






Peripheral Ischemia Risk in Dialysis Patients Without Diabetes
High risk of peripheral ischemia in patients on dialysis without diabetes mellitus.
Lene Boesby1, Kristine Hommel2, Jonas B. Olesen3, Louise De La Motte4, Christian Wied5, Pernille Mork Hansen6
- Dept. of Nephrology and Endocrinology, Rigshospitalet, Denmark
- Dept. of Medicine, Holbaek Hospital, Denmark
- Dept. of Cardiology, Herlev and Gentofte University Hospital, Denmark
- Dept. of Vascular Surgery, Copenhagen University Hospital, Rigshospitalet, Denmark
- Dept. of Orthopedic Surgery, Hvidovre Hospital
- Dept. of Nephrology, Herlev Hospital, Denmark
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Boesby, L., Hommel, K., et al., 2024. High risk of peripheral ischemia in patients on dialysis without diabetes mellitus. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.6038
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.6038
ISSN 2375-1924
ABSTRACT
Background: Patients on dialysis have an increased risk of peripheral arterial disease. This nationwide Danish cohort study describes the incidence of lower extremity amputation or revascularization in patients treated with dialysis and explores influence of diabetes mellitus and dialysis modality over time.
Methods: By individual-linkage between nationwide registries, risk of lower extremity amputation or revascularization was compared between two time periods and groups of patients treated with hemodialysis or peritoneal dialysis, with or without diabetes mellitus.
Results: We assessed risk of lower extremity amputation or revascularization in 75 419 patients with diabetes not on dialysis and 10 908 dialysis patients. Compared with the background population, hazard ratio for lower extremity amputation or revascularization associated with diabetes or treated with peritoneal dialysis without diabetes was equal, hazard ratio 12. Patients with diabetes on hemodialysis had hazard ratio 117(104-131) in the period 1997-2004 with lower hazard ratio in the later period, hazard ratio 68(60-77). For patients treated with hemodialysis with no diabetes, hazard ratio was not lower in the second time period; hazard ratio 15(13-18) vs hazard ratio 17(14-20). Hazard ratios of lower extremity amputation or revascularization were not significantly lower in patients with peritoneal dialysis and diabetes in the later period, hazard ratio 38(30-48) vs 30(23-37). For patients on hemodialysis with diabetes a lower hazard ratio was found in the later period. Patients without diabetes had almost the same risk of lower extremity amputation or revascularization over time. Patients on peritoneal dialysis had, compared to patients treated with hemodialysis, lower risk of lower extremity amputation or revascularization.
Conclusions: Patients on dialysis without diabetes had an equal or increased risk of lower extremity amputation or revascularization compared to patients with diabetes not on dialysis. Patients on dialysis with diabetes had higher risk compared to those without diabetes. Risk was higher in patients on hemodialysis compared to patients on peritoneal dialysis. Over time there was a trend towards decreased risk in dialysis patients with diabetes. The Danish programme for yearly evaluation of peripheral ischemia by podiatricians in patients with diabetes may be one of the reasons for the differences seen in risk reduction.
Keywords: Cohort study; dialysis; diabetes; peripheral vascular disease; amputation; revascularization
INTRODUCTION
There is a worldwide increase in number of patients treated with chronic dialysis and in number of patients with diabetes mellitus (DM). In the state of chronic uremia, accelerated vascular aging is present with vascular calcification including atherosclerosis and arteriosclerosis, both leading to increased risk of peripheral ischemia with the need for revascularization procedures or amputations. Even in patients with chronic kidney disease without diabetes there is a high risk of peripheral ischemia. Peripheral ischemia could potentially result in lower quality of life. Therefore, it is important to describe the incidence of peripheral ischemia and risk of amputation or revascularization as well as to identify risk factors, particularly if they are modifiable.
A programme for monitoring foot status by podiatricians was established in Denmark in 1981 (personal communication) for the population of patients with diabetes mellitus (DM). The same awareness has not been given to patients treated with dialysis, but with no DM. The aim of this large cohort study was to investigate the risk of lower extremity amputation (LEA) or surgical revascularization over time in the Danish dialysis population (hemodialysis (HD) vs peritoneal dialysis (PD)) compared to the background population stratified by presence of DM. Two time periods were chosen in order to evaluate improvement in preventive measures.
