





Predicting Severe Adhesions in Repeat Caesarean Section
Abdominal striae gravidarum in Preoperative prediction of severe intraperitoneal adhesions in women undergoing repeat caesarean section
Mawande Mayibenye¹, G.A.B Buga¹, M.L. Mdaka¹, Mirabel Nanjoh²
- Department of Obstetrics and Gynaecology faculty of medicine and health sciences, Walter Sisulu University.
- Department of public health, faculty of medicine and health sciences, Walter Sisulu University. Mthatha, Eastern Cape, South Africa.
OPEN ACCESS
PUBLISHED: 30 November 2025
CITATION: Mayibenye, M., Buga G., A., B., Mdaka, M., L., Nanjoh, M., Abdominal striae gravidarum in Preoperative prediction of severe intraperitoneal adhesions women undergoing repeat caesarean section. Medical Research Archives, [online] 13(11). https://doi.org/10.18103/mra.v13i10.7056
COPYRIGHT © 2025 European Society of Medicine. This is an open- access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i10.7056
ISSN 2375-1924
ABSTRACT
Objectives: Caesarean section is the most commonly performed procedure known to be associated with the development of intra-abdominal adhesions. These adhesions may lead to difficult repeat surgery and complications like haemorrhage, bladder and bowel injury. Determining which women are at risk for adhesions would help with triaging which women may have a risk for complicated repeat surgery. The presence of abdominal striae gravidarum, among others has been proposed as one of the preoperative prediction tools for intraperitoneal adhesions.
Design: This was a prospective observational study
Setting: Nelson Mandela Academic Hospital, a tertiary hospital in the Eastern Cape region of South Africa between July 2021 and July 2022.
Participants: 419 women with a previous caesarean section scar were approached in the third trimester and examined for severity of striae gravidarum.
Methods: The severity of striae gravidarum was determined according to Davey’s scoring system. Intraperitoneal adhesions were evaluated according to the modified Nair scoring system. Three groups were established according to the severity of striae gravidarum, was assessed whether we could use this method to predict the presence of intraperitoneal adhesions at repeat caesarean section.
Results: Between July 2021 and July 2022 we enrolled 419 women. Adhesions were present in 53.5%. Then 17.4% (N=73/419) had severe striae gravidarum, and 4.5% (N=19/419) had mild striae gravidarum. Women with dense adhesions were older, had more previous caesarean sections, longer incision-to-delivery time and more blood loss. The presence of mild/moderate striae gravidarum had a sensitivity of 27.23% and specificity of 84.10. The presence of severe striae gravidarum had a sensitivity of 21.4% and specificity of 87.2%. The presence of striae gravidarum in overall did not predict adhesions.
Conclusions: Although the striae gravidarum has a low sensitivity in predicting dense intraperitoneal adhesions, it has an excellent specificity. The striae gravidarum can therefore be used by surgeons to identify patients who are unlikely to have dense intraperitoneal adhesions. This would be particularly useful in district hospitals for triaging patients with previous caesarean sections whom they can operate safely, while referring others to level 2 or 3 hospitals. The results cannot be generalized because there were very small number of patients with striae gravidarum. More studies are needed before the results can be applied to the general population.
Keywords: Striae gravidarum, adhesions, prediction, caesarean section
Introduction
Caesarean section is the most commonly performed abdominal surgery worldwide.¹ Unfortunately, there are complications associated with this surgery, which include intraperitoneal adhesion formation. These adhesions are subsequently associated with maternal and perinatal morbidities such as delayed delivery of the baby, postpartum haemorrhage (PPH), bowel and bladder injury during adhesiolysis, and it may lead to mortality especially in cases where the surgeon is less experienced in dealing with these adhesions. The incidence of intraperitoneal adhesion formation after caesarean section is estimated to be between 24% and 38%.²,³,⁴ Identifying which women may be at risk for dense intraperitoneal adhesions may be important. If one could identify which women were at high risk, it would allow for triage, planning and counselling of patients about the associated complications. The surgeon may decide to use midline skin incision instead of transverse skin incision on those patients identified as high risk of dense adhesions on triaging. This would be particularly valuable in low- and-middle income countries where surgeries are often performed in rural areas with less support.
