





Physician Well-Being: Mentoring and Coaching Strategies
Mentoring, coaching and peer-support programs promoting well-being for physicians: A systematic review
Mark R Ellis*¹, Gwen Wilson², Esme Nulan¹, Margaret A Day², Jane A McElroy²
- School of Medicine-Springfield Clinical Campus, University of Missouri-Columbia, Columbia, Missouri, United States of America
- Department of Family and Community Medicine, University of Missouri-Columbia, Columbia, Missouri, United States of America
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Ellis, MR., Wilson, G., et al., 2024. Mentoring, coaching and peer-support programs promoting well-being for physicians: A systematic review. Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5618
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5618
ISSN 2375-1924
ABSTRACT
Introduction As many as half of U.S. physicians experience impactful levels of burnout. In early-career physicians, the consequences of burnout are significant with linkage to poor professionalism and patient care. A nurturing peer community and physician mentoring may mitigate against burnout and its associated sequelae; however, such programs for early-career physicians are rare and their impact largely unknown. We aim to synthesize the current literature on the impact of longitudinal mentoring and coaching programs for physicians.
Methods The authors searched four bibliographic databases to conduct a systematic review following PRISMA guidelines. Included studies were published between 01 January 2000 to 30 October 2022 and peer-reviewed articles reporting original research. The review examined associations between either a career mentoring, coaching, or peer support theme and outcomes in the career path of physicians.
Results Review of 5528 records yielded 23 articles that met inclusion criteria, with about half describing U.S. programs and half completed since 2017. Of these, 14 studies were of “high” or “medium” quality, 7 studies involved primary care physicians and 3 studies focused only on early-career physicians. In mixed methods studies, participants consistently reported positive experiences from their mentorship involvement and the 8 randomized control or cohort studies also reported positive effects with the mentoring programs.
Conclusion Rigorous data supporting the value of mentorship, including the best approach to be used (coaching, mentorship, or peer support) is lacking. However, a growing database of quality studies affirms physician mentoring as important to physician retention, wellbeing and quality healthcare delivery.
Keywords
- Mentoring
- Coaching
- Peer-support
- Burnout
- Physician well-being
Introduction
Over 40 years ago, Maslach and Jackson defined burnout as “a syndrome of emotional exhaustion and cynicism that occurs frequently among individuals who do ‘people-work’ of some kind. A key aspect of the burnout syndrome is increased emotional exhaustion which is related to job satisfaction, performance and retention.” Although the syndrome was named over 40 years ago, this phenomenon has been a focus of intensive research. Studies have linked feelings of burnout to adverse mental health issues among healthcare providers and to compromised healthcare for their patients. Working in healthcare is increasingly demanding. Studies completed in the last two years report a burnout rate of forty to fifty percent among U.S. Physicians. Nearly one-quarter of these are planning to leave medical practice within two years. Burnout is reported by 24% to 75% of resident physicians and may increase during the first year of practice. These declining trends in job satisfaction have also been reported among British and Norwegian general practitioners. This is of particular concern during the first five years of practice, wherein high demands and lack of professional resources result in lack of engagement, withdrawal behaviors, and harms to personal health.
Numerous studies have identified predictors of burnout, such as use of electronic medical record, poor work control and greater time pressure. This has led to multiple suggestions to reduce the factors associated with burnout, with much less attention given to programs to support well-being among healthcare clinicians. Coaching, mentoring, and peer support each have potential to enhance well-being. Mentorship, in which a more experienced and knowledgeable healthcare professional guides a less experienced colleague in career development, has been utilized since the dawn of medical practice. It requires an ongoing relationship between the mentor and one who is being mentored. Peer support—the sharing of experience, knowledge, and a social network among individuals of equivalent experience and a common background − is a close cousin of mentorship. Coaching, a process of inquiry, encouragement, and accountability, seeks to increase self-awareness and to facilitate a person’s navigation of professional life and career choices. It does not require the person and his/her coach to share a professional background.
The recent epidemic of physician burnout-especially in young and mid-career physicians-has led to a proliferation of related commentaries and small mentorship studies. What has been lacking is a cogent compilation and overview of this body of research. We sought to examine the impact of longitudinal coaching mentoring, and peer support programs for physicians.
Methods
Our systematic review follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. We performed a comprehensive search of four bibliographic databases: PubMed, CINAHL, Scopus, APA PsycINFO with PsycARTICLES for studies published in English between 01 January 2000 and 30 October 2022. The initial search was conducted on 30 June 2022 and last updated on 30 October 2022. We restricted our search to articles focused on physicians, with emphasis on mentoring, coaching, or peer support programs. Sample search terms utilized were physician, doctor, hospitalist, mentor, coach, orientation, onboarding, retention, burnout, stress, resilience.
Eligible publications included either mentoring or coaching intervention programs for physicians, excluding studies with the objective of developing specific clinical skills. We included only studies of physicians who had completed training. We excluded systematic or narrative reviews, program overviews, conference abstracts, opinion pieces, and protocols. Screening was performed using Rayyan, a freely available online screening tool. Two reviewers conducted independent blinded screening on title and abstract. After the initial independent decisions, two reviewers met to review records with conflicting decisions. The full text review was screened by one reviewer, and any uncertainties discussed with a second reviewer.
