





Psychometric Evaluation of Clinical Leadership in Nurses
Development and Psychometric Evaluation of Registered Nurses’ Clinical Leadership Scale (RN-CLS) in Bangladesh
Abdul Latif1, Nongnut Boonyoung2, and Aranya Chawalit3
- Senior Consultant (Nurse Admin), Capacity Building Nursing Services (CBNS), JICA, Bangladesh. (Ex PhD Nursing Student, Prince of Songkla University, Thailand).
- Associate Professor, Faculty of Nursing, Prince of Songkla University, Thailand.
- Assoc. Professor and Dean, Faculty of Nursing, Prince of Songkla University, Thailand.
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: Latif, A., Boonyoung, N., and Chawalit, A., 2025. Development and Psychometric Evaluation of Leadership Scale (RN-CLS) in Bangladesh. Medical Research Archives, [online] 13(3). https://doi.org/10.18103/mra.v13i3.6386
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6386
ISSN 2375-1924
ABSTRACT
As the largest front-line healthcare workforce, active clinical leadership among nurses is vital for ensuring high-quality patient care and an effective response to the growing needs of healthcare. A number of Clinical Nurse Leadership scales were found in current literature, but none of them were suitable or consistent with the current study context. Hence, the aim of this study was to develop a context specific Registered Nurses’ Clinical Leadership Scale for Bangladesh and evaluate its psychometric properties. An inductive mixed-methods design used in this study as well the specific factor structure of the Scale. The development and psychometric evaluation of the Clinical Nurse Leadership Scale involved a two-phase, eight-step process, beginning with an extensive literature review and culminating in the examination of content validity, face validity, a pilot evaluation, and construct validity using exploratory factor analysis. Inte α coefficient, using data from 627 clinical registered nurses. Contrasted group analysis was performed for known-group validity testing, and test-retest reliability was assessed for stability. The Registered Nurses Clinical Leadership Scale demonstrated an acceptable level of construct validity and excellent internal consistency. Factor analysis identified 9 components for 92 items, accounting for a total variance of 52.06%. ranged from 0.84 to 0.92, across 9 components. These were: assessment and evaluation, patient-centered intervention, imply quality and safety, caring relationship, interdisciplinary collaboration, skills of communication, professional values in caring, decision making or problem-solving and professional development. There was statistically significant difference between low and high. The test-retest result also found significantly high correlation between the test one and two on the scores of the scale (r = 0.92; p<.001). Thus, the final version of the Registered Nurse Clinical Leadership Scale (RN-CLS), consisting of 92 items across nine factors demonstrated high validity and reliability.
Keywords:
Clinical Nurse Leadership, Registered Nurse, Scale Development, Psychometric Evaluation
1. Introduction
Globalization and advances in medical technology are impacting healthcare in Bangladesh by increasing access to quality care, but also posing challenges to meet the growing demands for such care. These changes affect not only the structure of healthcare but also the knowledge and skills of healthcare professionals including nurses in clinical care. As in other countries, nurses in Bangladesh’s public hospitals are the second largest workforce, responsible for providing direct patient care. According to the Directorate of Nursing and Midwifery, more than 95% of nurses are working in different public hospitals as bedside nurse. However, the quality of nursing care in public hospitals is a major concern and is relatively low compared to non-government hospitals or neighboring countries. According to In-depth Country Assessment on Nursing and Midwifery, the issue of this poor-quality nursing care was reported as a direct link to the low reputation and poor image of nursing in Bangladesh.
Regardless of few controversies about the factors associated with the quality of patient care, a number of studies claimed that the poor-quality patient care is largely associated with ineffective role performance and skills of clinical nurses. Yeh et al. identified three major challenges contributing to the lack of access to quality nursing care in Bangladesh: a scarcity of nurses in clinical care, a lack of appropriately skilled nurses, and a lack of professional leadership. Consequently, nursing suffers from poor recognition and receives inadequate priority as an important member of the healthcare team. In addition, due to a lack of updated knowledge, skills, and leadership confidence, nurses are frequently excluded from active participation in clinical care decision-making or clinical change management. Thus, nurses are usually reliant on physician’s order and instruction in managing patient care or taking clinical decisions.
Although it is true that the problem of nursing leadership in Bangladesh is not only on the clinical side, this problem exists at every nursing administrative level. However, problems associated with clinical nursing leadership (CNL) are more acute because they are directly related to patient outcomes and satisfaction. Moreover, the quality of clinical nursing care is the mirror of the quality of nurses and the standard of healthcare services. Thus, given that nurses are the largest frontline workforce, strong clinical leadership is essential for an effective response to the growing needs and reforms that call for innovations to meet patient satisfaction and address evolving healthcare challenges. But unfortunately, nurses in Bangladesh were inadequately prepared with the expected skills to perform their active role as effective clinical leaders and respond to the growing needs in healthcare. In the healthcare of Bangladesh, ineffective professional leadership was reported as a major challenge for advancing the nursing profession. Based on the existing situation, there was a lack of study in Bangladesh to address the issue of clinical leadership, particularly demonstrating identical leadership quality by nurses when they are involved in direct patient care.
At the same time, it was also unknown to what extent existing nurses in Bangladesh were prepared in terms of required clinical skills to meet growing demands in healthcare. Although some related instruments exist in the literature, they have several limitations regarding their validity and reliability within the clinical nursing context of Bangladesh. This is because most of them were not specifically designed for clinical nurses, were developed in Western healthcare contexts, and have demonstrated inadequate psychometric evaluations. Therefore, the researcher in the present study focused on the importance of clinical nurse leadership scale development in the context of nursing and healthcare in Bangladesh. Therefore, this study explored the components of clinical nurse leadership skills to create a context-specific, culturally valid, and reliable measure that would enhance nurses’ knowledge and skills within their scope of practice.
