

Refractive Outcomes of LuxSmart Lens After Cataract Surgery
Refractive Results of a Novel Non-Diffractive Extended Focus Lens Implanted After Cataract Surgery, First Mexican Experience
Dr. Roberto Varela Gress 1, Dr. Arturo Iván Pérez Pacheco 1, Dr. Roberto Varela González1, Dr. Inés Ortega Cervantes
- Department of Ophthalmology, Research, Anterior Segment service and Refractive Surgery, Innovia Vision Clinic, Querétaro, Mexico
Dr. Roberto Varela Gress
https://orcid.org/0009-0008-2621-0598
Dr. Arturo Iván Pérez Pacheco
https://orcid.org/0000-0002-1150-1463
Dr. Roberto Varela González
https://orcid.org/0009-0009-9363-541X
Dr. Inés Ortega Cervantes
https://orcid.org/0009-0004-1213-4310
OPEN ACCESS
PUBLISHED: 31 December 2025
CITATION: Gress, RV., Pérez Pacheco, AI., et al., 2025. Refractive Results of a Novel Non-Diffractive Extended Focus Lens Implanted After Cataract Surgery, First Mexican Experience. Medical Research Archives, [online] 13(12).
https://doi.org/10.18103/mra.v13i12.7086
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i12.7086
ISSN 2375-1924
Abstract
Introduction: Nowadays vision impairment, drastically affects the patient’s and family members quality of life. In the other hand, cataracts remain the leading cause of blindness, with approximately 15.2 million cases comprising 45% of global blindness, as cataracts arise for an aging global population, the knowledge of the capabilities and the diverse intraocular lenses (IOL) can provide to each patient, becomes essential to the current cataract surgeon.
Objective: The aim of this study was to determine the refractive results of a novel non-diffractive extended focus lens implanted after Cataract Surgery, been the first Mexican experience.
Methodology: The execution of this original article was possible through metasearch engines like Wiley Online Library, EBSCO, Cochrane, Clinicalkey, and MEDLINE PubMed, retrieve studies from January, 2024, to January, 2025. With MeSH Terms associated with “Cataract surgery AND non-diffractive extended focus lens AND LuxSmart”. The study design was a retrospective cohort study, where 48 patients were included, corresponding to 71 eyes, performed by a single surgeon and within the same clinic during all this time.
Results: The intervention improved near visual acuity, reducing both the median and variability of values. Wilcoxon test was performed. We found excellent performance in distance visual acuity and Jaeger from J6 to J2 for near vision, with the possibility of functional intermediate vision and independence from glasses for properly selected patients.
Conclusion: There is a significant reduction in the measured variables after LuxSmart IOL implantation surgery. The statistical analysis is moderate to large, suggesting a significant improvement in each patient.
Keywords
EDOF; LuxSmart; Mexican experience; Defocus curve; Cataract Surgery.
Introduction
Nowadays vision impairment, drastically affects the patient’s and family members’ quality of life. In the other hand, cataracts remain the leading cause of blindness, with approximately 15.2 million cases comprising 45% of global blindness. As cataracts arise for an aging global population, the knowledge of the capabilities that the diverse intraocular lenses (IOL) can provide to each patient, becomes essential to the current cataract surgeon.
The patient needs have changed over the years. Nowadays, longer life expectancy, the better overall health, and daily activities demand for that reason, better intermediate vision.
The use of computers, tablets, and screens, in general, has become an essential tool for most employees, which demand an intermediate vision, characteristic and fundamental element to develop in a high-standard society.
The increasingly demanding needs of users for good intermediate vision without having the disadvantages of photopic phenomena, coming from multifocal intraocular lenses, has made it mandatory to develop a new technology that satisfies these needs.
The extended depth-of-focus intraocular lenses (EDOF-IOL) have arrived to satisfy these requirements. The American National Standard Institute defines an EDOF as an IOL whose function is the correction of aphakia, with an extended range of focus, in addition to a functional visual acuity threshold, defined to provide practical distance and intermediate vision with visual acuity decreasing stepwise from the best distance focal point.
The adaptive advantage that this type of lenses create is that depth of focus in an EDOF-IOL prevents the creation of secondary images that are out of focus (compared with a mono-focal lens), which helps create a clear intermediate vision.
