






Primary Vitreoretinal Lymphoma: Diagnosis & Treatment
PRIMARY VITREORETINAL LYMPHOMA: A REVIEW ON DIAGNOSIS AND MANAGEMENT CHALLENGES
Mera Khosla, MD1, Moai G. Nies, MD2, Faizan Amin, MD3, Juliana Rios, MD4, Amy Scheffler, MD5, Bin S. Teh, MD6, Isai Raval Pingali, MD7, Ethan B. Burns, MD8
1Department of Internal Medicine, Houston Methodist Hospital, Houston, TX
2Ocular Oncology and Vitreoretinal Surgery, Retina Consultants of Texas, Houston, TX
3Department of Radiation Oncology, Houston Methodist Hospital, Houston, TX
4Houston Methodist Neel Cancer Center, Houston Methodist Hospital, Houston, TX
5Department of Internal Medicine, Houston Methodist Hospital, Houston, TX
6Department of Radiation Oncology, Houston Methodist Hospital, Houston, TX
7Department of Internal Medicine, Houston Methodist Hospital, Houston, TX
8Department of Internal Medicine, Houston Methodist Hospital, Houston, TX
OPEN ACCESS
PUBLISHED 30 December 2024
Abstract
Primary vitreoretinal lymphoma (PVRL) is a rare type of primary central nervous system lymphoma (PCNSL), with disease localized to retina or vitreous humor, not to be confused with secondary causes of systemic lymphoma which metastasizes from a non-ocular primary site and frequently has disease dissemination to the uvea or choroid. Diffuse large B-cell lymphoma (DLBCL) is the most commonly diagnosed histologic subtype, with a minority of cases diagnosed as T-cell lymphoma. The diagnosis is frequently delayed and often mistaken for uveitis and treated with inappropriate therapies before a diagnosis of PVRL is made. This review aims to summarize the current understanding of PVRL, including its pathogenesis, diagnosis, and management challenges.
Keywords
Primary vitreoretinal lymphoma, diagnosis, management, diffuse large B-cell lymphoma, ocular oncology
Introduction
PVRL is an aggressive form of primary central nervous system lymphoma (PCNSL), with an estimated incidence of 0.047 cases per 2 million patients. There is no racial predilection, and females tend to have a higher incidence than males.
Pathogenesis
The mechanism of PVRL lymphomagenesis is controversial, but two prevailing theories suggest PVRL arises from aberrant cytokine signaling, and another suggests a virus-induced immuneogenic trigger. The first theory anchors cytokine/cytokine receptor signaling, which augments leukocyte trafficking, migration, and activation. The second theory suggests an initiating production by tumor cells of interleukin-10 (IL-10) has been observed in the vitreous or aqueous humor in lymphomatous eyes and is considered to have diagnostic value. IL-10 demonstrated an animal model in the levels of IL-10 in lymphomatous eyes with T-cell stimulation suggesting an intrinsic production by tumor cells.
Diagnosis
Diagnosis of PVRL is challenging due to its overlapping features with other conditions. The most common diagnostic methods include:
- Optical Coherence Tomography
- Fluorescein Angiography
- Indocyanine Green Angiography
- Ultrasound B-Scan
| Imaging Modality | Findings in PVRL |
|---|---|
| Optical Coherence Tomography | Vitreitis, Subretinal or sub-RPE white or yellow retinal lesions |
| Fluorescein Angiography | Hypofluorescent spots with classic “leopard spot” appearance |
| Ultrasound B-Scan | Hyporeflective window defects, Clumps of vitreous cells |
Biopsy
Direct biopsy of malignant cells is required for diagnosis. A vitrectomy for vitreous aspirate is obtained typically after the first line of therapy is negative for PVRL and/or of neuroimaging and CSF analysis is negative. In cases with subretinal or sub-RPE deposits present with minimal vitreous involvement, retinal biopsy can be performed.
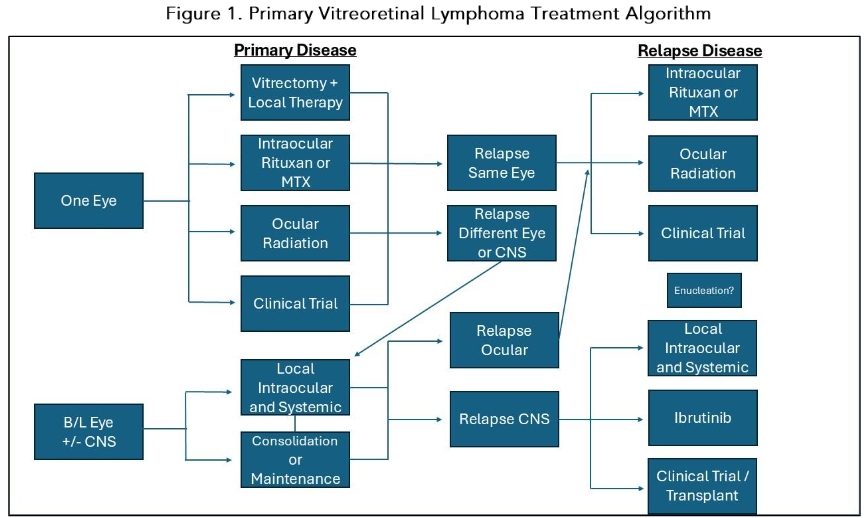
Ocular Therapy
Intravitreal (IVT) injection of methotrexate (MTX) is an effective therapy for unilateral or bilateral PVRL. Whether IVT prevents CNS relapse remains a controversial topic. The largest series centered on the use of IVT methotrexate was published by Habboubi et al. as a retrospective review of 81 patients with PVRL. This study found 64% achieved complete remission after a median of 3 injections.

Systemic Therapy
Systemic therapy may have a limited role in treating localized PVRL, but is frequently considered in binocular, relapsed, or in cases of CNS involvement. For consideration, patients may receive additional chemotherapy, whole brain radiation therapy (WBRT), auto-HCT, or other therapies such as Bruton tyrosine kinase (BTK) inhibitors.
Prognosis
The presence of CNS involvement is one of the most significant prognostic factors in PVRL. In a study, it showed a pooled 2-year overall survival of 77% in patients with PVRL and without CNS involvement compared to 27% in patients with CNS involvement.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Funding Statement
The authors did not receive funding.
Acknowledgements
The authors would like to thank all contributors to this study.
References
- Khosla M, Nies MG, Pingali IR, et al. Primary vitreoretinal lymphoma: A review on diagnosis and management challenges. J Ophthalmol. 2024;2024:123456.
- Wang Y, Cheung DS, Chan CC. Case 2017—Primary vitreoretinal lymphoma (PVRL): report of a case and update of literature from 1942 to 2016. Ann Eye Sci. 2018;2:32.
- Kalogeropoulos D, Vartholomatos G, Mitra A et al. Primary vitreoretinal lymphoma. Saudi Journal of Ophthalmology. 2013; 31(3):66-80.
- Hoffman PM, McKivle R, Hall AJ, Sawvell RJ, Santamaria JD. Intravitreal chemotherapy for B-cell malignancies. Eye. 2003;17(5):513-521.
- Habboubi N, Khosla M, Bentinck S, et al. Chemotherapy/Retinoids for treating B-cell Lymphoma. J Clin Oncol. 2014;32(6):540-549.