





Remission After Tisagenlecleucel in Down Syndrome B-ALL
Ongoing Remission Following Early B-Cell Recovery After Tisagenlecleucel in a Patient with Down Syndrome and B-ALL: A Case Report
April L. Rahrig, 1 Stayce Woodburn, 1 Jessica Harrison, 1 Magdalena Czader, 2 Audrey Hopper, 3 Jodi L. Skiles 1
- Department of Pediatrics, Indiana University School of Medicine, Indianapolis, IN, USA
- Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, Indianapolis, IN, USA
- Department of Pediatrics, Riley Hospital for Children at IU Health, Indianapolis, IN, USA
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: RAHRIG, April L. et al. Ongoing Remission Following Early B-Cell Recovery After Tisagenlecleucel in a Patient with Down Syndrome and B-ALL: A Case Report. Medical Research Archives, [S.l.], v. 12, n. 12, dec. 2024. Available at: <https://esmed.org/MRA/mra/article/view/6130>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6130
ISSN 2375-1924
Abstract
Background: Chimeric antigen receptor-T cell therapy with tisagenlecleucel has durable efficacy and manageable safety in pediatric relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL). However, evidence of its efficacy and safety in patients with Down syndrome-associated B-ALL is currently limited.
Case Report: Here, we describe a male pediatric patient with Down syndrome-associated refractory B-ALL who was infused with tisagenlecleucel twice. He was minimal residual disease-negative and had central nervous system 1 status before and after each tisagenlecleucel infusion. Adverse events of special interest following the first infusion included grade 2 cytokine release syndrome, which resolved without the need for tocilizumab, and grade 1 immune effector cell-associated neurotoxicity syndrome. Though clinically well, B-cell recovery was detected <6 months after the first tisagenlecleucel infusion. The second tisagenlecleucel infusion, followed by pembrolizumab, was administered in an unsuccessful attempt to restore B-cell aplasia. Four years after the first tisagenlecleucel infusion, the patient is disease-free with no ongoing pembrolizumab toxicity.
Conclusions: Treatment with two doses of tisagenlecleucel was relatively safe and effective in this pediatric case with Down syndrome-associated relapsed/refractory B-ALL. The results also suggest that achieving long-term B-cell aplasia may not be required for long-term remission in some cases.
Keywords
B-cell acute lymphoblastic leukemia, Down syndrome, tisagenlecleucel, CAR-T cell therapy, pediatric oncology
Introduction
Children with Down syndrome have an increased risk of developing B-cell acute lymphoblastic leukemia (B-ALL) compared with age-matched children without this disorder. Moreover, patients with Down syndrome and B-ALL have an increased risk of treatment-related toxicities from standard chemotherapy and overall worse outcomes versus those without trisomy 21. Overall, new therapies for pediatric patients with B-ALL and Down syndrome are urgently needed. Tisagenlecleucel is a cluster of differentiation (CD)19-directed chimeric antigen receptor (CAR)-T cell therapy approved for the treatment of patients up to 25 years of age with B-ALL that is refractory or in second or later relapse. CAR-T cell therapy is an individualized immunocellular therapy that genetically reprograms a patient’s immune cells to target and eliminate cancer cells. Tisagenlecleucel has demonstrated durable efficacy and a manageable safety profile in pediatric patients with relapsed/refractory (r/r) B-ALL. Although subgroup analyses from tisagenlecleucel clinical trials have demonstrated clinical benefits in patients with Down syndrome, limited evidence exists regarding its tolerability, safety, and efficacy in patients with Down syndrome and B-ALL. Herein we describe a pediatric patient with Down syndrome and refractory B-ALL who was infused with tisagenlecleucel, received a second infusion on early B-cell recovery, and has ongoing, durable remission despite very early loss of B-cell aplasia.