The EDOF-IOLS can be classified into five types, depending on the way the depth of focus is achieved; type 1 uses spheric aberrations to elong the depth-of-focus, type 2 utilizes a pinhole effect, type 3 is a multifocal IOL with low addition, Type 4 is a hybrid lens with spheric aberrations with near addition, and type 5 uses geometry (LuxSmart) to create a gradient power from the center to the periphery.
This is the first documented experience in Latin America, and particularly among the Mexican population, with the EDOF-IOL LuxSmart platform from the Bausch & Lomb commercial house.
The aim of this study was to determine the refractive results of a novel non-diffractive extended focus lens implanted after Cataract Surgery, been the first Mexican experience.
Materials and Methods
The execution of this original article was possible through metasearch engines like Wiley Online Library, EBSCO, Cochrane, Clinicalkey, and MEDLINE PubMed (National Library of Medicine, National Institutes of Health), to retrieve studies from January, 2024, to January, 2025, following “The World Medical Association (WMA) has developed the Declaration of Helsinki” as a statement of ethical principles, with MeSH Terms associated with “Cataract surgery AND non-diffractive extended focus lens AND LuxSmart”.
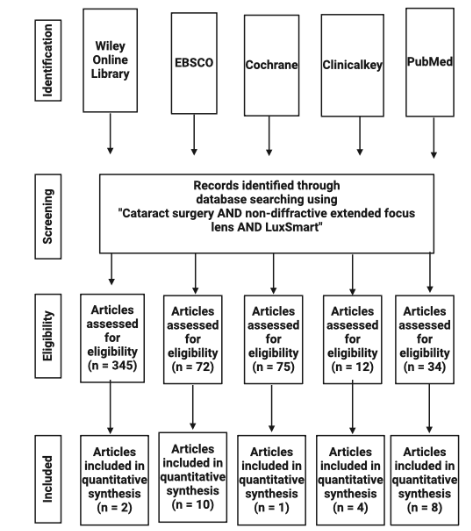
The study design was a retrospective cohort study, which was carried out with one year of follow-up, where 48 patients were included, corresponding to 71 eyes, performed by a single surgeon and within the same clinic during all this time.
All subjects had a cataract diagnosis and received a complete ophthalmic evaluation. The inclusion criteria were determined according to the international cataract classification LOCS III, with the minimum entry score being: NO2 NC2 C3 P2. Furthermore, with an uncorrected far VA (UFVA) >0.4 logMAR, the IOL calculation, was performed by using optic biometry IOLMaster 700, with the Barret Universal II formula.
The uncorrected intermediate visual acuity (UIVA) was measured at 66 cm, and the uncorrected near visual acuity (UNVA) was measured at 40 cm.
The evaluation that was carried out after 3, 6 months and one year was through the uniform and sequential measurement of a complete ophthalmological examination combined with the values of the uncorrected intermediate visual acuity, at 66 cm, and the uncorrected near visual acuity at 40 cm. Followed by its statistical unification and reporting.
Regarding the phacoemulsification surgical technique, since it was performed in a single ophthalmologic center and by the same surgeon, the result to be evaluated was repeatable and reproducible. With a phacoemulsification technique with 15-degree accessory knife incisions, the main port with a 2.4 mm incision. Each one performed on a Zeiss microscope and Centurion Vision System.
The exclusion criteria were related to: not wanting to participate in the study in principle, or refusing to sign the informed consent, in addition to this, where measurements were obtained for the placement of a toric intraocular lens or astigmatic measurements greater than 1 diopter. In mesopic conditions, where the pupil was greater than 5 mm, all pathologies other than cataracts, whether ocular external pathologies or retinal, were excluded.
Distance acuity measurements were recorded in logMAR format to allow for consistent statistical comparison. Near acuity measurements were expressed directly in spherical equivalent diopters (SE), which at the same time became Jaeger for near vision and decimal conversion.
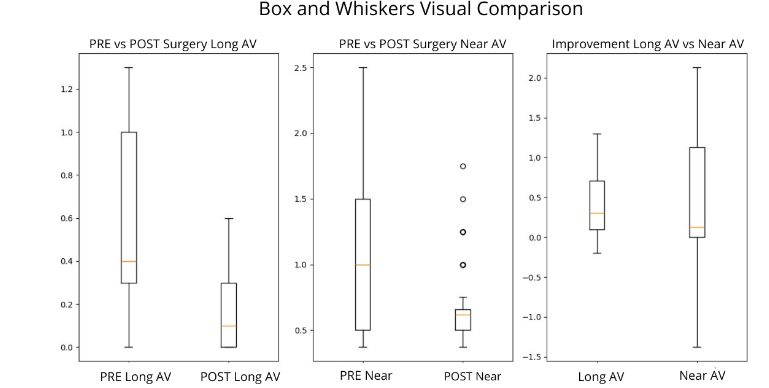
A visual comparison (Box and Whiskers) was performed, very useful for demonstrating the pre- and post-distribution and individual improvements.
