Predictors of Mortality in Stable COPD Patients
Predictors of Mortality Among Stable COPD Patients: Results from A Longitudinal Study in India
Dua Ruchi 1, (MBBS, MD, DNB); Singh Randeep 1, (MBBS, DNB); Malik Saloni 1, (PhD); Sharma Prakhar 1, (MBBS, MD); Saini Lokesh K. 1, (MBBS, MD); Mishra Mayank 1, (MBBS, MD); Sindhwani Girish 1, (MBBS, MD); Chowdhury Nilotpal 2, (MBBS, MD)
- Department of Pulmonary Medicine, All India Institute of Medical Sciences (AIIMS), Rishikesh, Uttarakhand, India
- Department of Pathology & Laboratory Medicine, All India Institute of Medical Sciences (AIIMS), Rishikesh, Uttarakhand, India
OPEN ACCESS
PUBLISHED 28 February 2025
CITATION Ruchi, D., Randeep, S., et al., 2025. Predictors of Mortality Among Stable COPD Patients: Results from A Longitudinal Study in India. Medical Research Archives, [online] 13(2). https://doi.org/10.18103/mra.v13i2.6250
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i2.6250
ISSN 2375-1924
ABSTRACT
Aims: Studies regarding predictors of mortality among stable chronic obstructive pulmonary disease (COPD) patients are limited, with existing data suffering from heterogeneity in terms of the study population, parameters analysed and results, necessitating generalisation from data of high-income countries. This longitudinal observational study aims to analyse factors responsible for 5-year all-cause mortality among stable COPD patients from a single tertiary care centre in India.
Methods: Spirometry diagnosed stable COPD patients were contacted telephonically at the end of 5 years, and the outcome was recorded as alive or dead based on telephonic response. Demographic details including age, sex, residence, smoking status, body mass index (BMI), spirometric indices, six-minute walk distance, combined assessment, modified Medical Research Council dyspnea scores, presence or absence of anxiety/depression, history of previous hospitalisation was available at baseline.
Results: Out of 130 participants at baseline, 75 responded telephonically, with a mortality rate of 26.6% among the 75 subjects. BMI and combined assessment demonstrate a significant association with mortality and fare better than the demographic variables, multivariate indices and spirometric severity on univariate and multivariate analysis.
Conclusion: BMI is a better predictor of mortality among COPD patients than other demographic characteristics. Combined assessment is not only a tool for initial stratification and treatment initiation but also has prognostic utility in stable COPD patients and fares better than other clinical characteristics.
Keywords: Chronic obstructive pulmonary disease, stable, mortality predictors
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a leading non-communicable respiratory disorder that causes significant morbidity and mortality worldwide. Increasing longevity, changing lifestyles, and rising air pollution levels have contributed to the increasing magnitude of this progressive, debilitating disease. While globally, it affects around 10.1% of people aged 40 years or more, its prevalence in India is estimated to be 7.4%. World over COPD is the third leading cause of death overtaken only by ischemic heart disease and stroke in spite of under reporting of actual disease burden. In India COPD contributes 8·7% of total deaths and 4·8% of total disability adjusted life years (DALYs) and is the second leading cause of disease burden among respiratory diseases. Preceding years have seen a paradigm shift in understanding of this disease with an increasing recognition of spillover of underlying inflammation and its extrapulmonary co-morbidities. Course of COPD is often marked by periods of acute worsening or exacerbations which not only increase COPD related mortality but also all-cause mortality including cardiovascular events related mortality. Though exacerbations increase risk of mortality even stable COPD patients have a higher risk of mortality. There have been a few studies regarding predictors of mortality among stable COPD patients, and prognostic indicators have varied from multidimensional tools to single parameters, including demographical, spirometric, radiological, inflammatory and novel markers. Overall, studies, especially cohort or longitudinal from developing countries that bear the maximal burden of this crippling disease, are limited. This longitudinal observational study is aimed at analysing factors responsible for 5-year all-cause mortality among stable COPD patients attending a tertiary care centre.