DATA EXTRACTION AND QUALITY ASSESSMENT
We created a data extraction table to gather data on objectives, interventions, length of intervention, participants, settings, outcome, instruments, and key findings. Data extraction was performed by one reviewer and verified by a second reviewer. Quality assessment was measured by study type (quantitative, qualitative, or mixed methods). We assessed quantitative studies using the National Heart, Lung, and Blood Institutes’ study quality assessment tools, based on the study methodology. We assessed qualitative studies using the Critical Appraisal Skills Programme (CASP) Qualitative Checklist. Mixed method studies were assessed using both quality assessment tools and the average reviewer rating. Two reviewers independently rated each study; conflicting ratings were discussed to reach consensus.
Results
STUDY SELECTION
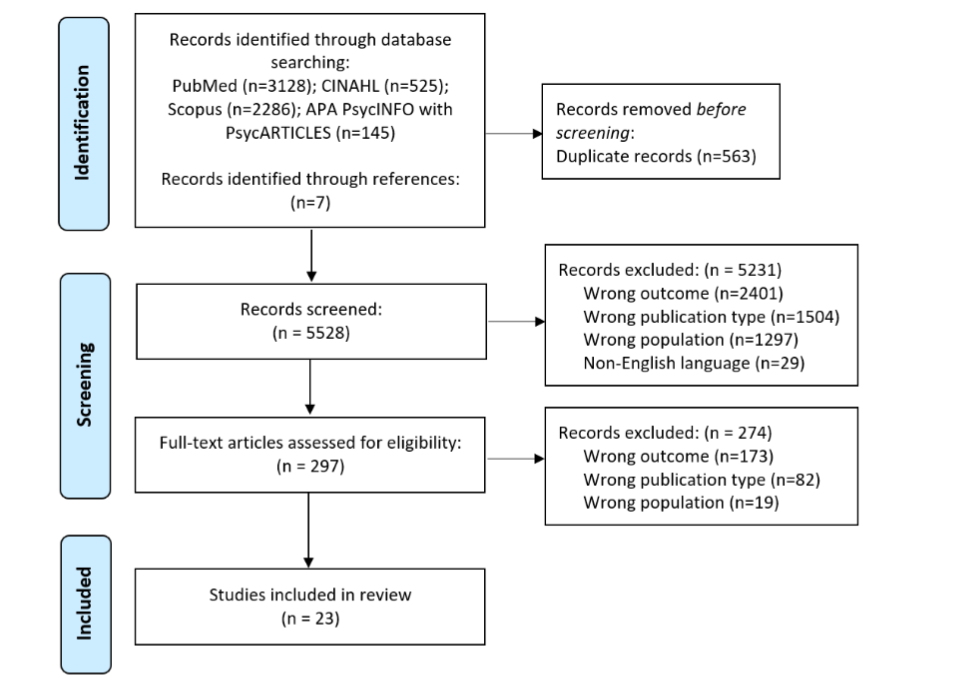
As shown in Figure 1 once duplicates were removed, 5528 records were screened based on title and abstract. After the initial screen, we reviewed 297 full text articles. The most common reason for full text article exclusion was wrong outcome (n=3593) which included both lack of outcomes (i.e., commentary) and clinical outcomes (i.e., surgical procedure). Among the 297 articles, 23 articles met our inclusion criteria.
STUDY CHARACTERISTICS
Nearly half of the 23 selected articles described U.S. programs and were completed after 2017. Nine studies reported participants’ age; in six of these, the majority of subjects were aged 50 or less (Table 1). Participants’ average years since training, recorded in ten studies, ranged from 2.5 years to 20 years post-residency (Table 2). Thirteen studies recorded neither the age of participants nor their number of years in practice. Although thirteen studies reported a male/female gender breakdown, only three of 23 studies recorded race or marital status data (Table 1). Nine studies involved general practitioners, family physicians, or other primary care physicians and three studies focused on early-career physicians. The number of participants ranged from 9 to 525 with all but four studies occurring within the last decade. Fourteen studies were of “high” or “medium” quality,” based on established quality ratings tools (Table 3). Only six studies used an experimental design, whereas others used a post-intervention survey, cross-sectional survey, or qualitative interviews.
| First Author | Average Age (in years) | Gender (% Female) | Married/In committed relationship (%) | Race (%White) |
|---|---|---|---|---|
| Connor et al | ns | ns | ns | ns |
| Cuaron et al | ns | ns | ns | ns |
| Dyrbye et al | 31-40 yrs (16%) 41-50 yrs (52%) 51-60 yrs (28%) >60 yrs (7%) |
55% | 86% | ns |
| Gardiner et al | 2/3rd 30-50 yrs (from parent study) | 29% overall; 32% intervention |
87% (from parent study) | ns |
| Gordon et al | ns | 55% | ns | 85% |
| Hernandez-Lee et al | ns | ns | ns | ns |
| Lin et al | ns | 44% | ns | 58% |
| Mann et al | ns | ns | ns | ns |
| McGonagle et al | 43 yrs | 79% | ns | ns |
| McKimm et al | 30-50 yrs (100%) | 69% | ns | 76% |
| Menzin et al | <50 yrs (62%) ≥50 yrs (31%) missing (7%) |
70% | ns | ns |
| Saperstein et al | <35 yrs (81%) ≥35 yrs (19%) |
26% | ns | ns |
| Schneider et al | ns | ns | ns | ns |
| Sekerka et al | 43 yrs | 31% | ns | ns |
| Sharieff et al | ns | ns | ns | ns |
| Splig et al | 46 yrs | 35% | ns | ns |
| Steven et al | ns | ns | ns | ns |
| Tietjen et al | ns | ns | ns | ns |
| Tom et al | ns | ns | ns | ns |
| Welch et al | ns | 100% | 72% | ns |
| West et al | ns | 34.0% | ns | ns |
| West et al | <30 yrs (2%) 31-40 yrs (32%) 41-50 yrs (30%) 51-60 yrs (27%) >60 yrs (10%) |
43% | ns | ns |
| Wilkie et al | ns | ns | ns | ns |
| First Author | Average Years Post Residency (in Practice) | Specialty | Proportion of Time in Direct Patient Care | Location of study |
|---|---|---|---|---|
| Connor et al | ns | ns | ns | UK |
| Cuaron et al | ns | Radiation Oncology | ns | USA (NY) |
| Dyrbye et al | 16 yrs | Medicine Family Medicine Pediatrics |
<25% (2%) 25-49% (16%) 50-74% (27%) 75-99% (35%) 100% (20%) |
USA (AZ, FL, MN, WI) |
| Gardiner et al | > 80% in rural practice >5 yrs (from parent study) |
General Practice | 79% >7 sessions per week (from parent study) | South Australia |
| Gordon et al | 0% | General Practice Medical Specialist Surgical Specialist Lab-based Specialty Anesthesiology |