Finally, the statistical analysis was carried out using the SPSS statistical package, version 21.0, where the observed relationship was analyzed in the form of graphs, tables and defocus curves, to make more evident the smooth transition that light makes at different distances; Furthermore it was used the Wilcoxon test, this test being ideal for documenting the association that exists between two sets, that do not follow a normal and non-parametric distribution.
Results
The results are based on an analysis evaluating the effectiveness of the LuxSmart intraocular lens, designed to improve visual acuity at distance and intermediate distances. Pre- and postoperative visual measurements were used to determine the implant’s impact.
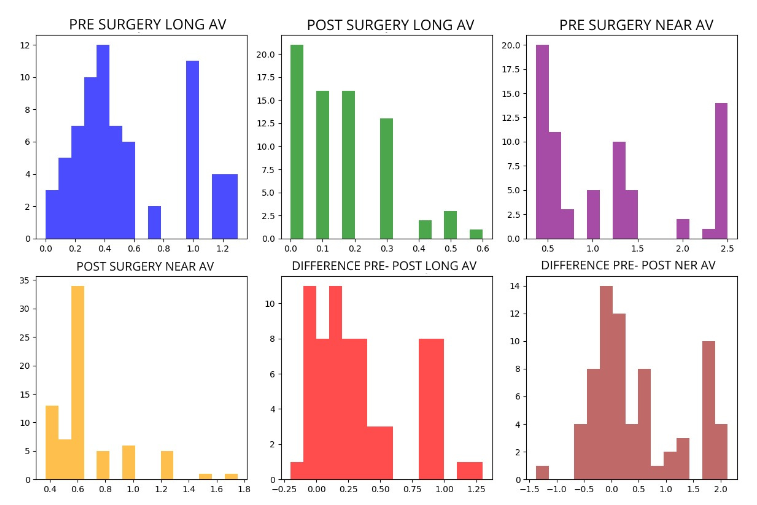
The visual acuity results obtained in pre-surgical distance vision versus post-surgical distance vision were (LogMAR): Pre-mean: 0.5437, Pre-median: 0.4000, Pre-mode: 0.4000, Post-mean: 0.1524, Post-median: 0.1000, Post-mode: 0.0000. Test used: Wilcoxon (non-normal distribution). With a statistically significant p-value of: p:0.00000000001. A statistically significant difference was found between the pre- and post-measurements. This suggests that the intraocular lens had a measurable impact on distance visual acuity.

The results for near visual acuity before and after surgery were: Pre-mean: 1.1761, Pre-median: 1.0000, Pre-mode: 0.3700, Post-mean: 0.6769, Post-median: 0.6200, Post-mode: 0.6200. Test used: Wilcoxon (non-normal distribution). p-value: 0.0000490985. A statistically significant difference can also be observed between the pre- and post-measurements. This suggests that the intraocular lens had a measurable impact on near visual acuity.
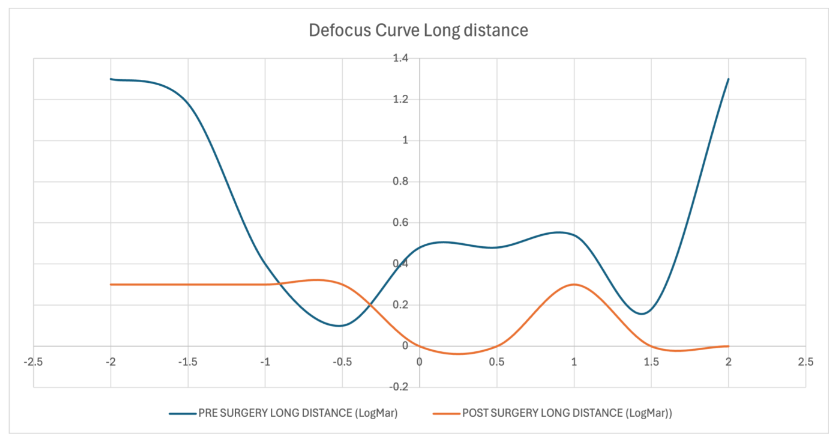
Defocus Curve results for long distance, in Pre-surgery (blue curve): Visual acuity values ranged from approximately 0.0 to 1.3 LogMAR, indicating poor visual performance with significant degradation away from the optimal focal point. The best focus occurred near -0.5 D, but visual quality remained limited. Post-surgery (orange curve): After EDOF IOL implantation, the curve flattened markedly, maintaining near 0.0 LogMAR over a wide defocus range (approximately -1.0 to +1.5 D). This indicates a significant improvement in long-distance vision and a broader effective range of focus, characteristic of EDOF optical performance.