METHODS
Stable COPD patients diagnosed based on spirometry (GOLD guidelines) who attended a tertiary care hospital outpatient department (All India Institute of Medical Sciences Rishikesh, India) and had complete baseline records (January 2015-December 2018), were contacted telephonically at the end of 5 years. We recorded the outcome as alive or dead based on the telephonic response and only natural cause of death, as per the telephonic response, was considered. All patients at baseline via a questionnaire had records of demographic details including age, sex, residence, smoking status including pack years, body mass index (BMI), spirometric indices (forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC) functional exercise capacity as six-minute walk distance (6MWD), combined assessment as per GOLD guidelines, dyspnea scores in terms of modified Medical Research Council dyspnea scale (mMRC), presence or absence of anxiety/depression as per Hospital Anxiety and Depression Scale (HADS) / Patient Health Questionnaire-9 (PHQ-9) / Generalized Anxiety Disorder-7 (GAD-7) scores along with a history of previous hospitalization or exacerbation over preceding one year. Spirometry at baseline was performed with an ATS/ERS compliant spirometer and 6MWD was measured as per ATS guidelines. For PHQ-9/GAD-7 Hindi validated tools were available while for HADS a Hindi tool by forward backward translation was used. The institutional Ethics committee duly approved this longitudinal analysis (AIIMS/IEC/23/108) and it complies with the Helsinki Declaration.
STATISTICAL ANALYSIS
Demographic data for continuous variables is displayed as mean ± standard deviation, while the demographic data for categorical variables is displayed as frequencies and percentages. The univariate association between the variables and survival was measured using the Cox Proportional Hazards regression. The variables found significant at an alpha of 0.05 were then analysed using multivariate Cox Proportional Hazards regression. The assumption of Proportional hazards was checked by the cox.zph function in the package “survival” of R statistical software, version 4.0.3 used to analyse the data.
RESULTS
PATIENT CHARACTERISTICS
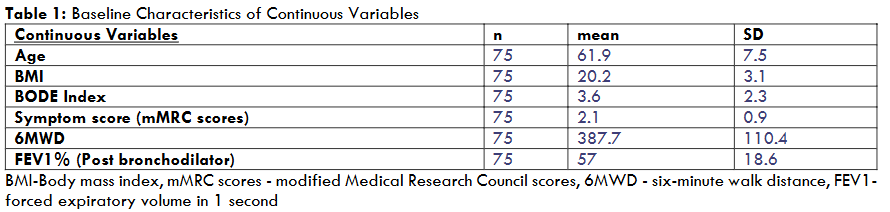
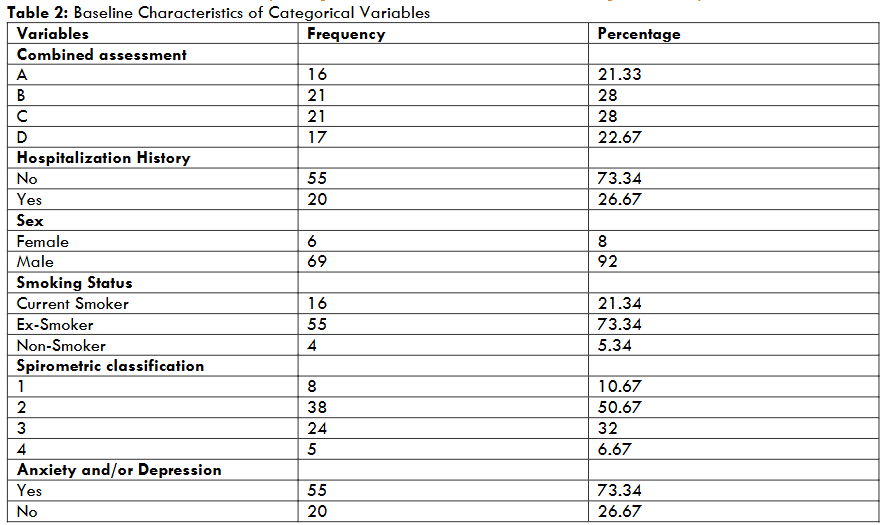
Out of 130 participants at baseline, 75 responded telephonically and were included in the analysis. Out of 75 patients whose outcome was known, 92% were males, and 9% were females with a mean ± standard deviation (SD) age of 61.9±7.5 years. 21.34% were smokers, 73.3% were ex-smokers, and 5.34% were non-smokers. Symptom scores in terms of the mMRC Scale were 2.1 ± 0.9 (mean+ SD), and Body Mass Index (BMI) was 20.2±3.1. Post bronchodilator FEV1% was 57 ± 18.6 (mean ± SD), with 10.67% with mild, 50.67% with moderate, 32% with severe, and 6.67% with very severe obstruction as per GOLD guidelines. Patients were evenly distributed in combined groups B and C, with 28% in each, 21.3% in A and 22.6% in group D, respectively. 26.6% of patients were hospitalised, and 6 MWD was 387.7 ± 110.4 metre (mean ± SD). The BODE index had a mean score of 3.6 ± 2.3, while 73.3% had anxiety and/or depression.