Case Report
A 12-year-old Caucasian male with Down syndrome was diagnosed with B-ALL. The patient had multiple cytogenetic findings (38-48,XY, t[1;15][q21;q22], der[20]t[1;20][q21;q11.2], +21c[cp8]/47, XY,+21c [12], and fluorescent in situ hybridization: [+] RUNX1) but was otherwise negative in his acute lymphoblastic leukemia panel. As first-line therapy, the patient received a three-drug induction of pegaspargase (2500 IU/m2, day 4), vincristine (1.5-2.0 mg intravenous [IV], days 1 and 8), and age-based steroid therapy (≥10 years old: prednisone 60 mg/m2/day by mouth, days 1-28) along with intrathecal cytarabine (70 mg, day 1) and methotrexate (15 mg days, 8 and 29) for newly diagnosed high-risk B-ALL. The patient’s initial response to first-line induction therapy by day 15 was 68% blasts by morphology in his bone marrow; therefore, daunorubicin (50 mg/m2) was added for the remainder of the treatment per Children’s Oncology Group Protocol AALL1131 Down syndrome arm. At the end of induction therapy (day 29), the patient had minimal residual disease (MRD) by flow cytometry (FCM), with 32% blasts in his bone marrow. He continued with consolidation therapy per AALL1131 Down syndrome arm, and mild consolidation (day 29) bone marrow revealed MRD by FCM of 14%. At the end of consolidation therapy, the patient had MRD by FCM with 3.3% blasts. Due to his primary refractory disease and the known increased toxicity and treatment-related mortality associated with stem cell transplant in patients with Down syndrome, he was referred for CAR-T cell therapy.
TREATMENT
Leukapheresis material was initially collected for CAR-T cell production at another medical facility. Leukapheresis material was collected without incident, but the patient required a temporary central venous catheter because peripheral venous access was not feasible. The patient received bridging chemotherapy with a maintenance dose of daily 6-mercaptopurine and weekly methotrexate. Disease evaluation by bone marrow MRD by FCM prior to lymphodepleting chemotherapy was 2.6%, and he had central nervous system 1 (CNS1) status (cerebrospinal fluid negative). After an appropriate washout period following bridging chemotherapy, subsequent lymphodepleting chemotherapy with fludarabine (30 mg/m2/day IV for 4 days) and cyclophosphamide (500 mg/m2/day IV for 2 days) was given. After 2 days of rest, the patient was infused with tisagenlecleucel (2.1×106 CAR-T cells/kg) on a managed access program protocol (NCT03601442), due to a slightly suboptimal CAR+ T-cell viability of 68%.
The patient experienced some adverse events (AEs) post infusion, including grade 2 cytokine release syndrome with hypoxia at day 6, which resolved with low-flow supplemental oxygen via a nasal cannula. There was no associated fever or hypotension, and he did not require tocilizumab. The patient also experienced grade 1 immune effector cell-associated neurotoxicity syndrome (ICANS) on day 2 with pupil asymmetry. His Cornell Assessment of Pediatric Delirium score was 0, and no medical intervention was required. The ICANS resolved by day 3 (duration of 1 day). Day 28 bone marrow evaluation revealed that he was MRD-negative by FCM (<0.2%). Although the patient was clinically well, early B-cell recovery was detected in peripheral blood by day 81 (CD19+ 3%; absolute CD19+ count 69 cells/µL) and confirmed on day 92 (CD19+ 5%; absolute CD19+ count 106 cells/µL); he was also bone marrow FCM MRD-negative and had continued CNS1 status.
An additional dose of tisagenlecleucel was available from the original manufacturing process. After repeat lymphodepletion with fludarabine/cyclophosphamide (same as previously described), a second tisagenlecleucel infusion (2.10×106 CAR-T cells/kg) was given in an attempt to restore B-cell aplasia. Disease status was reassessed prior to lymphodepletion; the patient remained FCM MRD negative (<0.02%) with CNS1 status and had absolute CD19+ count 148 cells/µL in his peripheral blood.
