





Post-Operative OCT and OCTA in Macular Hole Surgery
Post-operative role of OCT and OCTA in the evaluation of idiopathic macular hole surgery, anatomic versus functional success. A review article
Ahmed Darwish MD.1
- Prof. of Ophthalmology, Ain Shams University, Egypt.
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Darwish, A., 2025. Post-operative role of OCT and OCTA in the evaluation of idiopathic macular
hole surgery; anatomic versus functional success. A review article. Medical Research Archives, [online]
13(10). https://doi.org/10.18103/mra.v 13i10.7015
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original author and
source are credited.
DOI https://doi.org/10.18103/mra.v 13i10.7015
ISSN 2375-1924
ABSTRACT
Purpose: To evaluate the role of OCT and OCTA as prognostic tools in the evaluation of the results of idiopathic macular hole surgery from the anatomical and functional points of view.
Methods: This is a review article gathering the conclusions of many articles in the literature discussing this important issue.
Results: The integrity of the external limiting membrane and the ellipsoid zone were found to be the most important prognostic criteria for visual recovery. A U-type shape pattern of closure and a flat closed closure were also associated with a favorable visual gain. On the other hand, retinal displacement following surgery may be responsible for post operative residual metamorphopsia. A foveal hyper-reflective lesion during the healing process and age-related sub foveal deposits are poor prognostic signs for visual improvement. An early post operative appearance of a foveal detachment, outer foveolar defects or signs of a dissociated optic nerve fiber layer were not found to be important signs in the determination of the final post operative visual acuity.
Conclusion: OCT and OCTA proved to be very beneficial in the evaluation of the macular status following successful macular hole (MH) surgery and in linking the anatomic success criteria to the expected functional status.
Keywords: OCT – OCTA – idiopathic macular hole – macular hole closure – macular hole surgery – vitrectomy.
1. Introduction
Idiopathic macular hole surgery has been greatly refined in the past few years with high primary rate of anatomical closure reaching up to 90% in several studies. The degree of functional improvement, however, showed variable results¹. Through OCT and OCTA, this study comprehensively reviewed the post successful macular hole surgery changes in retinal and choroidal morphology, linking each morphologic finding to its effect on the final visual function.
2. Post-operative role of OCT: anatomic versus functional success criteria
It was found suitable to divide the OCT tomographic signs analyzed in this review according to the involved portion of the retina into:
“external retinal layers” (Fig 1) including, the four hyper-reflective outer lines on SD-OCT: the external limiting membrane (ELM); the inner segment ellipsoid zone (EZ); the cone outer segment tips (COST) or interdigitation zone (IZ); and the retinal pigment epithelium (RPE)
and “inner retinal layers” including all the structures between the internal limiting membrane (ILM) and the external limiting membrane (ELM) namely, the retinal nerve fiber layer (RNFL), the ganglion cell layer (GCL) and the inner plexiform layer (IPL)².
2.1. OUTER RETINAL LAYERS
Successful macular hole surgery (MHS) is followed by sequential restoration of the external limiting membrane (ELM) and ellipsoid zone (EZ). Reconstruction of the foveal ELM precedes restoration of EZ⁴. It is believed that intact ELM is mandatory for the restoration of the EZ⁵. Restoration of EZ is necessary for visual improvement as visual results are significantly better in eyes with restored EZ than in those with disrupted EZ³.
A grading system showing the degree of restoration of the ELM and EZ (fig 2) was developed as follows³:
a) Grade 0: macular hole has closed, but the ELM and EZ are discontinuous (arrow). Normal foveal contour has been restored.
b) Grade 1: macular hole has closed with complete restoration of the ELM. EZ defect persists (arrow) (defect length: 51 µm).
c) Grade 2: macular hole has closed and both the ELM and EZ have been restored³.
➤ In the postoperative period, the ELM, EZ, and COST line get restored in 100%, 69%, and 17% of eyes, respectively. Foveal reconstruction after successful closure of FTMH depended on a fine balance between the proliferating glial and Muller cells and the centripetal bridging of ELM. This is usually followed by subsequent reapproximation of the normal photoreceptors to the central fovea. This is a slow but progressive process and takes place in the first 6 months after the surgical procedure⁷.
➤ Before the process gets completed, three different tomographic signs can be recognized in the foveal area;
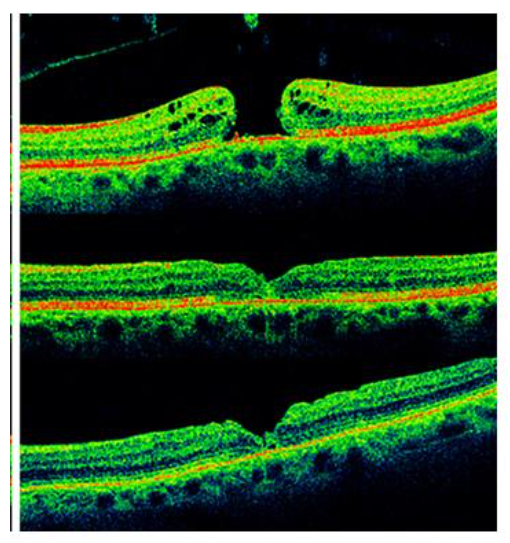
Fig 1: SD-OCT scan showing a small operculum on the roof of the macular hole. Bottom right magnification of the scan showing a detail of the four external retinal layers².