Several non-invasive methods have been investigated for the prediction of intra-peritoneal adhesions following surgery. These include the presence of severe abdominal striae gravidarum,⁵,⁶ abdominal scar characteristics including the type of skin incision, the number of incision and features of the scar, and transabdominal ultrasound imaging to assess uterine mobility by assessing if the uterus can slide under the anterior abdominal wall (sliding sign).⁷–¹³ The index study, among other predictive methods, was evaluating whether the presence of striae gravidarum could be predictive of dense intraperitoneal adhesions in those patients undergoing repeat caesarean section.
Striae gravidarum are the linear bands formed as a result of the structural changes in the connective tissue which is observed frequently in pregnancy. Their prevalence varies between 50% and 90%.¹⁴ Among others, this noninvasive method has been studied as a possible predictor of intraperitoneal adhesions. It is simple, cheap, noninvasive and easy to learn.
We aimed to prospectively evaluate whether the presence of striae gravidarum could correctly predict the presence of dense intraperitoneal adhesions in patients undergoing a repeat caesarean section in third trimester.
METHODS:
Study cohort and design
This prospective observational study was conducted at Nelson Mandela Academic Hospital, a referral hospital in the Eastern Cape Province of South Africa. Consecutive pregnant women scheduled for a repeat caesarean section who were over 18 years of age and signed informed consent were included. Women who needed an urgent delivery where there was no time for preoperative assessment were not included.
The preoperative assessments of striae gravidarum was performed by one researcher (MM) who did not perform any of the caesarean sections. Striae gravidarum characteristics were described using the Davey scoring system. To do this, the abdomen was divided into four quadrants at the midline and horizontally through the umbilicus. Each quadrant was given a score. No points were allocated if there were no striae. One point was given for moderate striae defined as 1 to 3 striae per quadrant and 2 points were given if there were 4 or more striae. A total score of 0 to 2 was classified as no to mild striae. A score of 3–8 was considered to represent severe striae gravidarum.
All surgeons were trained to describe adhesions and were classified using a method described by Tulandi & Lyell.¹⁵ Adhesions were described by severity and site, in this system we used a point system, and the scores from multiple sites, between uterus and bladder, between uterus and
abdominal fascia, between uterus and omentum, between omentum and abdominal fascia, and adhesions from other pelvic structures that interfere with the delivery were additive. These were described if they were filmy or dense adhesions. The area of incision covered by adhesions was divided into <3cm, 3–6 cm, and >6 cm.
Women with filmy adhesions and no adhesions were compared to women with dense adhesions.
Time from skin incision to incision of the uterus, time from skin incision to delivery of the baby, and overall surgical time were collected. Perinatal outcomes included 5-minute Apgar scores, birth weight and birth injuries. Data on adhesiolysis, bowel and/or bladder injuries, intraoperative bleeding, and/or the need for hysterectomy were collected. Charts were reviewed for short-term complications like haemorrhage, wound haematoma, wound infection and deep vein thrombosis.
Data was collected on data sheets and then transferred into Microsoft Excel, cleaned, checked and then exported to Statistical Package for the Social Sciences (SPSS) software program for analysis.
Statistical methods
The prevalence of adhesions post caesarean section was estimated to be 50% based on the study done by Nuamah et al.¹⁷ and Moro et al.³⁰ Using an alpha error of 0.05 at power of 80% with 95% confidence levels, the estimated sample size was 384.¹⁶ We increased the sample size by 10% to account for dropouts and loss to follow up. The final sample size was 420.