ns | UK |
| Hernandez-Lee et al | ≤5 yrs | Family Medicine | ns | Canada |
| Lin et al | median time since residency 2.5 yrs (clinical); 3 yrs (research) | Radiation Oncology | ns | US (NY) |
| Mann et al | ns | General Practice | ns | UK |
| McGonagle et al | 11 yrs | Primary Care | ns | USA (Northeastern) |
| McKimm et al | ns | General Practice | ns | UK |
| Menzin et al | ns | Physicians Nurses Physician Assistants Chaplains Pharmacists Psychologists Social Worker |
ns | USA (NY) |
| Saperstein et al | <10 yrs (63%) ≥10 yrs (37%) |
Family Medicine | “majority” 75% or more | USA Navy |
| Schneider et al | 1st yr resident to “latter stage” | Primary Care | ns | USA (NC) |
| Sekerka et al | 12 yrs | Family Medicine | ns | USA (Ohio) |
| Sharieff et al | ns | ns | ns | ns |
| Splig et al | 14 yrs | Internal Medicine Hematology Palliative Care Neurology Cardiology Geriatrics Endocrinology Physical Medicine and Rehabilitation Nuclear Medicine |
ns | Canada (Ontario) |
| Steven et al | ns | ns | ns | UK |
| Tietjen et al | 2-20 yrs | Primary Care Hospitalists |
ns | USA (Connecticut) |
| First Author | Sample Size (n) | Retention (%) | Participation Proportion (%) | Data collection year(s) | Hospital/clinic system | Quality Assessment Score |
|---|---|---|---|---|---|---|
| Connor et al | 151 | n/a | 69% | 1997 | ns | Low |
| Cuaron et al | 9 | 85% | 100% | May-Dec 2018 | Memorial Sloan Kettering Cancer Center (Academic) | Low |
| Dyrbye et al | 88 | 93% | 12% | Oct 9, 2017-Mar 27, 2018 | Mayo clinic sites; both academic and community practice | High |
| Gardiner et al | 245 | 71% | 64% | around 2000 (from parent study) | Rural general practitioners from South Australia | High |
| Gordon et al | 20 | 90% | ns | 2016-2017 | Community and hospital settings | High |
| Hernandez-Lee et al | 525 | n/a | 7% | Jul 2017 | ns | Low |
| Lin et al | 36 | 89% | 86% | Jul 2020-Jul 2021 | Memorial Sloan Kettering Cancer Center (Academic) | High |
| Mann et al | 14 | 85% | ns | ns | ns | Low |
| McGonagle et al | 58 | 66% | ns | ns | Community-and hospital-based settings | High |
| McKimm et al | 50 | 76% | 54% | Apr 2016-Mar 2017 | ns | Medium |
| Menzin et al | 106 | ns | ns | Oct 2017-Jul 2018 | Northwell Health | Medium |
| Saperstein et al | 186 | n/a | 61% | May 2018 | Military medical service | High |
| Schneider et al | 11 | 100% | 44% | Oct 2012-May 2013 | Duke University Medical Center | Medium |
| Sekerka et al | 13 | 100% | 50% | ns | Case Western Reserve University, School of Medicine | Medium |
| Sharieff et al | 16 | ns | ns | ns | ns | Low |
| Splig et al | 40 | 80% | 15% | Jan-Aug 2019 | The Ottawa Hospital | High |
| Steven et al | 49 | 100% | ns | ns | General practice, hospital, and public health organization | Medium |
| Tietjen et al | 27 | n/a | 69% | 2013 | Western Connecticut Health Network and New Milford Hospitals | Low |
| Tom et al | ns | n/a | ns | 2017-2018 | The Permanente Medical Group | Low |
| Welch et al | 46 | ns | 64% | 2010 | Indiana University Health Methodist Hospital Emergency Medicine | Low |
| West et al | 72 | 97% | 13% | Sep 2010-Jun 2012 | Mayo Clinic | High |
| West et al | 125 | 86% | 21% | Oct 2013-Oct 2014 | Mayo Clinic | High |
| Wilkie et al | 84 | n/a | 46% | Nov-Dec 2017 | ns | Low |
In our review, of the 18 studies that evaluated interventions, 7 were about coaching, 8 mentorship, and 3 peer support. Coaching involves inquiry, encouragement, and accountability to increase self-awareness, motivation, and the capacity to take effective action. Coaches do not need to be physicians or be directly involved in health care. Professional coaching can be tailored to focus on the aspects desired by recipients and can assist individuals in their effort to navigate their professional life, their choices, and the direction of their career. Mentorship is characterized by a relationship in which one individual who is more knowledgeable and experienced guides a less knowledgeable and less experienced individual; it may involve physicians or other individuals with direct experience in the health field. Peer support denotes collegiality among and support from peers. It involves the sharing of knowledge, experience, and emotional and social support between individuals who have common experiences. It is an informal relationship between colleagues.