2. Study Aim
This study aimed to develop and evaluate the psychometric properties of Clinical Leadership Scale for the Registered Nurses in Bangladesh (RN-CLS).
3. Methods
Study design:
This study used an inductive mixed-methods research design for the development and psychometric evaluation of the Clinical Leadership Scale of Registered Nurses in Bangladesh (RN-CLS). De Vellis’s guidelines for scale development and evaluation was followed in this study, which consist of two phases with eight steps: Phase 1 (5 steps) and Phase 2 (3 steps).
4. Research Process
4.1. Phase 1: Instrument Development
Step 1: Determining the Content Domains:
The aim of this step was to clarify the concept, determine a related theory, and explore the critical elements of the scale as predetermined components. This step began with an extensive review of related theories, concepts, and existing tools, and included two focus group discussions with 14 nurses from nursing administration, nursing education, and clinical care. Three skills leadership theory was used as theoretical foundation including, Technical Skills, Conceptual Skills, and Human Skills. Finally, based on the skill leadership approach, the American Association of Colleges of Nursing’s concept of the Clinical Nurse Leader (CNL), and the results of focus group discussions (FGDs), 11 predetermined scale components were selected to represent the clinical leadership skills of Registered Nurses (RNs) in Bangladesh. These were: 1) diagnose the genuine problems and needs of the patients, 2) develop patient-centered intervention, 3) imply quality and safety in patient care, 4) monitor and evaluate clinical effectiveness, 5) optimize patient care with the competence in medical technology, 6) establish caring relationship with patients and families, 7) encourage interdisciplinary collaboration, 8) demonstrate understandable communication skills, 9) practice with professional values of nursing, 10) problem-solving and decision-making skills, and 11) participate in enhancing professional advancement.
Step 2: Defining the Target Constructs and Generating the Items:
This step involved specifying a clear objective for each construct, providing operational definitions, and generating the item pool. An explicit operational definition was provided for each of the identified skill categories based on the literature review and the focus group suggestions. Next, grounded on operational definitions and objectives of each skill component of the RN-CLS, a total of 122 items were generated.
Step 3: Determining the Format for the Measurement:
The response format of the RN-CLS was designed as a 5-point Likert-type with a summated rating scale ranged from 1=never perform/practice this skill, to 5= always perform/practice this skill. A norm reference framework was used to guide the design and interpretation of the scale.
Step 4: Examining the Content Validity:
The initial item pool was reviewed by five content experts in nursing and nursing leadership to determine the Content Validity Index (CVI). Experts independently rated each item for clarity and relevance using a four-point scale (1 = not relevant/clear to 4 = very relevant/clear). Ratings of 3 or 4 were used to calculate the Content Validity Index (CVI). The overall Scale Content Validity (S-CVI) was 0.85 and Item Content Validity (I-CVI) ranged from .80 to 1.00 for 122 items. Two items were revised for more clarity, resulting in a total of 124 items after the CVI process.
Step 5: Pre-Testing the Items:
After assessing content validity, formatted questionnaires were sent to five clinical RNs to examine clarity, comprehensiveness, time to answer, and administrative feasibility in a subsequent trial. Next, the RN-CLS was applied for pretesting among 30 clinical RNs in the conditions similar to anticipated study settings and subjects. The RN-CLS was 0.96; and for sub-scales ranged from 0.68 to 0.86. Only 2 items were deleted due to the item-total correlation of <.30. Finally, 122 item pools were used in the final field test of the RN-CLS.
4.2: Phase 2: Evaluation of the Psychometric Properties
This phase consists of three steps. Step-6, a field test was conducted to evaluate the reliability and validity; step-7, to estimate the test-retest reliability; and step-8, to examine the contrast group validity for the final version of the RN-CLS.
Step 6: Administering the Items for Field Test:
After necessary revisions based on the pilot study, the RN-CLS was employed for field test to determine the psychometric properties with a large group of study samples as empirical evidence. This step was performed through employed the RN-CLS in a large sample of clinical registered nurses in two medical college hospitals in Bangladesh. The data were used to evaluate the internal consistency reliability, scale length, and different types of validity.
4.3 Study participants:
This study was carried out in two tertiary level medical college hospitals. These were Dhaka Medical College Hospital (a 2500-bed hospital and the largest in the capital) and Mymensingh Medical College Hospital (a 1000-bed hospital and the largest divisional hospital) in Bangladesh. Of the 890 clinical RNs included in this study, 689 returned the questionnaire, yielding a 76.4% return rate. Sixty-two incomplete datasets (with >10% missing data) were excluded, resulting in a final sample of 627 complete datasets for factor analysis.
4.4 Ethical consideration:
Data collection began after receiving approval from the Institutional Review Board (IRB) of the Faculty of Nursing, Prince of Songkla University, Thailand, and obtaining permission from the selected study settings. Written consent was obtained from study participants after explaining the purpose of the study and emphasizing their voluntary participation. The data were collected and handled anonymously. Because this was a risk-free study, the return of the questionnaire was considered implied consent to participate.
4.5 Data Analysis:
The statistical analysis was performed in two stages using SPSS 16.00 software: first, the data screening using descriptive statistics including the completeness or missing and assumption tests; and the secondly performed descriptive analysis for demographic data and were summarized using descriptive statistics (mean, SD and percentage). Psychometric tests, including construct validity, were examined by Exploratory Factor Analysis (EFA) and the Contrasted Group Technique. Reliability was assessed using Cronbach’s alpha coefficients and test-retest methods for stability. T1 was used as the extracting criterion with varimax and oblique rotation to examine which factors were comprised of coherent groups of items in the scale. The overall score on clinical leadership skills of RN-CLS was calculated by averaging the values of the skills-related items. The item-total correlation matrix also examined by correlation coefficients (r), in which, the items for (r) less than 0.3 were excluded after initial analysis.
