





Reducing Dementia Burden with Talking Mats Framework
Reducing the Burden of Dementia by Using the Talking Mats® Framework to Help People with Dementia and their Carers Communicate More Effectively
Introduction
Deterioration in communication is one of the most distressing aspects of dementia¹. All types of dementia are progressive with a gradual decline in the person’s ability to remember, understand, reason and communicate. Depending on the type and cause of dementia the communication difficulties may include reduced vocabulary, word-finding difficulty, problems with reasoning, perseveration (repetition of previously used words, phrases or behaviour), lack of coherence, losing track of topic and distractibility²˒³. As the illness progresses, the person with dementia becomes harder to reach and it is increasingly difficult to ensure that their views are included in decisions about their lives. Some of the most difficult decisions that have to be made are related to the ability of the person with dementia to carry out tasks of daily living, which require short term memory and are often the main reasons for having to consider accepting care. There is a danger that, if carers or staff have difficulty communicating with them, people with dementia may be progressively disempowered, their rights may be restricted, and choices may be imposed on them by others⁴˒⁷.
This paper aims to describe how the Talking Mats communication tool can help share and thus reduce the burden of dementia by supporting people with dementia, their carers and staff to communicate and interact more effectively. It will outline three key research projects which have been carried out to determine:
i) the effectiveness of Talking Mats for people at different stages of dementia;
ii) how Talking Mats can support decision making for people with dementia and their carers;
iii) how Talking Mats can assist staff working with people with late-stage dementia in a long stay facility
The paper will also refer to other people’s research using Talking Mats and will finally offer implications for clinical practice and policy.
Development of Talking Mats
Talking Mats was originally developed by research Speech and Language Therapists at the University of Stirling, Scotland, who went on to establish Talking Mats Ltd as a Social Enterprise
https://www.talkingmats.com/. Talking Mats Ltd is now recognised worldwide for its robust research and contribution to clinical practice and policy. A distinctive feature of Talking Mats, compared with most other Augmentative and Alternative Communication (AAC) systems, is the empirical evidence of its effectiveness with different client groups⁸˒¹².
Talking Mats uses a system of three sets of picture symbols – topics, options and visual top scale. Once the topic has been chosen, the participant is given the options one at a time and asked to think about each one, placing the relevant image below the visual scale to indicate how they feel about it.
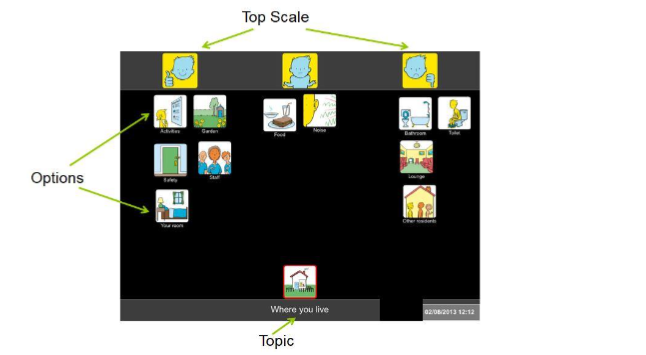
Figure 1. Example of a Talking Mat
The World Health Organization International Classification of Functioning Disability and Health (ICF)¹³ is a framework for describing and organising information on functioning and disability. It aims to provide a standard language for the description of the complete range of health-related states and experiences of health. A Talking Mats resource was developed using the ICF to create a framework containing the domains from the ICF as a starting point to help people consider issues in their lives by focusing on just one domain or topic at a time.
The Talking Mats Health and Well-being Resource –
https://www.talkingmats.com/product/health-wellbeing/ uses specifically designed communication symbols to help people organise their thoughts when discussing their health and well-being. It consists of 13 topics broken down into four areas and supports the individual to become more actively involved in making decisions about their life. It is relevant to professionals working in Health, Social Care, and Third Sector settings to support holistic and person-centred planning. It is now used by a range of practitioners and researchers with a wide spectrum of people with and without communication difficulties, including people with dementia¹⁴.