Categorical variables were expressed as frequencies and proportions. Univariate analyses were performed for categorical variables using Chi-square or Fisher’s exact test. Continuous variables were presented as means with standard deviations, if normally distributed. If the data was skewed it was presented as medians with interquartile ranges and were compared using the Student T-test or Mann-Whitney U-test, as appropriate. The sensitivity, specificity, positive and negative predictive values, and the positive and negative likelihood ratios were calculated. Odds ratios were calculated for the patients to assess the odds of finding adhesions at repeat caesarean section in patients with normal and abnormal striae. For multivariable analysis, forward conditional logistic regression was used with intraperitoneal adhesions as the dependent variable, and age, BMI, number of caesarean sections, abdominal scar characteristics, striae gravidarum as independent variables. Age, BMI and the number of caesarean sections were included as continuous variables, while all other variables were categorical. The level of significance was set at 5% (p <0.05) for all comparisons. For multivariable analysis, forward conditional logistic regression was used to identify the predictive performance of bivariate significant variables in the prediction of intra-peritoneal adhesions.
Ethical considerations
Prospective ethical clearance (Certificate No. 061/2021) was obtained from the Ethics and Biosafety Committee of the Faculty of Health Sciences, Walter Sisulu University. Permission to conduct the research was also sought from the Eastern Cape Department of Health.
RESULTS
Background characteristics
440 women were approached and 420 were included, and 20 women declined to be involved because they did not consent. We were able to collect outcome data on 419 women. One woman who was included was under 18 years old.
Baseline characteristics are presented in table one. Half of the women were obese. Women were more likely to have dense intraperitoneal adhesions if they were older and had more than 2 previous caesarean sections.
Table 1: Demographic characteristics of 419 repeat caesarean section participants.
| Variable | All<br>Median (IQR) | Dense<br>Mean rank | Filmy<br>Mean rank | None<br>Mean rank | P-value* |
|---|---|---|---|---|---|
| Age (years) | 29 (25–33) | 239.45 | 197.08 | 188.99 | <0.0001 |
| BMI (kg/m²) | 30 (27–34) | 222.62 | 202.87 | 201.47 | 0.224 |
| Gravity | 3 (3–4) | 249.46 | 199.36 | 179.83 | <0.0001 |
| Parity | 2 (2–3) | 250.95 | 191.03 | 181.09 | <0.0001 |
| GA (week/days) | 38 (37.4–38.3) | 206.26 | 223.25 | 209.16 | 0.640 |
| Previous CS | 2 (2–2) | 263.47 | 202.81 | 166.93 | <0.0001 |
*Kruskal-Wallis H, BMI (Body mass index), GA (Gestational age), CS (caesarean section)
Adhesions were present in 53.5% (224/419) and absent in 46.5% (195/419). Almost 40% (165/419) participants had dense intra-peritoneal adhesions and 14.1% (59/419) had filmy adhesions. Of those with adhesions, 98.2% (220/224) had adhesions between the anterior abdominal wall and the uterus, and 74.1% (166/224) involved the bladder and anterior abdominal wall. Omental-uterine adhesions were found in 17.9% (40/224). Only 2/224 (0.9%) had adhesions between bowel and the uterus.
In terms of how many anatomical sites involved: Multi-site adhesions were observed in 171/224 (76.3%) women, with the 140/224 (82.0%) having adhesions at two sites, 29 (17.0%) at three sites, and two (1.2%) at all four intra-peritoneal sites, which refers to the uterus, bladder, bowel, and omentum, as per the classification of intra-abdominal adhesions by Tulandi and Lyell.¹⁵ The incision-to-delivery time was significantly longer in women with dense adhesions, and estimated blood loss was more during surgery. The incision-to-delivery times in minutes were 31.8 minutes, 19.5 minutes, and 12.2 minutes when there were dense adhesions, filmy adhesions, or no intraperitoneal adhesions respectively.