The patient received his second tisagenlecleucel infusion on day 144
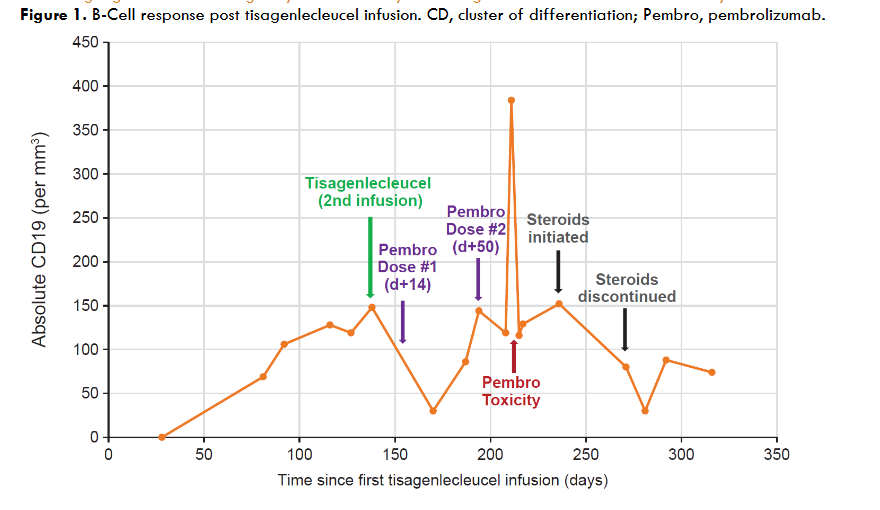
followed by pembrolizumab 14 days later (10 mg/kg, 200 mg maximum). On day +28, following the second dose of tisagenlecleucel, the patient was FCM MRD negative with CNS1 status. He achieved hematologic recovery, but peripheral blood FCM after the second dose of tisagenlecleucel (day +36) revealed B-cell aplasia was not re-established (CD19+ 2%; absolute CD19+ count 30 cells/μL). A second dose of pembrolizumab (10 mg/kg, 200 maximum) was given on day 50 to aid in achieving B-cell aplasia. Pembrolizumab induced an autoimmune response, including fever and cough. Computed tomography (CT) of the chest showed left lower lobe pneumonia (day +71). Blood cultures and bronchoalveolar lavage testing were negative for infectious etiologies, and the patient was discharged from the hospital.
The patient was readmitted on day +85 with a continued cough, low-grade fever, poor appetite, nausea, vomiting, and diarrhea. Chest CT was repeated and showed new right middle lobe pneumonia. Blood cultures and bronchoalveolar lavage were again negative, and the patient was discharged with voriconazole to treat a presumed fungal infection. The patient was readmitted to the hospital on day +101 with continued cough, low-grade fever, nausea, vomiting, diarrhea, poor appetite, significant weight loss, stomatitis, and angular cheilitis. He received IV methylprednisolone (1 mg/kg/day) for a presumed pembrolizumab-induced autoimmune response, after which he clinically improved. After 3 days of IV methylprednisolone treatment, the patient transitioned to oral prednisone (1 mg/kg/day), which was gradually tapered over 1 month.
OUTCOME AND FOLLOW-UP
At the most recent follow-up (day +1572, 52 months after the first tisagenlecleucel infusion), the patient was clinically well with no overt signs of disease relapse or ongoing pembrolizumab toxicity. The patient never achieved a second B-cell aplasia but remains alive and disease free >4 years after the first tisagenlecleucel infusion.
Discussion
CAR-T cell therapy with tisagenlecleucel was effective and tolerable in this patient with primary refractory B-ALL and Down syndrome. Despite experiencing early B-cell recovery (day 81) following the first tisagenlecleucel infusion, and not achieving restoration of B-cell aplasia after reinfusion with a second dose of tisagenlecleucel, the patient remains in remission and is without relapse. Previous case reports in pediatric patients with B-ALL have shown that pembrolizumab administered with CAR-T cell reinfusion can increase and/or prolong CAR-T cell persistence. Furthermore, it has been shown that the addition of pembrolizumab was well tolerated, with no increase in the incidence or severity of key AEs associated with CAR-T cell infusion and no additional autoimmune toxicity. In contrast, our patient case showed the addition of pembrolizumab following the second tisagenlecleucel infusion did not help restore B-cell aplasia, but instead resulted in pembrolizumab-related toxicity.
Maintenance of B-cell aplasia post CAR-T cell infusion is generally considered a surrogate marker for CAR-T cell persistence. Indeed, clinical outcomes are typically better in patients who have CAR-T cell persistence ≥6 months, and early B-cell recovery may indicate CAR-T cell therapy failure, warranting consideration of stem-cell transplantation. However, this case supports a “watch and wait” approach, which is especially noteworthy for patients with Down syndrome who may not tolerate stem-cell transplantation and may develop toxicities related to additional immunotherapy attempting to re-establish B-cell aplasia. Further, as more data become available, MRD assessed by next-generation sequencing may be a more sensitive and reliable predictor of a patient’s risk of relapse, independent of B-cell recovery.
