

Proprioceptive Mandibular Advancement in Orthopedics
Dento Maxillo Facial Orthopedics: Proprioceptive Functional Mandibular Advancement Appliance
Rivero JC, MD, DDS1, PhD.; Rivero C2
- Rivero JC, MD, DDS, PhD Professor of Prophylaxis, Pediatric Stomatology, and Orthodontics. Complutense University of Madrid, Spain. Director of Master’s Degree in Orthodontics and Dentofacial Orthopedics, LaSalle University, Madrid, Spain. Director of Master’s Degree in Orthodontics and Dentomaxillary Orthopedics, San Pablo CEU University, Madrid. Spanish Board in Orthodontics & Dentofacial Orthopedics. Active EOS Member. Honorary Member and Honorary Award EAS (European Aligner Society).
- Rivero C Graduate in Dentistry, U. San Pablo, CEU, Madrid. Master’s Degree in Orthodontics and Dentomaxillary Orthopedics, U. San Pablo CEU, Madrid.
OPEN ACCESS
PUBLISHED 30 April 2025
CITATION Rivero, JC., Rivero, C., et al., 2025. Dento Maxillo Facial Orthopedics: Proprioceptive Functional Mandibular Advancement Appliance. Medical Research Archives, [online] 13(4). https://doi.org/10.18103/mra.v13i4.6444
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6444
ISSN 2375-1924
ABSTRACT
Brief historical/bibliographic review of Dentomaxillary Orthopedics, Classification of mandibular advancement appliances and their usefulness as orthopedic therapy in the correction of skeletal class II, with mandibular hypoplasia. We also present a new device, which we call Proprioceptive Functional Appliance, AMAR™, its physiological principles, design, manufacturing, clinical management and uses in the correction of class II with mandibular hypoplasia, and its improvement in the craniofacial development of growing patients. We report three clinical cases.
Keywords: Functional dento maxillo facial orthopedics, skeletal class II, malocclusion, mandibular hypoplasia, Functional Proprioception, AMAR™, Mandibular advancement. Clinical cases.
A – Introduction
Mandibular advancement is a physiological act or movement of the mandible as a structural and organic part of the stomatognathic complex. This movement is not only in the sagittal plane, but also develops in the vertical and transverse plane, closely linked to the mandibular condylar movements and trajectories, related to the structures of the temporal bones (glenoid fossae, eminences, etc.) articular and muscular on both sides, which must function in a synchronized manner. There are not two Temporomandibular Joints, but only one, but double, the right and the left. One cannot function independently of the other.
The physiological stimulus that the muscles exert on the bone structures, through the ligamentous and articular insertions, determines an increase in the growth of the primary and secondary cartilages, and the remodeling of the bones.
When the functions of the Stomatognathic System are adequate and balanced, the forces generated, as a consequence of these functions (respiratory, labial, lingual, masticatory, etc.), and without bad habits, provide an environment in which all structural parts will grow and develop harmoniously. If due to various etiopathogenic factors, any of these functions is not balanced, the structures will not develop adequately, and dental and skeletal malocclusions will arise, which can be very varied and individual, generating a Malocclusive Syndrome.
We define Class II Syndrome, as a malocclusion in the sagittal plane of dental, alveolar and/or skeletal cause that is relative to the transverse and vertical problem and therefore, it could be defined as the relationship resulting from the correlation of the jaws in the three planes of space, determined by the congenital neuromuscular pattern and its interaction with the environment, in which the mandible is located behind the maxilla in the sagittal sense.
Among the possible consequences of malocclusion are dentoalveolar and/or maxillary skeletal protrusion, mandibular retrognathism and the lack of harmony of the transverse and vertical components or a sum of all of them. However, we make a clear distinction between dental malocclusion defined by Angle, and skeletal malocclusion. As well as the obvious difference between class II, division 1 and division 2, since they are totally different entities in terms of neuromuscular, skeletal, dental, functional and genetic patterns. Class II, div 1, appears in meso/dolic patterns. Class II, div 2, appears in brachyfacial, neuromuscular patterns.