Of the studies that evaluated interventions (n=18), eleven were ranked high-or medium quality, three employed qualitative or mixed methods design and eight quality studies utilized randomized controlled trial or prospective cohort design. Interventions employed in these studies included onboarding for new physicians, professional or positive psychology coaching sessions, a cognitive behavioral coaching retreat followed by online sessions, junior-senior faculty dyad mentoring using suggested topics, and physician mentoring or coaching provided through health system leadership. Group interventions included small group sessions led by trained physician facilitators, facilitated small group sessions for RNs and physicians lead by various health professionals, a single evidence-based workshop with a follow-up on-line program, and physician small group sessions utilizing a guideline but without a trained (physician) leader.
Five of the included studies used structured core content for mentoring or coaching activities. Key mentoring topics included optimizing meaning in work, integrating personal and professional life, building social support and community at work, improving work efficiency, addressing workload, building leadership skills, pursuing hobbies and recreation, engaging in self-care, and strengthening relationships outside of work. Those studies that utilized a guided program also focused on identifying a vocational purpose and personal strengths, building effective work teams, and dealing with stressors; or on dealing with differences or conflict, medical error, and giving feedback in challenging circumstances. Qualitative studies stressed the importance of boundary-setting and prioritization, self-compassion, and self-awareness among physicians who were being mentored.
Tools used during mentoring/coaching sessions included positive psychology (reframing negative situations, goal setting, simulation of work-related scenarios, mindfulness tools, reflecting on experiences that have brought joy, gratitude tools) and use of validated strengths-based tools (Best-self Tool, Values in Action Assessment, Using Strengths in New Ways Tool).
Three high- or medium-quality studies did not utilize interventions but provided useful perspectives on coaching and mentoring. Gordon et al. studied twenty recent UK medical graduates over six to nine months, performing content analysis of audio-diaries. Respondents identified having a senior colleague as an informal mentor and having peer support as key factors that eased the transition to clinical practice. Saperstein et al. performed a cross-sectional study of 186 Navy family physicians, finding a positive association between having a mentor and job satisfaction. Sekerka et al.’s qualitative study of thirteen family medicine faculty focused on the benefit of coaching to the coaches themselves. The key informants expressed that serving as a peer coach encourages times for reflection and learning and has benefit to personal and professional development.
Nine studies were rated as lower quality studies. This was based on limitations of sample size, unrecorded demographic factors, choice of methodology, or methodologic flaws, but each study was nevertheless instructive. These studies included a qualitative/post-intervention survey of senior United Kingdom mentors (N=151) of junior physicians, a post-intervention survey for new radiation oncologists (N=9) who had completed an onboarding mentorship program, a cross-sectional survey of early-career Canadian family physicians (N=525) exploring respondents’ perceived mentorship needs, a small randomized controlled trial comparing 1:1 and group mentoring for UK physicians with self-identified mentorship needs (N=14), and a post-intervention cohort survey to study the impact of mentoring on participants’ patient experience scores (N=16). Additional lower quality studies used post-intervention or cross-sectional survey methodology to evaluate new physician mentorship programs, to analyze the content and perceived value of a “women in Emergency Medicine” mentorship program, and report the use of a mentorship checklist for new physicians.
| First Author | Purpose/Objective | Study type |
|---|---|---|
| Connor et al | To evaluate the impact of participating in a mentorship training program on senior physicians’ experiences of mentoring junior doctors | Qualitative interviews and post-intervention survey of cohort |
| Cuaron et al | To evaluate physician-reported assessments of an established faculty orientation program for new radiation oncology physicians and to prospectively analyze the effects of an onboarding program based on those assessments | Post-intervention survey of cohort |
| Dyrbye et al | To evaluate improvements in well-being, job satisfaction, resilience, and fulfillment in physicians and burnout from professional coaching intervention | Randomized control trial |
| Gardiner et al | To determine the relationship between cognitive behavioral coaching, the well-being of rural general practitioners (GPs), and intentions to leave | Intervention trial |
| Gordon et al | To explore trainee doctors’ experiences of the transition to trained doctor. Research questions were 1) What multiple and multidimensional transitions are experienced as participants move from trainee to trained doctor? 2) What facilitates/hinders doctors’ successful transition experiences? 3) What is the impact of these transitions on doctors? | Qualitative interviews and content analyses of respondents’ audio diaries of cohort |
| Hernandez-Lee et al | To explore the need for mentorship in early-career family physicians | Cross-sectional survey |
| Lin et al | To evaluate differences in satisfaction with mentorship for clinical and research junior faculty and the relative importance of mentoring program components | Pre- and post-intervention survey of cohort; content analysis of focus group interviews |
| Mann et al | To explore the use of an action learning approach to mentoring of physicians, by comparing one-to-one mentoring or a group mentoring scheme | Randomized control trial |
| McGonagle et al | To investigate the impact of a positive psychology-based coaching on primary care physicians’ personal and work-related well-being, stress, and burnout | Randomized control trial |
| McKimm et al | To assess the impact of a confidential coaching program for retention of GPs who are at risk for leaving the profession or recently returned to practice | Pre- and post-intervention surveys of cohort |