A range of further Talking Mats resources have been developed for a variety of purposes including goal setting, determining capacity and long term planning as well as training courses for individuals and organisations.
TALKING MATS RESEARCH WITH PEOPLE WITH DEMENTIA
The Talking Mats Team, led by the author, have carried out a number of research projects
https://www.talkingmats.com/research/publications/ including several aimed at reducing the burden of dementia. This paper summarises the outcomes from three specific projects.
Project 1. The effectiveness of the talking mats framework with people with dementia¹⁵.
Purpose: This project examined the effectiveness of Talking Mats for 31 people with dementia at different stages in their illness.
Methods: To meet the inclusion criteria participants had to have a confirmed diagnosis of dementia, to have sufficient vision to see picture symbols and to be physically well enough to take part. Participants who were eligible and willing to take part were assigned to one of three “stages of dementia” on the advice from staff at the relevant dementia service or care home who knew the participant well. Of the 31 people included in the research, 10 were judged to be at early-stage dementia, 11 at middle-stage dementia and 10 at late-stage dementia. The participants’ ages ranged from 54 to 90. Seven lived in their own home, 2 lived in sheltered housing (with warden support) and 22 were in residential care homes. A policy of ongoing consent was followed whereby the researcher made sure at each visit that the participants were aware of what was expected of them and were happy to proceed. Care was taken to adapt the consent and information forms to take account of cognitive and/or communication difficulties. Where the person was not able to give informed consent a family member/appointee was involved.
The participants were interviewed using Talking Mats about four well-being topics – Activities, People, Environment and Self, each containing a set of relevant options with specially designed communication symbols. A digital photo was taken of each completed ‘Mat’ to act as a record of the participant’s views. In addition to the Talking Mats conversation the participants were interviewed twice, first using their usual communication methods in an unstructured conversation and then in a structured conversation which mirrored the Talking Mats conversation, covering the same topics and options presented in the same order, but without the visual support. The visits were carried out according to a crossover design to ensure that any influences from one type of interview to another could be identified. All conversations were video-recorded and analysed which allowed a comparison to be made between the different styles of interaction.
Results: Three aspects of communication were considered: effectiveness, perseveration and on- task behaviour. The video recordings were studied by two researchers and a final-year psychology student to examine the effectiveness of communication in the three conditions. A consensus approach was used to analyse the video recordings in all three conditions¹⁶˒¹⁸.
Data were analysed using SPSS. Because data related to communication effectiveness, perseveration and on-task behaviour were ordinal and not normally distributed, results across interview conditions were compared using the Wilcoxon signed-rank test (Bonferroni-corrected).
A). Effectiveness (measured using the indicators on the Effectiveness Framework of Functional Communication¹⁹)
| TM | SC | UC | TM vs. SC | TM vs. UC | |
|---|---|---|---|---|---|
| Participant Understanding | 3.79 | 3.38 | 3.25 | z = 3.84, p < 0.001 | z = 3.61, p < 0.001 |
| Engagement | 3.88 | 3.46 | 3.50 | z = 3.72, p < 0.001 | z = 3.02, p < 0.005 |
| On Track | 3.63 | 2.50 | 2.25 | z = 4.43, p < 0.001 | z = 4.00, p < 0.001 |
| Researcher Understanding | 3.71 | 3.00 | 2.17 | z = 4.18, p < 0.001 | z = 4.28, p < 0.001 |
TM – Talking Mats conversation; SC – Structured conversation; UC – Unstructured conversation
Figure 2. Median scores for each communication indicator across all participants by interview condition and asymptotic z-scores and associated p-values (2-tailed)
Figure 2 identifies that Talking Mats conversations were more effective than both structured and unstructured conversations, in relation to all four measures of communication effectiveness, in helping people with dementia communicate their views. Significantly, the largest differences between Talking Mats and structured and unstructured conversations were evident in people with moderate and late-stage dementia. At late-stage, communication was less effective using all three methods, but Talking Mats still scored higher than structured and unstructured conversation.