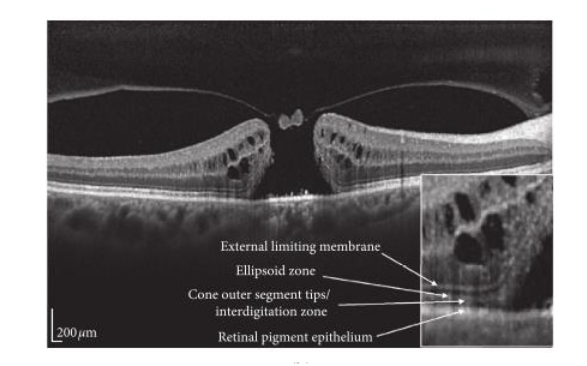
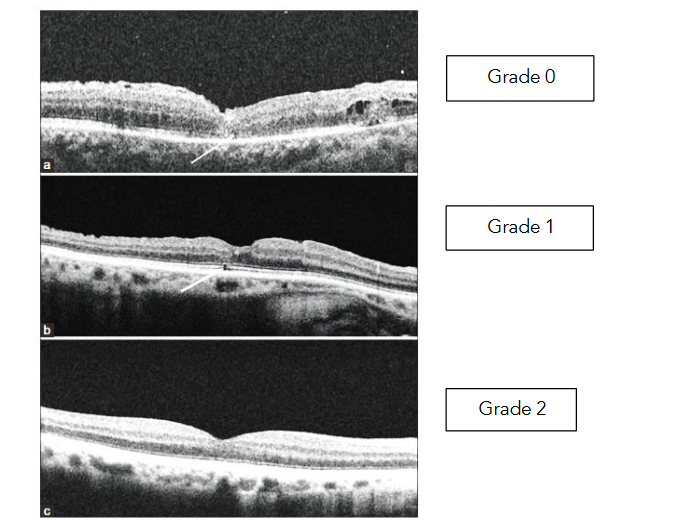
Fig 2: Successful macular hole surgery grading system, highlighting the healing of the ELM and EZ in SD-OCT images:
a). First, a foveal detachment (Fig 3) can persist in the first months in up to 43% of closed MHs, suggesting that bridging of the inner neuroretinal tissue may be the initial step in MH repair⁸˒⁹.
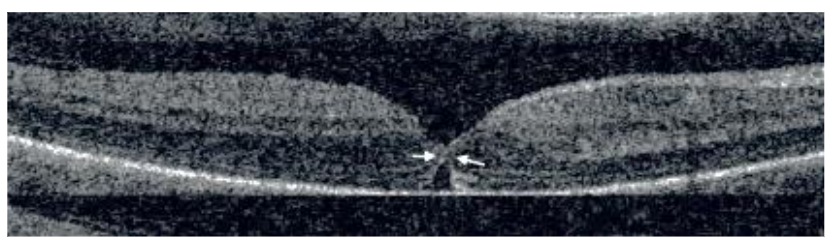
Fig 3: Foveal detachment following successful macular hole surgery¹⁰.
b). Secondarily, outer foveolar defects (OFDs) (Fig 4) also called “foveolar lucencies,” or “foveolar cysts,” can be transiently recognized in the early postoperative follow up in about 26% of patients undergoing successful macular hole surgery and were more observed with smaller preoperative MH. They occur with and without indocyanine green–assisted internal limiting membrane peeling. Earlier disappearance of the foveolar lucency does not correlate with the type of gas used for tamponade. They gradually decrease and eventually resolve with time without additional surgical intervention and with further improvement of visual acuity. They disappear between one and eleven months after the surgery. Recently, the development of these lesions has been interpreted as a normal state of recovery after MH repair, associated with a more favorable surgical outcome and need only follow up and patient reassurance¹¹.
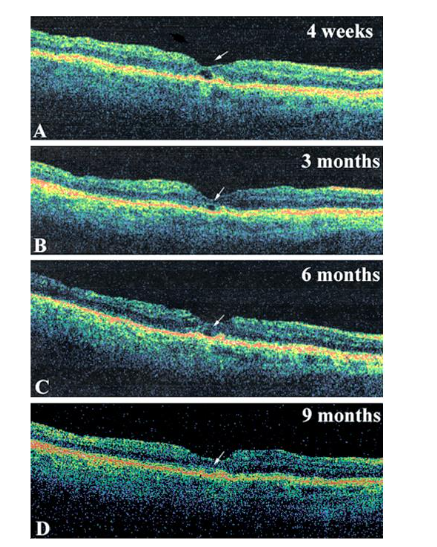
c). Finally, a foveal hyper-reflective lesion (Fig 5) was noticed, formed of a cluster of proliferative glial cells (Müller cells or astrocytes), reapproximating the normal photoreceptors to the central fovea. The persistence of this (glial seal) for a long time postoperatively was associated with worse visual recovery because if the foveal defect is filled by the proliferating glial cells before the bridging of the ELM takes place, reestablishment of EZ at the central fovea will be impeded¹².
Age related subfoveal deposits (Fig 6): Better visual outcomes and earlier recovery of ELM and/or EZ were achieved in younger age subgroups after surgery. This can be explained by the fact that in older age there is:
- Impaired ionic calcium homeostasis which underlies the increased susceptibility of neurons to damage and decrease their ability to regenerate.
- Failing of subretinal macrophages in the aged retina with the accumulation of debris in them formed mainly of lipoproteins and fatty acids from oxidized photoreceptors might lead to diminished regeneration of macular hole induced damaged neurons.
2.2. INNER RETINAL LAYERS
OCT changes in eyes undergoing internal limiting membrane peeling during macular hole surgery: ILM peeling during vitrectomy has become a standard surgical procedure for the treatment of idiopathic MH, as the procedure, as proved by many studies, significantly increases the MH closure rate and lowers the recurrence rate.