| Menzin et al | To assess the effect of a faculty development program (Mentoring and Professionalism in Training [MAP-IT]) that fosters humanism in medicine on elements of burnout and the development of resilience | Pre- and post-intervention surveys of cohort |
| Saperstein et al | To examine whether having a mentor is associated with positive job satisfaction among Navy family physicians | Cross-sectional survey |
| Schneider et al | To evaluate the perceived impact of Physician Well-being Coaching on physician stress and resiliency | Qualitative interviews |
| Sekerka et al | To identify perceived benefits coaches received from a coaching encounter and how this relates to their own process of professional development | Qualitative interviews |
| Sharieff et al | To investigate processes that would engender and sustain improvement in individual physician experience scores | Post-intervention survey of cohort |
| Splig et al | To assess the impact of the SMART program on academic physicians’ levels of resilience, subjective happiness, stress, and anxiety | Randomized control trial |
| Steven et al | To investigate National Health Service doctors’ perceived benefits of being involved in mentoring schemes and explore overlaps between areas of benefit | Qualitative interviews |
| Tietjen et al | To determine physicians’ reasons for participating in a physician mentoring program, evaluate the program, and recommendations for improvement | Post-intervention survey of cohort |
| Tom et al | To evaluate and improve use of a competencies-based mentoring checklist to help new physicians understand the basic work environment and resources in their daily jobs as well as achieve needed competencies | Post-intervention survey of cohort |
| Welch et al | To describe the content, perceived value, and ongoing achievements of the “Women in Emergency Medicine Mentoring Program” | Post-intervention survey of cohort |
| West et al | To test the hypothesis that an intervention involving a facilitated physician small group curriculum would result in improvement in well-being | Randomized control trial |
| West et al | To evaluate physician small groups to promote physician well-being in a scenario with provided discussion topics but without trained facilitators, without protected time for participants | Randomized control trial |
| Wilkie et al | To support the implementation of an organizational framework for physician wellness | Cross-sectional survey |
Of the studies that evaluated interventions (n=18), eleven were ranked high-or medium quality, three employed qualitative or mixed methods design and eight quality studies utilized randomized controlled trial or prospective cohort design. Interventions employed in these studies included onboarding for new physicians, professional or positive psychology coaching sessions, a cognitive behavioral coaching retreat followed by online sessions, junior-senior faculty dyad mentoring using suggested topics, and physician mentoring or coaching provided through health system leadership. Group interventions included small group sessions led by trained physician facilitators, facilitated small group sessions for RNs and physicians lead by various health professionals, a single evidence-based workshop with a follow-up on-line program, and physician small group sessions utilizing a guideline but without a trained (physician) leader.
Five of the included studies used structured core content for mentoring or coaching activities. Key mentoring topics included optimizing meaning in work, integrating personal and professional life, building social support and community at work, improving work efficiency, addressing workload, building leadership skills, pursuing hobbies and recreation, engaging in self-care, and strengthening relationships outside of work. Those studies that utilized a guided program also focused on identifying a vocational purpose and personal strengths, building effective work teams, and dealing with stressors; or on dealing with differences or conflict, medical error, and giving feedback in challenging circumstances. Qualitative studies stressed the importance of boundary-setting and prioritization, self-compassion, and self-awareness among physicians who were being mentored.
Tools used during mentoring/coaching sessions included positive psychology (reframing negative situations, goal setting, simulation of work-related scenarios, mindfulness tools, reflecting on experiences that have brought joy, gratitude tools) and use of validated strengths-based tools (Best-self Tool, Values in Action Assessment, Using Strengths in New Ways Tool).
Three high- or medium-quality studies did not utilize interventions but provided useful perspectives on coaching and mentoring. Gordon et al. studied twenty recent UK medical graduates over six to nine months, performing content analysis of audio-diaries. Respondents identified having a senior colleague as an informal mentor and having peer support as key factors that eased the transition to clinical practice. Saperstein et al. performed a cross-sectional study of 186 Navy family physicians, finding a positive association between having a mentor and job satisfaction. Sekerka et al.’s qualitative study of thirteen family medicine faculty focused on the benefit of coaching to the coaches themselves. The key informants expressed that serving as a peer coach encourages times for reflection and learning and has benefit to personal and professional development.
Nine studies were rated as lower quality studies. This was based on limitations of sample size, unrecorded demographic factors, choice of methodology, or methodologic flaws, but each study was nevertheless instructive. These studies included a qualitative/post-intervention survey of senior United Kingdom mentors (N=151) of junior physicians, a post-intervention survey for new radiation oncologists (N=9) who had completed an onboarding mentorship program, a cross-sectional survey of early-career Canadian family physicians (N=525) exploring respondents’ perceived mentorship needs, a small randomized controlled trial comparing 1:1 and group mentoring for UK physicians with self-identified mentorship needs (N=14), and a post-intervention cohort survey to study the impact of mentoring on participants’ patient experience scores (N=16). Additional lower quality studies used post-intervention or cross-sectional survey methodology to evaluate new physician mentorship programs, to analyze the content and perceived value of a “women in Emergency Medicine” mentorship program, and report the use of a mentorship checklist for new physicians.
