

Root Canal Treatment Before Extraction in Orthodontics
The method of Root Canal Treatment before Extraction Technique in an Orthodontic Extraction Case
Cristian Romanec D.D.S. PhD 1, Cristina Gena Dascalu Assoc. Prof. PhD 2, Michiko Aonuma D.D.S. 3, George Anka D.D.S., M.S. 4- Orthodontic Department, University of Medicine and Pharmacy Grigore T. Popa, Iași, 700115, Romania; [email protected]
- Medical Informatics and Biostatistics Dept. Faculty of Dental Medicine, University of Medicine and Pharmacy “Gr.T.Popa” University no. 16 Iași, Romania
- Smile Forever Medical Corporation, Tokyo, 206-0011, Japan; [email protected]
- Smile Forever Medical Corporation, Tokyo, 206-0011, Japan; [email protected]
*Questions related to this paper are kindly directed to the e-mail below:
[email protected]
OPEN ACCESS
PUBLISHED: 31 December 2025
CITATION: Romance, C., Dascălu, C.G., et al., 2025. The method of Root Canal Treatment before Extraction Technique in an Orthodontic Extraction Case. Medical Research Archives, [online] 13(12).
https://doi.org/10.18103/mra.v13i12.7016
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i12.7016
ISSN 2375-1924
Abstract
Extraction to resolve malocclusion is common in orthodontics, and it may take several months or years to close the extraction gap. Leaving an extraction site unclosed leads to alveolar bone resorption, narrowing the bone width and making it difficult to close the gap later. The study pertains to orthodontic cases with a substantial arch-length discrepancy that require extractions; Class II Division 1 and 2 cases typically favor first bicuspid extractions. The root canal treatment of the indicated extraction bicuspids facilitates interproximal reduction of the mesial and distal area, which will provide spaces. This method will offer the option to reduce the Arch Length Discrepancy and to delay extraction timing at the initial alignment stage. Therefore, given time for the orthodontist to align the crowded area and correct the Curve of Spee. The treatment could begin with bracket placement before reaching a stage where it is ready to extract the space, which was provided without extraction at the beginning. This study aims to determine the time needed to close an extraction site in typical cases involving the removal of the first bicuspid tooth. The goal is to determine whether delaying extraction can shorten the time to close the extraction gap, thereby reducing overall orthodontic treatment time. The timing results can then be compared with previous research outcomes to identify any differences or advantages of delaying extraction using the Root Canal First Before Extraction method. Keywords: regional acceleration phenomena (RAP), bone density, delayed tooth extraction timing, root canal treatment (RCT), time to close the extraction site in orthodontics, arch length discrepancy (ALD), interproximal reduction (IPR), tooth movement.Introduction:
Moving the tooth to a narrow alveolar ridge and thin cortical bone increases the risk of relapse during post-retention. The alveolar ridge experiences a sharp reduction within three to six months after extraction, resulting in nearly a 50% decrease in width within the first year. The alveolar width decreases as early as 3 months post-extraction. Closing the extraction gap takes longer after alveolar resorption occurs. It is essential to close the extraction gap promptly and reliably to prevent relapses. Initiating a study to close the extraction gap immediately after extraction is advisable. Utilizing the regional acceleratory phenomenon (RAP) and leveraging the decreased bone density during orthodontic treatment can also be advantageous. A systematic review and meta-analysis have been conducted on the study of delayed early versus delayed space closure in relation to the rate of orthodontic tooth movement. Early traction, initiated a week after tooth extraction, has a minimal effect on the rate of tooth movement compared to delayed traction. A comparison study of healed extraction and fresh extraction showed that the fresh site closed more rapidly than the counterpart. However, the use of delayed extraction after aligning the first stage of orthodontic treatment, followed by root canal treatment, has not been studied. The initial aim of the study is to prevent the later problem of closure of the extraction site when the case involves alveolar resorption, as this can affect closure.The preparation
Before orthodontic treatment, root canal procedures were performed on all bicuspids that needed to be extracted. Extraction is performed after aligning the maxillary and mandibular arches, followed by placement of closing arch wires to close the extraction gap. The closing process commenced immediately after the teeth were extracted. The study investigates the time required to close extraction sites in standard clinical situations. Crowding cases with an arch length discrepancy of 9mm or more but without severe skeletal problems are considered routine clinical cases. The method assumes that RAP and reduced bone density will reliably close the extraction site within a specified time frame. The need for bicuspid extraction varies among clinicians. An arch length discrepancy of 5–9 mm may be necessary, and it is usually required for an ALD of more than 10 mm. The selected cases had ALD exceeding 9 mm. We must assess the cephalometric data and potential for arch expansion before deciding on extraction. The first bicuspid, often extracted, has two roots. Front teeth retract distally to improve facial structure after treatment.Criteria
All cases were treated by the same orthodontist using the same technique. The potential mixed dentition line ages were 15, with both males and females included. Bone maturity and density could affect the rate of tooth movement, so it is essential to select the exact condition of bone density. Cases had ALD greater than 9 mm. The fixed appliances bracket uses the self-ligating straight wire method. The closing loop applied was the Multiple Loops Edgewise (MEAW) technique.

