






Resurgence of Pediatric Tuberculosis in Post-COVID India
Resurgence of Pediatric Tuberculosis in India
Dr C. K. Sasidharan1, Dr Swetha B Ram2,Dr Athira Sasidharan3, Dr Hareesh Thanikachalam4,
- Senior Consultant & Former Professor (Calicut Medical College) of Paediatrics; Baby Memorial Hospital, Calicut
- Resident, Dept of Paediatrics; Baby Memorial Hospital, Calicut
- Associate professor; Dept of pathology; KMCT Medical College, Calicut
- Resident, Dept of Paediatrics; Baby Memorial Hospital, Calicut
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Sasidharan, Ck., et al., 2025. Resurgence of Pediatric Tuberculosis in India. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i9.7001
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.7001
ISSN 2375-1924
ABSTRACT
The post-COVID-19 era has witnessed a resurgence of pediatric tuberculosis (TB) in India, highlighting its continued status as an important public health challenge. This review aims to analyse this resurgence, associated diagnostic challenges, recent advancements in detection methods, and strategies for effective management and prevention. It places particular emphasis on clinical presentations, the role of molecular diagnostics, and national programs towards TB elimination.
Aims and Scope: The objective of this article is to analyze the burden, clinical spectrum, diagnostic tools, and treatment protocols of pediatric tuberculosis in India. The scope includes an overview of epidemiology, methodology of diagnostic strategies, and national policies with emphasis on future directions for tuberculosis elimination.
Keywords
Pediatric Tuberculosis, India, Public Health, COVID-19, Diagnostic Challenges, Treatment Protocols
Introduction
Tuberculosis poses a significant public health concern in India and globally. Following the COVID-19 pandemic, pediatric tuberculosis cases have shown a resurgence, largely due to disrupted healthcare services and delayed diagnosis. TB is among the top 10 causes of death among children worldwide.
In India, approximately 3.42 lakh children (0-14 years of age) are estimated to get TB every year, and account for about 6% of total TB cases reported to National Tuberculosis Elimination Program (NTEP) in 2021. In 2020, approximately one lakh children with TB (0 to 14 years of age) were reported to the NTEP, while an additional 1.4 lakh children were reported to the NTEP in the age group of 15-18 years. The heterogeneous clinical presentation, disparities in access to healthcare, and prevailing social stigma complicate disease recognition and management.
Study Methodology
This review is based on an analysis of published literature, reports from the National Tuberculosis Elimination Program (NTEP), and recent clinical case discussions. Data were drawn from peer-reviewed journals, government health reports, and international tuberculosis surveillance studies to consolidate current knowledge on pediatric TB in India.
Discussion
The global burden of pediatric tuberculosis remains underestimated due to surveillance limitations in low- and middle-income countries. In India, nearly one-third of global childhood tuberculosis cases are reported, with children under five years at greatest risk. The most common presentation is pulmonary TB, though extrapulmonary forms are relatively more frequent in children compared with adults.
Advanced diagnostic modalities such as cartridge-based nucleic acid amplification tests (CB-NAAT), line probe assays, and interferon-gamma release assays have improved early case detection, but accessibility and cost remain barriers. Management protocols now emphasize universal drug sensitivity testing and fixed drug combination regimens, along with prophylaxis for childhood contacts. Government initiatives, including Nikshay, community awareness programs, and the Dare2eraD TB genome sequencing project, represent significant progress toward elimination, though challenges remain.
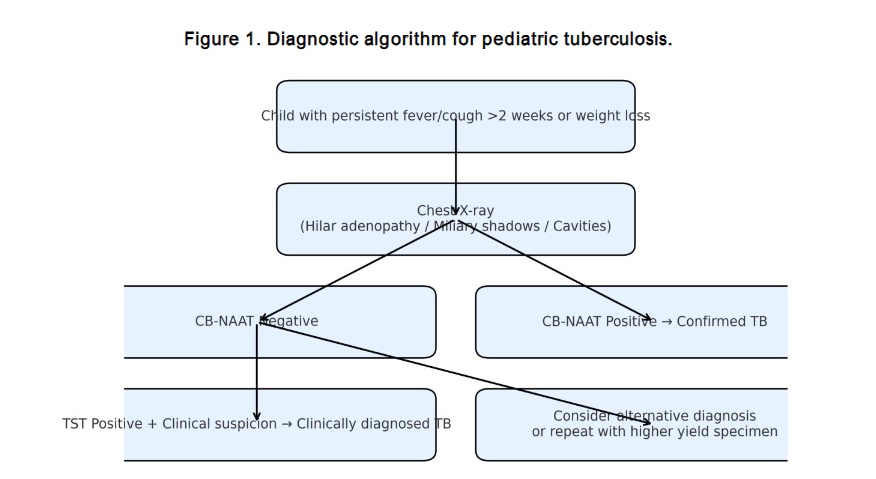
DIAGNOSTIC STRATEGIES IN PEDIATRIC TUBERCULOSIS
NTEP has approved rapid molecular diagnostic methods, including cartridge-based nucleic acid amplification tests (CB-NAAT/Xpert-RIF/Truenat) and line probe assays (LPA), which demonstrate superior sensitivity to conventional smear testing. Sputum induction using hypertonic saline and gastric aspirate verification can enhance diagnostic yield; however, in over 700 gastric aspirates collected in our centre over the years, the sputum yield was as low as 20%. Extrapulmonary tuberculosis necessitates additional modalities such as tuberculin skin tests (TST), interferon-gamma release assays, and biopsies, with culture studies considered the gold standard. For suspected tuberculous meningitis, cerebrospinal fluid culture and advanced molecular assays, including Xpert Ultra and loop-mediated isothermal amplification, offer increased sensitivity.