All of this generates disharmonies and imbalances in the vertical vector of facial growth and development, which are determinants in diagnosis and treatment planning. When, after a rigorous analysis and diagnosis, and after considering the chronological moment, dental development, arch development, neuromuscular pattern, bone maturation and growth curves, of each patient, the need to stimulate mandibular growth of that particular patient is determined, and under strict professional design and control, Dentomaxillofacial Orthopedic Appliances can be used.
The use of these devices is intended to exert artificial, external and therefore non-physiological forces, with the aim of modulating, stimulating or slowing the growth and development of the jaws.
B – Background / Historical Review, on Mandibular Advancement Appliances
These devices and the orthopedic philosophy that supports them were not always recognized or well accepted by the profession, and it was not until the studies of the functional matrix of Moss, the growth theory of Petrovic and the studies of Woodside, that the bases for the capacity to modulate condylar growth and remodeling began to be laid. In addition, with respect to therapy, there has been, and continues to be, a disparity of opinions on when, how and why treatment should be carried out.
There are multiple causes of this controversy, from the comparison of devices with very different mechanics, the lack of consensus regarding the ages of application, the use of variable and modifiable cephalometric points according to the position of the head and mandible, inconsistencies in measurements, non-randomized or non-randomized samples, no specification of the time of use of devices and their fixed or removable use, lack of control groups, non-homogeneous study groups.
In the meta-analysis carried out by Santamaría-Villegas et al., they selected only 5 of 50 investigations, according to their inclusion criteria and evaluated the effectiveness of removable appliances in increasing mandibular length (measured Co-Gn or Co-Pg) and concluded, in order of effectiveness: Sander Bite Jumping, Twin-Block, Bionator, Harvold Activator and Frankël. This conflicts with the conclusions of Cozza P, in which the order of effectiveness was first Herbst (cemented) followed by Twin-Block.
Pancherz H, in his studies on Herbst Appliance, demonstrated that there were changes in condylar and glenoid fossa remodeling, as well as an increase in mandibular length, containment of maxillary growth and favorable facial changes. Watted N, et al. examined the impact on the temporomandibular joints (TMJ), the condylar shape and position, and the disc-condyle relationship, of the Bionator + extra-oral traction. The underlying reactions were studied by means of magnetic resonance images (MRI) obtained from n = 15 successfully treated patients (mean age 11.6 years).
Rivero JC, et al. conducted a comparative cross-sectional study between two groups of patients (N=10) with skeletal class II, with mandibular hypoplasia, age range between 10-14 years. One group was treated with HBO (Herbst Occlusal Rod) and the other with Twin-Block. Cephalometric values were compared between T0 and T1 between both groups, to determine if there were differences in terms of mandibular advancement obtained, proclination of the mandibular incisor, mandibular posterior rotation, etc. After comparing the means with the Student T test, it was concluded that there were no statistically significant differences between the two groups (p > 0.05). HBO achieved greater advancement, but also greater proclination of the lower incisor and greater secondary mandibular posterior rotation.
In short, we cannot ignore that the results of the vast majority of research indicate that advancement orthopedic appliances have a favorable effect in the correction of mandibular retrognathism. That is, regardless of the lack of consensus on numerous dimensions of functional advancement, it is effective for the correction of CII, Div 1, of mandibular cause.
There is consensus regarding the effect of mandibular advancement devices:
- At the muscular level: re-education of the muscles
- At the dental level: distalization of the upper arch and retroclination of the upper incisors, mesialization of the lower arch and proclination of the lower incisors.
- At the skeletal level: inhibition of maxillary growth and remodeling of the condyle and glenoid fossa.
C – Classification of Advanced Appliances for Class II, with Mandibular Hypoplasia.
Summarizing a lot, we can classify them as:
- Dental supported. – They force mandibular advancement by dental support.
- a. Fixed (Herbst, Forsus, Advancing, POT)
- b. Removable (Twin-Block, HBO, etc.)
- Functional appliances. – They stimulate advancement by stretching the insertion fibers of the muscles. They inevitably have some support and therefore, dento-alveolar effect. (Fränkel, Bimler, etc.)
- Proprioceptive functional appliances. – They really stimulate muscle function in advancement, lateral movements and mastication, by nociceptive-proprioceptive contact on the mucous membranes, minimizing dental contact and the dento-alveolar effect. Its effects are much more basal structural. Among these we include the Bass Plate, Rivero Nociceptive Activator, ANAM.