| Continuous Variables | n | mean | SD |
|---|---|---|---|
| Age | 75 | 61.9 | 7.5 |
| BMI | 75 | 20.2 | 3.1 |
| BODE Index | 75 | 3.6 | 2.3 |
| Symptom score (mMRC scores) | 75 | 2.1 | 0.9 |
| 6MWD | 75 | 387.7 | 110.4 |
| FEV1% (Post bronchodilator) | 75 | 57 | 18.6 |
| Variables | Frequency | Percentage | |
|---|---|---|---|
| Combined assessment A | 16 | 21.33 | |
| B | 21 | 28 | |
| C | 21 | 28 | |
| D | 17 | 22.67 | |
| Hospitalization History | No | 55 | 73.34 |
| Yes | 20 | 26.67 | |
| Sex | Female | 6 | 8 |
| Male | 69 | 92 | |
| Smoking Status | Current Smoker | 16 | 21.34 |
| Ex-Smoker | 55 | 73.34 | |
| Non-Smoker | 4 | 5.34 | |
| Spirometric classification | 1 | 8 | 10.67 |
| 2 | 38 | 50.67 | |
| 3 | 24 | 32 | |
| 4 | 5 | 6.67 | |
| Anxiety and/or Depression | Yes | 55 | 73.34 |
| No | 20 | 26.67 |
UNIVARIATE ANALYSIS
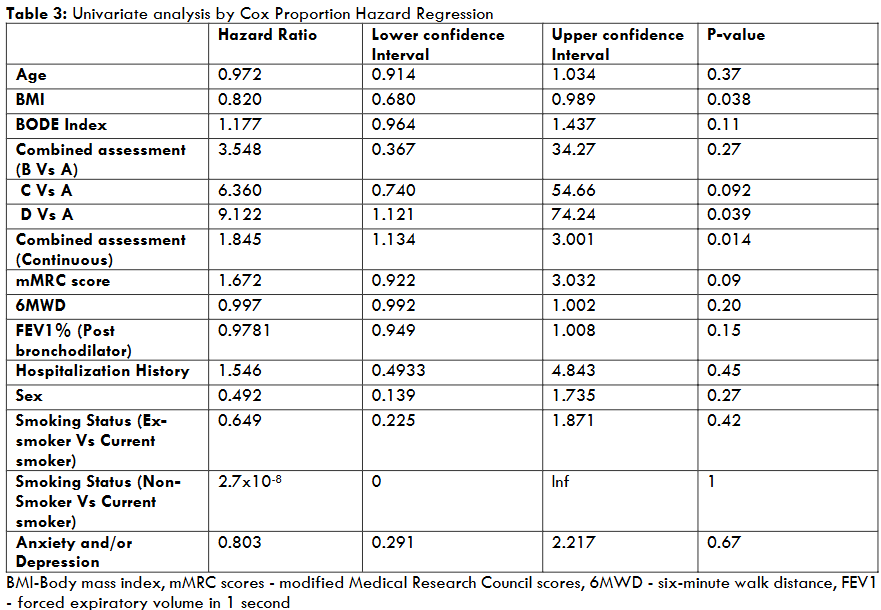
Only BMI and Combined assessment were found to be significantly associated with survival by the Cox Proportional Hazards test at an alpha of 0.05. The test for proportional hazards assumption failed to demonstrate any violation of the assumption at an alpha of 0.1. Age, gender, BODE index, smoking status, symptom score, spirometry variables, 6MWD and anxiety/depression did not show any significant association.
