





Renal Outcomes of SGLT2 Inhibitors in Type 2 Diabetes
Renal outcomes with sodium-glucose cotransporters 2 inhibitors in Patients with Type 2 Diabetes Mellitus with Chronic Kidney Disease Stages 3-4
Issa Afif Kawalit¹*, Abdulraqeeb Hasan Al-Omari², Zeina H. Kalaji³, Asad Ibrahim Al-Tirawi¹, Muhand Salama Eltwal¹, Abbas Y. El-Khatib⁴
- Department of Nephrology, Royal Bahrain Hospital, Bahrain.
- Department of Nephrology, Salmaniya Medical Complex, Bahrain.
- Department of Medicine, University of Jordan, Amman, Jordan.
- Department of Nephrology, Arab Renal Care Group, Amman, Jordan.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Kawalit, IA., Al-Omari, AH., et al., 2024. Renal outcomes with sodium-glucose cotransporters 2 inhibitors in Patients with Type 2 Diabetes Mellitus with Chronic Kidney Disease Stages 3b-4. Medical Research Archives, [online] 12(11).
https://doi.org/10.18103/mra.v12i11.5877
COPYRIGHT: © 2024 European Society of Medicine. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5877
ISSN 2375-1924
ABSTRACT
Introduction: Randomized clinical trials have shown that sodium-glucose cotransporter 2 (SGLT2) inhibitors significantly reduce renal events in patients with type 2 diabetes mellitus (T2DM) at high risk for cardiovascular disease. However, these trials included only a small number of patients with moderate-to-severe chronic kidney disease (CKD), leaving the renoprotective effects of SGLT2 inhibitors in T2DM patients with impaired renal function unclear.
Methods: This retrospective study evaluated the effects of SGLT2 inhibitors on kidney function in T2DM patients with CKD stages 3b-4 with estimated glomerular filtration rate (eGFR) 15–45 mL/min/1.73 m². Conducted by a single nephrology group across two medical centers, the study included 175 T2DM patients who initiated SGLT2 inhibitor therapy and continued treatment for at least one year. The primary outcomes were changes in eGFR and urinary protein excretion over a one-year period.
Results: After one year of SGLT2 inhibitor therapy, the median eGFR showed no significant change from baseline. However, the annual decline in eGFR significantly improved, and urinary protein excretion decreased significantly. Despite these positive renal outcomes, HbA1c reduction was not significant.
Conclusion: This study demonstrated that SGLT2 inhibitors offer renoprotective benefits in T2DM patients with moderate-to-severe CKD by improving the annual decline in eGFR and reducing urinary protein excretion. Further prospective clinical studies are required to assess the long-term effects of SGLT2 inhibitors on glycemic control and renal function in this patient population.
Keywords: Sodium-glucose co-transporter 2 inhibitors, Type 2 diabetes mellitus, Renoprotection.
Introduction
The incidence of type 2 diabetes mellitus (T2DM) is increasing worldwide¹. Diabetic nephropathy / diabetic kidney disease is a serious complication of T2DM, leading to end-stage kidney disease (ESKD) requiring hemodialysis, making it a critical issue in clinical practice and public health¹,². Clinical assessment of renal damage through measurements of urine protein-to-creatinine ratio (UPCR) and estimated glomerular filtration rate (eGFR) is recommended to promote active interventions with renoprotective effects³. The annual decline in eGFR is a clinically useful biomarker reflecting dynamic and time-dependent changes in renal function⁴. Patients with higher 1-year rates of decline in eGFR (over 7.5%) are considered “rapid eGFR decliners” and are associated with poor renal prognosis in T2DM patients. There is a need for practical strategies to preserve and improve renal function, especially in patients with CKD stages 3b-4 who are at high risk of developing ESKD despite being asymptomatic⁵,⁶,⁷. In patients with severely impaired kidney function, treatment options for hyperglycemia are limited due to drug metabolic pathways, side effects, and risk of hypoglycemia⁸,⁹. Glucose-lowering therapies with renoprotective effects are considered to have additional clinically important effects and advantages for comprehensive T2DM management¹⁰,¹¹.