The estimated blood loss during surgery was 297 mL, 172 mL, and 147 mL when there were dense adhesions, filmy adhesions, or no adhesions, respectively. There were no differences in 5-minute APGAR scores between groups. In terms of the level of the surgeon, in 392 repeat caesarean sections, the surgeon was an experienced registrar, and in the case of 27 repeat caesarean sections, the surgeon was an experienced medical officer (those waiting to join the registrar programme).
Table 2: Immediate maternal and neonatal outcomes following repeat caesarean section
| Outcome variables | Median (IQR) | Minimum – Maximum |
|---|---|---|
| Incision-to-delivery time (minutes) | 12 (10 – 15) | 8 – 50 |
| Blood loss (ml) | 400 (400 – 500) | 150 – 1800 |
| Apgar scored at 5 minutes | 9 (8 – 9) | 6 – 9 |
| Apgar score at 10 minutes | 10 (10 – 10) | 7 – 10 |
| Complications (n=8) | N | % |
|---|---|---|
| Post-partum Haemorrhage | 4 | 50.0 |
| Wound sepsis | 1 | 12.5 |
| Bladder injury | 3 | 37.5 |
Accuracy of striae gravidarum in predicting intraperitoneal adhesions
In predicting the presence of intra-peritoneal adhesions, the presence of mild/severe striae gravidarum had a sensitivity of 27.23% (95% CI: 22.97–31.49), and a specificity of 84.10% (95% CI: 80.60–87.60), indicating that the characteristics of striae gravidarum could not accurately identify women with intraperitoneal adhesions but could correctly exclude those without adhesions. The positive predictive value (PPV) was 66.3% (95% CI: 61.78–70.83) and the negative predictive value (NPV) was 50.2% (95% CI: 45.37–54.94). Thus, only slightly more than half of women who were suspected to have adhesions had it and only half of those suspected of not having adhesions turned out to not have adhesions. The positive likelihood ratio (LR+) was 1.71, and the negative likelihood ratio (LR−) was 0.87. The LR+ is very small and the LR− is large signifying that this characteristic should not be used in determining the probability of adhesions during repeat caesarean section.
The sensitivity of severe striae gravidarum in the prediction of intra-peritoneal adhesion was 21.4% (95% CI: 17.50%–25.36) and the specificity was 87.2% (95% CI: 83.98–90.38), indicating that it had a low ability to accurately identify participants with adhesions but a good ability to accurately classify participants without adhesions. The PPV was 65.75% (95% CI: 61.21–70.30) and the NPV was 49.13% (95% CI: 44.53–53.92). The PPV showed that among those with severe striae gravidarum, the probability of having adhesions was 65.75%. Similarly, based on the NPV, participants suspected of not having adhesions (absence of severe striae gravidarum) had a lower probability of truly not having adhesions.
Severe striae had an LR+ of 1.67 and an LR− of 0.90 (Table 3). Since the expectation is to get a large LR+ and a small LR−, this means that severe striae gravidarum will only produce a very small shift in post-test probability and thus will not help determine intra-peritoneal adhesions and its absence in participants undergoing repeat caesarean section.
Table 3: Accuracy of striae gravidarum in the prediction of intra-peritoneal adhesion
| Accuracy indicators | Mild/moderate striae gravidarum<br>% (95%CI) | Severe striae gravidarum<br>% (95%CI) |
|---|---|---|
| Sensitivity | 27.23% (22.97% – 31.49%) | 21.43% (17.50% – 25.36%) |
| Specificity | 84.10% (80.60% – 87.60%) | 87.18% (83.98% – 90.38%) |
| Positive Predictive Value | 66.30% (61.78% – 70.83%) | 65.75% (61.21% – 70.30%) |
| Negative Predictive Value | 50.15% (45.37% – 54.94%) | 49.13% (44.35% – 53.92%) |
| Positive Likelihood Ratio | 1.71 | 1.67 |
| Negative Likelihood Ratio | 0.87 | 0.90 |
Discussion
The proportion of women with intra-abdominal adhesions found in the index study is on the higher end, although still in the range found following caesarean section by Awonuga et al.²,¹⁰. Caution may be needed in applying the findings to the general population due to small number of patients who had striae gravidarum in the study and due to low sensitivity in identifying women at high risk of adhesions.