| Hazard Ratio | Lower confidence Interval | Upper confidence Interval | P-value | |
|---|---|---|---|---|
| Age | 0.972 | 0.914 | 1.034 | 0.37 |
| BMI | 0.820 | 0.680 | 0.989 | 0.038 |
| BODE Index | 1.177 | 0.964 | 1.437 | 0.11 |
| Combined assessment (B Vs A) | 3.548 | 0.367 | 34.27 | 0.27 |
| C Vs A | 6.360 | 0.740 | 54.66 | 0.092 |
| D Vs A | 9.122 | 1.121 | 74.24 | 0.039 |
| Combined assessment (Continuous) | 1.845 | 1.134 | 3.001 | 0.014 |
| mMRC score | 1.672 | 0.922 | 3.032 | 0.09 |
| 6MWD | 0.997 | 0.992 | 1.002 | 0.20 |
| FEV1% (Post bronchodilator) | 0.9781 | 0.949 | 1.008 | 0.15 |
| Hospitalization History | 1.546 | 0.4933 | 4.843 | 0.45 |
| Sex | 0.492 | 0.139 | 1.735 | 0.27 |
| Smoking Status (Ex-smoker Vs Current smoker) | 0.649 | 0.225 | 1.871 | 0.42 |
| Smoking Status (Non-Smoker Vs Current smoker) | 2.7×10-8 | 0 | Inf | 1 |
| Anxiety and/or Depression | 0.803 | 0.291 | 2.217 | 0.67 |
MULTIVARIATE ANALYSIS
The multivariate analysis allows for the simultaneous consideration of multiple variables, accounting for their combined effects on mortality. In this analysis, both BMI and combined assessment demonstrate significant association with mortality, and including both these variables improves the overall model fit.
BMI: After controlling for other variables, BMI has an HR of 0.8242, with an LCI of 0.6792 and a UCI of 1. The p-value is 0.0503, indicating a borderline significant association between BMI and mortality. The overall p-value for the model is 0.004, suggesting that the model including BMI as a predictor variable is statistically significant. The proportional hazards assumption has a value of 0.36, indicating that the assumption holds for BMI.
Combined assessment: Considering the continuous variable for COPD combined assessment, the HR is 1.826, with an LCI of 1.107 and a UCI of 3.011. The p-value is 0.01832, indicating a significant association between Combined assessment and mortality. However, the likelihood ratio test yielded a chi-square statistic of 11 on 2 degrees of freedom, with a p-value of 0.004, indicating that the model as a whole is statistically significant. The proportional hazards assumption has a value of 0.66, suggesting that the assumption holds for Combined assessment.
| Hazard ratio | Lower Confidence interval | Upper confidence Interval | P-value | Overall P- Value | |
|---|---|---|---|---|---|
| BMI | 0.824 | 0.679 | 1 | 0.050 | 0.004 |
| Combined assessment 1(Continuous) | 1.826 | 1.107 | 3.011 | 0.018 |
DISCUSSION
Studies on mortality prediction among COPD patients suffer from heterogeneity in terms of both enrolled subjects and prediction tools analysed, ranging from clinico-demographic features to spirometric, radiological and novel tools. Moreover, studies from low and middle-income countries (LMIC) are lacking, limiting the generalisation of results from high income countries. In the present study, out of 130 participants at baseline whose records were complete, 75 responded telephonically and were included in the analysis with a mortality rate of 26.6%. Univariate analysis showed that BMI and combined assessment tool, were associated with mortality, which was confirmed by multivariate analysis while other demographic variables, mMRC scores, FEV1, exercise capacity or psychiatric co-morbidities showed no significant association.
In a retrospective cohort study among 1729 stable COPD patients from China listed in a database and classified into more versus less symptomatic groups (based on GOLD 2017), a significant association in a multivariate model with age (> 65 years) (OR = 2.047, 95% CI = 1.020-4.107), smoking status and COPD assessment test scores (CAT) (more than 30) (OR = 2.609, 95% CI = 1.339-5.085) for mortality was seen over 18 months follow-up. Contrary to this study, we found no significant association between age/symptom scores and mortality, though we used only mMRC and not CAT scores at baseline. Similar to this study, we found no significant association between gender, FEV1 and mortality.