Recent studies have shown that SGLT2 inhibitors, like dapagliflozin and empagliflozin, provide protective effects against glomerular damage and tubulointerstitial injury in patients with insufficiently controlled T2DM¹². Large randomized clinical trials in patients at high risk for atherosclerotic cardiovascular disease (ASCVD) revealed that SGLT2 inhibition has protective effects on renal events¹³,¹⁴,¹⁵. However, these trials included only small numbers of patients with moderate-to-severe CKD. The glucose-lowering effect of SGLT2 inhibitors is diminished in advanced CKD patients, leading to recommendation against their use in T2DM patients with impaired renal function (eGFR < 45 mL/min/1.73 m²). Therefore, the renoprotective effects of SGLT2 inhibitors remain unclear in T2DM patients with severely impaired renal function¹⁶,¹⁷,¹⁸.
This study aimed to retrospectively examine the potential beneficial effects of SGLT2 inhibitor therapy on renal function in T2DM patients with CKD stages 3b-4.
Materials and Methods
STUDY POPULATION AND STUDY PROTOCOL
Based on clinical data from the electronic medical records of two renal centers, we retrospectively identified patients with type 2 diabetes mellitus (T2DM) who began treatment with SGLT2 inhibitors between January 2020 and May 2024. We selected patients with moderate-to-severe renal impairment (CKD stages 3b-4) at the initiation of SGLT2 inhibitor therapy and who continued treatment for at least one year. Exclusion criteria included type 1 diabetes mellitus, unstable cardiovascular disease, active inflammation, autoimmune disorders, infectious diseases, severe liver disease, dementia, and cancer. Additionally, newly diagnosed diabetic patients not undergoing treatment and those with ketosis were excluded.
We investigated annual changes in eGFR before and after SGLT2 inhibitor therapy. The primary outcome was the quantitative assessment of annual changes in eGFR. We analyzed eGFR one year before and one year after SGLT2 inhibitor therapy. This was a retrospective, observational, single-arm, 2-center study. The study was conducted following the Review Board approval. No patient informed consent needed since no patient identity was revealed.
ASSESSMENTS AND MEASUREMENT OF CLINICAL PARAMETERS
We collected clinical information on medical treatments, complications, and history, as well as data on body weight, height, blood pressure, and pulse rate. Blood and urine analyses were conducted in the hospital laboratory to measure hemoglobin, hematocrit, blood glucose, HbA1c, creatinine, blood urea nitrogen (BUN), uric acid (UA), urinary protein, and urinary creatinine. Urinary protein excretion was assessed. eGFR was before SGLT2 inhibitor therapy (one year and six months before), at the initiation of therapy, and after therapy (six months and one year after). We calculated the annual changes in eGFR.
STATISTICAL ANALYSES
The primary endpoint was the treatment-induced annual changes in eGFR. We aimed to analyze significant improvements in annual changes in eGFR before and after SGLT2 inhibitor therapy. A power analysis indicated that enrolling over 22 patients was required to detect a mean difference in annual changes in eGFR of -3.0 mL/min/1.73 m² per year before SGLT2 inhibitor therapy and -1.0 mL/min/1.73 m² per year after therapy, with a power of 80% and a two-sided alpha value of 0.05.
Normally distributed continuous variables are presented as means (standard deviation), while skewed distribution variables are presented as medians (interquartile range). Paired Student’s t-test or Wilcoxon’s test was used to analyze the effects of SGLT2 inhibitor therapy on body weight, BMI, blood pressure, and pulse rate. Spearman’s rank correlation coefficient was used to analyze correlations between changes in annual eGFR decline and changes in HbA1c. A P-value < 0.05 was considered statistically significant.