ILM is, however, the basement membrane of Müller cells, the inner barrier of the neural retina, and anatomically adjacent to RNFL and GCL which poses a great challenge for the surgeon not to injure those important structures during the peel to preserve the best of functional visual improvement.
a) Dissociated optic nerve fiber layer:
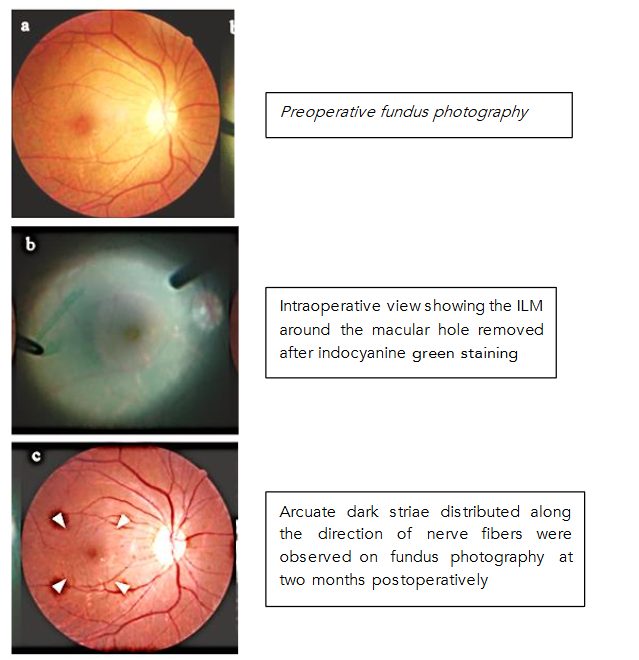
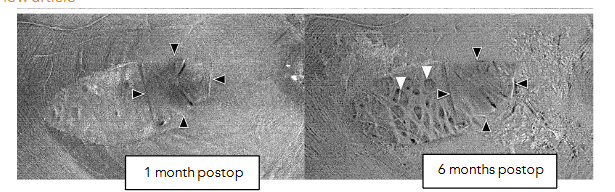
Qualitatively, more than 50% of the eyes that underwent successful MH repair surgery developed alterations named as Dissociated optic nerve fiber layer (DONFL) which appeared on fundus photography as arcuate, slightly dark, extramacular striae along the course of optic nerve fiber.
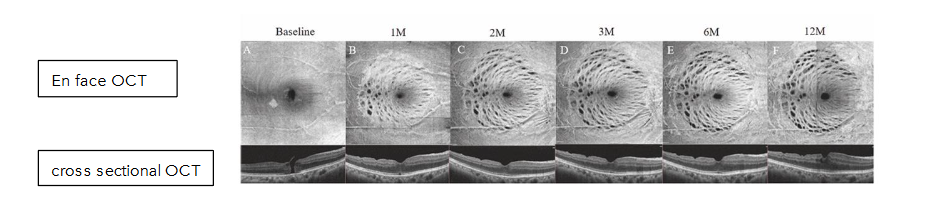
On en face OCT, they appear as multiple dark dots along the course of RNFL, called concentric macular dark spots (CMDSs), and on cross sectional OCT they appear as dimples in the inner retinal layers called dissociated optic nerve fiber layer (DONFL). CMDS were mostly found on the temporal side of the macula within two months after the ILM peeling procedure. The lesion progresses within 6 months after the surgery but remains unchanged after 12 months.
DONFLs do not develop in eyes without ILM peeling and are detectable only in the areas where the ILM peeling was performed. In the temporal inverted ILM flap technique, where a 2-disk diameter ILM is removed from the temporal side of the fovea and inverted to cover the macular hole preserving the nasal ILM in place it was observed that there was a decrease in the area of dissociated optic nerve fiber layer appearance (only limited to the peeled area) with the same anatomical and functional results compared with the original inverted ILM flap technique.
At 1-year postoperative follow-up, the extent and depth of DONFL as diagnosed by OCT were greater on the temporal side of the macula, both as early as 2 months and up to 12 months postoperatively. Several speculations were given to explain this distribution and can be summarized as follows:
- More nerve fibers enter the optic disc from the nasal side than from the temporal side, while there are more glial cells on the temporal side.
- The absence of large blood vessels temporal to the macula decreases the resistance of this area to stretch.
- Within the superior and inferior vascular archades, more branches are present on the temporal side of the macula increasing the susceptibility of this area for the formation of adjacent recesses.
- The temporal nerve fiber layer is thinner, rendering the retinal dimples to be more pronounced.
- After ILM peeling, the fovea in many cases is displaced toward the optic disc, widening the spaces between the RNFL bundles temporal to the macula, making the DONFL more apparent.
Studies have shown that DONFL is not restricted to the RNFL, but can extend to the GCL and IPL. Sabry et al. divided the changes in the inner retina after ILM peeling into CMDS with intact GC-IPL and CMDS with evident localized defects in the underlying GC-IPL based on en face OCT. Kim et al, classified DONFLs into three types: unidirectional, bidirectional, and complicated bidirectional dimples.
b) Changes in the thickness of the inner retinal layers and alterations of their architecture:
Changes in thickness of the RNFL after ILM peeling: It was found that there is an increase in RNFL thickness, only in the area nasal to fovea, where ILM was peeled, 1 month postoperatively, with subsequent reduction in thickness at 6 months postoperatively. This was attributed to the early inflammatory responses with subsequent reduction of thickness secondary to the damage inflicted to the macular retinal nerve fiber layer as a result of ILM peeling.
Changes in GCL thickness after ILM peeling: Ganglion cell layer was found to be the only layer to show thinning in medial and temporal sectors signifying the fact that this layer bears maximum brunt of the maneuver and show significant damage over a large area around the fovea.
GCL thinning can be caused by several postulated theories:
- The loss or alteration of Muller cells in the region of DONFLs secondary to trauma during ILM peeling may be the cause of GCL thinning not the GC death.
- A protein involved in apoptosis (i.e., βA3/A1 crystallin) was identified. This protein was found to be expressed in retinal ganglion cells, speculating that anoikis (apoptosis) of retinal ganglion cells is the cause of GCL thinning following ILM peeling.