Risk factors for intra-peritoneal adhesions following caesarean section
The median age of the women who participated in this study was 29 years (IQR = 25–33). The women who had dense intra-peritoneal adhesions were significantly older than those with filmy or no adhesions (p<0.0001). Nuamah, in Ghana, also found that women with intra-peritoneal adhesions were significantly older than those without adhesions.¹⁷ This difference is probably because the older women may have a higher parity and a bigger number of previous caesarean sections. It is known that the incidence of adhesions following caesarean section increases with each repeat caesarean section to reach approximately 83% with the fourth caesarean section.¹⁹–²¹ In the index study, parity was significantly higher among women who had dense intra-peritoneal adhesions compared to those with filmy or no adhesions (P<0.0001). In addition, the women who had dense intra-peritoneal adhesions also had a greater number of previous caesarean sections than those who had filmy or no adhesions, and this difference was also statistically significant (p<0.0001).
In the index study, 50% of the women had a body mass index (BMI) of ≥30 kg/m² and were therefore obese. Obesity has been implicated as a risk factor for striae gravidarum and intra-peritoneal adhesions following caesarean section.²² Although women with dense intraperitoneal adhesions had a higher BMI than those with filmy or no adhesions, this difference was not statistically significant (p>0.05).
Striae gravidarum characteristics
Abbas et al investigated the value of the Davey Score for striae gravidarum in predicting the presence of pelvic adhesions prior to repeat caesarean delivery.⁷ Patients were divided into two groups depending on the Davey Score of the striae gravidarum. Patients with a score of 0–2 were in group I, and patients with a score of 3–8 were in group II.
Pelvic adhesions were evaluated during repeat caesarean section, and the pelvic adhesions were classified according to the Nair scoring system. Approximately 90% of women with severe striae (score 3–8) were found to have pelvic adhesions, compared with 82.5% of women with no striae or only mild striae (score 0–2). The Nair score was significantly correlated with the Davey score. They concluded that the striae gravidarum score in women with a previous caesarean section might help in preoperative prediction of pelvic adhesions status before repeat surgery. Other studies have had more or less similar findings.²⁴–²⁶ These findings were contrary to the findings of the index study as it did not correctly predict adhesions in a repeat caesarean section.
The Davey scoring system for classifying abdominal striae gravidarum first described in 1972 was used in the current study.²⁷ Of the 419 women who participated in this study 78% (N=327) did not have any abdominal striae gravidarum, whereas 17.4% (N=73) had severe striae gravidarum, and 4.5% (N=19) only had mild striae gravidarum.
In predicting the presence of intra-peritoneal adhesions, the presence of mild/severe striae gravidarum had a sensitivity of 27.23% (95% CI: 22.97–31.49), and a specificity of 84.10% (95% CI: 80.60–87.60), indicating that the characteristics of striae gravidarum could not accurately identify women with intraperitoneal adhesions but could correctly exclude those without adhesions. The positive predictive value (PPV) was 66.3% (95% CI: 61.78–70.83) and the negative predictive value (NPV) was 50.2% (95% CI: 45.37–54.94). Thus, only slightly more than half of women who were suspected to have adhesions had it and only half of those suspected of not having adhesions turned out to not have adhesions. The positive likelihood ratio (LR+) was 1.71, and the negative likelihood ratio (LR−) was 0.87. The LR+ is very small and the LR− is large signifying that this characteristic should not be used in determining the probability of adhesions during repeat caesarean section.