C.3.A.- FUNCTIONAL PROPRIOCEPTIVE, ANAM®.
The term “nociception” comes from the Latin “nocere” “to harm” and was defined by C. S. Sherrington to distinguish the physiological process (nervous activity) from the subjective and psychological experience of pain. We define nociception (or also nocioception or nociperception) as the neuronal process by which potentially harmful stimuli against tissues or organs are encoded and processed. It is an afferent (sensitive) physiological activity of the Peripheral Nervous System towards the Central Nervous System.
It is produced by the stimulation of specialized free nerve endings called nociceptors or “pain receptors” that only respond to changes above the system’s threshold, whether chemical, mechanical or thermal in nature. Potentially harmful mechanical, thermal and chemical stimuli are detected by free nerve endings called nociceptors, which are found in the skin, on internal surfaces such as the oral mucosa, periosteum, joint surfaces and in some internal organs. The concentration of nociceptors varies throughout the body, being found in greater numbers in the skin and mucous membranes, than on deeper internal surfaces. Nociceptors have a certain threshold, that is, they require a minimum intensity of stimulation before they trigger a signal. Once this threshold is reached a signal is passed along the axon of the neuron into the spinal cord.
Based on these principles, we designed and used the Nociceptive Advancement Activator, which subtly contacts the lingual mucosa below and behind the lower incisors, avoiding contact with the teeth. In this way, a physiological muscular activity of mandibular advancement is unconsciously stimulated, which, during growth periods, increases the development of the mandible and the TMJ, without affecting the maxilla or the teeth.
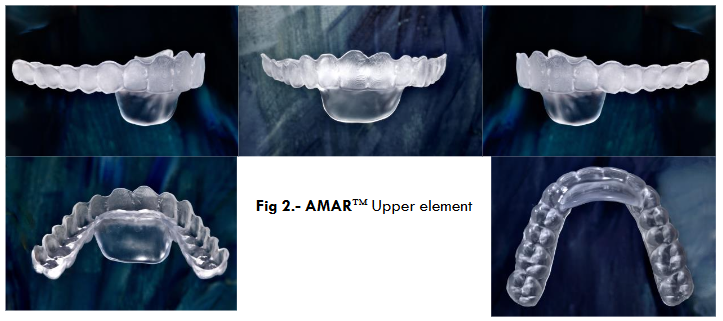
C.3.B. – PROPRIOCEPTIVE FUNCTIONAL APPLIANCE, AMAR™ (MANDIBULAR ADVANCEMENT ACTIVATOR RIVERO™)
It is a double device, upper and lower, independent of each other, thermo-cured methacrylate cap type 0.75 mm thick, ESSIX, or made by stereolithography or 3D printing, which accurately covers the clinical crowns of all teeth. Generically called Sequential Transparent Aligners.

A Protrusion Ramp is incorporated or added to the upper element (maxillary arch) that we call Advancement Platform, which in a sagittal view resembles an “Elephant Trunk”.
The clinical procedure consists of taking records of the working models obtained by intraoral scanning of both dental arches, and of the palatal and lingual mucosa. The interocclusal record must be scanned, faithfully respecting the constructive bite in advance, with a flame-heated Godiva (jig). At 2/3 of the maximum clinical advancement.
The manufacturing is customized, to the exact measurement of each patient and each stage of treatment, by thermo-curing, stereolithography, or 3D printing. Regarding clinical management and given that physiologically a posterior and anterior disocclusion occurs between both arches, motivated by the condylar trajectory, following the articular eminences and, because it is closely related to the neuromuscular pattern of each patient (the more brachyfacial, the more posterior disocclusion), we must manage the vertical development of the posterior dentoalveolar processes and the anterior dentoalveolar dimension (incisal) depending on whether we need to intrude or extrude one or the other, at the same time that we will correct the transverse parameters correlating both arches.
