





Prophylactic Antibiotics in Acute Deep Dermal Burns Study
Role of Prophylactic Systemic Antibiotics in Acute Deep Dermal Burns: A Comparative Study in a Tertiary Burn Care Centre
Dr Bhupendra Prasad Sarma 1; Dr Prajna P Y 2
- NEMCARE hospital, Guwahati, Assam, India
- NEMCARE Hospital, Guwahati,Assam, India
OPEN ACCESS
PUBLISHED: 31 January 2026
CITATION: Sarma, BP., Y, and Prajna P., 2026. Role of Prophylactic Systemic Antibiotics in Acute Deep Dermal Burns: A Comparative Study in a Tertiary Burn Care Centre. Medical Research Archives, [online] 14(1).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v14i1.7243
ISSN 2375-1924
ABSTRACT
Introduction: Infection in the burn patient is a leading cause of morbidity and mortality. Strict aseptic measures, constant wound surveillance with regular sampling for culture growth, early excision and wound closure remain the principal adjuncts to control invasive infection in burn wounds. Numerous studies show prophylactic antibiotics has a role in prevention of burn wound infections in severe burns. There is a controversy as to whether prophylactic antibiotics have a role in burn wounds below 40% of total body surface area.
Materials & Method: 100 patients presenting with acute deep dermal burns with 20-40% total body surface area were randomly assigned to two groups in which one group received prophylactic antibiotic of Pipericillin and Tazobactum for 7 days and the other group did not receive any antibiotics. Physical examination of the wounds and wound swabs were taken at regular intervals to assess burn wound infection. Wound swab culture was also done on specified date to find any bacterial growth. Burns wounds were treated according to our burn unit protocol. The study ended when wound healing was complete or the patient developed an established wound infection.
Result: The mean age of the participants was 37 yrs, the average percentage of burn severity was 28.7%, incidence rate of burn wound infection in the antibiotic group was 37.5% and in the no-antibiotic group was 25%. Organisms isolated from burn wounds were Pseudomonas, Acinetobacter, E. coli, and Staphylococcus. The average hospital stay was 7.6 days. Statistical analysis showed no significant association between antibiotic usage and prevention of burn wound infection in acute deep dermal burns of 20-40% total body surface area.
Conclusion: The study concluded that prophylactic systemic antibiotics have no beneficial role in preventing burn wound infection in 20-40% total body surface area burns, though there is a need for randomized control trials to assess further.
Keywords: Burns, Deep-dermal, Antibiotic prophylaxis
Introduction
Burn injuries are one of the significant health hazards, resulting in the exposure of intact skin or tissues to extreme heat sources from various forms of energy primarily by thermal forms of energy which include flames, flash burns, and hot objects, followed by other sources such as chemical, electricity, and radiation. Though burns pose a major health problem throughout the globe, the impact on low and middle-income countries was observed to be comparatively higher when compared to other regions. According to the World Health Organization (WHO), it has been estimated that 180000 deaths have been attributed to burn injuries annually. Asia accounted for nearly half of the global burden of burn injuries (46%), deaths (47%), and Disability-adjusted life years (46%). Among the Asian regions, Southeast Asia was the most affected one, contributing a substantial burden of cases.
The increased burden of burn injuries in low and middle-income countries can be attributed to the wide prevalence of poor socio-economic conditions, and cultural practices that increase the exposure the burn injuries particularly making children and women vulnerable. Besides the above-mentioned factors, rapid industrialization added by poor safety regulations that led to an increased prevalence of work-related burns.
Infection of the burn wounds is the leading cause of mortality and morbidity in burns. Inadequate infrastructures, paucity of resources, lack of trained manpower, poor personal hygiene are some of the causes of the prevalence of burn wound infection. 75% of all deaths in burns exceeding 40% total body surface area (TBSA) are due to burn wound infection. Hence infection remains one of the most challenging concerns for the burn team. The importance of preventing infection has been recognized by organized burn care units and hence strict antiseptic and aseptic measures have been followed. This included use of sterile gloves and dressing materials, wearing masks for dressing changes, and separation of patients, either using separate rooms or cubicles. The overall incidence of burn wound infection of the hospitalized patients was considerably high (60%) and majority of them (47%) developed the manifestation of wound site infection within the first week of initial injury.