The sensitivity of severe striae gravidarum in the prediction of intra-peritoneal adhesion was 21.4% (95% CI: 17.50%–25.36) and the specificity was 87.2% (95% CI: 83.98–90.38), indicating that it had a low ability to accurately identify participants with adhesions but a good ability to accurately classify participants without adhesions. The PPV was 65.75% (95% CI: 61.21–70.30) and the NPV was 49.13% (95% CI: 44.53–53.92). The PPV showed that among those with severe striae gravidarum, the probability of having adhesions was 65.75%. Similarly, based on the NPV, participants suspected of not having adhesions (absence of severe striae gravidarum) had a lower probability of truly not having adhesions.
Severe striae had an LR+ of 1.67 and an LR− of 0.90 (Table 3). Since the expectation is to get a large LR+ and a small LR−, this means that severe striae gravidarum will only produce a very small shift in post-test probability and thus will not help determine intra-peritoneal adhesions and its absence in participants undergoing repeat caesarean section.
Solyman et al. assessed striae gravidarum and scar characteristics in 400 women.²⁹ They concluded that abdominal striae and abdominal scar characteristics were good predictors of intraperitoneal adhesions. They found that a striae gravidarum Davey score of >6 had a sensitivity 61.3% and a specificity of 82.8% in predicting intra-abdominal adhesions. In contrast, in the index study, a Davey score >3 had a sensitivity of only 21.43% and specificity of 87.2%.
The results of the index study do not support the use of the severity of striae gravidarum in predicting intra-abdominal adhesions alone. However, Mayibenye et al, in the index study discovered that the accuracy of preoperative prediction of intra-abdominal adhesions in women undergoing repeat caesarean section increases with combination of different predictive methods such as sonographic sliding sign, scar characteristics, and striae gravidarum, rather than a single method.³⁰ Therefore, more studies are needed for generalizing the results.
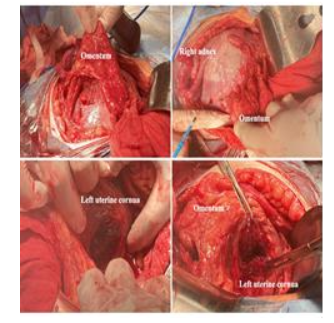
Figure-1 shows striae gravidarum picture by Buchana et al.³² Majority of patients in this study had adhesions like this one, which is described as severe striae according to Davey scoring system. According to Solyman et al,²⁹ this type of striae is associated with dense intraperitoneal adhesions as shown in figure-2. However, the index study did not show any statistically significant correlation between striae gravidarum and dense adhesions.³³

Women with filmy adhesions and no adhesions were compared to women with dense adhesions. The area of incision covered by adhesions was divided into <3 cm, 3-6 cm, and >6 cm. Time from skin incision to incision of the uterus, time from skin incision to delivery of the baby, and overall surgical time were collected. Perinatal outcomes included 5-minute Apgar scores and birth injuries. Data on adhesiolysis, bowel, and bladder injuries were also collected. Charts were reviewed for complications.
Research implications
The method is easy to learn for the medical officers and registrars. More studies should be done to assess if it can be used to triage women undergoing repeat caesarean section in district hospitals and identify patients who may need to be referred to a higher level of care for repeat caesarean section.
References
1. Cavallaro FL, Cresswell JA, Franca GVA, et al. (2013). Trends in caesarean delivery by country and wealth quintile: cross-sectional surveys in southern Asia and sub-Saharan Africa. Bull World Health Organ. 91:914-922D. doi: http://dx.doi.org/10.2471/BLT.13.117598.
2. Awonuga AO, Fletcher NM, Saed GM, Diamond MP. (2011). Postoperative adhesion development following caesarean section and open intra-abdominal gynaecological operations: a review. Reprod Sci. 18(2):1166-1185.
3. Hesselman, S., Högberg, U., Råssjö, E. B., Schytt, E., Löfgren, M., & Jonsson, M. (2018). Abdominal adhesions in gynaecologic surgery after caesarean section: a longitudinal population‐based register study. BJOG: An International Journal of Obstetrics & Gynaecology, 125(5), 597-603.