MANAGEMENT OF PEDIATRIC TUBERCULOSIS
Current guidelines recommend daily fixed drug combination (FDC) regimens for pediatric tuberculosis. Drug-resistant cases must be referred to nodal centers. In children co-infected with HIV, tuberculosis treatment is prioritized, with antiretroviral therapy initiated within two weeks to two months. The prevalence of multi drug resistance is 2.8% among newly diagnosed cases and 14% among previously treated cases. Multiple studies have shown inter patient variation to drug responses attributed probably to nutritional status and genetic polymorphisms.
Implementation of therapeutic drug monitoring of second line drugs may throw light on the ceiling dose required for clinical response in non responders. Further research into pharmacogenomics, pharmacokinetics and pharmacodynamics is the need of the hour. The following summarizes the treatment regimens:
Conclusion
Pediatric tuberculosis continues to be a critical challenge for India’s public health system. Despite advancements in diagnostics and treatment, gaps remain in surveillance, early recognition, and contact management. Sustained national efforts, technological innovation, and community engagement are essential to achieve the ambitious goal of tuberculosis elimination in the near future.
Case Study
A six-month-old infant presented with fever, failure to thrive, and progressive abdominal distension. On examination, the child was severely malnourished with massive hepatomegaly and palpable splenic tip. BCG scar reactivation was observed. Maternal history revealed pulmonary tuberculosis with pleural effusion, acquired from a caregiver with active infection. The mother was diagnosed while pregnant and was on treatment. The infant was born with normal birth weight (3 kg) and remained asymptomatic until 5 months of age. Investigations revealed normal chest X-ray and granulomatous hepatitis on liver biopsy. Antitubercular therapy was initiated, leading to clinical improvement. Given the hepatomegaly with normal lungs, the probability of transplacental transmission was considered.
References
- Finlayson H, Lishman J, Palmer M. What’s new in childhood tuberculosis. Curr Opin Pediatr. 2023;35(2):166-175. doi:10.1097/MOP.0000000000001226
- Swaminathan S, Rekha B. Pediatric tuberculosis: Global overview and challenges. Clin Infect Dis. 2010;50(Suppl 3):S184-S194. doi:10.1086/651490
- Nelson LJ, Wells CD. Global epidemiology of childhood tuberculosis. Int J Tuberc Lung Dis. 2004;8(5):636-647.
- Central TB Division. Nikshay Data from National Tuberculosis Elimination Program. Ministry of Health and Family Welfare, Government of India; 2021.
- Central TB Division. India TB Report 2020. National Tuberculosis Elimination Program Annual Report. New Delhi: Ministry of Health and Family Welfare, Government of India; 2020.
- Sharma SK, Mohan A, Kohli M. Extrapulmonary tuberculosis. Expert Rev Respir Med. 2021;15(7):931-948.
- Lin F. Tuberculous meningitis diagnosis and treatment: classic approaches and high-throughput pathways. Front Immunol. 2024;15:1543009.
- Hemanth Kumar AK, Kumar A, Kannan T, et al. Pharmaco-kinetics of second-line Ministry of Health and Family Welfare, New Delhi, India, Central TB Division. Pediatric Tuberculosis Management Guideline 2022. RNTCP 2022. Available at: https://theindia.mobfw.gov.in/pediatric-th/ Accessed Apr 5, 2025
- Seddon JA, Hesseling AC, Marais BJ, et al. Paediatric use of second-line anti-tuberculosis agents: A review. Tuberculosis. 2012:92:9-17.
- Thee S, Seifart HL, Rosenkranz B, et al. Pharmacokinetics of ethionamide in children. Antimicrob Agents Chemother 2011:55-4594-600.
- Chien S, Wells TG, Blumer J., et al. Levofloxacin pharmacokinetics in children. J Clin Pharmacol. 2005,45:153-60.