It could, therefore, be speculated that the formation of DONFL may be related to GCL-IPL defect, secondary to changes in Muller cells and/or retinal ganglion cells.
Changes in thickness of the other inner retinal layers: There is significant thickening of retina in central, inner, and outer nasal quadrants with maximum contribution from increase in thickness to inner nuclear and IPLs while temporally, significant reduction in retinal thickness was observed, with maximum thinning observed in ganglion cell and IPLs at 3 months post-operatively.
Influence of the type of dye used in macular hole surgery on the above retinal changes: Apart from ICG which has largely been proven to provide a dose and time dependent retinal cytotoxicity, other dyes as Trypan blue (TB) and Brillant Blue has shown a very high biocompatibility with retinal structures. Heavy dyes for macular surgery as Double dyne TM and Twin TM also were proven to be safe.
Correlation between CRT and visual outcome: It was found that an increased CRT at 1 month post successful macular hole surgery was positively correlated with a better visual outcome.
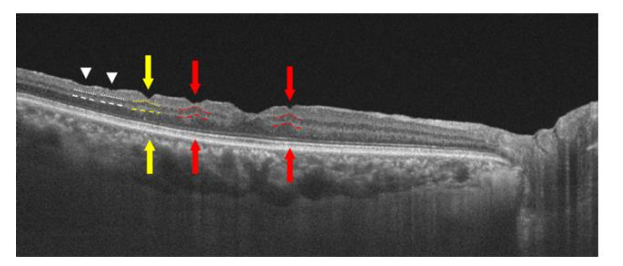
c) Retinal and choroidal displacement:
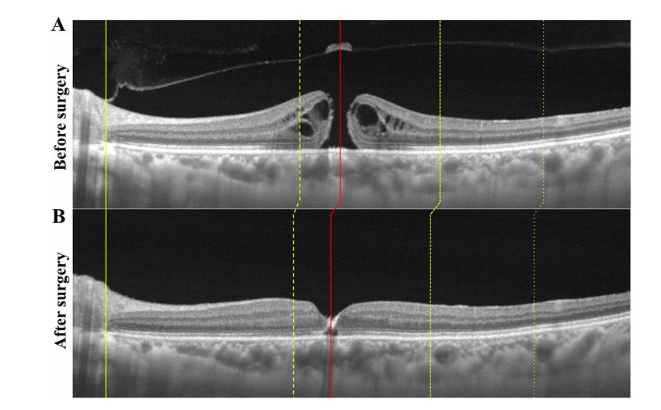
The yellow line indicates the temporal edge of the optic disc, and no displacement was observed after the surgery. The fovea was displaced after the surgery. The choroid was also displaced after the surgery especially in the temporal quadrants. The degree of choroidal displacement was found to be different from the degree of retinal displacement. This effect could be explained as follows:
- The removal of the ILM (which comprises 50% of the retinal rigidity) causes a lack of the structural support of the retina which probably causes the contraction of the nerve fibers (where the ILM was peeled) towards the lamina cribrosa to which the nerve fibers are connected with subsequent displacement of the inner retina toward the optic disc.
- The choriocapillaris is opposed to the outer layer of Bruch’s membrane which adheres to the RPE layer so it is proposed that the choriocapillaris is not displaced from the RPE layer.
- However, there is no adhesive connection between the intermediate choroidal vessels and the choriocapillaris as the choroidal vasculature is embedded in a stroma of collagen and elastic fibers causing a gap in the displacement between the choroid and the retina following the surgery.
This means that the subfoveal choroid following surgery is different as regards thickness and vasculature from that before surgery.
2.3. THE PATTERNS OF POST OPERATIVE MACULAR HOLE CLOSURE BY OCT
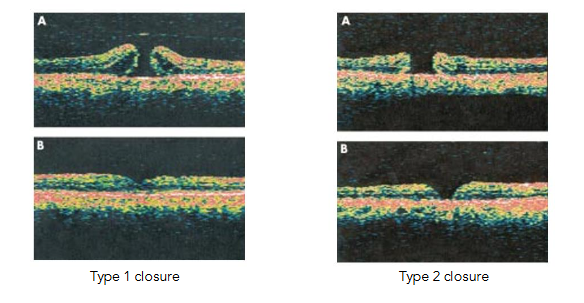
Basically, there are 2 types of macular closure diagnosed post operatively by OCT:
- Type 1 closure indicates that the macular hole is closed with an intact foveal neurosensory retina covering the RPE.
- Type 2 closure indicates that a foveal defect of the neurosensory retina persists postoperatively at the base of the macular hole although the whole rim of the macular hole is attached to the underlying RPE.
Imai et al categorized the successfully repaired macular hole into three patterns with OCT; U-type (normal foveal contour), V-type (steep foveal contour), and W-type (foveal defect of neurosensory retina). Post operative visual acuity was best with the U-type followed by the V-type and worst in the W-type group. Similarly, visual acuity was better in the type 1 group as compared to the type 2 group.
In one study, it was found that the presence of a fluid cuff at the margin of the macular hole facilitates the centripetal movement of retinal tissue towards the fovea increasing the chance of success of a second surgical intervention to close the macular hole as compared to those cases without this fluid cuff.
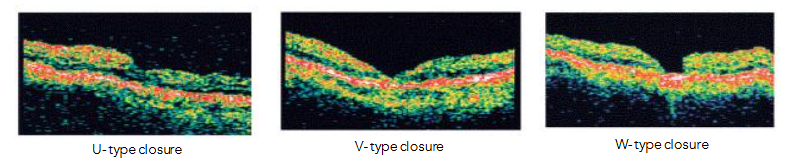
Fig 13:
Type (1) closure may correspond to a U or V pattern, and type 2 closure to a W pattern⁵⁴.
Post operative visual acuity was best with the U-type followed by the V-type and worst in the W-type group⁵⁵. Similarly, visual acuity was better in the type 1 group as compared to the type 2 group⁵⁴.