Normally, when advancing the mandible, we will have to expand the upper arch or in severe cases we will have to do Maxillary Disjunction. By incorporating the AMAR™ Advancement Platform to clear aligners of any type, we can also perform all the individual dental movements that are necessary, incorporating as many attachments and auxiliary designs as we need to correct dental malocclusions, during the advancement phases, since there are no wings or occlusal ramps, in the posterolateral sectors, as there are with other elements (Precision Wings™, Twin-Block type ramps, Occlusal Ramps™, etc.)
All teeth have their clinical crowns and occlusal surfaces completely covered, so the upper and lower occlusal plane is completely controlled. If it were necessary to achieve greater anchorage of the appliances, we would design the trimming of the appliances, more towards the gingival, approaching the mucosal border of the maximum contour of the inserted, keratinized gum (Wala Ridge), avoiding the insertion of the buccal and lingual frenulums.
D – Classification of Advanced Devices for Sleep Apnea.
- MAD: Mandibular Advancement Devices. Without mandibular occlusal stability.
- MAP: Mandibular Advancement Positioner. The important thing is to give stability to the mandible in a static, non-functioning position during sleeping hours, and thus increase the permeability of the airways in the lower pharynx or hypopharynx, with repositioning of the hyoid.
E- Recapture Appliances of the Articular TMJ Disc, in Reversible Disc Displacements.
In those cases in which, after a correct clinical diagnosis and after an exhaustive analysis of DEMR (Dynamic Electro Magnetic Resonance of the TMJ), a Disc Recapture is proposed, a MAP or an AMAR™ can be used, if at the same time a corrective orthodontic treatment is planned.
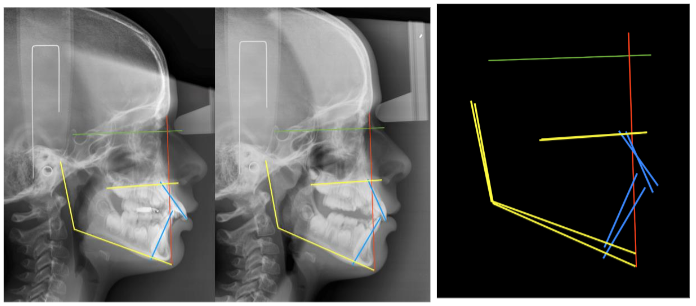
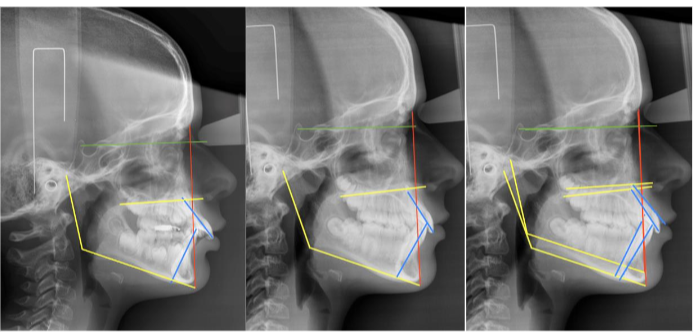
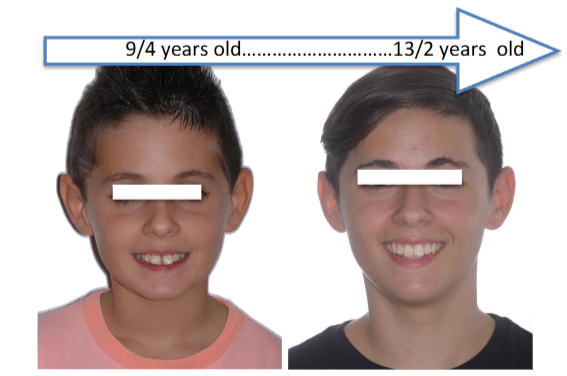
F- FIGURES

E- References/Bibliography
- Enlow DH. Crecimiento MaxiloFacial. 3ª edición. Interamericana McGraw-Hill. HealthCare Group. ISBN 968-25-1737-0. ISBN 07216-2843-5 (Original Ed)
- Proffit WR, et al. Ortodoncia Contemporánea. 6ª Ed. Elsevier. ISBN-13-978-8491134770
- Gershater E, Li C, Ha P, Chung CH, Tanna N, Zou M, Zheng Z. Genes and Pathways Associated with Skeletal Sagittal Malocclusions: A Systematic Review. Int J Mol Sci. 2021 Dec 2;22(23):13037
- Riolo ML, Moyers RE, McNamara JA. An atlas of craniofacial growth: cephalometric standards from the University School Growth Study, University of Michigan Monograph 2 Craniofacial Growth Series Center for Human Growth and Development; University of Michigan, Ann Arbor, 1974; 106
- Bishara SE. Class II malocclusions: diagnostic and clinical considerations with and without treatment. Semin Orthod. 2006; 12:11-24
- Angle EH. Classification of malocclusion. Dental Cosmos 1899;41:248-264
- Thilander B. Basic mechanisms in craniofacial growth. Acta Odontol Scand. 1995 Jun;53(3):144-51
- Williams RE, Ceen RF. Craniofacial growth and the dentition. Pediatr Clin North Am. 1982 Jun;29(3):503-22
- Wroblewski ME, Bevington J, Badik C. Head Growth. Pediatr Rev. 2015 Sep;36(9):426-7.