In a Korean cohort of 322 COPD patients followed up for 7.3 years (range: 0.1–12.4 years), among whom 56(17.6%) died found lower thoracic vertebral bone density on chest computed tomograms, older age, lower BMI, lower FEV1, and lower diffusion capacity to be independent predictors of all-cause mortality. Combined assessment was not part of this study as patients were enrolled in a previous time period. Similar to this study, we found BMI to be a predictor, but contrary to this study, age or FEV1 severity did not correlate in our study. Similar to these studies, a study from Malaysia among 112 eligible COPD patients found a 14.2% COPD-associated mortality rate with age, BMI, and CAT scores to be independently associated with mortality on multivariate Cox analysis along with CT emphysema index. Lack of association of age could potentially be due to <70-year age of enrolment of our index study.
A systematic review designed to map and assess multivariable prognostic models for outcome prediction in patients with COPD, including patients in outdoor, indoor and emergency settings, found age, FEV1, sex, BMI, and smoking to be the most commonly used predictors. Endpoints included mortality, risk for acute exacerbation of COPD, and risk for readmission after the index hospital admission. The authors found methodological pitfalls and a low rate of external validation among enrolled studies and concluded that existing models focused on Western populations lacked generalisation and, thus, needed external validation studies in other populations.
There is a lack of studies from India, and our study is a step in this direction. BMI was found to be a significant predictor of mortality in both the univariate and multivariate analyses at the end of 5 years. This is consistent with previous studies that have shown that low BMI is associated with increased mortality in COPD patients. The mechanisms underlying this association may be multifactorial, related to the effects of low BMI on muscle mass, respiratory function, and immune function. A low BMI can also be a marker of increased systemic inflammation, as it is now well-known that COPD is a disease with extrapulmonary manifestations due to systemic spill-over of inflammation. In a dose-response meta-analysis to elucidate the relationship between BMI and mortality, being underweight (BMI<21.75 kg/m2) significantly increased the risk of all-cause mortality by 40%, with a nonlinear relationship between the two.
Combined assessment has been relatively underexplored for mortality prediction, as it is a relatively new entrant and still an evolving tool. It is potentially better than FEV1 as it incorporates both symptoms and a history of adverse events (exacerbations/hospitalisations), thus improving its prediction potential. Despite its various advantages, there is potential underutilisation at the community level both due to lack of awareness and seeming complexity. We found it to be better at predicting mortality than lung functions, mMRC scores and exacerbation history individually, emphasising its potential as both a management and prognostic tool. Other factors that were not found to be significantly associated with mortality in this study included smoking status, functional exercise capacity and anxiety/depression.
Inflammatory biomarkers have been investigated as potential markers for adverse events in COPD trajectory both in isolation as well as in combinations. C-reactive protein (CRP), high-sensitivity troponin I (hs-TnI), proadrenomedullin, with CRP being historically most widely studied, though most studies by non-randomised design and varying cut-offs suffer from methodological heterogeneity. Among novel tools, volumetric CT with Convolutional neural network (CNN) model architecture has also been used for mortality prediction in a recent study. Apart from the above-mentioned tools, multiple variables have been analysed to predict mortality in COPD patients, including haematological and frailty indicators. By their easy availability and applicability, BMI and combined assessment tool can serve as markers of patients prone to adverse outcomes even in the most remote of centres. Nutritional strategies aimed at BMI and timely pharmacological management approaches to improve symptoms and exacerbation events, as components of combined assessment, may potentially improve outcomes among patients with this progressive disease.
CONCLUSION
This study provides insights into the predictors of mortality in stable COPD patients in low-middle-income settings. The findings suggest that BMI and Combined assessment are both predictors of mortality and may perform better than other demographic, spirometric and multivariate tools in stable patients. However, more extensive multicentre studies are needed to validate these findings.
LIMITATIONS
The study has some limitations, including a small sample size and being single centric study. We have not considered all comorbid conditions and inflammatory biomarkers that may potentially impact outcomes and all multivariate prognostic tools. Further research with larger and more diverse populations is needed to confirm these findings.
ACKNOWLEDGEMENT
We would like to extend gratitude to Research cell and staff at AIIMS Rishikesh for all the support.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
This study is an extension of an index study supported by an intramural grant from AIIMS Rishikesh (AIIMS/IEC/23/108).