Tornambe et al⁵⁶ classified the macular state post macular hole surgery into three types fig 14:
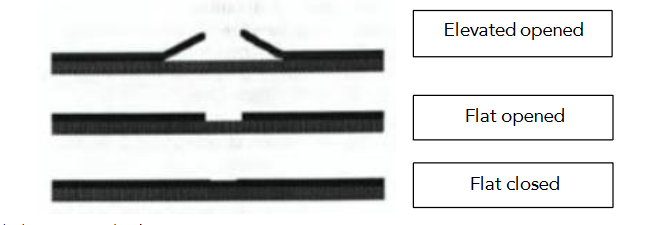
Fig. 14: Macular hole surgery end points
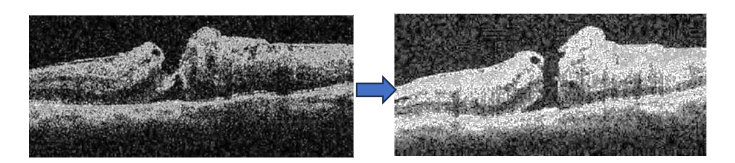
1) Elevated opened: In this type the circular edge of the hole is elevated with fluid under the hole. This type indicates unsuccessful surgery with no improvement in visual acuity.
2) Flat opened: In this type, although the hole is flat against the RPE, yet its edges are visible and separated. This type can be considered as a successful surgery but with moderate visual improvement.
3) Flat closed: In this type, the hole is flat against the RPE and the edges are not visible. Visual acuity is best in this type⁵⁶.
In one study, it was found that the presence of a fluid cuff at the margin of the macular hole facilitates the centripetal movement of retinal tissue towards the fovea increasing the chance of success of a second surgical intervention to close the macular hole as compared to those cases without this fluid cuff⁵⁷˒⁵⁸.
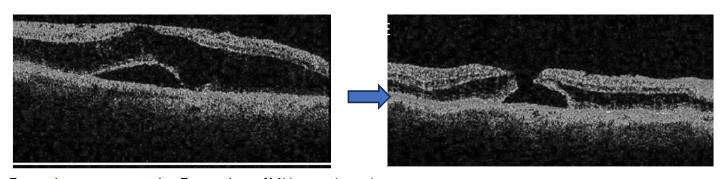
2.4. LATE REOPENING OF PREVIOUSLY REPAIRED MACULAR HOLES
Reopening of macular holes occurs in approximately 5% of cases following successful macular hole surgery. Several mechanisms have been postulated for spontaneous reopening of previously repaired macular holes:
-
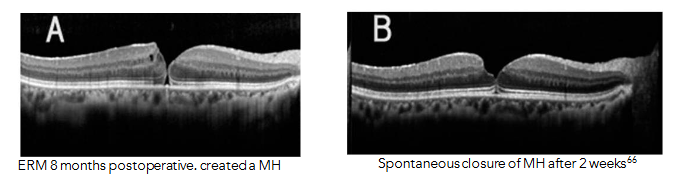
- Tangential tractional type of MH: This occurs secondary to the development of an epiretinal membrane (ERM) which exerts tangential traction on the fovea leading to the development of a MH.
-
- A degenerative process without vitreofoveal traction, in which dehiscence of an umbo of glial tissue, was proposed as one of the steps of full-thickness MH formation.
- The cystoid degeneration type of MH: MH develops in eyes with cystoid macular edema. In this type two mechanisms are postulated, either small cysts are merged with one another to form a larger cyst or a larger cyst can directly rupture to form a full-thickness MH usually by degenerative forces.
- Iatrogenic trauma during vitrectomy might be another possible mechanism for triggering the formation of secondary MHs.
2.5. SPONTANEOUS CLOSURE OF SECONDARY MACULAR HOLES
Spontaneous closure of reopened macular holes after an initial successful surgery can be caused by a shift in the tractional forces of an epiretinal membrane and/or the bridging of retinal tissues or epiretinal proliferations in the macular hole.
3. Postoperative role of OCTA after successful macular surgery
3.1. MACULAR PERFUSION FOLLOWING MACULAR HOLE SURGERY
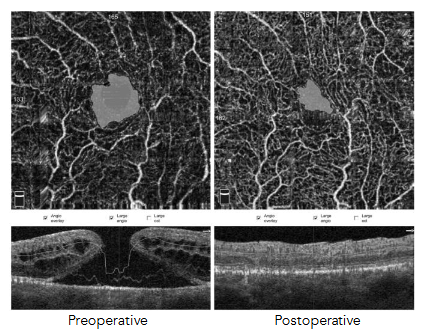
It was observed that 2 weeks post operatively there was marked reduction in FAZ parameters. This finding could be explained by centripetal movement of the foveal tissue towards the central fovea after macular hole closure.
Kim et al and Demirel et al observed that the vascular densities in post operatively successfully closed macular holes, particularly in the deep plexus, was lower than that in both fellow eyes or healthy eyes. Most VD values recovered only to the preoperative status; this may impede the healing process and be one cause for unsatisfactory postoperative visual gain in spite of successful anatomic closure of the MH. It was also postulated that the deep plexus was more prone to ischemia and this might partially lead to disruption of the photoreceptors and contribute to a lower visual function. It was postulated that if the preoperative macular microvasculature was dense especially in the deep capillaries, VA after surgery post operatively was expected to improve to better degrees.
The superficial retinal blood flow density (SRBFD) increased at 1 month and 3 months after the operation, and the choroidal blood flow density (CBFD) continued to increase post operatively. Quantification of SRBFD and CBFD may serve as a biomarker for assessing macular disease progression and prognosis.