The burden of wound infection in burn injury can be attributed to complex interconnected factors, one such contributing factor is depth of the burn injury, in which full-thickness or third-degree burns are associated with an elevated risk of infection compared to partial thickness or superficial burns. The infection is attributed to extensive damage to the skin, leading to the formation of favorable environment for colonization and proliferation of microbial organisms. Widespread use of early excision of full thickness burns has improved survival by preventing wound infection to a large extent. Burns provide an optimized medium for bacteria to proliferate and enter the bloodstream. The epithelial barrier loss, hyper metabolic state and immune-suppression predispose to infection in burn patients. The severity and depth of burn injury associated with extensive tissue damage is directly proportional to increased infection rate among the patients. The burn itself is a source of local and systemic complications as it leads to a dysfunction in the immune system, a higher bacterial load, the risk of bacterial translocation within the gastrointestinal tract, longer hospital length of stay and a variety of diagnostic and therapeutic interventions that may have devastating complications. Alternative sources of infection other than wound infection in burn patients include pneumonia, catheter associated infections and thrombophlebitis.
Early excision of burn wound and skin grafting has significantly improved the outcomes for severe burn injured patients by reducing mortality rate and days of hospital stay. However, slow wound healing, infection, pain, and hypertrophic scarring continue to remain a major challenge in burn management in such patients. Among patients with severe burn injuries, prophylactic antibiotics play a vital role in improving patient outcomes by reducing mortality and infection rates. While no such significance had been demonstrated by the patients, who were treated for the non-severe burn injury. While there is evidence that suggests the potential benefits, significant controversies exist about the routine usage of prophylactic antibiotics in burn injury patients. A finding from the systematic review revealed that the administration of systemic antibiotics for prophylaxis to manage the infection among patients with burn injuries does not significantly reduce the infection rate or complications among patients with non-severe burns patients.
The rationale for using systemic antibiotics prophylaxis among burn patients is the balance between infection prevention and risks associated with antibiotic resistance. Though a large number of studies have shown beneficial effects of prophylactic systemic antibiotics in severe and extensive burns, studies showing similar or opposite effects in less severe burns are limited. Our study aims to address these gaps by evaluating the role of prophylactic systemic antibiotics for the management of less severe, acute deep dermal burns involving the total body surface area of 20% to 40%.
The aim of the study was to find the role of prophylactic systemic antibiotics in deep dermal burns of 20%-40% total body surface area (TBSA). The objectives however were- (1) To find the incidence of burn wound infection in 20% to 40% burns in two randomized groups of patients (2) To provide a study-based role of the use of prophylactic systemic antibiotics in burn patients with less than 40% total body surface area burn injury in a relatively clean environment. (3) To find the prevalence of different types of organisms in burn wound infection.
Materials and Methods
The study was conducted in the Tertiary Care Burn Unit of NEMCARE Hospital, Guwahati (Assam), India, as a hospital-based prospective comparative study for the duration of 12 months starting from June 2022 to May 2023. The burn unit, which is an isolated and inclusive unit comprising of 10 bedded wards, ICU, dressing room and operation theatre, is staffed with a trained burn team and adopts a standard protocol of treatment. The unit also maintains a standard Infection Prevention Protocol like- (1) Wearing of sterile scrubs for all staff inside the burn unit. (2) Observance of strict aseptic precautions in dressings in the dressing room. (3) Strict hand-washing protocol before and after examining the patients. (4) Strict prohibition of outside food, materials and person as attendants with the patients. (5) Deep cleaning of the burn ward after discharge of every patient. (6) Daily dusting and scrubbing with antiseptic solution of the burn unit (7) Aseptic monitoring of the wards by examining swab culture of the air and the nook and corners of the burn unit every fortnight. The study was conducted after due approval of the Ethical Committee of NEMCARE Hospital. Written and informed consent was also taken from each of the participants of the study. Conflict of interest- There is no conflict of interest in the study.