B). Perseveration (repetition of previously used words, phrases or behaviour)
| TM (IQR) | SC (IQR) | USC (IQR) | TM vs. SC | TM vs. USC | |
|---|---|---|---|---|---|
| All stages | 0.63 (0.00–1.67) | 1.56 (0.13–2.67) | 1.33 (0.13–2.92) | z = 3.54, p < 0.001 | z = 3.12, p < 0.01 |
| Early | 0.00 (0.00–0.03) | 0.10 (0.00–0.22) | 0.00 (0.00–0.22) | z = 2.21, p < 0.05 | z = 0.71, n.s. |
| Moderate | 0.86 (0.21–1.42) | 2.08 (1.25–2.67) | 1.67 (1.00–2.92) | z = 2.40, p < 0.05 | z = 2.40, p < 0.05 |
| Late | 1.90 (1.25–2.35) | 2.69 (1.73–3.00) | 2.33 (1.42–3.94) | z = 1.99, p < 0.05 | z = 1.72, p < 0.05 |
TM = Talking Mats; SC = Structured conversation; UC = Unstructured conversation; IQR = Inter Quartile Range
Figure 3. Median scores for perseveration at each stage of dementia by interview condition and asymptotic z-scores and associated p-values (2-tailed)
Figure 3 shows that participants at all stages, particularly people at late stage, exhibited significantly less perseverative behaviour when being interviewed using the Talking Mats framework than structured or unstructured conversation.
C) On-task behaviour (active engagement with interviewer or symbols)
| TM (IQR) | SC (IQR) | USC (IQR) | TM vs. SC | TM vs. USC | |
|---|---|---|---|---|---|
| All stages | 0.87 (0.65–0.95) | 0.68 (0.47–0.93) | 0.66 (0.18–1.00) | z = 3.38, p < 0.01 | z = 2.40, p < 0.05 |
| Early | 0.98 (0.90–1.00) | 0.94 (0.75–0.99) | 1.00 (1.00–1.00) | z = 1.37, n.s. | z = 0.67, n.s. |
| Moderate | 0.81 (0.59–0.93) | 0.63 (0.49–0.73) | 0.66 (0.30–1.00) | z = 2.19, p < 0.05 | z = 1.07, n.s. |
| Late | 0.75 (0.39–0.86) | 0.39 (0.11–0.57) | 0.10 (0.00–0.45) | z = 2.30, p < 0.05 | z = 2.50, p < 0.05 |
TM = Talking Mats; SC = Structured conversation; UC = Unstructured conversation; IQR = Inter Quartile Range
Figure 4. Median scores for on-task behaviour at each stage of dementia by interview condition and asymptotic z-scores and associated p-values (2-tailed)
Figure 4 shows that participants at all three stages exhibited more on-task behaviours, i.e. were less distractible, when being interviewed using the Talking Mats framework than when being interviewed using structured or unstructured conversation.
Conclusion: This key research project showed that Talking Mats can help people at all stages of dementia, and in particular at middle stage, to express their views more effectively than when using their usual communication methods. Consequently, using Talking Mats may help people with dementia take an active role for longer in shaping decisions about their daily lives.
Project 2. The use of Talking Mats to support people with dementia and their carers to make decisions together²⁰.
Purpose: People with dementia who feel included in decisions about their care show higher well-being and positive adjustment to accepting care than those who feel their family make decisions for them²¹. Most carers want to involve the person with dementia in decision making and care arrangements, but many struggle because of the communication and cognitive problems associated with the illness. This project used topics from the Talking Mats Health and Well-being Resource to examine whether the Talking Mats framework could help people with dementia and their family carers feel more involved in decisions about managing their daily living.