MATERIALS AND METHODS:
STUDY DESIGN
Retrospective national cohort study.
Setting and participants
Persons above 18 years of age in Denmark were included at 1st of January 1997 and grouped according to +/- DM. Incident patients starting dialysis from 1st of January 1997 to 27th of January 2014 were also included. All patients on dialysis were grouped according to DM, dialysis modality PD or HD and period of inclusion 1997-2004 or 2005-2014. Patients living with a kidney transplant were excluded. Patients were followed until lower extremity amputation, -revascularization, emigration, death or end of study at 31st of December 2016. Dialysis patients were identified in the Danish Nephrology Registry. Persons with DM were identified in the National Patient Registry by ICD-10 diagnoses E10-14 6 months before inclusion or in the Danish Prescription Registry by filling a prescription of antidiabetic medication ATC MA10.
BASELINE VARIABLES AND OUTCOME
Gender and age at study start were found in the Danish Civil Registration System. Comorbidity was identified in the National Patient Registry one year before study start. Treatment with cholesterol lowering medication, platelet inhibitors or insulin was identified in the Danish Prescription Registry. Outcome was lower extremity revascularization procedures or – amputations registered in the National Patient Registry.
DATA SOURCES
Information on date of chronic renal replacement therapy start and modality was obtained from the Danish Nephrology Registry, where all patients actively treated for end-stage kidney disease (ESRD) in Denmark are registered. The Danish civil registration system holds information including date of birth and death on the Danish population. Information on comorbidity and revascularization procedures and amputations was identified in the National Patient Registry. This contains information on all hospital admissions in Denmark including diagnoses, operations, dates, hospitals and departments since 1978 and from 1995 also information on out-patient treatment. Information on medical treatment was obtained from the Danish Register of Medicinal Product Statistics of the Danish Medicines Agency. The registry contains information on dispensed drugs from Danish pharmacies since 1995. Cross-linkage between registries was possible due to the unique personal identification number assigned to all Danish citizens from birth or immigration.
ETHICAL CONSIDERATIONS
The study was approved by the Danish Data Protection Agency.
STATISTICAL ANALYSIS
Baseline characteristics were given for persons +/- DM and for dialysis patients furthermore in two time periods 1997-2004 and 2005-2014 with percentages, medians and interquartile ranges where appropriate. Incidence rates were standardized according to gender and age using five age groups with the direct method and the Danish background population as reference. The age strata 18-39 years, 40-49 years, 50-59 years, 60-69 years and +70 years of age were used. Test for interaction was performed and if present, appropriate stratification was done. There was a significant interaction between treatment group and age, gender, previous revascularization, peripheral vascular disease or amputation, gastrointestinal ulcer, cardiovascular disease, rheumatic disease, ischemic heart disease, chronic heart failure, obstructive pulmonary disease, use of cholesterol lowering drugs and platelet inhibitors. Though, none appeared to influence the risk of lower extremity revascularization or amputation. Cox proportional hazards models with revascularization and amputation of the lower extremity as outcome were fitted to the data. Stepwise adjustment was made for gender, age, comorbidity, prior revascularization or amputation and drug use. Proportional hazards were checked graphically and proportional hazards assumption was met. Sensitivity analysis with lower extremity amputation as lone outcome was performed. Analyses were performed using SAS version 9.4, SAS Institute Inc.
RESULTS
A total of 75 419 patients with diabetes not on dialysis and 10 908 patients on dialysis were included. Tables 1A and 1B show baseline characteristics of the background population and patients with and without DM in Denmark according to dialysis modality in the two time periods, respectively. Patients with DM or treated with dialysis were older than the background population. Overall, patients had a greater number of comorbidities if treated with dialysis, regardless of modality and those with DM had even more, besides DM, than those without DM. There was a trend towards higher age in all dialysis patients in the late period.