5. Results
5.1 Characteristics
Among the 627 study participants, 50% were between 30 and 45 years old (mean = 35.6 ± 9.2 years). The majority of subjects were female (88%), and almost two-thirds (75%) held a diploma as their highest professional nursing qualification. The average job experience was 12.3 ± 8.6 years in the public hospitals, in which nearly 60% were between 21 years and over of the job experiences as clinical nurse. In terms of current job positions, around 88% participants were senior staff nurse (as general RNs and nearly 12% of them were working as staff nurse in-charge from the different units of the hospitals.
5.2 Scale Evaluations
The final evaluation of the RN-CLS included examinations of construct validity and assessments of the scale’s reliability. The construct validity of the RN-CLS was assessed using EFA with orthogonal varimax rotation. Following the assessment of construct validity by EFA and internal consistency using Cronbach’s alpha, further construct validity was examined using the Contrasted Group Technique with two additional groups of study participants. The details of each validity and reliability tests are given below:
Initial item performance: Inter-item and item-total correlation statistics were used to examine the reliability of each item. Based on these results, 22 items with low item-total correlations (<0.30) were excluded from the EFA. The average item-total correlation for the 92 items ranged from 0.30 to 0.64. Because deleting items with low values did not improve reliability, the 92-item scale was retained. The details of the scale reliability results are shown in the Table 1.
Construct validity:
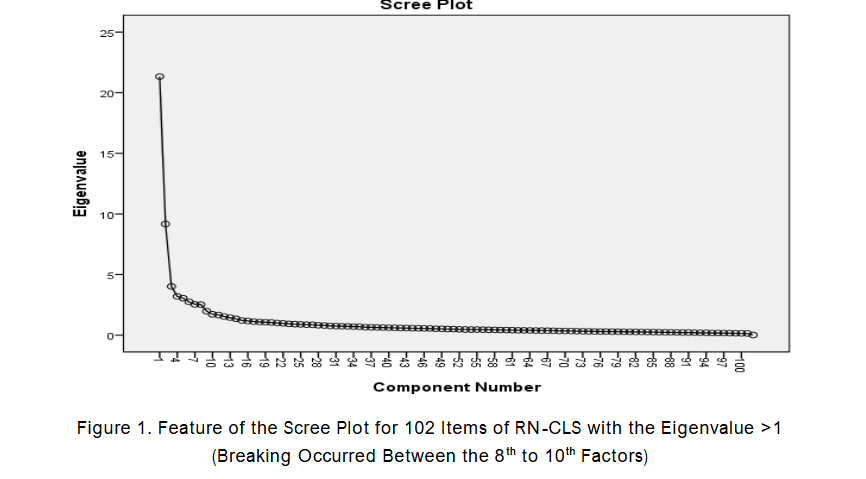
The construct validity of RN-CLS was examined by exploratory factor analysis (EFA) using Principal Component Analysis (PCA) with varimax rotation of factor loadings that sphericity was significant (χ2 = 42961.42, p = 0.000), and the Kaiser-Meyer-Olkin (KMO) value was 0.92 with 102 items. The initial EFA showed 20 factor solutions with eigenvalues of > 1.0 and factor loadings cutoff point at least 0.30. The inspection of the scree plot revealed that an 8 to 10 factor solution was appropriate. After sequential analysis, 9 factor structures were found to be the best factor solution which together accounted for 52.06% variance explained for 92 items with factor loadings cutoff point was at least 0.40, and eigenvalues ranging from 4.01 to 10.25. The results of factor analysis with extracted 9 (nine) factors were showed in Table 1. The results of internal consistency reliability for the scale, overall RN-CLS was 0.96 for 92 items, and across the 09 sub-scales.
Step: 7 Examine Stability Reliability:
The test-retest for stability reliability of the RN-CLS was tested by administering the scale among 30 clinical registered nurses in two time points with 10 days intervals, who were purposively selected. The participants were also asked to mention how long it took them to answer the entire questionnaire including the demographic data form. The results significantly high correlation between two tests and across 9 subscales (r) ranged from 0.73 and 0.91, indicating an acceptable stability between the test sessions. The average duration for answering the whole questionnaires was 30 min.
Table 2: Test-Retest Reliability of the RN-CLS (N=30).
| RN-CLS with 9 Subscales | Test-1 | Test-2 | (r) | Mean (SD) | Mean (SD) |
|---|---|---|---|---|---|
| Assessment and evaluation | 56.0(6.0) | 58.9(8.3) | .88** | ||
| Patient-centered intervention | 49.9(6.1) | 52.4(6.5) | .83** | ||
| Imply quality and safety | 42.1(3.5) | 38.4(4.6) | .91** | ||
| Caring relationship | 35.9(5.3) | 40.5(5.3) | .73** | ||
| Interdisciplinary collaboration | 34.9(3.6) | 37.0(3.7) | .78** | ||
| Skills of communication | 28.93(3.78) | 30.60(3.95) | .78** | ||
| Professional values in caring | 22.46(2.30) | 26.86(2.93) | .86** | ||
| Decision-making | 83.13(8.70) | 89.26(9.74) | .85** | ||
| Professional development | 28.40(4.57) | 29.60(3.17) | .85** | ||
| Overall RN-CLS | 381.8(31.5) | 403.6(39.5) | .92** |
Step:8 Contrasted Known Groups Analysis:
To assess the evidence of construct group validity, the final version of the RN-CLS was administered to two contrasting familiar groups of 60 clinical registered nurses: the high-performance group (n=30) and low-performance (n=30) group. The subjects in the two groups were selected with different known clinical performance and job ensured by the Nursing Supervisor of the hospital. The results of an independent samples t-test indicated a significant difference between the two groups’ mean scores on the RN-CLS (t = 3.872, p < 0.001).