Discussion
Previous systematic reviews evaluated the prevalence of burnout in physicians, presented evidence that burnout is associated with safety-related quality of care and explored physicians’ perspectives about organizational, contextual, relational and individual factors that mitigate against burnout. Meta-analyses have affirmed the importance of organization-directed and physician-directed burnout interventions, including psychosocial skills and mindfulness training for physicians. In contrast, limited studies have explored strategies to improve satisfaction and well-being for physicians that address organizational or system factors. Our systematic review has uncovered more than a dozen quality studies that, taken together, clearly demonstrate the value and promise of mentoring/coaching/peer group meetings in enhancing physician wellbeing. However, it is difficult to draw conclusions or make recommendations based on these 23 studies due to their heterogeneity of the purpose, design, and outcomes. Of special concern is the issue of the early-career physician. Although we initially focused our review on this population alone, we found only three relevant studies of early-career physicians. The narrowness of Lin et al.’s prospective cohort (junior faculty mentees from a single specialty) limits the application of that study’s findings. The qualitative methodology of Hernandez-Lee et al. and Gordon et al. is exploratory rather than definitive. And yet, given that over a quarter of early career physicians report burnout, a strong mentoring focus for early career physicians seems vital. Sparse information was provided on study participants’ characteristics. Specifically, half of the studies provided information on number of years in practice and only three reported the proportion of time the participants engaged in direct patient care. Similarly, only three studies indicated the race of participants, about one third indicated age and half indicated sex. Absence of this information limited a more comprehensive understanding of this topic.
Cordova et al. has proposed a developmental model for physician resilience training, beginning in the preclinical years and extending throughout the physician lifecycle. The model affirms attentional practices including mindfulness; the necessity of healthy lifestyles and behaviors; the importance of building safe and diverse workplaces; the value of reflective practice and conflict management. It underscores the need to lead clinical teams well, to give and receive feedback, to recognize and address burnout, and to transition to a role in advocating policy and systems change. Shanafelt and Noseworthy have outlined organizational strategies to promote physician engagement and prevent physician burnout. Their nine strategies include emphases on harnessing the power of leadership, cultivating community at work, promoting flexibility and work-life integration, and providing resources to promote resilience and self-care. Our systematic review’s studies complement Shanafelt and Noseworthy’s work by including a variety of employable, effective 1:1 and group strategies for physicians, but these require institutional support and funding. At issue are several key questions for system leaders and researchers: How will the healthcare system balance financial outlays necessary for programmatic support with future perceived gain? Are less costly interventions such as formalized and approved peer group meetings effective enough to justify their widespread use, and when should more costly but possibly more effective formal mentoring and coaching interventions be employed? Clearly, more study of and emphasis on peer coaching and senior-junior partner mentorship, employed especially for new physicians, is needed to answer these vital questions.
Conclusion
Rigorous data validating the value of mentorship, including the best approach to be used (coaching, mentorship, or peer support) is lacking. However, a growing database of quality studies, sufficient to justify additional studies of mentoring in early- and mid-career physicians, affirms physician mentoring as central to physician retention and wellbeing. Although sparse evidence supports one particular type of program over another (i.e., coaching, mentoring, or peer group support), each one of these programs, as described in this systematic review, reported positive outcomes. The trifecta for effective healthcare encompasses improved care for the patient, better population health, and reduced healthcare costs. Given the overwhelming evidence of mental ill-health, burnout, and reduced retention among healthcare professionals, all three of these goals rest on improving well-being, satisfaction and flourishing among healthcare professionals and instituting a well-being program can aid in that endeavor.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Acknowledgements. This study was performed in collaboration with the CoxHealth (Springfield, MO) and University of Missouri Rural Health Research Center.
References
- Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav. 1981;2(2):99-113. doi:10.1002/job.4030020205
- Hodkinson A, Zhou A, Johnson J, et al. Associations of physician burnout with career engagement and quality of patient care: systematic review and meta-analysis. BMJ. 2022;378:e070442. doi:10.1136/bmj-2022-070442
- West CP, Dyrbye LN, Sinsky C, et al. Resilience and burnout among physicians and the general US working population. JAMA Netw Open. 2020;3(7):e209385. doi:10.1001/jamanetworkopen.2020.9385
- Baxter SL, Saseendrakumar BR, Cheung M, et al. Association of electronic health record inbasket message characteristics with physician burnout. JAMA Netw Open. 2022;5(11):e2244363. doi:10.1001/jamanetworkopen.2022.44363
- Dillon EC, Tai-Seale M, Meehan A, et al. Frontline perspectives on physician burnout and strategies to improve well-being: interviews with physicians and health system leaders. J Gen Intern Med. 2020;35(1):261-267. doi:10.1007/s11606-019-05381-0
- Abbasi J. Pushed to their limits, 1 in 5 physicians intends to leave practice. JAMA. 2022;327(15):1435-1437. doi:10.1001/jama.2022.5074
- Dyrbye L, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ. 2016;50(1):132-149. doi:10.1111/medu.12927
- Dyrbye LN, Burke SE, Hardeman RR, et al. Association of clinical specialty with symptoms of burnout and career choice regret among US resident physicians. JAMA. 2018;320(11):1114-1130. doi:10.1001/jama.2018.12615
- Ricker M, Maizes V, Brooks AJ, Lindberg C, Cook P, Lebensohn P. A longitudinal study of burnout and well-being in family medicine resident physicians. Fam Med. 2020;52(10):716-723. doi:10.22454/FamMed.2020.179585
- Monrouxe LV, Bullock A, Tseng HM, Wells SE. Association of professional identity, gender, team understanding, anxiety and workplace learning alignment with burnout in junior doctors: a longitudinal cohort study. BMJ Open. 2017;7(12):e017942. doi:10.1136/bmjopen-2017-017942
- Sherlock C, John C. Adaptation practice: Teaching doctors how to cope with stress, anxiety and depression by developing resilience. British Journal of Medical Practitioners. 2016;9(2):916-923.