Results
BASELINE CLINICAL PARAMETERS OF PATIENTS
A total of 1,188 stable T2DM patients newly treated with SGLT2 inhibitors were initially identified, of whom 190 (16.0%) had moderate-to-severe CKD (stages 3b-4) at initiation. Fifteen patients were excluded for not continuing treatment for over one year, resulting in a final cohort of 175 patients. Mean age was 64.8 years, 71.4% were male, mean duration of T2DM was 18 years, and mean BMI was 28.2 kg/m². Hypertension and dyslipidemia were present in 95.2% of patients, and 23.8% had a history of cerebrovascular/cardiovascular diseases. Median HbA1c was 7.6%, with an average of three antidiabetic drugs used, including insulin. Metformin and insulin were used by 50.0% and 71.4% of patients, respectively. The most frequently used SGLT2 inhibitor was dapagliflozin (33.0%). Median eGFR was 40.4 mL/min/1.73 m². Data on urinary protein excretion was available for 150 patients. No patient was treated with erythropoietin (table 1).
Table 1: Baseline Characteristics of the study Population
Characteristics | Value
Total Number of patients | 175
Age (years) | 64.8 ± 10.2
Male (%) | 71.4
Duration of T2DM (years) | 18.0 ± 5.0
BMI (kg/m²) | 28.2 ± 4.5
Hypertension (%) | 95.2
Dyslipidemia (%) | 95.2
History of CVD (%) | 23.8
HbA1c (%) | 7.6 (6.9–8.3)
Median eGFR (mL/min/1.73 m²) | 40.4 (35.0–45.0)
UPCR (g/g creatinine) | 0.36 (0.23–0.54)
ACEi or ARBs (%) | 30%
CHANGES IN CLINICAL PARAMETERS AFTER ONE YEAR OF SGLT2 INHIBITOR THERAPY
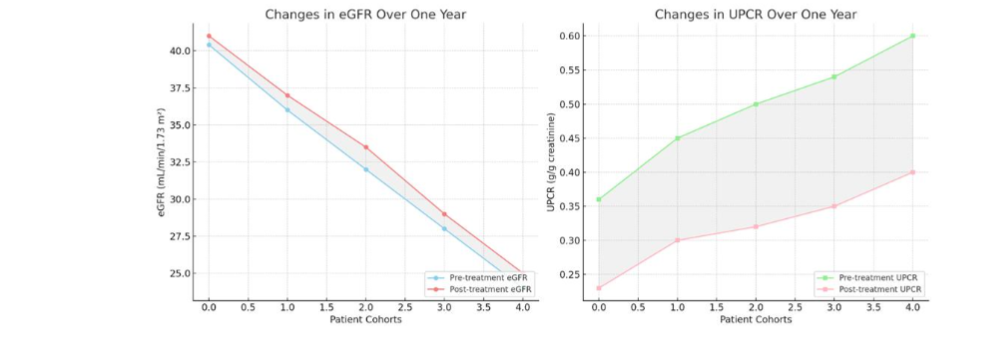
After one year of SGLT2 inhibitor therapy, median HbA1c levels decreased from 7.6% to 7.5% (not significant), while body weight significantly decreased by 3.5 kg (P < 0.01) and blood pressure significantly decreased by 10 mmHg systolic and 5 mmHg diastolic (P < 0.01). Hemoglobin levels significantly increased by 0.5 g/dL (P < 0.01) (table 2). The median eGFR after one year was 41.0 mL/min/1.73 m², showing no significant change from baseline. However, the annual decline in eGFR significantly improved (median eGFR decline: pre-treatment -3.8 vs. post-treatment 0.1 mL/min/1.73 m² per year, P < 0.01). Urinary protein excretion also significantly decreased (urinary protein-to-creatinine ratio: pre-treatment 0.36 vs. post-treatment 0.23 g/g creatinine, n = 150, P < 0.01) (Figure 1).