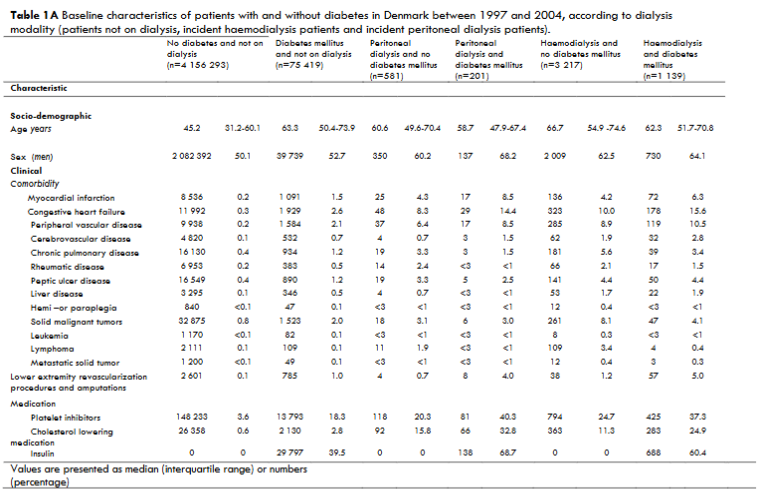
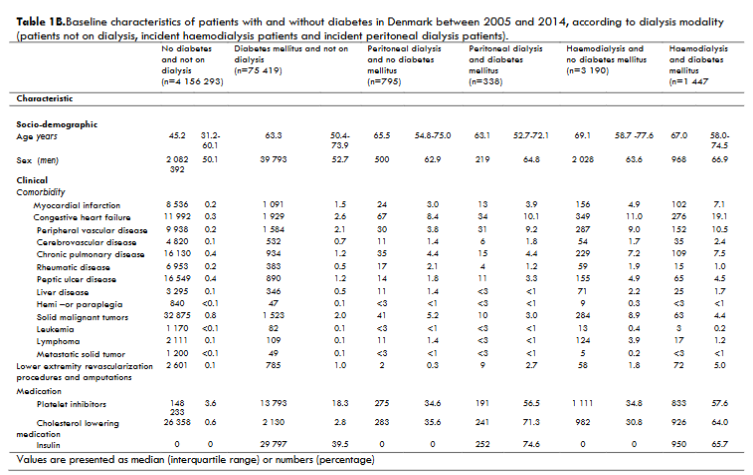
There was no difference in vascular disease such as myocardial infarction (MI), heart failure, cerebrovascular disease at baseline over time. There was a trend of higher prevalence at baseline of peripheral arterial disease (PAD) in dialysis patients with DM and HD patients compared to PD-patients. More revascularizations and amputations were present at baseline in patients included in the later period. The use of platelet inhibitors and cholesterol lowering medication at baseline was higher in dialysis patients in the later period.
Tables 2A and 2B show incidence rates of lower extremity revascularization procedures (LER) and lower extremity amputations (LEA) from 1997-2004 and 2005-2014 according to dialysis modality and presence of DM.