Table 3: RN-CLS (N=60).
| Groups | Score of RN-CLS | t-test | p-value | |
|---|---|---|---|---|
| High-performance group | 418.23 | 41.71 | 3.872 | .000 |
| Low-performance group | 363.33 | 58.32 |
Table 4: The Item Loadings and level of Commonalities of the RN-CLS BD Scale by Items and Factors (N= 627):
RN-CLS Scale and subscale with item loadings.
| Factor’s Name | Eigen-values | Total variance | Number of items | alpha levels | Item-total correlations |
|---|---|---|---|---|---|
| 1. Assessment and evaluation | 8.76 | 7.45 | 14 | .89 | .46-.73 |
| 2. Patient-centered intervention | 3.16 | 6.53 | 12 | .90 | .43-.70 |
| 3. Imply quality and safety | 3.95 | 6.88 | 10 | .91 | .60-.75 |
| 4. Caring relationship | 2.60 | 4.20 | 9 | .84 | .41-.68 |
| 5. Interdisciplinary collaboration | 2.43 | 4.07 | 8 | .85 | .42-.78 |
| 6. Skills of communication | 3.01 | 4.54 | 7 | .86 | .45-.77 |
| 7. Professional values in caring | 1.94 | 4.01 | 5 | .90 | .68-.85 |
| 8. Decision-making | 20.04 | 10.25 | 20 | .92 | .47-.71 |
| 9. Professional development | 2.51 | 4.12 | 7 | .86 | .56-.74 |
| RN-CLS overall scale level | 20.04 | 52.06 | 92 | .96 | .41-.85 |
Step: 7 Examine Stability Reliability:
The test-retest for stability reliability of the RN-CLS was tested by administering the scale among 30 clinical registered nurses in two time points with 10 days intervals, who were purposively selected. The participants were also asked to mention how long it took them to answer the entire questionnaire including the demographic data form. The results significantly high correlation between two tests and across 9 subscales (r) ranged from 0.73 and 0.91, indicating an acceptable stability between the test sessions. The average duration for answering the whole questionnaires was 30 min.
Step: 8 Contrasted Known Groups Analysis:
To assess the evidence of construct group validity, the final version of the RN-CLS was administered to two contrasting familiar groups of 60 clinical registered nurses: the high-performance group (n=30) and low-performance (n=30) group. The subjects in the two groups were selected with different known clinical performance and job ensured by the Nursing Supervisor of the hospital. The results of an independent samples t-test indicated a significant difference between the two groups’ mean scores on the RN-CLS (t = 3.872, p < 0.001).
Table 3: RN-CLS (N=60).
| Groups | Score of RN-CLS | t-test | p-value | |
|---|---|---|---|---|
| High-performance group | 418.23 | 41.71 | 3.872 | .000 |
| Low-performance group | 363.33 | 58.32 |
Table 4: The Item Loadings and level of Commonalities of the RN-CLS BD Scale by Items and Factors (N= 627):
RN-CLS Scale and subscale with item loadings.
| Factor’s Name | Eigen-values | Total variance | Number of items | alpha levels | Item-total correlations |
|---|---|---|---|---|---|
| 1. Assessment and evaluation | 8.76 | 7.45 | 14 | .89 | .46-.73 |
| 2. Patient-centered intervention | 3.16 | 6.53 | 12 | .90 | .43-.70 |
| 3. Imply quality and safety | 3.95 | 6.88 | 10 | .91 | .60-.75 |
| 4. Caring relationship | 2.60 | 4.20 | 9 | .84 | .41-.68 |
| 5. Interdisciplinary collaboration | 2.43 | 4.07 | 8 | .85 | .42-.78 |
| 6. Skills of communication | 3.01 | 4.54 | 7 | .86 | .45-.77 |
| 7. Professional values in caring | 1.94 | 4.01 | 5 | .90 | .68-.85 |
| 8. Decision-making | 20.04 | 10.25 | 20 | .92 | .47-.71 |
| 9. Professional development | 2.51 | 4.12 | 7 | .86 | .56-.74 |
| RN-CLS overall scale level | 20.04 | 52.06 | 92 | .96 | .41-.85 |
6. Discussion
The discussion of study findings was organized in four main aspects: (1) the development of the RN-CLS, (2) the factors structure and psychometric properties of the RN-CLS, (3) the scope and limitations of the study, (4) conclusions and recommendations.
6.1 The Development of the RN-CLS
This study revealed a lack of scales to assess leadership skills among clinical RNs in Bangladesh. Existing scales in the literature have limitations related to context, cultural variations, comprehensiveness, and psychometric evaluations (including tests of validity and reliability). The RN-CLS was developed as a theory grounded, concept and context-specific self-assessment measure to assess the clinical leadership skills of the RNs in Bangladesh. The contents of the RN-CLS development focused on the leadership-related skills and ability to deal with patients, families, coworkers, and interdisciplinary teams. The CVI results were highly acceptable at both the individual item level (I-CVI = 0.80-1.00) and the scale level (S-CVI average = 0.85) on 122 items. Based on expert feedback and suggestions, two new items were added, and several items were modified, resulting in a 124-item scale. Prior to administering the RN-CLS for final evaluation, face validity and a pretest study were conducted. This resulted in the modification of 19 items to improve clarity. The modified and finalized draft, now containing 124 items, was then used in a field test to examine the scale’s psychometric properties.