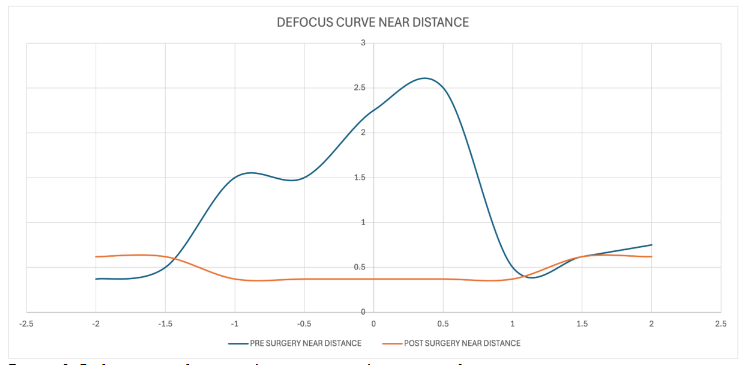
Defocus Curve results for Near-Distance vision, Pre-surgery (blue curve): The curve showed poor near visual acuity, with LogMAR values between 0.5 and 2.5, suggesting strong dependence on corrective lenses for reading and close work. Post-surgery (orange curve): The curve became remarkably stable and flat, maintaining LogMAR values between 0.2 and 0.5 across the defocus range. This demonstrates a significant functional recovery of near vision, achieved without compromising intermediate or distance performance.
Discussion
The increase in life expectancy, as well as overall health and the substantial increase in the use of electronic devices, has created increasingly demanding patients who want to eliminate their dependence on lenses.
The intermediate vision today has a more valuable connotation in the sense of the number of activities that a person performs today, since less than 50 years ago many of the activities performed were relegated to younger relatives, being today used by older adults, such is the case with the indiscriminate use of mobile applications for all kind of occasions.
The advantages offered by EDOF are substantially greater than any monofocal and even superior in visual quality to trifocals, since they reduce photopic phenomena and maintain a continuous range of vision.
One of the strong features of this type of technology is that it ensures that out-of-focus secondary images are not created, as Meggiddo and collaborators point out.
The ideal patients for EDOF IOLs are those who use high-intensity electronic devices or screens daily, those who are not ideal candidates for trifocal IOLs, and patients who are willing to wear near-field lenses.
Postoperative curves show: A flatter profile, indicating reduced sensitivity to defocus. Lower LogMAR values, reflecting enhanced visual performance. A wider range of functional focus, covering distance, intermediate, and part of the near vision zone.
These findings are consistent with published literature, in which EDOF IOLs, such as the Tecnis Symfony or AcrySof IQ Vivity, provide a continuous visual range without abrupt focal transitions, maintaining contrast sensitivity and minimizing photic phenomena.
The observed postoperative defocus curves confirm the expected optical behavior of EDOF lenses, offering extended depth of focus and improved patient satisfaction through increased spectacle independence.
Satisfaction questionnaires, such as: NEI-RQL-42 (National Eye Institute Refractive Error Quality of Life Instrument), validated worldwide and used in different series, allow us to know the result in a real world, not just academic or numbers, and it is here where aspects such as: clarity, expectations, near vision, far vision, diurnal light fluctuations, limitation of activities, glare, symptoms, dependence on glasses, concern for the patient, residual optical correction or refractive surprises, appearance and satisfaction with their surgery, were the elements to analyze, where as a result, truly incredible answers are obtained, there is practically no limitation in daily activities and near vision in 8 out of 10 is complete.
The optical quality of IOLs is becoming more precise every day and by observing the Abbe number, we can measure the dispersion of light that each IOL refracts. The number for the LuxSmart IOL is very high, at 43, where its close relative EDOF IQ Vivity from Alcon comes close with an Abbe number of 37. This element clinically supports the argument that the patient subjectively refers to, as clarity and better quality of life.