- Rosta J, Aasland OG, Nylenna M. Changes in job satisfaction among doctors in Norway from 2010 to 2017: a study based on repeated surveys. BMJ Open. 2019;9(9):e027891. doi:10.1136/bmjopen-2018-027891
- Hariharan TS, Griffin B. A review of the factors related to burnout at the early-career stage of medicine. Med Teach. 2019;41(12):1380-1391. doi:10.1080/0142159x.2019.1641189
- Wu Y, Wu M, Wang C, Lin J, Liu J, Liu S. Evaluating the prevalence of burnout among health care professionals related to electronic health record use: systematic review and meta-analysis. JMIR Med Inform. 2024;12:e54811. doi:10.2196/54811
- Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care: results from the MEMO Study. J Am Med Inform Assoc. 2014;21(e1):e100-106. doi:10.1136/amiajnl-2013-001875
- Linzer M, Manwell LB, Williams ES, et al. Working conditions in primary care: physician reactions and care quality. Ann Intern Med. 2009;151(1):28-36, w26-29. doi:10.7326/0003-4819-151-1-200907070-00006
- Rabatin J, Williams E, Baier Manwell L, Schwartz MD, Brown RL, Linzer M. Predictors and outcomes of burnout in primary care physicians. J Prim Care Community Health. 2016;7(1):41-43. doi:10.1177/2150131915607799
- Kang C, Sarkar IN. Interventions to reduce electronic health record-related burnout: a systematic review. Appl Clin Inform. 2024;15(1):10-25. doi:10.1055/a-2203-3787
- Sullivan AB, Davin SA, Lapin B, et al. Effects of flexible scheduling and virtual visits on burnout for clinicians: 1-year follow-up. Mult Scler Relat Disord. 2023;75:104721. doi:10.1016/j.msard.2023.104721
- Prasad K, Poplau S, Brown R, et al. Time pressure during primary care office visits: a prospective evaluation of data from the healthy work place study. J Gen Intern Med. 2020;35(2):465-472. doi:10.1007/s11606-019-05343-6
- Sambunjak D, Straus SE, Marusic A. Mentoring in academic medicine: a systematic review. JAMA. 2006;296(9):1103-1115. doi:10.1001/jama.296.9.1103
- Wright WR, Jr., Dirsa AE, Martin SS. Physician mentoring: a process to maximize the success of new physicians and enhance synchronization of the group. J Med Pract Manage. 2002;18(3):133-137.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
- National Heart Lung and Blood Institute. Study quality assessment tools. National Institutes of Health. Accessed April 15, 2023. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
- Critical Appraisal Skills Programme. CASP: Qualitative Checklist. Accessed November 10, 2022. https://casp-uk.net/images/checklist/documents/CASP-Qualitative-Studies-Checklist/CASP-Qualitative-Checklist-2018_fillable_form.pdf
- Connor MP, Bynoe AG, Redfern N, Pokora J, Clarke J. Developing senior doctors as mentors: a form of continuing professional development. Report of an initiative to develop a network of senior doctors as mentors: 1994-99. Med Educ. 2000;34(9):747-753. doi:10.1046/j.1365-2923.2000.00630.x
- Cuaron JJ, Gillespie EF, Gomez DR, Khan AJ, Mychalczak B, Cahlon O. From orientation to onboarding: a survey-based departmental improvement program for new radiation oncology faculty physicians. JCO Oncol Pract. 2020;16(4):e395-e404. doi:10.1200/JOP.19.00641
- Gordon L, Jindal-Snape D, Morrison J, et al. Multiple and multidimensional transitions from trainee to trained doctor: a qualitative longitudinal study in the UK. BMJ Open. 2017;7(11):e018583. doi:10.1136/bmjopen-2017-018583
- Mann R, Ball K, Watson G. Mentoring for NHS general practitioners: a prospective pilot study of an action learning approach. Educ Prim Care. 2011;22(4):235-240. doi:10.1080/14739879.2011.11494006
- McKimm J, Povey J. Evaluating the impact of a coaching pilot on the resilience and retention of UK general practitioners. BMJ Leader. 2018;2(4):144-148. doi:10.1136/leader-2018-000089
- Menzin AW, Kline M, George C, Schindler J, Yacht AC, Fornari A. Toward the Quadruple Aim: impact of a humanistic mentoring program to reduce burnout and foster resilience. Mayo Clin Proc Innov Qual Outcomes. 2020;4(5):499-505. doi:10.1016/j.mayocpiqo.2020.05.001
- Sharieff GQ. MD to MD coaching: improving physician-patient experience scores: what works, what doesn’t. J Patient Exp. 2017;4(4):210-212. doi:10.1177/2374373517715008
- Steven A, Oxley J, Fleming WG. Mentoring for NHS doctors: perceived benefits across the personal-professional interface. J R Soc Med. 2008;101(11):552-557. doi:10.1258/jrsm.2008.080153
- Tom W, Tom W, Albarran D, Salman N, Van Groenou A. Ensuring mentorship of new physicians in their first year: constructs for new mentoring processes. Perm J. 2019;23. doi:10.7812/tpp/18-122
- Welch JL, Jimenez HL, Walthall J, Allen SE. The women in emergency medicine mentoring program: an innovative approach to mentoring. J Grad Med Educ. 2012;4(3):362-366. doi:10.4300/jgme-d-11-00267.1
- West CP, Dyrbye LN, Rabatin JT, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174(4):527-533. doi:10.1001/jamainternmed.2013.14387
- West CP, Dyrbye LN, Satele DV, Shanafelt TD. Colleagues Meeting to Promote and Sustain Satisfaction (COMPASS) groups for physician well-being: a randomized clinical trial. Mayo Clin Proc. 2021;96(10):2606-2614. doi:10.1016/j.mayocp.2021.02.028
- Wilkie T, Tajirian T, Stergiopoulos V. Advancing physician wellness, engagement and excellence in a mental health setting: a Canadian perspective. Health Promot Int. 2022;37(1). doi:10.1093/heapro/daab061
- Tietjen P, Griner PF. Mentoring of physicians at a community-based health system: preliminary findings. J Hosp Med. 2013;8(11):642-643. doi:10.1002/jhm.2094
- Dyrbye LN, Shanafelt TD, Gill PR, Satele DV, West CP. Effect of a professional coaching intervention on the well-being and distress of physicians: a pilot randomized clinical trial. JAMA Intern Med. 2019;179(10):1406-1414. doi:10.1001/jamainternmed.2019.2425
- Sekerka LE, Chao J. Peer coaching as a technique to foster professional development in clinical ambulatory settings. J Contin Educ Health Prof. 2003;23(1):30-37. doi:10.1002/chp.1340230106
- Gardiner M, Kearns H, Tiggemann M. Effectiveness of cognitive behavioural coaching in improving the well-being and retention of rural general practitioners. Aust J Rural Health. 2013;21(3):183-189. doi:10.1111/ajr.12033
- Saperstein AK, Viera AJ, Firnhaber GC. Mentorship and job satisfaction among Navy family physicians. Mil Med. 2012;177(8):883-888. doi:10.7205/milmed-d-11-00362
- McGonagle AK, Schwab L, Yahanda N, et al. Coaching for primary care physician well-being: A randomized trial and follow-up analysis. J Occup Health Psychol. 2020;25(5):297-314. doi:10.1037/ocp0000180
- Hernandez-Lee J, Pieroway A. Mentorship for early career family physicians: is there a role for the first five years in family practice committee and the CFPC? Can Fam Physician. 2018;64(11):861-862.