Methods: Inclusion criteria were – the person with dementia must be aware of their diagnosis and be comfortable with the terminology involved; the person with dementia should be at the early stages of the condition; the person with dementia must be living at home and have a relative or friend (unpaid family carer) who is knowledgeable about how they are managing their daily living activities and be able to discuss this with them; both the person with dementia and the family carer should be native speakers of English and have the visual acuity to see the Talking Mats.
Eighteen people with dementia took part in the study – ten males and eight females. They had an average age of 77 years (range 60–86). Eighteen family carers also took part in the project – five males and thirteen females. They had an average age of 69 years (range 44–89). The comprehensive consent procedure carried out in the previous project was adhered to¹⁵.
Eighteen couples in Scotland and England were recruited and visited at home 3 times. The first visit was to explain the project and the second and third visits involved the collection of data. Participants were asked to discuss together how the person with dementia was managing 4 aspects of daily living – Personal Care (e.g. washing, dressing), Getting Around (e.g. walking, using stairs), Housework (e.g. cooking, making the bed) and Activities (e.g. watching TV, listening to music). Each couple was interviewed having i) a conversation using Talking Mats and ii) a conversation without Talking Mats. The order of the discussion types was counterbalanced. During both types of discussion, the focus was on how both members of the couple felt the person with dementia was managing the options within each of the four topics chosen for discussion. It was explained that the role of the researcher was to facilitate discussion by asking open-ended questions such as “How are you managing washing your hair?”, and that both members of the couple should discuss each option together and come to a decision.
In order to explore how involved each person felt, after each type of discussion both the person with dementia and the family carer were asked to complete the Involvement Measure, which is a short questionnaire comprised of six questions that measure different aspects of involvement. It was devised in collaboration with the project advisory group using questions adapted from the ‘Freedom of Choice Interview Schedule’ presented by Frossard et al. (2001) (as cited in Tyrrell et al., 2006)⁷. Both parties completed the questionnaire independently to avoid biasing answers, and assistance was offered to the participants with dementia where necessary.
Results: The following figure shows the views of both sets of participants about their feeling of involvement both with and without Talking Mats.
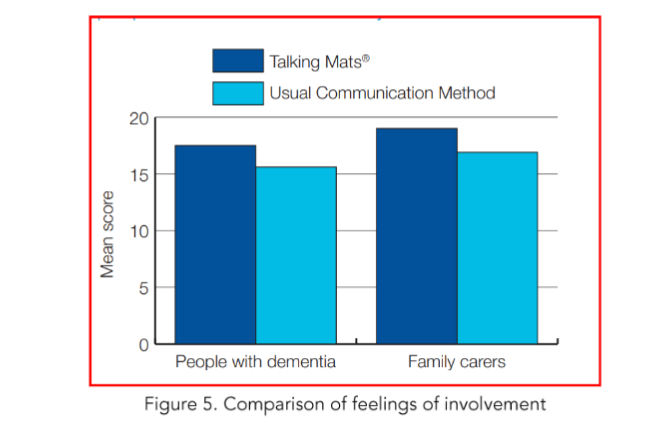
Figure 5. Comparison of feelings of involvement
Figure 5 shows that both the person with dementia and their family carer felt more involved in discussions about managing daily living when using the Talking Mats framework than with usual communication methods. The participants with dementia had a mean score of 17.5 out of 20 and the family carers had a mean score of 19 out of 20 for feelings of involvement using Talking Mats. For the Usual Communication Method discussions, the participants with dementia had a mean score of 15.6 out of 20 and the family carers had a mean score of 16.9 out of 20 for feelings of involvement.
People with dementia reported that Talking Mats clarified their thoughts and enabled them to convey their views to their carers and helped them to reach a decision about how they were managing various aspects of their lives.
The following comments illustrate the findings:
➤ I found it [Talking Mats] a big help, sometimes I get the words muddled and can’t get out what I am trying to say.
➤ It is so difficult to tell [my wife] what I think when I can’t remember the words, the pictures help me a lot.