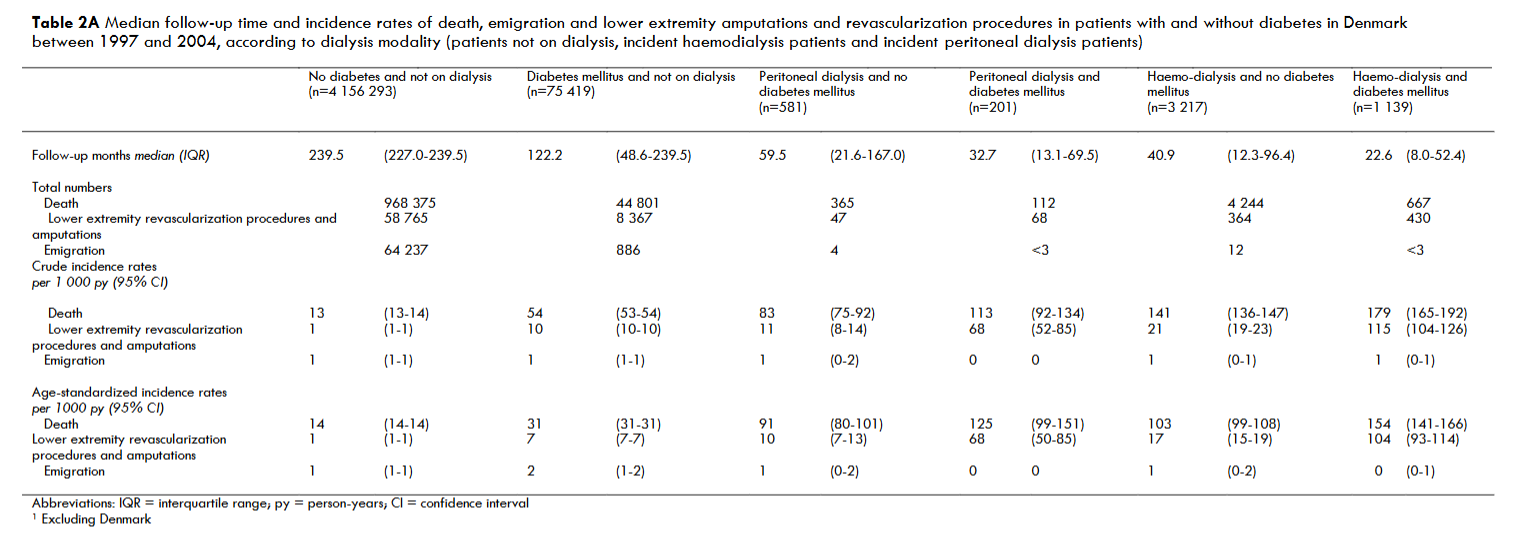
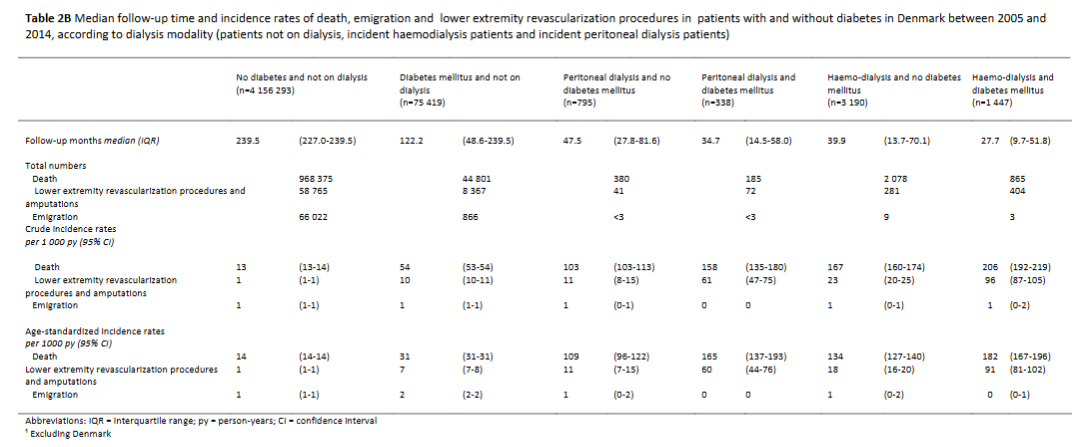
Table 3 shows hazard ratios for lower extremity revascularization procedures and amputations in patients with and without diabetes in Denmark between 1997 and 2014, according to dialysis modality (patients not on dialysis, incident haemodialysis patients and incident peritoneal dialysis patients) and time period of starting dialysis (1997-2004 and 2005-2014).
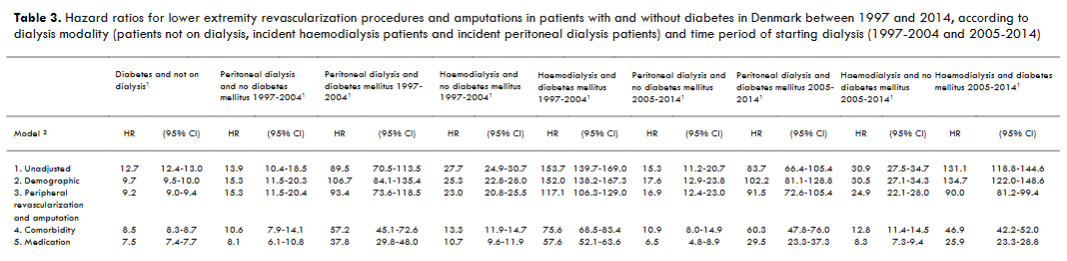
Table 4 shows hazard ratios for lower extremity amputations in patients with and without diabetes in Denmark between 1997 and 2014, according to dialysis modality (patients not on dialysis, incident haemodialysis patients and incident peritoneal dialysis patients) and time period of starting dialysis (1997-2004 and 2005-2014).