3.2. DIAGNOSING RETINAL DISPLACEMENT BY OCTA IN EYES UNDERGOING MACULAR HOLE SURGERY
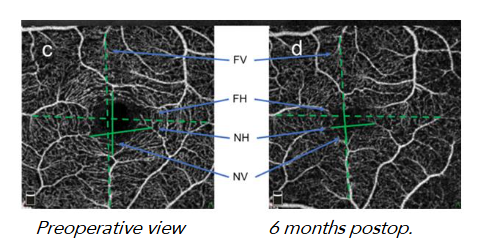
Following successful macular hole surgery, the vessels in the macular region are displaced nasally towards the optic disc. The retina in the temporal quadrant is displaced significantly more than in the nasal quadrant and the area of the superficial FAZ became smaller, indicating a centripetal retinal movement.
Although retinal displacement near the macular region contributes to MH closure after surgery yet it displaces the photoreceptors which cause residual metamorphopsia in some cases. The larger the MH diameter and the thinner the outer retinal thickness after surgery the greater the retinal displacement and consequent metamorphopsia.
Conclusion:
The integrity of the external limiting membrane (ELM) and the ellipsoid zone (EZ) were found to be the most important prognostic criteria for visual recovery. A U-type shape pattern of closure and a flat closed closure were also associated with a favorable visual gain. On the other hand, retinal displacement following surgery may be responsible for postoperative residual metamorphopsia. A foveal hyper-reflective lesion during the healing process and age-related sub foveal deposits are poor prognostic signs for visual improvement. An early postoperative appearance of a foveal detachment, outer foveolar defects or signs of a dissociated optic nerve fiber layer (DONFL) were not found to be important signs in the determination of the final postoperative visual acuity.
Conflict of Interest Statement:
No conflicts of interest.
Funding Statement:
No funding received by the author from any company or institute.
Acknowledgements:
I am indebted to all my senior professors from whom I learned a lot in the field of retina through the past 30 years.
References:
- Fallico M, et al. Factors predicting normal visual acuity following anatomically successful macular hole surgery. Acta Ophthalmol. 2021;99(3):e324-e329. doi: 10.1111/aos.14575.
- Cicinelli MV, Marchese A, Bandello F, et al. Inner Retinal Layer and Outer Retinal Layer Findings after Macular Hole Surgery Assessed by means of Optical Coherence Tomography. J Ophthalmol. 2019;3821479. doi: 10.1155/2019/3821479.
- Singh S, Saxena S, Meyer CH, et al. Retinal photoreceptor ellipsoid zone is a structural biomarker for visual outcome after successful macular hole surgery: A novel grading system-based study. Indian J Ophthalmol. 2025;73(Suppl 1):S126-S131. doi: 10.4103/IJO.IJO_1031_24.
- Baba T, Yamamoto S, Arai M, et al. Correlation of visual recovery and presence of photoreceptor inner/outer segment junction in optical coherence images after successful macular hole repair. Retina. 2008;28(3):453-8. doi: 10.1097/IAE.0b013e3181571398.
- Saxena S, Ruia S, Prasad S, et al. Increased serum levels of urea and creatinine are surrogate markers for disruption of retinal photoreceptor external limiting membrane and inner segment ellipsoid zone in type 2 diabetes mellitus. Retina. 2017;37(2):344-349. doi: 10.1097/IAE.0000000000001163.
- Jain A, Saxena S, Khanna VK, et al. Status of serum VEGF and ICAM-1 and its association with external limiting membrane and inner segment-outer segment junction disruption in type 2 diabetes mellitus. Mol Vis 2013; 19:1760–8. http://www.molvis.org/molvis/v19/1760.
- Wakabayashi T, Fujiwara M, Sakaguchi H, et al. Foveal microstructure and visual acuity in surgically closed macular holes: Spectral-domain optical coherence tomographic analysis. Ophthalmology. 2010;117:1815-24. doi: 10.1016/j.ophtha.2010.01.017.
- Hee MR, Puliafito CA, Wong C, Duker JS, Reichel E, Schuman JS, Swanson EA, Fujimoto JG. Optical coherence tomography of macular holes. Ophthalmology. 1995 May;102(5):748-56. doi: 10.1016/s0161-6420(95)30959-1. PMID: 7777274.
- Sano M, Shimoda Y, Hashimoto H, Kishi S. Restored photoreceptor outer segment and visual recovery after macular hole closure. Am J Ophthalmol. 2009;147(2):313-318.e1. doi: 10.1016/j.ajo.2008.08.002.
- Mansour AM, Parodi M, Uwaydat SH, et al. Idiopathic Macular Hole: Algorithm for Nonsurgical Closure Based on Literature Review. J Ophthalmic Vis Res. 2023;18(4):424-432. doi: 10.18502/jovr.v18i4.14555.
- Mahmoud TH, McCuen BW 2nd. Natural history of foveolar lucencies observed by optical coherence tomography after macular hole surgery. Retina. 2007;27(1):95-100. doi: 10.1097/01.iae.0000223758.17543.49.
- Oh J, Smiddy WE, Flynn HW Jr, et al. Photoreceptor inner/outer segment defect imaging by spectral domain OCT and visual prognosis after macular hole surgery. Invest Ophthalmol Vis Sci. 2010;51(3):1651-8. doi: 10.1167/iovs.09-4420.
- Goldberg JL, Klassen MP, Hua Y, et al. Amacrine-signaled loss of intrinsic axon growth ability by retinal ganglion cells. Science. 2002;296(5574):1860-4. doi: 10.1126/science.1068428.
- Shewan D, Berry M, Cohen J. Extensive regeneration in vitro by early embryonic neurons on immature and adult CNS tissue. J Neurosci. 1995;15(3 Pt 1):2057-62. doi: 10.1523/JNEUROSCI.15-03-02057.1995.
- Li D, Field PM, Raisman G. Failure of axon regeneration in postnatal rat entorhinohippocampal slice coculture is due to maturation of the axon, not that of the pathway or target. Eur J Neurosci. 1995;7(6):1164-71. doi: 10.1111/j.1460-9568.1995.tb01106.x.