➤ The mat shows that I am able to do much more than I thought. I didn’t realise how much she is doing in the house. (People with dementia)
A similar pattern was also evident in responses from family carers, who acknowledged the value of Talking Mats in encouraging and maintaining communication.
➤ It [Talking Mats] gives a focus to your conversation; it can be so difficult sometimes to find out what he feels,
➤ I can definitely see a place for it [Talking Mats] when communication really becomes a problem. (Family carers of people with dementia)
An unexpected finding was that, although the people with dementia and family carers both felt more involved in discussions using Talking Mats, the increased feeling of involvement was higher for the family carers. The 18 family carers who took part in the study repeatedly reported that Talking Mats made them feel ‘listened to’ by the person with dementia whom they cared for, and also felt that their relative could actually ‘see’ their point of view.
Conclusion: This project showed that people with dementia and family carers can use Talking Mats together to feel more involved in making decisions about managing daily life. Perhaps most importantly, comments from participants indicated that Talking Mats has the potential to help improve the relationship between the person with dementia and family carers, if all involved feel that their views are being acknowledged.
Project 3. Talking Mats: a model of communication training in a long stay hospital²².
Purpose: Staff working with people with advanced dementia in long stay provisions often rely on relatives to gather information about a patient’s needs and preferences, a process that can be protracted and usually depends on second-hand accounts. This in turn can lead to frustrations which can damage relationships, result in poor care and cost time. This project investigated if training nursing staff in the use of Talking Mats could improve communication with patients with dementia in a long stay facility. The purpose of the training was to give staff practical skills as well as time to reflect on their own communication, to evaluate the effectiveness of Talking Mats and to embed its use in practice.
Methods: A Talking Mats training model was delivered to 12 staff working with people mainly with late-stage dementia in a long stay hospital in Glasgow. The training was delivered over two separate days approximately four months apart and included a pre- and post-course online evaluation to examine the impact of Talking Mats training on practice. Each participant received:
• Background to Talking Mats
• Hand-outs
• Social Care symbol pack
• Pre/post on-line evaluation survey
• Hands-on practice
• Reflection templates
At the end of Day 1 staff said that they found the day helpful and were excited by the prospect of having a new tool that they could use to improve their communication with their patients. The aim was that they could start using Talking Mats with their patients immediately.
Day 2 included:
• Reflection and discussion on how participants had used Talking Mats in their work (each participant brought at least one case study to share)
• Feedback on the on-line evaluation
• Update on Talking Mats developments
Staff who attended Day 2, four months later, reported on how beneficial the sessions were in helping them gain valuable information which could be shared with all staff and relatives. Participants said that they had used Talking Mats to find out about various issues, ranging from activities (which people either liked or disliked) to finding out people’s views about their health and living arrangements.
Results: The following figures shows results from the pre- and post- online evaluations.
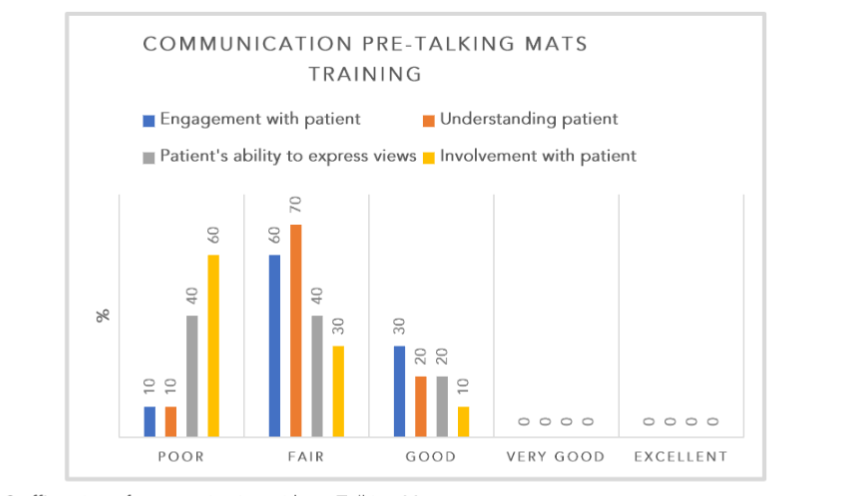
Figure 6. Staff’s rating of communication without Talking Mats
Figure 6 shows that, pre-Talking Mats training, none of the communication factors were rated as either very good or excellent by staff.