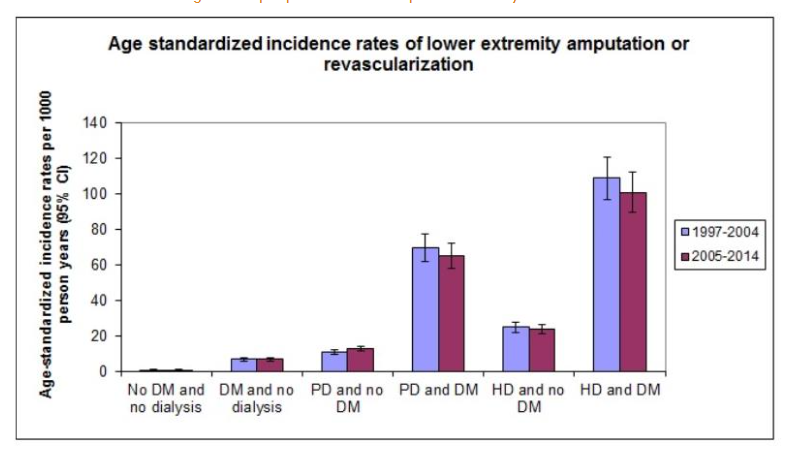
Figure 1 shows cumulative incidence curves for LEA with death as competing end point. The curves show the overall higher incidences of LEA’s if on dialysis and having DM. The incidences were lower in the later time period for both modalities of dialysis, more in PD. Patients with no DM had no difference in LEA in the two time periods.
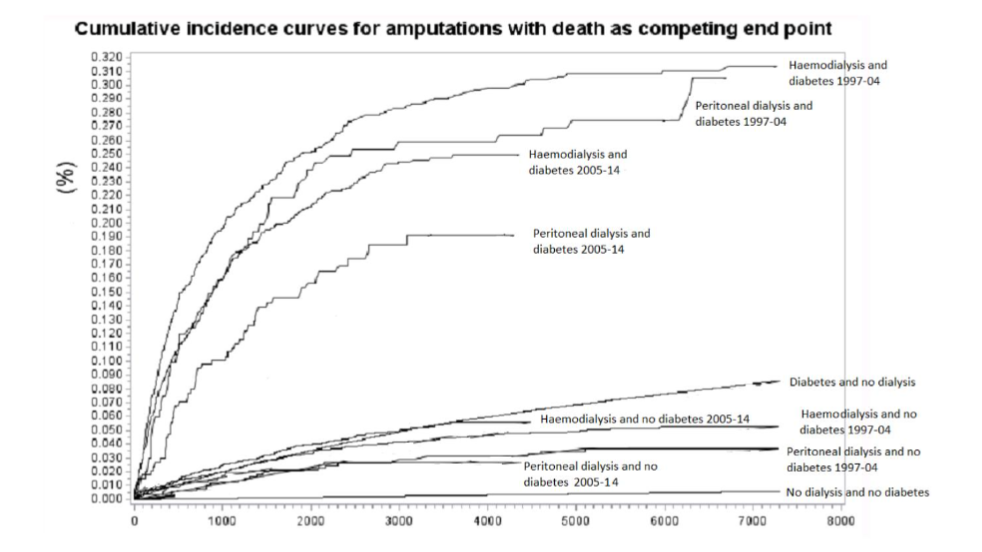
Figure 2 shows cumulative incidence curves for LEA and LER with death as competing end point. The curves show a clear difference between dialysis modalities and between patients with and without DM, the latter having more interventions than patients without DM. The two time periods differ as in Figure 1.
