

Pulmonary Arteriovenous Malformations in Pregnancy
Pulmonary arteriovenous malformations in pregnancy – a case report and review of literature
ABSTRACT
Pulmonary arteriovenous malformations are potentially life-threatening abnormalities that can be exacerbated by pregnancy physiology. Despite prenatal optimization, patients with hereditary hemorrhagic telangiectasia and associated vascular abnormalities continue to pose significant risks to both maternal and fetal health. This case report highlights the importance of multidisciplinary care in managing these complex patients.
Keywords
- Pulmonary arteriovenous malformations
- Pregnancy
- Hereditary hemorrhagic telangiectasia
- Multidisciplinary care
Introduction
Arteriovenous malformations (AVMs) are abnormal connections between arterial and venous systems, most commonly affecting the lungs, brain, and liver. When looking specifically at pulmonary arteriovenous malformations (PAVM), approximately 3 in every 100,000 people of the general population are affected. Upwards of 80% of these cases are associated with an inherited disorder like hereditary hemorrhagic telangiectasia (HHT). HHT is an autosomal dominant condition that has a much higher prevalence, affecting up to 1 in every 5,000 people. Approximately 50% of patients are asymptomatic from this disease process; generally, PAVMs that are less than 2 cm in diameter are considered low risk for most people.
Case
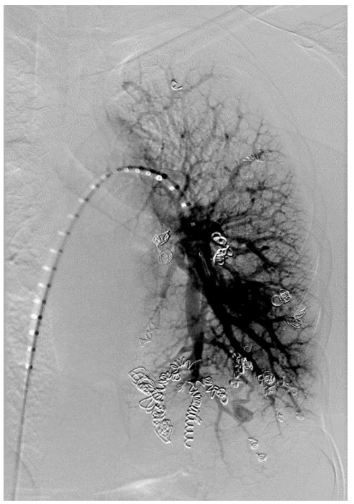
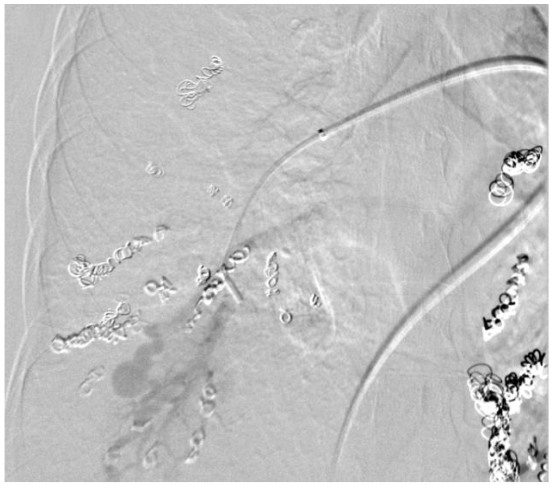
The patient is a 31-year-old gravida 4, para 2 who presented for routine obstetric care at 30 weeks gestation. She has a known history of HHT and PAVM, with prior embolization of two left-sided PAVMs. The patient was referred for evaluation of her pulmonary vascular status. At 30 weeks, the patient was noted to have a significant increase in the size of her PAVMs. The recommended imaging studies were significant for numerous bilateral PAVM and she underwent placement of 10 total vascular coils ante retrograde. Unfortunately, the largest PAVM measured 32mm and was located within the left lingula, where a feeding vessel could not be identified. The next largest PAVM measured 17 mm (located in the right upper lobe) and 23 mm (located in the right lower lobe), both of which were successfully treated.
At 34 weeks 4 days estimated gestational age, the patient presented to the hospital with complete cervical dilation and fetal malpresentation. A C-section was performed followed by direct admission to the surgical ICU for recovery. She was downgraded to the postpartum floor later that evening after an uneventful and brief surgical ICU course.