- Celsi F, Pizzo P, Brini M, et al. Mitochondria, calcium and cell death: a deadly triad in neurodegeneration. Biochim Biophys Acta. 2009;1787:335–344. doi: 10.1016/j.bbabio.2009.02.021.
- Kim Y, Kim ES, Yu SY, et al. Age-related clinical outcome after macular hole surgery. Retina. 2017;37(1):80-87. doi: 10.1097/IAE.0000000000001162.
- Chinnery HR, McLenachan S, Humphries T, et al. Accumulation of murine subretinal macrophages: effects of age, pigmentation and CX3CR1. Neurobiol Aging. 2012;33(8):1769-76. doi: 10.1016/j.neurobiolaging.2011.03.010.
- Cornish K, Lois N, Scott N, et al. Vitrectomy with internal limiting membrane (ILM) peeling versus vitrectomy with no peeling for idiopathic full-thickness macular hole (FTMH). Cochrane Database Syst Rev. 2013;(6):CD009306. doi: 10.1002/14651858.CD009306.pub2.
- Brooks HL Jr. Macular hole surgery with and without internal limiting membrane peeling. Ophthalmology. 2000;107(10):1939-48; discussion 1948-9. doi: 10.1016/s0161-6420(00)00331-6.
- Yoshida M, Kishi S. Pathogenesis of macular hole recurrence and its prevention by internal limiting membrane peeling. Retina. 2007;27(2):169-73. doi: 10.1097/01.iae.0000224940.79223.fb.
- Simon GJ, Desatnik H, Alhalel A, et al. Retrospective analysis of vitrectomy with and without internal limiting membrane peeling for stage 3 and 4 macular hole. Ophthalmic Surg Lasers Imaging. 2004;35(2):109-15. PMID: 15088820.
- Haritoglou C, Reiniger IW, Schaumberger M, et al. Five-year follow-up of macular hole surgery with peeling of the internal limiting membrane: update of a prospective study. Retina. 2006;26(6):618-22. doi: 10.1097/01.iae.0000236474.63819.3a.
- Christensen UC. Value of internal limiting membrane peeling in surgery for idiopathic macular hole and the correlation between function and retinal morphology. Acta Ophthalmol. 2009;87 Thesis 2:1-23. doi: 10.1111/j.1755-3768.2009.01777.x.
- Baba T, Sato E, Oshitari T, Yamamoto S. Regional reduction of ganglion cell complex after vitrectomy with internal limiting membrane peeling for idiopathic macular hole. J Ophthalmol. 2014;2014:372589. doi: 10.1155/2014/372589.
- Sabater AL, Velázquez-Villoria Á, Zapata MA, et al. Evaluation of macular retinal ganglion cell-inner plexiform layer thickness after vitrectomy with internal limiting membrane peeling for idiopathic macular holes. Biomed Res Int. 2014;2014:458631. doi: 10.1155/2014/458631.
- Clark A, Balducci N, Pichi F, et al. Swelling of the arcuate nerve fiber layer after internal limiting membrane peeling. Retina. 2012;32(8):1608-13. doi: 10.1097/IAE.0b013e3182437e86.
- Balducci N, Morara M, Veronese C, et al. Retinal nerve fiber layer thickness modification after internal limiting membrane peeling. Retina. 2014;34(4):655-63. doi: 10.1097/IAE.0000000000000004.
- Kumagai K, Ogino N, Furukawa M, et al. Retinal thickness after vitrectomy and internal limiting membrane peeling for macular hole and epiretinal membrane. Clin Ophthalmol. 2012;6:679-88. doi: 10.2147/OPTH.S30288.
- Ye X, Xu J, He S, et al. Quantitative evaluation of dissociated optic fibre layer (DONFL) following idiopathic macular hole surgery. Eye (Lond). 2023;37(7):1451-1457. doi: 10.1038/s41433-022-02150-y.
- He S, Ye X, Qiu W, et al. Analysis of Retinal Microstructure in Eyes with Dissociated Optic Nerve Fiber Layer (DONFL) Appearance following Idiopathic Macular Hole Surgery: An Optical Coherence Tomography Study. J Pers Med. 2023;13(2):255. doi: 10.3390/jpm13020255.
- Sabry D, El-Kannishy A, Kamel R, et al. Correlation between en face optical coherence tomography defects of the inner retinal layers and ganglion cell inner plexiform layer analysis after internal limiting membrane peeling for idiopathic full-thickness macular hole. Invest Ophthalmol Vis Sci. 2016;57(9):444-50. doi: 10.1167/iovs.15-18043.
- Ito Y, Terasaki H, Takahashi A. Dissociated optic nerve fiber layer appearance after internal limiting membrane peeling for idiopathic macular holes. Ophthalmology. 2005;112(8):1415-20. doi: 10.1016/j.ophtha.2005.02.023.
- Takai Y, Tanito M, Sugihara K, et al. Temporal inverted internal limiting membrane flap technique for a macular hole patient unable to maintain postoperative prone positioning. Retin Cases Brief Rep. 2016;10(4):323-6. doi: 10.1097/ICB.0000000000000258.
- Michalewska Z, Michalewski J, Nawrocki J, et al. Temporal inverted internal limiting membrane flap technique versus classic inverted internal limiting membrane flap technique: a comparative study. Retina. 2015;35(9):1844-50. doi: 10.1097/IAE.0000000000000555.
- Hirata A, Mine K, Hayashi K. Contractility of temporal inverted internal limiting membrane flap after vitrectomy for macular hole. Sci Rep. 2021;11(1):20035. doi: 10.1038/s41598-021-99509-0.