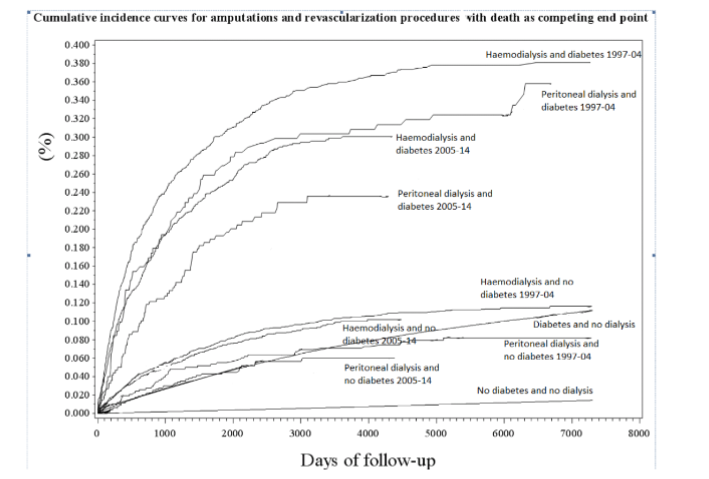
Figure 3 depicts HRs of LEA and LER in combination, stratified by time period, dialysis modality and diabetes state. When adjusting for age, sex, comorbidity, prior peripheral revascularization and amputation as well as medication, results remained unchanged.
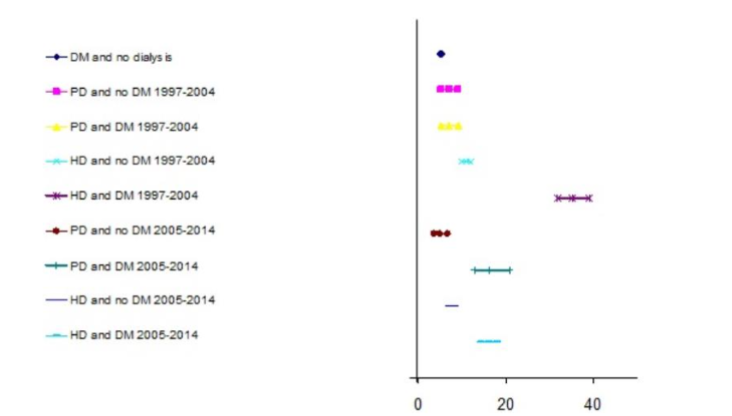
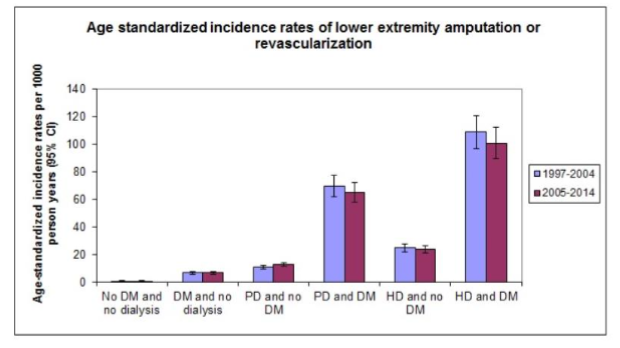
Figure 4 shows the smaller incidence rates of LEA/LER in the later time period for patients with DM.
DISCUSSION
This paper investigates the rates of LER and LEA in patients treated with dialysis, stratified by dialysis modality and presence of DM compared to the background population. Data were also investigated over time. We found that a great part of patients on dialysis had a high risk of LEA or LER compared to the background population and dialysis patients had a comparable or higher risk compared to diabetes patients not on dialysis.
We found a decrease in LER/LEA in patients with DM over time, but not in patients on dialysis without DM. This indicates that interventions have taken place and that these interventions have proven effective. Other studies have found the same trend. The suggested primary intervention is the formalized attention paid to foot ulcers and peripheral ischemia and neuropathy in the patients with DM. In Denmark since 1981 patients with DM have been screened for peripheral ischemia and neuropathy by podiatricians.
The same prevention programme has not been offered to patients treated with dialysis with no DM. In 2018 121,225 patients with DM had regular assessments of peripheral ischemia and neuropathy assessed by podiatricians by standardized observations. The number of patients, who accept this offer has been increasing since 2012 (personal communication).