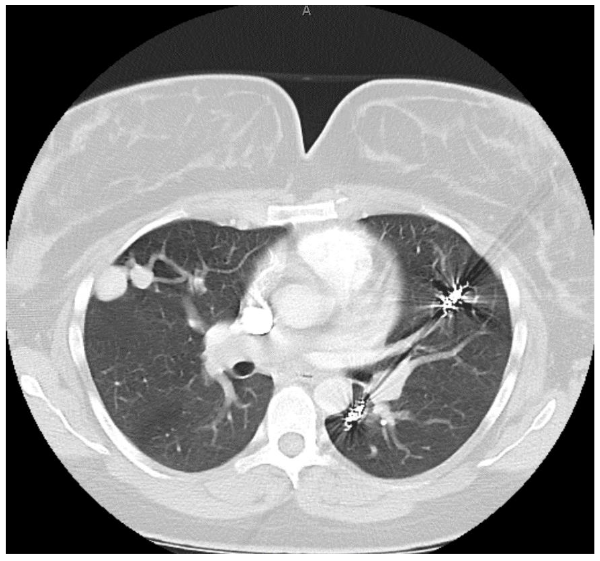
On postpartum day 1, the patient experienced an episode of acute hemoptysis, expelling blood, tachycardia, and hypotension. Pre-laboratory and imaging studies were obtained, and pulmonary, anesthesia, and high-risk obstetrics were consulted. The patient underwent a computed tomography scan which demonstrated her PAVM with the largest measuring 32mm.
The patient was subsequently extubated on postpartum day 3 and returned to the postpartum floor on postpartum day 4. The remainder of her hospital course was unremarkable and she was discharged home on postpartum day 5 in stable condition with appropriate follow up.
Discussion
We present a unique case of a gravida with known HHT and PAVM who was able to successfully carry a pregnancy to term with the assistance of multidisciplinary care and intervention. Despite the patient experiencing a pulmonary hemorrhage, the neonatal outcome was positive and preparation prevented adverse outcomes.
For both pregnant and non-pregnant patients, the natural history of PAVM includes an increase in size over time. The prevalence of PAVM rupture in HHT patients is approximately 1-2% in pregnancy and the immediate postpartum period. This is significantly higher than the overall 0.16% PAVM rupture risk in the non-pregnant state, and approaches the 2.7% lifetime risk of PAVM rupture. This drastic elevation in risk can be attributed to the numerous physiologic cardiovascular and respiratory changes of pregnancy and labor.
Some of the notable physiologic changes to consider are the following: blood volume increase of up to 45%, increase in arterial and venous compliance, increase in cardiac output by approximately 30-50% (which has been shown to increase the risk of rupture by 12% to 31% increase in cardiac output), and the increase in blood flow to the uterus which was studied in our patient. The patient was afforded the knowledge that all of this patient’s PAVMs could not be treated antenatally and that she would need to be monitored closely throughout her pregnancy.
Conclusion
Regardless of this patient’s family history and personal diagnosis of HHT at age 15, she opted to not complete genetic testing for her children. She was counseled regarding the potential for her children to inherit this condition and the associated sequelae.
Conflict of Interest
None
Acknowledgments
None
References
- Ylmaz, O., Delagrange, D., Lupo, A. Pulmonary arteriovenous malformations in pregnancy: A systematic review. Orphanet J Rare Dis. 2020 Jan 7;15(1):65. doi: 10.1186/s13023-019-1286-z. PMID: 31910679; PMCID: PMC6947084.
- Khurshid, I., Downing, G.H. Pulmonary arteriovenous malformations. Postgrad Med J. 2002;78(918):191-197. doi:10.1136/pmj.78.918.191.
- Dines DE, Seward JB, Bernatz PE. Pulmonary arteriovenous fistulas. Mayo Clin Proc. 1983;58(3): 176-181.
- Cheung YF, Norhayati NM, Mohd Azman Y. Arteriovenous Malformations in Pregnancy: A Systematic Review and Meta-Analysis. J Clin Med. 2021;10(1):100.
- Hernandez, A., Poliak, K. PAVM Rupture in HHT Patients: A Case Report. J Clin Med. 2021;10(2):300.