Table 2: Changes in Clinical Parameters After One Year of SGLT2 Inhibitor Therapy
Parameter | Pre-treatment | Post-treatment | P-value
HbA1c (%) | 7.6 (6.9–8.3) | 7.5 (6.8–8.2) | 0.22
Body weight (kg) | 70.1 ± 15.5 | 66.6 ± 14.7 | <0.01
Systolic BP (mmHg) | 140 ± 20 | 130 ± 18 | <0.01
Diastolic BP (mmHg) | 80 ± 10 | 75 ± 10 | <0.01
Hemoglobin (g/dL) | 12.5 ± 1.5 | 13.0 ± 1.6 | <0.01
Median eGFR (mL/min/1.73 m²) | 40.4 (35.0–45.0) | 41.0 (36.0–46.0) | 0.35
Median annual eGFR decline | -3.8 (-5.0 to -2.6) | 0.1 (-1.5 to 1.2) | <0.01
UPCR (g/g creatinine) | 0.36 (0.23–0.54) | 0.23 (0.15–0.35) | <0.01
Figure 1: Changes in eGFR Over One Year & Changes in UPCR Over One Year
Discussion
The study demonstrates that add-on treatment with SGLT2 inhibitors for over a year improves the annual decline in eGFR and reduces urinary protein excretion in T2DM patients with moderate-to-severe CKD. This finding is significant as it may provide a therapeutic advantage in managing patients with advanced CKD and help delay the progression to end-stage kidney disease (ESKD). SGLT2 inhibitors are known to offer protective effects against glomerular damage and tubulointerstitial injury. However, their full renoprotective mechanisms in patients with severely impaired renal function are not entirely understood. Recent research has suggested several potential mechanisms by which SGLT2 inhibitors exert their renoprotective effects. These include the reduction of podocyte damage and improvement in mitochondrial function, as well as decreased oxidative stress and inflammation within the kidney.
kidney. Clinicians should consider that when advanced renal dysfunction is identified, it may still be possible to intervene effectively and potentially delay the need for renal replacement therapy.
Limitations of the Study
This study has several limitations inherent to its retrospective design, which affects the control over variables and data completeness. Since this is an observational study, it lacks a controlled comparative group with randomization, and thus is susceptible to selection bias. The absence of a direct, randomized control group without SGLT2 inhibitor therapy limits the ability to attribute observed changes in renal function solely to SGLT2 inhibitors, as other unmeasured factors could have influenced outcomes. Instead, we compared each patient’s renal function during the one year of SGLT2 inhibitor therapy with their own historical data from the previous year without these inhibitors. While this within-patient comparison offers some control over individual variability, it cannot fully account for confounding factors that may have changed over time. Additionally, the relatively short follow-up period of one year restricts the study’s capacity to assess the long-term renal effects of SGLT2 inhibitors in advanced CKD patients.
These limitations suggest that while the study provides preliminary insights, prospective, randomized controlled trials with extended follow-up periods are essential to confirm the renoprotective benefits of SGLT2 inhibitors in T2DM patients with advanced CKD and to establish clearer causal relationships.
Conclusions
This study showed that SGLT2 inhibitors provided significant renoprotective effects, improving the annual decline in eGFR and reducing urinary protein excretion in T2DM patients with CKD stages 3b-4. However, HbA1c reduction was not significant. Further prospective clinical trials are needed to fully elucidate the effects of SGLT2 inhibitors on glycemic control and renal function in T2DM patients with moderate-to-severe renal impairment.
Conflict of Interest:
The authors declare that there are no conflicts of interest related to this study.
Funding Statement:
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements:
The authors would like to thank the staff at the Royal Bahrain Hospital and the Arab Renal Care Group for their assistance in data collection and patient care.
References
1. Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW, Malanda B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018; 138:271–281.
2. Duru OK, Middleton T, Tewari MK, Norris K. The landscape of diabetic kidney disease in the United States. Curr Diab Rep. 2018;18(3):14.
3. Doshi SM, Friedman AN. Diagnosis and Management of Type 2 Diabetic Kidney Disease. Clin J Am Soc Nephrol. 2017;12(8):1366–1373.
4. Levey AS, Inker LA, Matsushita K, Greene T, Willis K, Lewis E, de Zeeuw D, et al. GFR decline as an end point for clinical trials in CKD: a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am J Kidney Dis. 2014;64(6):821–835.
5. Nojima J, Meguro S, Ohkawa N, Furukoshi M, Kawai T, Itoh H. One-year eGFR decline rate is a good predictor of prognosis of renal failure in patients with type 2 diabetes. Proc Jpn Acad Ser B Phys Biol Sci. 2017;93(9):746–754.