6.2 Factors Structure of the RN-CLS
Field test data from the RN-CLS were used to examine the construct validity of the RN-CLS. The construct validity of the scale was determined using Exploratory Factor Analysis (EFA) and Principal Component Analysis (PCA) with orthogonal varimax rotation. All necessary assumptions for factor analysis were tested to ensure data appropriateness, and criteria for construct validity were determined based on pre-set standards. The factor loadings cutoff point needs a value like 0.40, demonstrated the 9-factor structure of the RN-CLS with 92 items as an acceptable psychometric evaluation result. The total percentage of variance accounted by 9 factors for 52.06% and across 9 factors variance ranged from 4.01% to 10.25%. According to Suhr (1984) a proportion of variance for each factor of at least 5% is considered good. Given that item loadings to each factor ranged from 7 to 20 items, the content validity of each factor logically (judgement) and empirically (statistical test) were acceptable in terms of covering the areas of contents of the constructs. The overall communalities of the items of the RN-CLS ranged from 0.30-0.78 which reflected a satisfactory correlation of an item with all other items. For item loadings of the scale, even though > 0.30 was acceptable, in this study increased to at least 0.40 (ranging from 0.41 to 0.85) thus improving the reliability of individual items and of the scale as a whole. The was 0.96 for the overall scale and across factors ranging from 0.84 to 0.91. The level of reliability of the RN-CLS in terms of internal consistency was adequate indicating that the scale is reliable. A discussion of each extracted factor and related findings are described below:
Factor 1. Assessment and Evaluation (AE):
The factor consisted of 14 items and was labeled by combining two predetermined components of the initial conceptual framework of the study. Although the 14 items originated from two separate components, the rotated or loaded items were highly consistent, supporting the new label for this factor. The factor loadings ranged from 0.46 to 0.73, indicating a satisfactory level of correlation between each item and the factor. For example, results revealed that 12 out of 14 items had moderate to high levels of correlation, while 2 items had relatively low levels of correlation with the factor. The percentage of variance accounted for was 7.45%, the second highest of the 9 factors, with eigenvalues of 8.76. The internal consistency reliability of Cronbach’s alpha was also acceptable with a value of 0.89. Satisfactory communalities of the items (0.40 to 0.62) demonstrated that each item contributed well to the variance of the factor. The factor of AE in the RN-CLS suggests that clinical registered nurses have the ability to perform an in-depth assessment and follow-up evaluation of each patient to identify critical health problems and promote progress in patient’s condition. The loaded items of this factor indicated the key skills contents of RN’s ability regarding: in-depth assessment of the health status of patients through collecting subjective and objective data, identify clinical changes and critical health problems with its etiology, evaluate risk, estimate a patient’s progress and needs for subsequent follow-up including gaps in existing practices. Thus, all of these key indicators were highly consistent to support the factor’s label.
Factor 2. Patient-Centered Intervention (PCI):
This factor consisted of 12 items with factor loadings ranging from 0.43 to 0.70 and comprised of component of RN-CLS, BD. The percentage of variance contributed by this factor on the total scale of 6.53%, the eigenvalue of 3.16, The high Cronbach’s alpha coefficient of this factor reflected a higher internal consistency among the items in terms of reliability. The individual factor loadings revealed that most of the item loadings (8 items) were above 0.50 to 0.70 indicating high levels of correlation to the factor. However, 4 item loadings had comparatively low item-factor correlation. As for factor loadings, the communalities of items were satisfactory as the observed variance accounted for by a common factor ranged from 0.30 to 0.65. The rotated items of the factor 2 were highly consistent measurement the attributes of PCI. The items of this factor reflected the RN’s ability to: recognize special needs requiring special intervention; conduct a critical inquiry to evaluate needs; respect patient and family preferences, involvement, response to wellbeing. Thus, all of these skill aspects were highly relevant to the PCI factor construct.
Factor 3. Imply Quality and Safety (IQS):
This factor incorporated 10 items with factor loadings ranging from 0.60 to 0.75, illustrating very good strengths in items to factor correlation reflecting a high level of reliability. The total accounted variance for this factor was 6.88%, which was among the highest contributions to accounted total variance in the scale. The eigenvalue of this factor extraction was 3.95 with an internal alpha coefficient at 0.91. The items-subscale correlations in this factor were also high, ranging from 0.59 to 0.77. The factor IQS was viewed as a clinical nurse’s ability to provide care to an individual patient that increases the desired outcomes and are consistent with the current clinical nursing knowledge and practices. The key measuring attributes for this factor were: evidence-based practice and decision-making, current and quality practice, ensure patient safety measures, and measures to prevent anticipated risks. The items for this factor were mostly informed by focus group findings, making the skills reflected in the items very consistent with the nursing care context of Bangladesh. The EFA confirmed the structure of this factor item, in which all items were loaded to this factor with a high loading range; reflecting good content validity. Therefore, it can be inferred that the factor construct was appropriate.
Factor 4. Caring Relationship (CR):
The construct of the RN-CLS was focused on clinical care. This factor consisted of 09 items with factor loadings ranging from 0.41-0.68 and an accounted variance of 4.20%. The eigenvalue of this factor was 2.60 and the internal consistency focus of this factor was the interpersonal skills of the RN clinical leader with patients and families. Clinical nurses were viewed as a respectful therapeutic relationship with patients and their families. Across the 9 items comprising this factor, key measuring attributes were: empathic listening, respectfulness, building rapport, tolerance and patience, and self-accountability, protecting patient rights and confidentiality. Thus, all of these attributes were skills. The statistical analysis for internal consistency was also acceptable.