The topic of optical aberrations is becoming more and more common in this world of refractive surgery in search of visual perfection. The LuxSmart IOL works with 4th and 6th order spherical aberrations in a neutral manner, thus resulting in a more uniform visual effect when it comes to light dispersion, halos and blurriness, in addition to fine focus.
In the other hand, by having such a high Abbe number (#43), it allows many of the patients with initial pathologies of glaucoma, diabetic retinopathy, hypertensive retinopathy and others to benefit from this type of intraocular lens, since many of the patients who seek independence from glasses are usually not optimal candidates for trifocal lenses and thus reduce their quality and visual expectation in relation to glasses-free activities.
The smooth transition of the defocus curves shown in the ray propagation visualization studies for monochromatic green source and photopic conditions allows the light to be scaled gradually rather than abruptly, unlike other EDOFs.
We have increased the world case series and provided a strong national one, which actual documentation does not exist, been these the first paper in Latin America at the moment, in addition to comparing it with some of the first studies of the international results, from the launch platform. We found excellent performance in distance visual acuity and Jaeger J2 for near vision, with the possibility of functional intermediate vision and independence from glasses for properly selected patients.
Conclusion
There is a significant reduction in the measured variables after LuxSmart IOL implantation surgery. The statistical analysis is moderate to large, suggesting a significant improvement in each patient. Furthermore, the values are very low and statistically significant, indicating that the result is hardly due to odds. Therefore, it can also be concluded that allowing a young person to be functionally independent from glasses, allowing them to carry out daily activities, which are becoming more demanding every day, makes EDOF IOLs a strong candidate for the working-age population and those approaching old age.
The postoperative flattening of the curves and reduction in LogMAR values indicate that the EDOF IOL provides: Enhanced depth of focus, stable visual acuity across defocus levels, restoration of overall visual function without compromising optical quality.
Ethics
INFORMED CONSENT: It was obtained.
PEER-REVIEW: Externally peer reviewed.
AUTHORSHIP CONTRIBUTION: Dr. Roberto Varela Gress designed and interpreted the manuscript. Dr. Arturo Iván Pérez Pacheco prepared, analyzed and interpreted the manuscript. Dr. Roberto Varela González prepared, analyzed and interpreted the manuscript. Dr. Inés Ortega Cervantes prepared, analyzed and interpreted the manuscript.
CONFLICT OF INTEREST: The authors declared no conflict of interest.
FINANCIAL DISCLOSURE: The authors declared that this study received no financial support.
References
- Steinmetz JD, Bourne RRA, Briant PS, Flaxman SR, Taylor HRB, Jonas JB, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. The Lancet Global Health 2021;9:e144–60. https://doi.org/10.1016/s2214-109x(20)30489-7.
- Rua Amaro D, Bertelmann E, von Sonnleithner C. Clinical outcomes and optical performance of a new segmental refractive extended depth-of-focus intraocular lens. BMC Ophthalmol 2024;24. https://doi.org/10.1186/s12886-024-03586-4.
- Megiddo-Barnir E, Alió JL. Latest Development in Extended Depth-of-Focus Intraocular Lenses: An Update. Asia-Pacific Journal of Ophthalmology 2023;12:58–79. https://doi.org/10.1097/apo.0000000000000590.
- American National Standards Institute – ANSI Home. (s. f.-b). American National Standards Institute – ANSI. https://www.ansi.org/
- Megiddo-Barnir E, Alió JL. Latest Development in Extended Depth-of-Focus Intraocular Lenses: An Update. Asia-Pacific Journal of Ophthalmology 2023;12:58–79. https://doi.org/10.1097/apo.0000000000000590.
- Schmid R, Borkenstein AF. Analysis of higher order aberrations in recently developed wavefront-shaped IOLs. Graefes Arch Clin Exp Ophthalmol 2021;260:609–20. https://doi.org/10.1007/s00417-021-05362-2.
- Borkenstein AF, Borkenstein E-M, Luedtke H, Schmid R. Optical Bench Analysis of 2 Depth of Focus Intraocular Lenses. Biomed Hub 2021;6:77–85. https://doi.org/10.1159/000519139.
- Schmid R, Luedtke H, Borkenstein AF. Enhanced Depth-of-focus Intraocular Lenses: Latest Wavefront-shaped Optics versus Diffractive Optics. Optom Vis Sci 2022;99:335–41. https://doi.org/10.1097/opx.0000000000001894.