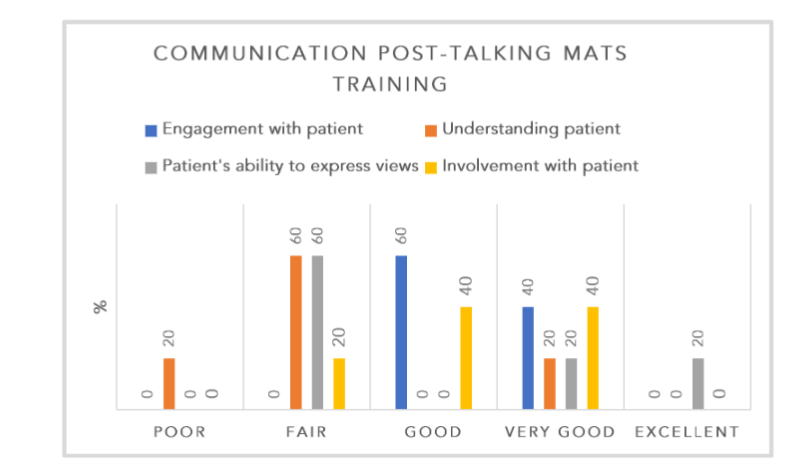
Figure 7. Staff’s rating of communication with Talking Mats
Figures 7 shows that there is a clear improvement in communication with patients post-Talking Mats training, with all four communication factors being rated as very good and patient’s ability to express views being rated as excellent by 20% of staff. This is a positive outcome bearing in mind that most of the patients in this hospital had severe communication problems due to late-stage dementia.
Here are a few of the powerful comments from staff in this project about the effects of using Talking Mats:
➤ Mrs B, who did not speak English, indicated that she really liked perfume. The nurse brought her some perfume which resulted in smiles and engagement every time that Mrs B saw that member of staff.
➤ Mrs C indicated that she was scared of locked doors because she had been in a fire as a child. Now that staff were aware of this they could reassure and comfort her.
➤ Mrs D indicated that she did not like games and puzzles, which was important to know as this was a regular activity on the ward.
➤ Mrs E was a depressed and anxious lady who rarely spoke. She really enjoyed using the Talking Mats and staff said they had never seen her laughing before.
Conclusion: The model of training using Talking Mats has been shown to be effective in terms of time and cost and successful in terms of improving the communication skills of staff working with people with dementia in a busy hospital setting.
OTHERS’ RESEARCH
Other researchers have used Talking Mats with adults with different neurological illnesses as the following publications show:
• Ferm et al found that participants with Huntington’s Disease commented that it was easier expressing feelings with Talking Mats, that it was a good method for reflecting on oral health and that it was easier thinking and understanding with Talking Mats than without²³.
• Hallberg et al found that TM can contribute to increased communicative effectiveness in group discussions for individuals with Huntington’s disease²⁴.
• Petit et al used Talking Mats to study the perspectives of adults with aphasia regarding the importance of nine life areas for rehabilitation²⁵.
• Hagelskjaer et al recommended using Talking Mats in the COPM (Canadian Occupational Performance Measure) interview with clients with cognitive and communicative impairments after a brain injury²⁶.
• Stans et al carried out a scoping review which yielded 73 publications using Talking Mats. Their study showed that Talking Mats had positive influences on technical communication effectiveness of conversations, and involvement and decision making in conversations²⁷.
Implications for policy and practice
The findings presented here have implications for the organisation, delivery, regulation and improvement of services for people with dementia.