4. Poole JH (2013). Adhesions following caesarean delivery: review of their occurrence, consequences and preventative management using adhesion barriers. Women’s Health. 9(5):467-477.
5. Cakir Gungor, A. N., Oguz, S., Hacivelioglu, S., Isik, S., Uysal, A., Gencer, M., & Cosar, E. (2014). Predictive value of striae gravidarum severity for intraperitoneal adhesions or uterine scar healing in patients with previous caesarean delivery. The Journal of Maternal-Fetal & Neonatal Medicine, 27(13), 1312-1315.
6. Abbas AM, Khalaf M, Abdel-Reheem F, El-Nashar I (2020). Prediction of pelvic adhesions at repeat caesarean delivery through assessment of striae gravidarum score: a cross-sectional study. J Gynecol Obstet Hum Reprod. 49:101619. http://dx.doi.org/10.1016/j.jogoh.2019.08.002
7. Salim R, Kadan Y, Nachum Z, et al. (2008). Abdominal scar characteristics as a predictor of intra-abdominal adhesions at repeat caesarean delivery. Fertil Steril. 90(6):2324-2327.
8. Stocker LJ, Glazebrook JE, Cheong YC (2008). Are skin scar characteristics associated with the degree of pelvic adhesions at laparoscopy? Fertil Steril. 101(2):501-505.
9. Kahyaoglu I, Kayikcioglu F, Kinay T, Mollamahmutoglu L (2014). Abdominal scar characetristics: Do they predict intra-abdominal adhesions with repeat caesarean deliveries. J Obstet Gynaecol Res. https://doi.org/10.11111/jog.12429.
10. Awonuga, A. O., Belotte, J., Abuanzeh, S., Fletcher, N. M., Diamond, M. P., & Saed, G. M. (2014). Advances in the pathogenesis of adhesion development: the role of oxidative stress. Reproductive sciences, 21(7), 823-836.
11. El-Agwany AS (2016). Pfannenstiel incision scar characteristics: relation to pelvic adhesion after caesarean section. Gynecol Surg. 13:525-527.
12. Pergialoitis V, Frountzas M, Siotos C, et al. (2017). Cesarean wound scar characteristics for the prediction of pelvic adhesions: a meta-analysis of observational studies. J Matern Fetal Neonatal Med. 30(4):486-491.
13. Khalaf M, Abdel-Reheem F, El-Nashar I, et al. (2020). Cesarean skin scar characteristics for preoperative predicition of intra-abdominal adhesions at repeat caesarean delivery; a prospective cohort study. Ann Gynecol Obstet. 4(1):72-76.
14. Tang‐Lin, L., Liew, H. M., Koh, M. J., Allen, J. C., & Tan, T. C. (2017). Prevalence of striae gravidarum in a multi-ethnic Asian population and the associated risk factors. Australasian Journal of Dermatology, 58(3).
15. Tulandi T, Lyell DJ (2013). Classification of intra-abdominal adhesions after caesarean delivery. Gynecol Surg. 10:25-29. DOI: 10.1007/s10397-012-07651.
16. Pourhoseingholi, M. A., Vahedi, M., & Rahimzadeh, M. (2013). Sample size calculation in medical studies. Gastroenterology and Hepatology from bed to bench, 6(1), 14.
17. Nuamah MA, Browne JL, Ory AV, et al. (2017). Prevalence of adhesions and associated postoperative complications after caesarean section in Ghana: a prospective cohort study. Reproductive Health. 14:143. DOI:10.1186/s12978-017-0388-0.
18. Okabayashi K, AshrafianH, Zacharakis E, et al. (2014). Adhesions after abdominal surgery: a systematic review of the incidence, distribution and severity. Surg Today. 44(3):405-420.