- Graber TM, Chung DD, Aoba JT. Dentofacial orthopedics versus orthodontics. J Am Dent Assoc. 1967 Nov;75(5):1145-66
- Cleall JF. Dentofacial orthopedics. Am J Orthod. 1974 Sep;66(3):237-50
- Schmuth GP. Considerations of functional aspects in dentofacial orthopedics and orthodontics: Sheldon Friel Memorial Lecture. Am J Orthod Dentofacial Orthop. 1999 Apr;115(4):373-81
- Fränkel R. Functional orthopedics. Am J Orthod Dentofacial Orthop. 2001 May;119(5):11A
- Meikle MC. Remodeling the dentofacial skeleton: the biological basis of orthodontics and dentofacial orthopedics. J Dent Res. 2007 Jan;86(1):12-24
- Manlove AE, Romeo G, Venugopalan SR. Craniofacial Growth: Current Theories and Influence on Management. Oral Maxillofac Surg Clin North Am. 2020 May;32(2):167-175
- Castaldo G, Cerritelli F. Craniofacial growth: evolving paradigms. Cranio. 2015 Jan;33(1):23-31
- Kluemper GT, Spalding PM. Realities of craniofacial growth modification. Atlas Oral Maxillofac Surg Clin North Am. 2001 Mar;9(1):23-51
- Cozza P, Baccetti T, Franchi L, De Toffol L, McNamara JA Jr. Mandibular changes produced by functional appliances in Class II malocclusion: a systematic review. Am J Orthod Dentofacial Orthop. 2006 May;129(5):599
- Santamaría-Villegas A, Manrique-Hernandez R, Alvarez-Varela E, Restrepo-Serna C. Effect of removable functional appliances on mandibular length in patients with class II with retrognathism: systematic review and meta-analysis. BMC Oral Health. 2017 Feb 1;17(1):52
- Vargervik K, Harvold EP. Response to activator treatment in Class II malocclusions. Am J Orthod. 1985; 88:242-251
- Clark WJ. The twin block technique. A functional orthopedic appliance system. Am J Orthod Dentofacial Orthop. 1988 Jan;93(1):1-18
- Pancherz H. Treatment of class II by jumping the bite with the Herbst appliance. A cephalometric investigation. Am J Orthod Dentofac Orthop. 1979;76:423-42.
- Watted N, Witt E, Kenn W. The temporomandibular joint and the disc-condyle relationship after functional orthopaedic treatment: a magnetic resonance imaging study. Eur J Orthod. 2001 Dec;23(6):683-93
- Rivero JC, et al. Hebst versus Twin-Block. V Simposio Internacional de Ortodoncia. 21-23 Febrero 2019. Madrid.