Human Rights are the basic rights and freedoms which belong to everybody. They are based around respect for the fundamental dignity, autonomy and equality of all people, and underpin Health and Social Care Standards. In the UK, the current legislation which protects our rights is the Human Rights Act 1998²⁸.
There is a considerable amount of legislation and policy in the UK stating that people have the right to be involved in decisions and have information presented to them in an accessible and meaningful way, including the Mental Capacity Act 2005 in England and Wales²⁹ and the Scottish Government’s Charter of Patient Rights and Responsibilities (revised: June 2022)³⁰.
Guidance, from both the UK Department of Health and devolved UK governments, recommends that people with dementia have the right to be involved in decisions about care options and key life transitions. Scottish Government policy also advocates that users and carers should influence how government strategies and targets are implemented³¹.
Talking Mats can address inequalities and can support patient rights to be informed and involved in decisions about their health and social care.
Conclusion
Deteriorating communication is arguably the most difficult aspect of dementia, not only for the person with the diagnosis, but even more so for the relative, friend or staff member. It increases an already distressing burden and at times can seem insurmountable.
The research outlined in the paper has shown that the Talking Mats approach can help reduce the burden of dementia in a number of ways.
Firstly, Talking Mats can be a more effective communication tool than usual communication methods for many people living with dementia. It can improve understanding, engagement, staying on-track and it can reduce perseveration and distractibility.
Secondly, using Talking Mats with couples living with dementia can improve feelings of involvement in making decisions about managing daily life and planning for the future, not only for the person with the diagnosis but also for the partner.
Thirdly, Talking Mats can help staff who work with people with more advanced dementia to find out concerns and emotions and feel more involved with them and discover aspects of the person’s life that they may not otherwise realise.
Finally, Talking Mats can be a significant tool for those implementing policy and seeking to change practice as it is an effective way to meet the needs of people who have failing communication and ensures that they can continue to have their views heard.
Conflict of Interest:
The author, Joan Murphy, was the lead researcher in the projects described and is now the retired director of Talking Mats Ltd.
Funding Statement:
- The effectiveness of Talking Mats with people with dementia – funded by the Joseph Rowntree Foundation 2010.
- Talking Mats and Involvement in Decision Making for People with Dementia and Family Carers – funded by the Joseph Rowntree Foundation 2011.
- Training staff in long stay facilities – funded by the Greater Glasgow and Clyde “A Right to Speak Project 2015
Acknowledgements:
Thanks to all the participants in the projects and those who support them. I was very privileged to have worked with them and to have heard their stories. I am encouraged that for many, Talking Mats has helped them manage their lives better.
Thanks also to Dr Sally Boa and Margo Mackay for their helpful comments on this paper.
References
1. Dijkstra K, Bourgeois MS, Allen RS, Burgio LD. Conversational coherence: discourse analysis of older adults with and without dementia. J Neurolinguistics. 2004;17(4):263–83.
2. Bayles KA. Communication in dementia. In: H Ulatowska (Ed) The Aging Brain: Communication in the elderly. Boston: College Hill Press. 1985.
3. Kempler D. Language changes in dementia of the Alzheimer type. In R. Ubinski (Ed.), Dementia and communication. San Diego: Singular Publishing Group. 1995.
4. Cheston R, Bender M, Byatt S. Involving people who have dementia in the evaluation of services: A review. J Ment Health. 2000;9(5):471-479.
5. Kitwood T. Dementia reconsidered: The person comes first. Open University Press, Buckingham. 1997.
6. Somme D. Participation et choix des résidents dans le processus d’entrée en institution. Dossiers Solidarité et Santé. 2003;1:35-47.
7. Tyrrell J, Genin N, Myslinski M. Freedom of choice and decision-making in health and social care: Views of older patients with early-stage dementia and their carers. Dementia: Int J Soc Res. 2006;5(4):479-502.
8. Murphy J. Enabling People with Motor Neurone Disease to Discuss their Quality of Life. Communication Matters. 1999;3(2):2-6.