Inclusion Criteria of the participants were:
- Patients presenting with 20%-40% TBSA acute and fresh burns.
- Patients with deep dermal burns caused by flame, scald, or chemicals.
- Patients aged between 18 and 60 years.
Exclusion Criteria were:
- Patients with established wound infections or systemic infections at presentation.
- Patients with inhalation injuries.
- Patients with electrical burns, superficial burns, or full-thickness burns.
- Patients treated outside before presenting to the burn unit.
- Patients with systemic diseases such as carcinoma, renal, or hepatic disorders, or immunosuppressive conditions.
The study included 100 patients who were randomly allocated into two groups, using computer software. Patients in Group A or No Antibiotic group received no systemic antibiotics, while the Group B or the Antibiotic group received Inj. Piperacillin-Tazobactam 4.5 Gm. by intravenous route every 8 hours a day for 7 days, as prophylactic antibiotic. The patients in both the groups were treated similarly according to our burn unit protocol. The burn wounds of the patients were assessed for percentage of TBSA Burn, using the Rule of Nine chart and classified based on depth. Detailed history, physical examination, and systemic evaluations were conducted. Wound swabs were collected on days 1, 4, 7, and 14 for culture and sensitivity testing. Wounds were managed by dressings with appropriate topical agents and burn wound covers, as per the protocol of the burn unit. Signs of infection like, fever, slough formation or discharge from the wounds were monitored, and wound swabs were also taken in cases of suspected infection even on non-specified dates. The endpoint of the study was determined as complete wound healing or development of established infection.
Statistical Analysis
The study employed descriptive statistics to summarize variables like age, total body surface area, and white blood cell (WBC) counts, presenting means, standard deviations, and ranges. Chi-square tests were used to analyze associations between categorical variables, such as burn percentage categories and infection status, revealing a significant association on Day 4 (p < 0.001) but not on Days 1 (p = 0.456) or 7 (p = 0.150). Similarly, no significant associations were observed between antibiotic usage and infection outcomes on Days 1, 4, or 7. Independent samples t-tests compared WBC counts and hospital stay durations between the antibiotic and non-antibiotic groups, showing no significant differences (p = 0.214 and p = 0.236, respectively). Proportions and percentages were used to describe categorical variables like the prevalence of fever, infection signs, and culture results across time points. Pearson’s correlation was applied to assess linear relationships between continuous variables, though specific results were not detailed. These statistical methods collectively evaluated the study objectives regarding the impact of prophylactic antibiotics on burn wound infections and related outcomes.
Results
The mean age of the patients in the study groups was 37 years, ranging from 19 to 60 years. Out of 100 patients, 62 were males and 38 were females. The average percentage of burn severity was 28.7%. Twenty patients in Group A and 21 in Group B had burn percentage between 20-25% TBSA; 14 in Group A & 12 in Group B had 25-30% TBSA burns; 7 in Group A and 7 in Group B had 30-35% TBSA burns and 11 in Group A and 8 in Group B had 35-40% TBSA burns.