O’Hare describes the fact that most dialysis patients are not screened for PAD despite easy access to patients and the high prevalence of PAD in this group of patients. Traditional risk factors for PAD all apply to dialysis patients along with other unconventional factors such as chronic inflammation, and a diversity of biomarkers. Reasons for differences in incidences of LEA/LER in patients on PD vs HD could be the greater comorbidity found in the population treated with HD together with the greater hemodynamic disturbances seen in patients on HD. Patients treated with PD have a greater preserved residual renal function, which could decrease the overall uremic toxin load. Treatment with statins and platelet inhibitors was more common in the second time period. This may also contribute to reduced incidence of LEA and LER.
Peripheral ischemia may be silent, because the affected patients often have neural damage along with ischemia. This may lead to unawareness of ulcers in the early state, thus letting them progress to larger ulcers with the need for surgical revision and high risk of infection. If ulcers cannot heal the risk of amputation increases and possibility of revascularization decreases.
Identification of the patients at risk is important. All patients with DM should ideally be seen by a podiatrician at intervals already suggested. Screening of peripheral ischemia should be done in all dialysis patients including those with no DM. The patients treated with center HD are in the department 2-4 times per week, for at least 3 hours, thus there should be ample opportunity to examine their feet. In the case of patients on PD or home HD, they are seen every 4-8 weeks and routine examination of feet thus possible. Guidelines have inferred recommendations for routine examination of feet in order to enable early identification of patients at risk.
The time to development of foot ulcers in the uremic state is unknown. We suggest interventions for patients on dialysis without DM of at least same standard as for the patients with DM. When patients are allocated to dialysis treatment a status of their feet should be made in the same manner as for those who have DM. Risk stratification will decide how often patients should be seen by a podiatrician. The standardized programme could be transferred to patients on dialysis. This comprises yearly status visits and by risk stratification a standardized reaction to either increased awareness of referral to orthopedic or vascular surgeon. Since patients on dialysis have frequent visits to the clinic it is feasible that trained nurses examine and evaluate patients’ feet i.e. every 4-8 weeks during dialysis sessions. For those in PD, they should have examinations when they are at the outpatient clinic.
If there is any doubt regarding pulse, referral for measurements of toe pressure should be made. In case of critically low values or ulcers referral to a vascular surgical department is necessary. Ankle/brachial index may be falsely high due to mediasklerosis and the presence of incompressible calcified blood vessels in patients with diabetes or uremia.
For those in HD, treadmills should be offered for patients who lead a physically inactive life.
CONCLUSION:
Greater awareness and regular visits to podiatricians for patients on dialysis with DM seems to have reduced the need of LEAs. The reduction was not due to greater number of LERs. Future investigations should be made in order to show if standardized evaluations of feet of patients on dialysis regardless of state of DM will reduce the risk of peripheral ischemia with the detrimental results of LER and/or LEA. It remains to be seen whether PD compared to HD will reduce the risk of peripheral ischemia or differences seen are a result of case mix. Future studies should investigate the effect of increased awareness and screening of ischemia and neuropathy with regards to reduction of LEA and LER. Interventions could consist of medical treatment and investigate the effect of increase exercise by treadmill.
LIMITATIONS:
This is a retrospective study.
ACKNOWLEDGEMENTS
The authors wish to thank Tina Ronhoj, podiatrician for personal communications.
CONFLICT OF INTEREST STATEMENT
The authors state to have no conflicts of interest.
FUNDING
No funding was used to prepare this manuscript.
REFERENCES
- https://www.who.int/bulletin/volumes/96/6/17-206441/en/ [Online]
- https://www.who.int/mediacentre/factsheets/fs138/en/ [Online]
- Briet M, Burns KD. Chronic kidney disease and vascular remodelling: molecular mechanisms and clinical implications. Clin Sci (Lond). Oct; 123 (7): 399-416 2012.
- O’Hare A, Johansen K. Lower Extremity Peripheral Arterial Disease Among Patients with End-stage Renal Disease. JASN. 2001(12), 2838-2847.
- Londero LS, Hoegh A, Houlind K, Lindholdt J. Major Amputation Rates in Patients with Peripheral Arterial Disease Aged 50 Years and Over in Denmark during the period 1997-2014 and their Relationship with Demographics, Risk Factors, and Vascular Services. Eur J Vasc Endovasc Surg. 2019 Nov;58(5):729-737. doi: 10.1016/j.ejvs.2019.06.007. Epub 2019 Sep 21.