9. Murphy J. Enabling people with aphasia to discuss quality of life. Br J Ther Rehabil. 2000;7 (11):454-457.
10. Cameron L, Murphy J. Enabling young people with a learning disability to make choices at a time of transition. Br J Learn Disabil. 2002;30:105-112.
11. Murphy J, McCallan S, Aitken J. Helping People make decisions about PEG feeding. Bulletin of Royal College of Speech and Language Therapists. 2003;618.
12. Murphy J, Tester S, Hubbard G, Downs M, MacDonald C. Enabling frail older people with a communication difficulty to express their views: the use of Talking Mats as an interview tool. Health Soc Care Community. 2005;13(2):95-107.
13. World Health Organisation 2001, WHO-ICF: International Classification of Functioning, Disability and Health World Health Organisation, Geneva.
14. Bornman J, Murphy J. Using the ICF in goal setting: clinical application using Talking Mats. Disabil Rehabil Assist Technol. 2006;1(3):145-154.
15. Murphy J, Gray CM Cox S, van Achterberg T, Wyke S. The effectiveness of the Talking Mats framework with people with dementia. Dementia. 2010;9(4):454-472.
16. Carter M, Iacono T. Professional judgments of the intentionality of communicative acts. Augment Altern Commun. 2002;18(30):177-191).
17. Roulstone S. Consensus and variation between speech and language therapists in the assessment and selection of preschool children for intervention: A body of knowledge or idiosyncratic decisions? Int J Lang Commun Disord. 2001;36 (3):329-346.
18. Ashton RH. A Review and analysis of research on the test-retest reliability of professional judgment. JBDM. 2000;13:277-194.
19. The Effectiveness Framework of Functional Communication https://www.talkingmats.com/wp-content/uploads/2021/10/EFFC-2016.pdf
20. Murphy J, Oliver TM. The use of Talking Mats to support people with dementia and their carers to make decisions together. Health Soc Care Community. 2013;21(2):171–180.
21. Bourgeois MS (1991) Communication treatment for adults with dementia. J Speech Hear Res. 1991;34:831–44.
22. Murphy J, Alexander J, McLinton A. Talking Mats: a model of communication training. The Journal of Dementia Care. 2016;24(5):22-25
23. Ferm U, Eckerholm Wallfur P, Gelfgren E, Hartelius L. Communication between Huntington’s Disease patients, their Support persons and the dental hygienist using Talking Mats. Huntington’s Disease — Core Concepts and Current Advances. 2012. DOI: 10.5772/31484
24. Hallberg L, Mellgren E, Hartelius L, Ferm, U. Talking Mats in a discussion group for people with Huntington’s disease. Disabil Rehabil Assist Technol. 2013; 8(1): 67–76
25. Pettit LK, Tönsing, Dada S. The perspectives of adults with aphasia and their team members regarding the importance of nine life areas for rehabilitation: a pilot investigation. Top Stroke Rehabil. 2016; doi:10.1080/10749357.2016.1207148.
26. Hagelskjær V, Krohn M, Christensen PS, Reffstrup Christensen J. Canadian Occupational Performance Measure Supported by Talking Mats: An Evaluation of the Clinical Utility. Occup Ther Int. 2019.doi: 10.1155/2019/9367315.
27. Stans, S.E.A., Dalemans, R.J.P., de Witte, LP. Using Talking Mats to support conversations with communication vulnerable people: A scoping review. Technol Disabil. 2019;30(4)153-176. doi: 10.3233/tad-180219
28. Human Rights Act 1998 https://www.legislation.gov.uk/ukpga/1998/42/contents
29. Mental Capacity Act England and Wales 2005 https://www.legislation.gov.uk/ukpga/2005/9/contents
30. Charter of patient rights and responsibilities https://www.gov.scot/publications/charter-patient-rights-responsibilities-revised-june-2022/
31. New Dementia Strategy Scotland: Everyone’s Story 2023 https://www.gov.scot/publications/new-dementia-strategy-scotland-everyones-story/