6. Tsimihodimos V, Filippatos TD, Filippas-Ntekouan S, Elisaf M. Renoprotective effects of SGLT2 inhibitors: beyond glucose reabsorption inhibition. Curr Vasc Pharmacol. 2017;15(2):96–102.
7. Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet. 2017;389(10075) :1238–1252.
8. Moen MF, Zhan M, Hsu VD, Walker LD, Einhorn LM, Seliger SL, Fink JC. Frequency of hypoglycemia and its significance in chronic kidney disease. Clin J Am Soc Nephrol. 2009;4(6):1121–1127.
9. Davies M, Chatterjee S, Khunti K. The treatment of type 2 diabetes in the presence of renal impairment: what we should know about newer therapies. Clin Pharmacol. 2016; 8:61–81.
10. Neumiller JJ, Alicic RZ, Tuttle KR. Therapeutic considerations for antihyperglycemic agents in diabetic kidney disease. J Am Soc Nephrol. 2017; 28(8):2263–2274.
11. Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032–2045.
12. Sugiyama S, Jinnouchi H, Kurinami N, Hieshima K, Yoshida A, Jinnouchi K, Tanaka M, et al. Impact of dapagliflozin therapy on renal protection and kidney morphology in patients with uncontrolled type 2 diabetes mellitus. J Clin Med Res. 2018;10(6):466–477.
13. Cherney DZI, Zinman B, Inzucchi SE, Koitka-Weber A, Mattheus M, von Eynatten M, Wanner C. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: an exploratory analysis from the EMPA-REG OUTCOME randomized, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017;5(8):610–621.
14. Perkovic V, de Zeeuw D, Mahaffey KW, Fulcher G, Erondu N, Shaw W, Barrett TD, et al. Canagliflozin and renal outcomes in type 2 diabetes: results from the CANVAS Program randomized clinical trials. Lancet Diabetes Endocrinol. 2018;6(9):691–704.
15. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357.
16. Kelly MS, Lewis J, Huntsberry AM, Dea L, Portillo I. Efficacy, and renal outcomes of SGLT2 inhibitors in patients with type 2 diabetes and chronic kidney disease. Postgrad Med. 2019; 131(1):31–42.
17. Dekkers CCJ, Wheeler DC, Sjostrom CD, Stefansson BV, Cain V, Heerspink HJL. Effects of the sodium-glucose co-transporter 2 inhibitor dapagliflozin in patients with type 2 diabetes and stages 3b-4 chronic kidney disease. Nephrol Dial Transplant. 2018;33(11):2005–2011.
18. Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, Rossing P, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669–2701.
19. Heerspink HJ, Kropelin TF, Hoekman J, de Zeeuw D, Reducing Albuminuria as Surrogate Endpoint C. Drug-induced reduction in albuminuria is associated with subsequent renoprotection: a meta-analysis. J Am Soc Nephrol. 2015;26(8):2055–2064.
20. Cassis P, Locatelli M, Cerullo D, Corna D, Buelli S, Zanchi C, Villa S, et al. SGLT2 inhibitor dapagliflozin limits podocyte damage in proteinuric nondiabetic nephropathy. JCI Insight. 2018;3(15)
21. Takagi S, Li J, Takagaki Y, Kitada M, Nitta K, Takasu T, Kanasaki K, et al. Ipragliflozin improves mitochondrial abnormalities in renal tubules induced by a high-fat diet. J Diabetes Investig. 2018;9(5):1025–1032.
22. Tanaka S, Sugiura Y, Saito H, Sugahara M, Higashijima Y, Yamaguchi J, Inagi R, et al. Sodium-glucose cotransporter 2 inhibition normalizes glucose metabolism and suppresses oxidative stress in the kidneys of diabetic mice. Kidney Int. 2018;94(5):912–925.
Most read articles by the same author(s)
- Issa A. Kawalit, Zeina H. Kalaji, Ahmed M. Ibrahim, Erfai M. Emtair, Laith F. Al-Rabadi, Multidisciplinary Approach to a Complicated Renal Angiomyolipoma: A Case Report Review , Medical Research Archives: Vol 12 No 10 (2024): October Issue, Issue 10, VOl.12