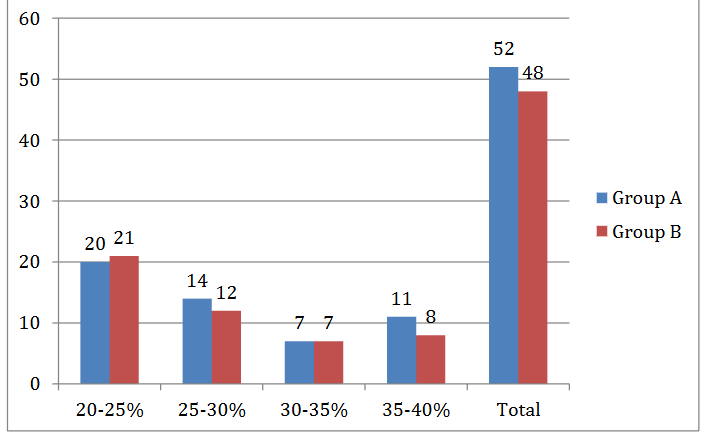
There were 52 patients in Group A, who were not given systemic antibiotics and 48 patients in Group B, who received systemic antibiotics. Majority (80%) of the patients had no co-morbidities. Among those with co-morbid conditions, 10% had hypertension (HTN), 4% had type 2 diabetes mellitus (T2DM), and smaller percentages had other conditions such as asthma (1%) and hypothyroidism (3%).
| Co-Morbidities | Group A Number | Group B Number | Total Number | Percentage of total |
|---|---|---|---|---|
| Hypertension | 6 | 4 | 10 | 10.0 % |
| HTN & T2DM | 1 | 1 | 2 | 2.0 % |
| T2DM | 2 | 2 | 4 | 4.0 % |
| Asthma | 0 | 1 | 1 | 1.0 % |
| Hypothyroidism | 2 | 1 | 3 | 3.0 % |
| No Co-Morbidities | 41 | 39 | 80 | 80.0 % |
The overall positivity for bacterial growth in serial cultures of the wounds revealed 25% in Group A and 37.5% in Group B. Culture results on various days were as follows: bacterial growth was positive in 2 patients in Group A on Day 1; 10 patients had positive growth in Group A and 15 patients in Group B on Day 4; one patient of Group A and 3 patients of Group B showed positive growth on Day 7 and no bacterial growth was detected in any group on Day 14. There was no significant association between antibiotic usage and culture results on Day 1, 4, 7 (p = 0.170), indicating that antibiotics did not significantly alter the infection status within the first few days.
| Antibiotics Usage | Bacterial growth + | Incidence (%) |
|---|---|---|
| NO (Group A) | 13 | 25.0% |
| YES (Group B) | 18 | 37.5% |
| Day | Patient’s Groups | Positive Growth | Negative Growth |
|---|---|---|---|
| Day 1 | Group A | 2 | 50 |
| Group B | 0 | 48 | |
| Day 4 | Group A | 10 | 42 |
| Group B | 15 | 33 | |
| Day 7 | Group A | 1 | 51 |
| Group B | 3 | 45 | |
| Day 14 | Group A | 0 | 52 |
| Group B | 0 | 48 |
Pseudomonas was the most common organism detected, and was present in 2% of cases on Day 1 and increasing to 19% on Day 4. Other organisms, such as Acinetobacter, E. coli, and Klebsiella, were observed less frequently. The average hospital stay of the patients who didn’t receive antibiotics (Group A) was 7.1 + 2.71, with a range from 4 to 19 days, while average stay of the patients, who received antibiotics (Group B) was 8.16 + 3.21 days, with a range from 4 to 20 days. This indicates that there was no significant difference in hospital stay between two groups.
| Groups | Total No of patients | Hospital stay Maximum days | Hospital stay Minimum days | Mean | Standard deviation |
|---|---|---|---|---|---|
| Group A | 52 | 19 | 4 | 7.1 | 2.71 |
| Group B | 48 | 20 | 4 | 8.16 | 3.21 |
| Groups | Number | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|
| Total count WBC Gr. A | 52 | 15529.81 | 2678.13 | 9800 | 21000 |
| Gr. B | 48 | 16284.38 | 3339.50 | 9800 | 25100 |
| Hospital Stay in Days Gr. A | 51 | 7.27 | 2.58 | 4 | 17 |
| Gr. B | 48 | 7.98 | 3.28 | 4 | 20 |
Independent Samples T-Test Results for White Blood Cell Counts and Hospital Stay Duration.