Factor 5. Interdisciplinary Collaboration (IDC):
The factor 5 was labeled as interdisciplinary collaboration (IDC) that consists of 8 items having a factor loading ranging from .42 to .78 with accounted percentage of variance 4.07%, an eigenvalue of 2.43, and communalities ranged from 0.39 to 0.71. The Cronbach’s alpha coefficient of the items for this factor in terms of internal consistency reliability was 0.85. In this study, the clinical nurse leader’s IDC skills were viewed as the RN’s ability to work in partnership with coworkers and other members of the healthcare team. This factor was important for a clinical RN in Bangladesh to empower them for creating an environment in the workplace that is conducive to sharing knowledge, skills, and experiences within teams and impact the quality of patient care. The RN-CLS in this study was an appropriate construct to measure interdisciplinary collaboration leadership skills among RNs in Bangladesh. The key measuring contents of this factor were: accept individual uniqueness; focus on group interest; encourage collective opinions; articulate team responsibility; accepting criticism and mistakes, and team sharing. Hence, these attributes were influential to label this factor.
Factor 6. Skills of Communication (SC):
The factor 6 consists of 7 items with the factor loadings ranged from .45 to .77 and an eigenvalue of 3.01. The accounted percentage of variance for SC was 4.54% and a Cronbach’s alpha coefficient of 0.86 reflecting the importance of communication skills in any types of leadership and in nursing its importance is unparalleled. The role of effective communication in healthcare is always linked to the quality and effectiveness of care evaluation. The factor “skills of communication” in the RN-CLS in the present study was consistent with various leadership scales including the general leadership scale as well as earlier scales of CNL. The key measuring attributes included: provide timely truthful information, spent time to talk to patients, use clear verbal and non-verbal communication skills, understand and consider patient’s views, audience-focused skills, use of feedback, and skills in effective negotiation.
Factor 7: Professional Values in Caring (PVC):
The EFA resulted in a factor with 7 items only. Although there were relatively fewer factor items compared to other factors, factor loadings across ranged from 0.68 to 0.85. This demonstrated a very good level of reliability for each item. The total accounted variance for this factor was the lowest (4.01%) among the 9 components of the RN-CLS, with an eigenvalue of 1.94, communalities ranging from 0.62 to 0.78 and an overall internal consistency for this factor of .86 reflecting good reliability. In the present study, the PVC was described as the RN’s ability to integrate core professional values of nursing into their clinical practice in dealing with the patients, families, and members of the health team. The measures for this factor include: the principle of equity or human dignity, empathy or morale, tolerance, advocacy, and professional standards. A review of related literature did not reveal existing instruments containing this extract construct. However, the holistic nursing competency scale (HNCS) developed by Takase competency was comparable to the factor “PVC” in the present study. In the HNCS, the ethical/legal practice competency dealt with a nurse’s attitude and behavior with regards to conforming to professional codes of conduct and laws.
Factor 8: Decision Making or Problem-Solving (DMPS):
This factor constituted the largest number of item loadings (20) and the highest percentages of variance (10.25%) with an eigenvalue of 20.04. In EFA, factor loadings of items ranged from 0.47 to 0.71 with 19 items showing moderate to high level of factor loadings (0.52-0.71) and only one item with 0.47 loading. The Cronbach’s alpha was also very high (0.92) and represented an excellent level of internal consistency reliability. The communalities of item ranged from 0.32 to 0.56 and reflected a satisfactory observed variance accounted by the common factors. The DMPS skills of the CNLs in this study were described as, the RNs ability to identify and process of choosing the best option through a comparative evaluation with others in order to make reliable, valid and durable clinical solutions. The key attributes included in this measurement were the ability to define and clarify issues, gather facts and understand causes, consider and compare creative solution options, make logical decisions, take responsibility, and attend to challenging decision-making. Thus, these attributes reflected that the labeling of this factor was appropriate. Although the DMPS component of the present study was not entirely relevant to other earlier CNL scales, it was mostly consistent with a subscale of the Clinical Leadership Competency Tool (CLCT) developed by the National Health System Leadership Academy.
Factor 9: Professional Development (PD):
The last factor in the RN-CLS was factor 9 labeled “professional development” (PD) skills. This factor consisted with 7 items. Across items, factor loadings ranged from 0.56 to 0.74 with an accounted variance of 4.12% and an eigenvalue of 2.51, while the factor’s reliability for internal consistency was 0.86. The key feature reflecting the ability to demonstrate professional guardianship in making constructive changes that are pertinent to the professional advancements or growths. The key attributes of this factor included supporting individual development, ensuring workplace safety, guiding professional standards, demonstrating multidisciplinary, the ability to attract public interest, promoting professional innovation, and acting as a role model. Both observable and statistical evaluation confirmed skills in the RN-CLS were analogous to the Efficacy for Clinical Nurses Leadership (SE-Nokes). However, content-wise the SE-CNL did not entirely mirror the RN-CLS in the present study.
6.3 Psychometric Properties of the RN-CLS
The discussion in this section comprises of three main aspects to support the validity and reliability of the RN-CLS, including: (1) content validity, (2) construct validity, and (3) reliability of the Bangladesh RN-CLS.
Content validity:
The content validity is one of the most important concerns in scale development and examines the degree to which the content of a tool explicitly represents the content domain. In the present study, a panel of five experts evaluated the RN-CLS items for relevance and clarity in representing the concepts against the selected domains. The overall as well for each individual item, the CVI was well acceptable; in present study for individual items, it was ranging from .80 to 1.00 and overall, at 0.85 on 122 items. The value of 0.80 was acceptable for individual predictor.
Construct validity:
The construct validity of the RN-CLS was examined by exploratory factor analysis (EFA) and contrasted group approach. Prior to conduct the EFA, an initial item analysis was executed by using item-total correlation to evaluate the item performance to the scale. Based on Nunnally and Bernstein’s recommendation, 22 items with item-total correlations lower than 0.30 were removed before conducting EFA. Next, to establish the construct validity of the RN-CLS, factor analysis was performed using Principal Component Analysis (PCA) and Exploratory Factor Analysis (EFA) in a series of steps. EFA using data from 627 subjects, as described previously, established a more parsimonious interpretation with nine factors and 92 items. This was supported by eigenvalue values greater than 1, 52.06% of the variance, and factor loading cutoff points of 0.40 and above. Although EFA was initially performed on 102 items using varimax rotation, increasing the cumulative percentage of variance from 49.5% to 52.06%, and 10 items did not load (<0.30). Thus, these 10 items were excluded in this step and total 92 items were retained for subsequent psychometric evaluations of the items to find a more parsimonious and interpretable.