- Campos N, Loureiro T, Rodrigues-Barros S, Rita Carreira A, Gouveia-Moraes F, Carreira P, et al. Preliminary Clinical Outcomes of a New Enhanced Depth of Focus Intraocular Lens. OPTH 2021;Volume 15:4801–7. https://doi.org/10.2147/opth.s344379.
- Tahmaz V, Siebelmann S, Koch KR, Cursiefen C, Langenbucher A, Hoerster R. Evaluation of a Novel Non-Diffractive Extended Depth of Focus Intraocular Lens – First Results from a Prospective Study. Current Eye Research 2022;47:1149–55. https://doi.org/10.1080/02713683.2022.2074046.
- Schmid R, Fuchs C, Luedtke H, Borkenstein AF. Depth of focus of four novel extended range of vision intraocular lenses. European Journal of Ophthalmology 2022;33:257–61. https://doi.org/10.1177/11206721221125081.
- Schmid R, Luedtke H, Borkenstein AF. Effect of decentration and tilt on four novel extended range of vision intraocular lenses regarding far distance. European Journal of Ophthalmology 2022;33:933–42. https://doi.org/10.1177/11206721221128864.
- Azor JA, Vega F, Armengol J, Millan MS. Optical Assessment and Expected Visual Quality of Four Extended Range of Vision Intraocular Lenses. J Refract Surg 2022;38:688–97. https://doi.org/10.3928/1081597x-20220926-01.
- Schmid R, Borkenstein AF. Enhanced Depth of Focus Intraocular Lenses: Through Focus Evaluation of Wavefront-Shaping versus Diffractive Optics. Biomed Hub 2023;8:25–30. https://doi.org/10.1159/000529234.
- Gawęcki M, Prądzyńska N, Kiciński K, Ratajczak A, Karska-Basta I, Grzybowski A. Patient reported outcomes after implementation of an enhanced depth of focus intraocular lens with low postoperative myopia. Advances in Ophthalmology Practice and Research 2023;3:86–92. https://doi.org/10.1016/j.aopr.2023.02.003.
- Nowrouzi A, Alió del Barrio JL, D’Oria F, Kamel NR, Alió JL. Visual Performance After Unilateral Implantation of an Extended Depth-of-Focus Intraocular Lens in Patients With Unilateral Cataract. J Refract Surg 2023;39:518–23. https://doi.org/10.3928/1081597x-20230710-01.
- Kohnen T, Berdahl JP, Hong X, Bala C. The Novel Optical Design and Clinical Classification of a Wavefront-Shaping Presbyopia-Correcting Intraocular Lens. OPTH 2023;Volume 17:2449–57. https://doi.org/10.2147/opth.s400083.
- Stodulka P, Pracharova Z. Evaluation of extended depth-of-focus hydrophobic intraocular lens with an optic concept based on combination of high-order aberrations. Ophthalmol Eye Dis 2023;15. https://doi.org/10.1177/25158414231200108.
- Ruiz-Mesa R, de Luna GC, Ruiz-Santos M, Jiménez-Nieto A, Tañá-Rivero P. Clinical Outcomes of a Toric Enhanced Depth-of-Focus Intraocular Lens Based on the Combination of 4th- and 6th-Order Spherical Aberration. J Refract Surg 2024;40. https://doi.org/10.3928/1081597x-20240501-02.
- Campos N. Clinical Outcomes and Patient Satisfaction of an Enhanced Depth of Focus Intraocular Lens Targeted for Mini-Monovision. OPTH 2024;Volume 18:1607–13. https://doi.org/10.2147/opth.s459868.
- Campos N. Clinical Outcomes and Patient Satisfaction of an Enhanced Depth of Focus Intraocular Lens Targeted for Mini-Monovision. Clin Ophthalmol. 2024;18:1607-1613. Published 2024 Jun 4. https://doi.org/10.2147/OPTH.S459868.
- Mendroch D, Oberheide U, Altmeyer S. Functional Design Analysis of Two Current Extended-Depth-of-Focus Intraocular Lenses. Trans Vis Sci Tech 2024;13:33. https://doi.org/10.1167/tvst.13.8.33.
- Vega F, Garzón N, García-Montero M, Millán MS. Power profile and optical performance of two extended range-of-vision intraocular lens designs. J Cataract Refract Surg 2024;50:1065–73. https://doi.org/10.1097/j.jcrs.0000000000001528.