| Statistic | df | p | |
|---|---|---|---|
| Total count WBC | Student’s t -1.25 | 98.0 | 0.214 |
| Hospital Stay in Days | Student’s t -1.19 | 97.0 | 0.236 |
Discussion
The present study was undertaken amongst the patients with 20%- 40% deep dermal burns (moderately severe burns), treated in a clean environment with the aim to find the incidence of burn wound infection with and without prophylactic systemic antibiotics. Most of the patients belonged to the reproductive and middle age groups. There were more males than females in our study. Muthukumar V et al in a retrospective study enrolled 157 patients with the mean age of 31.4 years, almost similar to the present study. They had 51% of males. While the average burn severity amongst our studied participants was 28.7%, the referred study conducted at a tertiary burn center, had an average of 47.3% total body surface area burns.
In our study, 20% of the participants had co-morbidities – hypertension being the commonest disease followed by type 2 diabetes mellitus. But the above-mentioned study by Muthukumar V et al excluded patients with diabetes mellitus. The average duration of hospital stay of their patients was also higher (21.48 days) than our study and could be attributed to higher average percentage of TBSA burns of their patients.
In the present study, antibiotics did not affect the infection outcomes throughout the first week of administration. It did not influence the patients WBC count and the length of the hospital stay. Instead, antibiotic administered patients had longer mean duration of hospital stay when compared to the control group. A Northern American prospective cohort study conducted by Sheridan RL et al found low prevalence of Group A streptococci infection during the first five days after burns and patients did not require penicillin prophylaxis. A Cochrane systematic review conducted by Barajas-Nava LA et al, concluded that the effects of prophylactic antibiotics in patients with burns are limited by the volume and quality of the existing research. They also mentioned one small study, which reported a reduction in incidence of pneumonia associated with a specific systematic antibiotic regimen. The conventional use of antibiotic prophylaxis in burn injury patients is also not endorsed by Muthukumar V et al; nevertheless, in some subgroups, such as patients with inhalational burns and those who develop pneumonia, its administration was recommended. When burn patients do not receive antibiotic prophylaxis, pneumonia becomes an independent risk factor for death.
Our study revealed that in the infected burn wounds, pseudomonas was the most common organism isolated, followed by Klebsiella, Staphylococcus, E. coli and Acinetobacter. The wound culture was reported to have highest growth on Day 4 in patients who had 36% to 40% burns followed by 26% to 30% burns. This association was statistically significant. The infection rate declined by Day 7 due to effective infection control measures and wound management. There was no growth seen on Day 14 in any of the wound samples. Almost similar to our findings, Yeong EK et al reported that the risk of wound infection decreased from 45% at week 1 post burn to 10% at week 4 after using systemic antibiotic prophylaxis for 2–14 days after admission. Furthermore, within the first week following the burns, there were no bloodstream infections. But, unlike our study, the top three wound pathogens that were cultured in their study were Candida albicans, Klebsiella Pneumonae, and multi drug resistant Acinetobacter baumannii. This study included patients from mass burn casualties.
While the controversy regarding the role of prophylactic systemic antibiotics in acute deep burn wounds is going on, the Practical Handbook of Burns Management published by National Program for Prevention, Management and Rehabilitation of Burn Injuries, India, states that, the use of prophylactic antibiotic is to be discouraged since it has not shown to lower the risk of infection. According to ISBI practice guidelines from 2016, prophylactic systemic antibiotics do not prevent sepsis and should be avoided. They suggested that wound microbiology should be monitored in settings with limited resources and that antibiotic prophylaxis may be helpful. The present study done in burns between 20% – 40% total body surface area, found no significant difference in infection rate amongst the antibiotic and non-antibiotic groups and also in length of hospital stay in both the groups of patients. Hence use of prophylactic antibiotics in such patients could not be recommended. This statement is consistent with the findings of Ramos GE, who, in a review article (from 1966 to 2006), inferred that severe infections are uncommon in mild to moderate burn patients and systemic antibiotic prophylaxis did not seem to affect the outcome, hence, there is no current evidence to support its indication. Although most of the reported trials in that study had low quality score, the lack of prophylaxis effectiveness was consistent across them. Consequently, a strong recommendation was not to use prophylactic antibiotics in this group of patients. The same study also depicts uncertainty on the efficacy of systemic antibiotic prophylaxis in perioperative period and even in extensive burns. Finally, prophylaxis could be useful for the prevention of split-thickness skin graft infection in elected procedures.