- Sakimoto S, Ikuno Y, Fujimoto S, et al. Characteristics of the retinal surface after internal limiting membrane peeling in highly myopic eyes. Am J Ophthalmol. 2014;158(4):762-768.e1. doi: 10.1016/j.ajo.2014.06.024.
- Kim KY, Yu SY, Kim M, et al. Morphological change of inner retinal layer on spectral-domain optical coherence tomography following macular hole surgery. Ophthalmologica. 2013;230(1):18-26. doi: 10.1159/000350552.
- Steel DH, Dinah C, Habib M, et al. ILM peeling technique influences the degree of a dissociated optic nerve fiber layer appearance after macular hole surgery. Graefes Arch Clin Exp Ophthalmol. 2015;253(5):691-8. doi: 10.1007/s00417-014-2734-z.
- Nukada K, Hangai M, Ooto S, et al. Tomographic features of macula after successful macular hole surgery. Invest Ophthalmol Vis Sci. 2013;54(4):2417-28. doi: 10.1167/iovs.12-10838.
- Spaide RF. “Dissociated optic nerve fiber layer appearance” after internal limiting membrane removal is inner retinal dimpling. Retina. 2012;32(9):1719-26. doi: 10.1097/IAE.0b013e3182671191.
- Ikeda T, Nakamura K, Sato T, et al. Involvement of anoikis in dissociated optic nerve fiber layer appearance. Int J Mol Sci. 2021;22(4):1724. doi: 10.3390/ijms22041724.
- Kim YH, Song MS, Togloom A, et al. Bidirectional dimples after internal limiting membrane peeling for a macular hole. Transl Vis Sci Technol. 2023;12(5):23. doi: 10.1167/tvst.12.5.23.
- Steel DH, Dinah C, White K, et al. The relationship between a dissociated optic nerve fibre layer appearance after macular hole surgery and Muller cell debris on peeled internal limiting membrane. Acta Ophthalmol. 2017;95(2):153-157. doi: 10.1111/aos.13195.
- Tao J, Yang J, Wu Y, et al. Internal limiting membrane peeling distorts the retinal layers and induces scotoma formation in the perifoveal temporal macula. Retina. 2022;42(12):2276-2283. doi: 10.1097/IAE.0000000000003619.
- Balducci N, Morara M, Veronese C, et al. Retinal nerve fiber layer thickness modification after internal limiting membrane peeling. Retina. 2014;34(4):655-63. doi: 10.1097/IAE.0000000000000004.
- Modi A, Giridhar A, Gopalakrishnan M. Spectral domain optical coherence tomography–based microstructural analysis of retinal architecture post internal limiting membrane peeling for surgery of idiopathic macular hole repair. Retina. 2017;37(2):291-298. doi: 10.1097/IAE.0000000000001129.
- Farah ME, Maia M, Rodrigues EB. Dyes in ocular surgery: principles for use in chromovitrectomy. Am J Ophthalmol. 2009;148(3):332-40. doi: 10.1016/j.ajo.2009.04.003.
- Piccirillo V, Sbordone S, Sorgente F, et al. Evaluation of efficacy and safety of new high-density dyes for chromovitrectomy. Sci Rep. 2021;11(1):15171. doi: 10.1038/s41598-021-94770-9.
- Takamura Y, Tomomatsu T, Matsumura T, et al. Correlation between central retinal thickness after successful macular hole surgery and visual outcome. Jpn J Ophthalmol. 2015;59(6):394-400. doi: 10.1007/s10384-015-0406-0.
- Wollensak G, Spoerl E, Grosse G, et al. Biomechanical significance of the human internal limiting lamina. Retina. 2006;26(8):965-8. doi: 10.1097/01.iae.0000250001.45661.95.
- Hogan MJ, Alvarado JA, Weddell JE. Histology of the Human Eye. An atlas and textbook Philadelphia: WB Saunders Company. (1971), 523–606. DOI:10.1001/jama.1972.03190280059024 Corpus ID: 72719454.
- Goto K, Iwase T, Akahori T, et al. Choroidal and retinal displacements after vitrectomy with internal limiting membrane peeling in eyes with idiopathic macular hole. Sci Rep. 2019;9(1):17568. doi: 10.1038/s41598-019-54106-0.
- Kang SW, Ahn K, Ham DI. Types of macular hole closure and their clinical implications. Br J Ophthalmol. 2003;87(8):1015-9. doi: 10.1136/bjo.87.8.1015.
- Imai M, Iijima H, Gotoh T, et al. Optical coherence tomography of successfully repaired idiopathic macular holes. Am J Ophthalmol. 1999;128(5):621-7. doi: 10.1016/s0002-9394(99)00200-7.
- Tornambe PE, Poliner LS, Cohen RG. Definition of macular hole surgery end points: elevated/open, flat/open, flat/closed. Retina. 1998;18(3):286-7. doi: 10.1097/00006982-199803000-00021.
- Hillenkamp J, Kraus J, Framme C, et al. Retreatment of full-thickness macular hole: predictive value of optical coherence tomography. Br J Ophthalmol. 2007;91(11):1445-9. doi: 10.1136/bjo.2007.115642.
- D’Souza MJ, Chaudhary V, Devenyi R, et al. Re-operation of idiopathic full-thickness macular holes after initial surgery with internal limiting membrane peel. Br J Ophthalmol. 2011;95(11):1564-7. doi: 10.1136/bjo.2010.195826.
- Ryan EH Jr, Gilbert HD. Results of surgical treatment of recent-onset full-thickness idiopathic macular holes. Arch Ophthalmol. 1994 Dec;112(12):1545-53. doi: 10.1001/archopht.1994.01090240051025.
- Banker AS, Freeman WR, Kim JW, et al. Vision-threatening complications of surgery for full-thickness macular holes. Vitrectomy for Macular Hole Study Group. Ophthalmology. 1997;104(9):1442-53. doi: 10.1016/s0161-6420(97)30118-3.