- Kofod DH, Almdal TP, Sørensen VR, Feldt-Rasmussen B, Hornum M. Micro- and macrovascular complications and risk factors for foot ulceration and amputation in individuals receiving dialysis with and without diabetes. Endocrinol Diabetes Metab. 2022 Jan;5(1):e00305. doi: 10.1002/edm2.305. Epub 2021 Oct 17.
- Otte J, van Netten JJ, Woittiez AJ. The association of chronic kidney disease and dialysis treatment with foot ulceration and major amputation. J Vask Surg. 2015 Aug;62(2):406-11. doi:10.1016/j.jvs.2015.02.051. Epub 2015 May 1.
- Combe C, Albert JM, Bragg‐Gresham JL, Andreucci VE, Disney A, Fukuhara S, Goodkin DA, Gillespie BW, Saito A, Jadoul M, Pisoni RL. The burden of amputation among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2009 Oct;54(4):680-92. doi:10.1053/j.ajkd.2009.04.035. Epub 2009 Jul 19.
- Kaminski MR, Lambert KA, Raspovic A, McMahon LP, Erbas B, Mount PF, Kerr PG, Landorf KB. Risk factors for foot ulceration in adults with end-stage renal disease on dialysis: a prospective observational cohort study. BMC Nephrol. 2019 Nov 21;20:423. doi: 10.1186/s12882-019-1594-5.
- Hommel K, Madsen M, Rasmussen S, Kamper A. The Danish Registry on Regular Dialysis and Transplantation: completeness and validity of incident patient registration. Nephrology Dialysis Transplantation. 2010, s. (25): 947–51.
- Pedersen, CB. The Danish Civil Registration System. Scand J Public Health. 2011: (39:) 22-25.
- Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015: (7) 449–90.
- Kildemoes HW, Sørensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health. July (39(7 Suppl): 38-41 2011.
- Franz D, Zheng Y, Leeper NJ, Chandra V, Montez-Rath M, Chang TI. Trends in Rates of Lower Extremity Amputation Among Patients With End-stage Renal Disease Who Receive Dialysis. JAMA Intern Med. 2018 Aug, Årg. 178 (8), 1025-1032.
- Wang IK, Hsu CH, Tsai CH, Chang SS, Lin CL, Yen TH, Lin SY, Lin CC, Liu JH, Chang CT, Sung FC. Comparison of the risk of non-traumatic lower extremity amputation between haemodialysis and peritoneal dialysis patients with end-stage renal disease. Nephrology (Carlton). 2018 Jan;23(1):86-92. doi: 10.1111/nep.12946. 23 (1), 2018 (JAN), 86-92.
- Parmar GM, Novak Z, Spangler E, Patterson M, Passman MA, Beck AW, Pearce BJ. Statin use improves limb salvage after intervention for peripheral arterial disease. Ref J Vasc Surg. 2019 Aug:70 (2), 539-46.
- McDivitt JD, Braun M, Kassop D. Cardiovascular disease: Lower Extremity Peripheral Artery Disease. FP Essent. 2019 Apr: 479, 11-15.
- Jovanovic DB, Matanovic DD, Simic-Ogrizovic SP, Stosovic MD, Bontic AC, Nesic VD. Polyneuropathy in diabetic and nondiabetic patients on CAPD: is there an association with HRQOL? Perit Dial Int. 2009 Jan; 29(1): 102-7.
- Mambelli E, Barrella M, Facchini MG, Mancini E, Sicuso C, Bainotti S, Formica M, Santoro A. The prevalence of peripheral neuropathy in hemodialysis patients. Clin Nephrol. 2012 Jun; 77(6): 468-75.
- Kaminski MR, Raspovic A , McMahon PL , Lambert KA, Erbas B, Mount PF, Kerr PG, Landorf KB. Factors associated with foot ulceration and amputation in adults on dialysis: a cross-sectional observational study. BMC Nephrol. 2017 Sep; 18(1):293.
- Kaminski MR, Raspovic A, McMahon LP, Strippoli GFM, Palmer SC, Ruospo M, Dallimore S, Landorf KB. Risk factors for foot ulceration and lower extremity amputation in adults with end-stage renal disease on dialysis: a systematic review and meta-analysis. Nephrol Dial Transplant. 2015 Oct: 30(10), 1747-66.