Ramos G et al, in another systematic review also concluded that available evidence does not support the role of systemic antibiotic prophylaxis in the management of the majority of burn patients. Nevertheless, it may be useful in patients with severe burns who require mechanical ventilation, and in selected split-thickness skin grafting procedures. Avni T et al in a systematic review and meta-analysis of 17 trials, inferred that prophylaxis with systemic antibiotics has a beneficial effect in burns patients, but the methodological quality of the data is weak. As such prophylaxis is currently not recommended for patients with severe burns other than perioperatively, there is a need for randomized controlled trials to assess its use. Takashi Tagami et al identified 2893 severe burns patients, treated at 583 hospitals in Japan, between July 2010 and March 2013. Their analysis revealed that prophylactic antibiotics use may result in improved 28-day in-hospital mortality in mechanically ventilated patients with severe burns but not in those who do not receive mechanical ventilation. Another review article by Jessica Dowling commented that all studies relating to prophylactic antibiotics in burns analyzed in that review had inconclusive results. Ramos et al described no benefit in systemic antibiotic prophylaxis. This was also supported by Muthukumar et al. Contrastingly, Yeong et al. suggested that systemic antibiotic prophylaxis was beneficial in burns. However, it must be noted that the particular study was carried out following a mass burn casualty incident. All authors were aware and exhibit the limitations of their studies namely single centered studies with lack of power calculation and non-standardized data collection techniques. John Weber et al, also commented that systemic antimicrobial treatment must be thoughtfully considered in the care of the burn patient to prevent the emergence of resistant organisms. The burn wound will always be colonized with organisms until wound closure is achieved and administration of systemic antimicrobials will not eliminate this colonization but rather promote emergence of resistant organisms. If antimicrobial therapy is indicated to treat a specific infection, it should be tailored to the specific susceptibility patterns.
Conclusion
This prospective, randomized study done in one year period and in limited number of patients, found no significant difference in infection rate amongst the antibiotic and the non-antibiotic groups. Hence it could be concluded that prophylactic systemic antibiotics has no role in prevention of burn wound infection in acute burns of less than 40% TBSA.
Acknowledgement
We thank the management of NEMCARE Hospital, Guwahati for allowing us to conduct the prospective study and also for allowing us to publish the manuscript.
References
- Tolles J. Emergency department management of patients with thermal burns. Emerg Med Pract. 2018 Feb; 20(2):1–24.
- Burns. World Health Organization [online]. [Cited 2025 Jan 13]. Available from: https://www.who.int/news-room/fact-sheets/detail/burns
- Collier ZJ, McCool K, Magee WP, Potokar T, Gillenwater J. 58 Burn Injuries in Asia: A Global Burden of Disease Study. J Burn Care Res. 2022 Mar 23;43(Suppl 1):S40–S41.
- Keshri VR, Jagnoor J. Burns in India: a call for health policy action. The Lancet Public Health. 2022 Jan 1; 7(1):E8–E9.
- Gerstl JVE, Ehsan AN, Lassarén P, Yearley A, Raykar NP, Anderson GA, et al. The Global Macroeconomic Burden of Burn Injuries. Plast. Reconstr. Surg. 2024 Mar 1; 153(3):743–52.