19. Morales KJ, Gordon MC, Bates GW Jr (2007). Postcesarean delivery adhesions associated with delayed delivery of infant. Am J Obstet Gynecol. 196(5):461.e1-e6.
20. Tulandi T, Agdi M, Zarei A, Miner L, Sikirica V (2009). Adhesion development and morbidity after repeat caesarean delivery. Am J Obstet Gynecol. 201(1):56.e1-e6.
21. Mooij R, Mwampagatwa IH, van Dillen J, Stekelenburg J (2020). Association between surgical technique, adhesions and morbidity in women with repeat caesarean section: a retrospective study in a rural hospital in Western Tanzania. BMC Pregnancy and Childbirth. 20:582.
https://doi.org/10.1186/s12884-020-03229-8.
22. Kinay T, Ucok BS, Ramoglu S, Tapisiz O, Erkaya S, Koc S (2022). Maternal obesity and intra-abdominal adhesion formation at caesarean delivery. J Matern Fetal Neonat Med. 35; 2241-2246.
23. Osman H, Rubeiz N, Tamim H, et al. (2007). Risk factors for the development of striae gravidarum. Am J Obstet Gynecol. 196(1): 62.e1-62.e5
24. Abd-Elaal NK, El Kelani OA, Saif-Elmast IA, et al. (2018). The relationship between striae gravidarum and intra-abdominal adhesions in pregnant women with previous caesarean section. Int J Curr Res. 10(1):64521-64527.
25. Cakir Gungor AN, Oguz Z, Hacivelioglu S, et al. (2014). Predictive value of striae gravidarum severity for intraperitoneal adhesions or uterine scar healing in patients with previous caesarean delivery. J Matern Fetal Neonatal Med. 27:1312-1315.
26. Celik EY, Ersoy AO, Yoruk O, et al. (2018). Is striae gravidarum related to cesarean scar and peritoneal adhesions? Pak J Med Sci. 34(3):568-573.
27. Davey CMH (1972). Factors associated with the occurrence of striae gravidarum. BJOG.
https://10.1111/j.1471-0528.1972.tb11896.x
28. Elprince ME, et al. (2021) Prediction of intraperitoneal adhesions using striae gravidarum and scar characteristics in women undergoing repeat caesarean section. BMC pregnancy and childbirth. 21:286.
29. Solyman AE, et al. (2021). Prediction of pelvic adhesions at repeat caesarean delivery by assessing caesarean section scar characteristics and striae gravidarum. Menoufia Med J. 4(34): 1464-1469).
30. Mayibenye, M., Buga, G. A. B., Mdaka, M. L., & Nanjoh, M. K. (2024). Transabdominal sonographic sliding signs for preoperative prediction of dense intra‐abdominal adhesions in women undergoing repeat Cesarean delivery. Ultrasound in Obstetrics & Gynecology, 64(6), 792-798.
31. Moro, F., Mavrelos, D., Pateman, K., Holland, T., Hoo, W. L., & Jurkovic, D. (2015). Prevalence of pelvic adhesions on ultrasound examination in women with a history of Cesarean section. Ultrasound in Obstetrics & Gynecology, 45(2), 223-228.
32. Buchanan, K., Fletcher, H. M., & Reid, M. (2010). Prevention of striae gravidarum with cocoa butter cream. International Journal of Gynecology & Obstetrics, 108(1), 65-68.
33. Nieto-Calvache, A. J., Ramasauskaite, D., Palacios-Jaraquemada, J. M., Hussein, A. M., Jauniaux, E., Ubom, A. E. B., Rivera-Torres, L. F., Nunes, I., Schlembach, D., Beyeza-Kashesya, J., Wright, A., Childbirth, F. C. o., & PPH. (2025). Complex cesarean section: Surgical approach to reduce the risks of intraoperative complications and postpartum hemorrhage. International Journal of Gynecology & Obstetrics, 168(3), 987-998.