- Lin D, Gomez DR, Zhang YH, et al. Radiation Oncology AcaDemic Mentorship Program (ROADMAP) for junior faculty: one-year results of a prospective single institution initiative. Int J Radiat Oncol Biol Phys. 2022;114(1):21-29. doi:10.1016/j.ijrobp.2022.05.012
- Schneider S, Kingsolver K, Rosdahl J. Physician coaching to enhance well-being: a qualitative analysis of a pilot intervention. Explore (NY). 2014;10(6):372-379. doi:10.1016/j.explore.2014.08.007
- Spilg EG, Kuk H, Ananny L, et al. The impact of Stress Management and Resilience Training (SMART) on academic physicians during the implementation of a new Health Information System: An exploratory randomized controlled trial. PLoS One. 2022;17(4):e0267240. doi:10.1371/journal.pone.0267240
- Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA. 2018;320(11):1131-1150. doi:10.1001/jama.2018.12777
- Dewa CS, Loong D, Bonato S, Trojanowski L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open. 2017;7(6):e015141. doi:10.1136/bmjopen-2016-015141
- Sibeoni J, Bellon-Champel L, Mousty A, Manolios E, Verneuil L, Revah-Levy A. Physicians’ Perspectives About Burnout: a Systematic Review and Metasynthesis. J Gen Intern Med. 2019;34(8):1578-1590. doi:10.1007/s11606-019-05062-y
- Norful AA, Brewer KC, Cahir KM, Dierkes AM. Individual and organizational factors influencing well-being and burnout amongst healthcare assistants: A systematic review. Int J Nurs Stud Adv. 2024;6:100187. doi:10.1016/j.ijnsa.2024.100187
- Alobayli F, O’Connor S, Holloway A, Cresswell K. Electronic health record stress and burnout among clinicians in hospital settings: a systematic review. Digit Health. 2023;9:20552076231220241. doi:10.1177/20552076231220241
- Engel T, Gowda D, Sandhu JS, Banerjee S. Art interventions to mitigate burnout in health care professionals: a systematic review. Perm J. 2023;27(2):184-194. doi:10.7812/tpp/23.018
- West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272-2281. doi:10.1016/S0140-6736(16)31279-X
- Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195-205. doi:10.1001/jamainternmed.2016.7674
- De Simone S, Vargas M, Servillo G. Organizational strategies to reduce physician burnout: a systematic review and meta-analysis. Aging Clin Exp Res. 2021;33(4):883-894. doi:10.1007/s40520-019-01368-3
- McKinley N, Karayiannis PN, Convie L, Clarke M, Kirk SJ, Campbell WJ. Resilience in medical doctors: a systematic review. Postgrad Med J. 2019;95(1121):140-147. doi:10.1136/postgradmedj-2018-136135
- Fox S, Lydon S, Byrne D, Madden C, Connolly F, O’Connor P. A systematic review of interventions to foster physician resilience. Postgrad Med J. 2018;94(1109):162-170. doi:10.1136/postgradmedj-2017-135212
- Scheepers RA, Emke H, Epstein RM, Lombarts K. The impact of mindfulness-based interventions on doctors’ well-being and performance: A systematic review. Med Educ. 2020;54(2):138-149. doi:10.1111/medu.14020
- Naehrig D, Schokman A, Hughes JK, Epstein R, Hickie IB, Glozier N. Effect of interventions for the well-being, satisfaction and flourishing of general practitioners-a systematic review. BMJ Open. 2021;11(8):e046599. doi:10.1136/bmjopen-2020-046599
- Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451. doi:10.1097/ACM.0000000000000134
- Cordova MJ, Gimmler CE, Osterberg LG. Foster well-being throughout the career trajectory: a developmental model of physician resilience training. Mayo Clin Proc. 2020;95(12):2719-2733. doi:10.1016/j.mayocp.2020.05.002
- Shanafelt TD, Noseworthy JH. Executive leadership and physician well-being: nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129-146. doi:10.1016/j.mayocp.2016.10.004