- Foncatti CF, Castanha Henriques JFC, Janson G. Long-term stability of Class II treatment with the Jasper jumper appliance. Am J Orthod Dentofacial Orthop. 2017; 152:663-671
- Bastiani C, Bellini-Pereira SA, Aliaga-Del Castillo A. Twin-block and mandibular anterior repositioning appliances effects in class II malocclusion correction. Am J Orthod Dentofacial Orthop. 2023; 163:181-190
- Janson G, Castello Branco N, Aliaga-Del Castillo A. Soft tissue treatment changes with fixed functional appliances and with maxillary premolar extraction in Class II Division 1 malocclusion patients. Eur J Orthod. 2018; 40:214-222
- Insabralde NM, de Almeida MR, de Almeida-Pedrin RR. Retrospective comparison of dental and skeletal effects in the treatment of Class II malocclusion between Herbst and Xbow appliances. Am J Orthod Dentofacial Orthop. 2021; 160:544-551
- Bilgiç F, Başaran G, Hamamci O. Comparison of Forsus FRD EZ and Andresen activator in the treatment of Class II, Division 1 malocclusions. Clin Oral Investig. 2015; 19:445-451
- Bozkurt AP, Aras I, Othman E. Comparison of 2 treatment protocols using fixed functional appliances in Class II malocclusion: treatment results and stability. Am J Orthod Dentofacial Orthop. 2020; 157:474-480
- Pancherz H. Treatment of class II by jumping the bite with the Herbst appliance. A cephalometric investigation. Am J Orthod Dentofac Orthop. 1979;76:423-42.
- Pancherz H, Bjerklin K. Mandibular incisor inclination, tooth irregularity, and gingival recessions after Herbst therapy: A 32-year follow-up study. Am J Orthod Dentofac Orthop. 2014;146:310-8.
- Howe RP, McNamara J. Clinical management of the bonded Herbst appliance. J Clin Orthod. 1983;17(7):456-63
- McNamara J, Howe RP. Clinical management of the acrylic splint Herbst appliance. Am J Orthod Dentofac Orthop. 1988;94(2):142-49.
- Franchi L, Baccetti T, McNamara Jr J.A. Treatment and posttreatment effects of acrylic splint Herbst appliance therapy. Am J Orthod Dentofac Orthop. 1999;115:429-38.
- Pancherz H. The Herbst appliance- It´s biological effects and clinical use. Am J Orthod Dentofac Orthop. 1985;87:1-20.
- Akan B, Veli I. Evaluation of soft-tissue changes in young adults treated with the Forsus fatigue-resistant device. Am J Orthod Dentofacial Orthop. 2020;157:481-489
- Rivero JC, Roldòs L, Esteve B. Advansync®: otro tratamiento ortopédico de clases II. Ortod Esp. 2012;52(3-4):129-138. ISSN 0210-1637.
- Rivero JC, Pereiro J, Sopeña M. Propulsor Oclusal Telescópico (POT®). Ortod Esp. 2021;59(1):23-43. ISSN 0210-1637.
- Clark WJ. The twin block technique. A functional orthopedic appliance system. Am J Orthod Dentofacial Orthop. 1988 Jan;93(1):1-18
- Vela A, Ponce de León JM, Lasagabaster F, Rico Lillo I. La “bisagra oclusal”: un nuevo aparato de avance mandibular. Rev Esp Ortod. 2002;32:43-7.
- Fränkel R. The treatment of Class II, Division 1 malocclusion with functional correctors. Am J Orthod. 1969 Mar;55(3):265-75
- Bimler HP. Dynamic functional therapy. The Bimler appliance. Trans Eur Orthod Soc. 1973:451-6
- Bimler HP. Bimler therapy. Part 2. Bimler appliance. J Clin Orthod. 1985 Dec;19(12):880-8
- Bass NM. Removable orthodontic appliance. Br Dent J. 1983 May 7;154(9):281
- Armstrong SA, Herr MJ. Physiology, Nociception. 2023 May 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. PMID: 31855389
- Coghill RC. The Distributed Nociceptive System: A Framework for Understanding Pain. Trends Neurosci. 2020 Oct;43(10):780-794
- Sharman MJ, Cresswell AG, Riek S. Proprioceptive neuromuscular facilitation stretching: mechanisms and clinical implications. Sports Med. 2006;36(11):929-39
- Silva MC, Oliveira MT, Azevedo-Santos IF, DeSantana JM. Effect of proprioceptive neuromuscular facilitation in the treatment of dysfunctions in facial paralysis: a systematic literature review. Braz J Phys Ther. 2022 Nov-Dec;26(6):100454