Contrasted group approach for construct validity:
After EFA, the RN-CLS was used for another form of construct validity by contrasted group methods with the involvement of 2 groups of 60 RNs in Bangladesh. The result of the high and low-performance groups was significantly varied using T-test for the score of the RN-CLS between two groups. The contrasted group approach is another method for testing the construct validity of a measure, used when two known groups are expected to exhibit extremely high and extremely low levels of the characteristics being measured by the scale. The key criteria of the subject selections were: the differences of job experience between group (high- and low-performance), which were ensured by their direct clinical supervisors. It is well said that a valid tool is able to make different the individuals who are known to be different on the constructed tool, which also confirmed by contrasted group results in this study.
Reliability of RN-CLS:
The second psychometric test was about the test of the reliability of the RN-CLS. In this study, two reliability tests were examined for the RN-CLS: the internal consistency and the test-retest for stability test of the scale. The internal consistency reliability test was performed using the Cronbach’s coefficient in three stages of the scale development. First, 30 clinical RN was involved in a pilot study to foresee the possible problems prior to administering the item pool in a large group of study subjects. At this stage, no items were deleted, but 19 items were revised due to item-total correlations of <.30, and the overall consistency of the RN-CLS was further examined using field test data from 627 subjects, assessing individual item performance via item-total correlation. At this stage, 22 items with item-total correlations below 0.30 were removed before conducting EFA. Following the removal of these items, the Cronbach’s α was 0.96 with 102 items. A final assessment of internal consistency, conducted with the remaining 92 items after EFA confirmed the factor structure of the RN-CLS, tested both the overall and subscale reliability of the 9-factor components. Results demonstrated an overall Cronbach’s α of 0.96 for the RN-CLS with 92 items, and Cronbach’s α values ranging from 0.84 to 0.92 for the 9 factor subscales, confirming good internal consistency across all subscales.
Test-Retest Reliability for Stability:
Test-retest reliability was used to assess the stability of the 92-item, 9-factor RN-CLS established by EFA. Test-retest reliability is an important method for assessing the external consistency and stability of a measure over time. In this study, to examine the stability of the RN-CLS, data were collected from a group of 30 clinical RNs on two occasions with a 10-day interval. The study results indicated a highly acceptable level of scale stability, as demonstrated by the overall correlation between the two test administrations of the RN-CLS (r = 0.92, p < 0.001). Correlations across the nine component levels were also acceptably high (r = 0.73 to 0.91). The finding indicated that among different administrations of the RN-CLS, the test result will be consistent for uses overtime in the same group of subjects. Hence, it can be concluded that the RN-CLS had an acceptable level of psychometric properties in terms of the construct validity, internal consistency reliability and test-retest reliability for stability. Moreover, this context-specific, theory-grounded, and concept-relevant instrument can be used as a valid and reliable tool to assess the clinical leadership skills of clinical Registered Nurses in Bangladesh and potentially in similar contexts in other countries.
7. Scope and Limitations of the Study
The author acknowledges that the study has its limitations in terms of the sampling strategy applied, scale length, and the variance accounted by each factor. The purposive sampling in this study, limited to clinical nurses from two medical college hospitals, may limit its generalizability. Further studies should include nurses in other clinical settings, such as Upazila and District hospitals, and specialized hospitals, to increase the generalizability of the findings. The final version of RN-CLS consisted of 92 items, could pose a burden for nurses to fully answer. The overall percentage of variance for 9 factors was only 52.06% in the present study, and 5 out of 9 factors with a percentage of variance were between 4.01% and 4.54%, whereas a variance >5% is desirable. Despite few limitations, it should be noted that this study had several strengths supporting the claim that overall, the developed RN-CLS is valid and reliable. Strengths of the study include its design, theory-grounded framework, contextual validation via focus group analysis, expert review of the item pool for content validity, the use of a Likert scale response format (a common performance assessment measure in clinical practice settings), an acceptable subject-to-item ratio (1:5.06), and Bartlett’s test of sphericity (p = 0.000), indicating that the statements comprising the scale of each variable actually measured what they were intended to measure. Moreover, all criteria for the factor analysis were tested before performing EFA resulting in sample adequacy; KMO 0.916; items at 52.06%; and the % variance by factor ranging from 4.01 to 10.25. Item rotations to 9 factors also confirmed the structure of the RN-CLS. The internal consistency overall and across the factors was more than 0.80, indicating high reliability. The additional test for construct validity, the contrasted group analysis confirmed that the RN-CLS with 92 items is a valid instrument to measure the clinical leadership skills of the RNs in Bangladesh.
8. Conclusion
The results of this study suggest that the final version of the RN-CLS (Bangladesh) possesses satisfactory psychometric properties for assessing the clinical leadership skills of registered nurses in Bangladesh. Comprehensive psychometric evaluations confirmed the RN-CLS as a valid and reliable measure. Therefore, in developing countries like Bangladesh, this instrument has potential for developing and evaluating nurses’ clinical leadership skills, empowering them as future professional leaders. Replication studies involving a larger sample of clinical nurses from diverse hospital settings are recommended to further assess the stability of the instrument across different contexts.
Conflict of Interest: None
Funding Statement: None.