Conclusions
This case contributes to the growing body of evidence that CAR-T cell therapy is safe and effective for patients with Down syndrome and r/r B-ALL and may help avoid chemotherapy-related toxicities. In general, the clinical community has presumed that prolonged CAR-T cell persistence and B-cell aplasia were needed for long-term remission, and that B-cell recovery was associated with a risk of CD19+ relapses. The results here seem to indicate that achieving long-term B-cell aplasia may not be required for long-term remission in some patients. Additional long-term follow-up of patients from clinical trials and the real-world setting will be needed to better understand whether patients may be considered cured without persistent B-cell aplasia.
Conflicts of Interest
All authors report no competing interests.
Funding
This work was supported by Novartis Pharmaceuticals Corporation.
Acknowledgements
Medical writing support was provided by Healthcare Consultancy Group, and funded by Novartis Pharmaceuticals Corporation.
References
- Whitlock JA. Down syndrome and acute lymphoblastic leukaemia. Br J Haematol. 2006;135(5):595-602. doi:https://doi.org/10.1111/j.1365-2141.2006.06337.x
- KYMRIAH (tisagenlecleucel) prescribing information. Novartis Pharmaceutical Corporation.
- Maude SL, Laetsch TW, Buechner J, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med. 2018;378(5):439-448. doi:10.1056/NEJMoa1709866
- Maude SL, Frey N, Shaw PA, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med. Oct 16 2014;371(16):1507-17. doi:10.1056/NEJMoa1407222
- Laetsch TW, Maude SL, Balduzzi A, et al. Tisagenlecleucel in pediatric and young adult patients with Down syndrome-associated relapsed/refractory acute lymphoblastic leukemia. Leukemia. Jun 2022;36(6):1508-1515. doi:10.1038/s41375-022-01550-z
- Laetsch TW, Maude SL, Grupp SA, et al. CTL019 therapy appears safe and effective in pediatric patients with Down syndrome with relapsed/refractory (r/r) acute lymphoblastic leukemia. Blood. 2017;130:1280. doi:https://doi.org/10.1182/blood.V130.Suppl_1.1280
- US National Library of Medicine. A phase III randomized trial for newly diagnosed high risk B-lymphoblastic leukemia (B-ALL) including a stratum evaluating dasatinib (NSC#732517) in patients with Ph-like tyrosine kinase inhibitor (TKI) sensitive mutations. ClinicalTrials.gov Identifier: NCT02883049. Posted August 30, 2016. Updated September 21, 2022. Accessed September 26, 2022. https://clinicaltrials.gov/ct2/show/NCT02883049
- Rubin CM, Mick R, Johnson FL. Bone marrow transplantation for the treatment of haematological disorders in Down’s syndrome: toxicity and outcome. Bone Marrow Transplant. 1996;18(3):533-540.
- US National Library of Medicine. Managed Access Program (MAP) Cohort Treatment Plan CCTL019B2003I to Provide Access for Patients With Out of Specification Leukapheresis Product and/or Out of Specification Manufactured Tisagenlecleucel (CTL019; Kymriah®). ClinicalTrials.gov Identifier: NCT03601442. Posted July 26, 2018. Updated September 6, 2022. Accessed September 26, 2022. https://clinicaltrials.gov/ct2/show/NCT03601442
- Maude SL, Hucks GE, Seif AE, et al. The effect of pembrolizumab in combination with CD19-targeted chimeric antigen receptor (CAR) T cells in relapsed acute lymphoblastic leukemia (ALL). J Clin Oncol. 2017;35(15 suppl):Abstract 103. doi:10.1200/JCO.2017.35.15_suppl.103
- Li AM, Hucks GE, Dinofia AM, et al. Checkpoint inhibitors augment CD19-directed chimeric antigen receptor (CAR) T cell therapy in relapsed B-cell acute lymphoblastic leukemia. Blood. 2018;132(suppl 1):Abstract 556. doi:10.1182/blood-2018-99-112572
- Pulsipher MA, Han X, Maude SL, et al. Next-Generation Sequencing of Minimal Residual Disease for Predicting Relapse after Tisagenlecleucel in Children and Young Adults with Acute Lymphoblastic Leukemia. Blood Cancer Discov. Jan 2022;3(1):66-81. doi:10.1158/2643-3230.BCD-21-0095
- Gardner RA, Finney O, Annesley C, et al. Intent-to-treat leukemia remission by CD19 CAR T cells of defined formulation and dose in children and young adults. Blood. 2017;129(25):3322-3331. doi:10.1182/blood-2017-02-769208