- Church D, Elsayed S, Reid O, Winston B, Lindsay R. Burn wound infections. Clin. Microbiol. Rev. 2006 Apr; 19(2):403–434.
- Joan Weber, Albert McManus, and Nursing Committee of the International Society for Burn Injuries: Infection Control in Burn Patients: Burns. 2004 Dec; 30(8):A16-24. doi: 10.1016/j.burns.2004.08.003.
- Zhou S, Xiao S, Wang X, Wang X, Han L. Risk Factors and Pathogens of Wound Infection in Burn Inpatients from East China. Antibiotics (Basel). 2023 Sep 11;12(9):1432. doi.org/10.3390/antibiotics12091432
- Sharma B R (2007) infection in patients with severe burns: causes and prevention there of: Infectious disease clinics of North America 21(3):745-759.
- Wang Y, Beekman J, Hew J, Jackson S, Issler-Fisher AC, Parungao R, et al. Burn injury: Challenges and advances in burn wound healing, infection, pain and scarring. Adv Drug Deliv Rev. 2018 Jan 1; 123:3–17. Doi: 10.1016/j.addr.2017.09.018
- Tagami T, Matsui H, Fushimi K, Yasunaga H. Prophylactic antibiotics may improve outcome in patients with severe burns requiring mechanical ventilation: propensity score analysis of a Japanese nationwide database. Clinical Infectious Diseases. 2016 Jan 1;62(1):60-6.
- Muthukumar V, Arumugam PK, Bamal R. Role of systemic antibiotic prophylaxis in acute burns: A retrospective analysis from a tertiary care center. Burns. 2020 Aug; 46(5):1060-1065
- Sheridan RL, Weber JM, Pasternack MS, Tompkins RG. Antibiotic prophylaxis for group A streptococcal burn wound infection is not necessary. J Trauma Injury Infect Crit Care 2001;51(2):352-5
- Barajas-Nava LA, Lopez-Alcalde J, Roque iFiguls M, Sola I, Bonfill Cosp X. Antibiotic prophylaxis for preventing burn wound infection. Cochrane Database Syst Rev 20136:CD008738Version published: 06 June 2013 doi.org/10.1002/14651858.CD008738.pub2
- Yeong EK, Sheng WH, Hsueh PR, Hsieh SM, Huang HF, Ko AT, Tai HC, Lai HS, Chang SC. The Wound Microbiology and the Outcomes of the Systemic Antibiotic Prophylaxis in a Mass Burn Casualty Incident. J Burn Care Res. 2020 Jan 30;41(1):95-103.
- Ministry of Health and Family Welfare. Government of India. National Programme for Prevention, Management and Rehabilitation of Burn Injuries (NPPMRBI). Practical Handbook of Burns Management. Available from: https://dghs.gov.in/WriteReadData/userfiles/file/Practical_handbook_revised_Karoon.pdf
- Allorto N, Atieh B, Bolgiani A, Chatterjee P, Cioffi W, Dziewulski P, et al.ISBI practice guidelines for burn care – part 2. Burns 2018;44(7):1617-706. Doi: 10.1016/j.burns.2018.09.012
- Ramos GE. Antibiotic Prophylaxis in Burn Patients: A Review of Current Trends and Recommendations for Treatment. J. Infectiology. 2018; 1 (1): 1-5.doi.org/10.29245/2689-9981/2018/1.1105
- Ramos G, Cornistein W, Cerino GT, Nacif G. Systemic antimicrobial prophylaxis in burn patients: systematic review. J Hosp Infect. 2017 Oct;97(2):105–14.
- Avni T, Levcovich A, Ad-El DD, Leibovici L, Paul M. Prophylactic antibiotics for burns patients: systematic review and meta-analysis. BMJ. 2010 Feb 15; 340:c241.
- Jessica Dowling. An update on the role of antibiotic prophylaxis for preventing burn wound infections in burn patients. Anesthesia & Surgery Open Access Journal Doi: 10.33552/ASOAJ.2024.05.000617