Acknowledgements: This study was funded by the Directorate General of Nursing and Midwifery and Ministry of Health and Family Welfare, the Government of the Republic of Bangladesh.
References:
- Institute of Medicine (IMO) Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine. The Future of Nursing: Leading Change, Advancing Health. Washington (DC): National Academies Press (US); 2011.
- Directorate General of Nursing and Midwifery (DGNM). Personnel management data sheet. https://dgnm.gov.bd/. Published 25 Aug, 2017. Accessed 28 December, 2017.
- Andaleeb SS, Siddiqui N, Khandakar S. Patient satisfaction with health services in Bangladesh. Health Policy Plan. 2010;22(4):263-73.
- Latif MA, Nahar L, Khatun S, Akter B, Akter N, Khatun S. In-depth country assessment on nursing and midwifery in Bangladesh. World Health Organization Bangladesh and Directorate of Nursing Services, Bangladesh; 2011.
- Yeh AC, Khan MA, Harlow J, Biswas AR, Akter M, Ferdous J. Hematopoietic stem-cell transplantation in the resource-limited setting: establishing the first bone marrow transplantation unit in Bangladesh and initial outcome. Global Oncology J. 2016;128(22):2384. doi:10.1200/JGO.2016.006486.
- Lund KD, Huda SN, Berland A. Cooperative dialogue on advanced nursing education in Bangladesh. Partners in Population and Development (PPD), Dhaka. https://www.partners-popdev.org/docs/Proceedings-Cooperative%20Dialogue%202013%20ANDA.pdf Published 15 January, 2013. Accessed 12 November, 2017.
- Hadley MB, Blum LS, Mujaddid S, Parveen S, Nuremowla S, Haque M, Ulalah M. Why structural factors on hospital wards in Bangladesh. Social Science & Medicine. 2007;64(6):1166-1177. doi:10.1016/jsocscimed.2006.06.030.
- Latif A, Thiangchanya P, Nasae T. Relationship satisfaction in Bangladesh. Paper presented at: The 2nd International Conference on Humanities and Social Sciences. Faculty of Liberal Arts, Prince of Songkla University. http://tar.thailis.or.th/bitstream/123456789/937/1/006.pdf. Published 10 April, 2010. Accessed 20 October, 2017.
- Latif A, Boonyoung N, Chaowalit A. Clinical leadership skills of registered nurse: a qualitative study from the perspective of Bangladesh. J. Research in Nursing-Midwifery and Health Sciences. 2017;37(Supplement):106-115.
- Weston M, Roberts DW. The influence of quality improvement efforts on patient outcomes and nursing work: a perspective from chief nursing officers at three large health systems. Online J Issues Nursing. 2013;18(3):2. Published 2013 Sep 30.
- Porter-O’Grady T. Future of nursing special: Leadership at all levels. Nursing Management. 2011;42(5):32-37. doi:10.1097/01.NUMA.0000396347.49552.86.
- NHS Leadership Academy (NHS). Clinical leadership competency framework. NHS Institute for Innovation and Improvement, Coventry House, University of Warwick Campus, Coventry, CV4 7AL. https://www.leadershipacademy.nhs.uk. Published 2012. Accessed 10 July 2017.
- Smola BK. Refinement and validation of a tool measuring leadership characteristics of baccalaureate nursing students. In: Waltz CF, Strickland OL, Eds. Measurement Of Nursing Outcome, Volume Two: Measuring Nursing Performance: Practice, Education and Research. New York, NY: Springer Publishing.
- Gilmartin MJ, Nokes K. A self-efficacy scale for clinical nurse leaders: results of a pilot study. Nursing Economic. 2015;33(3):133-143.
- Patrick A, Laschinger HKS, Wong C, Finegan J. Developing and testing a new measure of staff nurse clinical leadership: the clinical leadership survey. Journal of Nursing Management. 2011;19(4):449-460.
- DeVellis RF. Scale Development: Theory and Applications. 4th ed. Thousand Oaks, CA: Sage Publications; 2017.
- Katz RL. Management Skills: Skills of an Effective Administrator. Harvard Business Review; September, 1974. https://hbr.org/1974/09/skills-of-an-effective-administrator. Accessed 28 June, 2016.
- American Association of Colleges of Nursing (AACN). White paper on the education and role of the clinical nurse leader. https://cpb-us-e2.wpmucdn.com/faculty.sites.uci.edu/dist/d/469/files/2016/01/16.pdf. Published 16 Jan, 2016. Accessed January, 2017.
- Waltz CF, Strickland OL, Lenz ER. Measurement In Nursing and Health Research. 4th Edition. New York, NY: Springer Publishing Company; 2010.
- Nunnally JC, Bernstein IH. The Assessment of Reliability. Psychometric Theory. 3rd ed. New York, NY: McGraw-Hill; 1994.
- Munro E. A systems approach to investigating child abuse deaths. British Journal of Social Work. 2005;35(4):531-546. ISSN 0045-3102.
- Ennis G, Happell B, Reid-Searl K. The importance of communication for clinical leaders in mental health nursing: the perspective of nurses working in mental health. Issues in Mental Health Nursing. 2013;34(11):814-819.
- Takase M, Teraoka S. Development of the holistic nursing competence scale. Nursing & Health Science. 2011;13(4):396-403.
- Zangaro GA, Soeken KL. Meta-analysis of the reliability and validity of Part B of the index of work satisfaction across studies. Journal of Nursing Measurement. 2005;13(1):7-22. doi:10.1891/jnum.2005.13.1.7.
- Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Wolters Kluwer; 2017.
- Yong AG, Pearce S. A beginner’s guide to factor analysis: focusing on exploratory factor analysis. Tutorials in Quantitative Methods for Psychology. 2013;9(2):79-94.
- Polit DF, Hungler BP. Nursing Research: Principles and Methods. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999.