
Acknowledgements:
This research was funded by MCIN/AEI/ 10.13039/501100011033 grant number PID2020-117016RB-100. The authors thank the Spanish government (MCIN/AEI) and the Severo Ochoa Centre of Excellence Accreditation for financial assistance (CEX2021-001189-S/ MCIN/AEI/ 10.13039/501100011033).
References:
- Hedman S, Nydahl M, Faxén-Irving G. Individually prescribed diet is fundamental to optimize nutritional treatment in geriatric patients. Clin Nutr 2016;35(3):692-8. doi:10.1016/j.clnu.2015.04.018.
- Rattray M, Desbrow B, Roberts S. Comparing nutritional requirements, provision and intakes among patients prescribed therapeutic diets in hospital: an observational study. Nutrition 2017;39-40:50-6. doi:10.1016/j.nut.2017.03.006.
- Shimazu S, Yoshimura Y, Kudo M, Nagano F, Bise T, Shiraishi A et al. Frequent and personalized nutritional support leads to improved nutritional status, activities of daily living, and dysphagia after stroke. Nutrition 2021;83:111091. doi:10.1016/j.nut.2020.111091.
- IDDSI. IDDSI framework, Available from: https://iddsi.org/framework/.
- Okkels SL, Saxosen M, Bügel S, Olsen A, Klausen TW, Beck AM. Acceptance of texture-modified in-between-meals among old adults with dysphagia. Clin Nutr ESPEN 2018;25:126-32. doi:10.1016/j.clnesp.2018.03.119.
- Pouyet V, Cuvelier G, Benattar L, Giboreau A. Influence of flavour enhancement on food liking and consumption in older adults with poor, moderate or high cognitive status. Food Qual Preference 2015;44:119-29. doi:10.1016/j.foodqual.2015.04.014.
- Wright L, Hickson M, Frost G. Eating together is important: using a dining room in an acute elderly medical ward increases energy intake. J Hum Nutr Diet 2006;19(1):23-6. doi:10.1111/j.1365-277X.2006.00658.x.
- Pu D, Choi YY, Chan KMK, Poon MMW. Modifying puree meals in residential aged care facilities: a multi-centre feasibility and acceptability study. Geriatrics (Basel) 2021;6(4):108. doi:10.3390/geriatrics6040108.
- Pant A, Lee AY, Karyappa R, Lee CP, An J, Hashimoto M, et al. 3D food printing of fresh vegetables using food hydrocolloids for dysphagic patients. Food Hydrocoll 2021;114:106546. doi:10.1016/j.foodhyd.2020.106546.
- González-Fernández M, Brodsky MB, Palmer JB. Poststroke communication disorders and dysphagia. Phys Med Rehabil Clin N Am 2015;26(4):657-70. doi:10.1016/j.pmr.2015.06.005.
- Ettinger L, Keller HH, Duizer LM. A comparison of liking of pureed food between two groups of older adults. J Nutr Gerontol Geriatr 2014;33(3):198-209. doi:10.1080/21551197.2014.927305.
- Duerrschmid K, Danner L. Eye tracking in consumer research. In: Methods in consumer research, vol. 2. Woodhead Publishing; 2018. p. 279-318. doi:10.1016/B978-0-08-101743-2.00012-1.
- Mitterer-Daltoé ML, Queiroz MI, Fiszman S, Varela P. Are fish products healthy? Eye tracking as a new food technology tool for a better understanding of consumer perception. LWT Food Sci Technol 2014;55(2):459-65. doi:10.1016/j.lwt.2013.10.013.
- De Wijk RA, Kaneko D, Dijksterhuis GB, van Zoggel M, Schiona I, Visalli M et al. Food perception and emotion measured over time in-lab and in-home. Food Qual Preference 2019;75:170-8. doi:10.1016/j.foodqual.2019.02.019.
- Baranda AB, Ríos Y, Llorente R, Naranjo AB, da Quinta N. Neuroscience tools to study the effect of the presentation form on food-evoked emotion for senior population. Food Res Int 2024;183:114158. doi:10.1016/j.foodres.2024.114158.
- Costa A, Carrión S, Puig-Pey M, Juárez F, Clavé P. Triple adaptation of the Mediterranean diet: design of a meal plan for older people with oropharyngeal dysphagia based on home cooking. Nutrients 2019;11(2):425. doi:10.3390/nu11020425.
- Chahboun S, Flumini A, Pérez González C, McManus IC, Santiago J. Reading and writing direction effects on the aesthetic appreciation of photographs. Laterality 2017;22(3):313-39. doi:10.1080/1357650X.2016.1196214.
- Stasi, A., Songa, G., Mauri, M., Ciceri, A., Diotallevi, F., Nardone, G., & Russo, V. (2018). Neuromarketing empirical approaches and food choice: A systematic review. Food research international, 108, 650-664.
- Kohout, S., Kruikemeier, S., & Bakker, B. N. (2023). May I have your Attention, please? An eye tracking study on emotional social media comments. Computers in Human Behavior, 139, 107495.
- Nabi, R. L. (1999). A cognitive‐functional model for the effects of discrete negative emotions on information processing, attitude change, and recall. Communication theory, 9(3), 292-320.
- Yasui Y, Matsuo S, Kakudo M, Tanaka J, Tanaka M. Association between food preferences and gaze in healthy young adults using eye tracker. Jpn J Dysphagia Rehab 2017;21:11-9. doi:10.32136/jsdr.21.1_11.
- Tichy J, Rosenlacher P, Marsalkova L. Neuromarketing approach to efficient food styling; 2017. Interdiscipl AAJ. Res 2017;7:180-3.
- Keller HH, Duizer LM. What do consumers think of pureed food? Making the most of the indistinguishable food. J Nutr Gerontol Geriatr 2014;33(3):139-59. doi:10.1080/21551197.2014.927302.
- Carrillo E, Laguna L, Arancibia C, Tárrega A. Rescuing Flavor identity and dynamic perception in Puréed dishes; a restructuring solution for the Purée diet. Foods 2021;10(4):905. doi:10.3390/foods10040905.
- Beukema S, Jennings BJ, Olson JA, Kingdom FAA. The pupillary response to the unknown: novelty versus familiarity. Iperception 2019;10(5):2041669519874817. doi:10.1177/2041669519874817.
- Franzen L, Cabugao A, Grohmann B, Elalouf K, Johnson AP. Individual pupil size changes as a robust indicator of cognitive familiarity differences. PLOS One 2022;17(1):e0262753. doi:10.1371/journal.pone.0262753.
- Naber M, Frässle S, Rutishauser U, Einhäuser W. Pupil size signals novelty and predicts later retrieval success for declarative memories of natural scenes. J Vis 2013;13(2):11. doi:10.1167/13.2.11.