Method
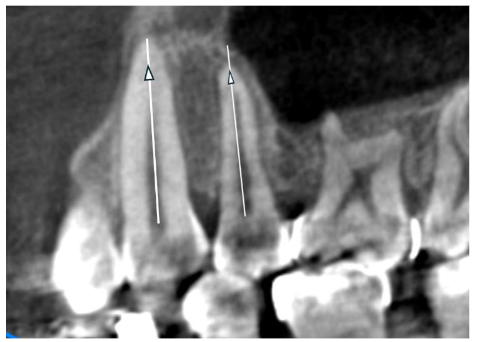
Cone Beam Computed Tomography (CBCT) was employed multiple times for different reasons during this study. First, a CBCT scan was taken during the initial record-taking stage, before extraction and after the extraction space was closed. The initial CBCT taken before treatment serves two purposes: it measures the lengths of the canines and second bicuspids and assesses the density of the alveolar bone. A second CBCT was taken before extraction to assess bone density and the space between the crowns of adjacent teeth and the roots. The third CBCT was performed to confirm the spacing and root positions. The third CBCT is also essential for the upcoming treatment stages, where the entire maxillary dentition will be retracted more distally; in this case, Temporary Anchorage Devices (TADs) will be used to plan their placement. The TADs will not be discussed in this manuscript. In this study, the extraction spaces were closed using posterior teeth anchorage to close the gap through en-masse retraction. The study included 21 patients and 60 extraction sites. One patient had only the upper first bicuspid extracted, while two others had a single lower bicuspid extracted due to a missing incisor. The length of the canine and second bicuspid roots can be measured using data from the initial CBCT.
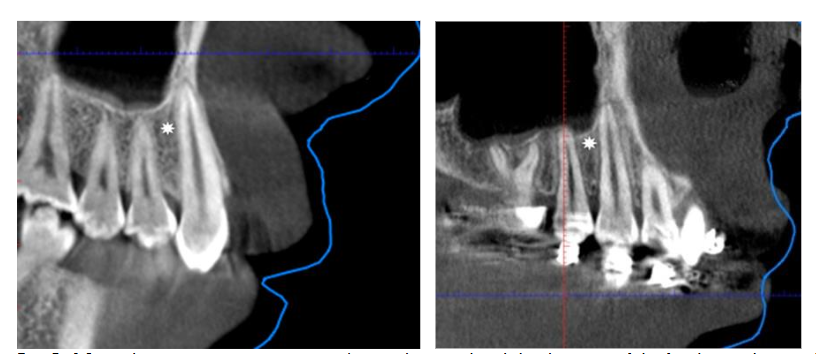




 X-ray of the post-extraction site.
X-ray of the post-extraction site.
THE PROCESS OF CLOSING THE EXTRACTION SPACE:
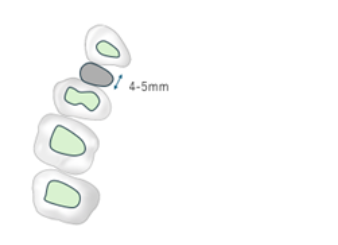
In cases of crowding, the canine is retracted to create space for aligning and correcting the inclination of the anterior teeth. The 2nd bicuspid will move mesially as a reciprocal force when the canine is retracted. The area in front of the 2nd bicuspid is the fresh wound of the extracted 1st bicuspid, and there was space. Alveolar bone density tends to decrease during orthodontic movement, as previously mentioned. Therefore, the primary retention in closing the extraction space in this situation is the distal movement of the canine; the density of these areas was measured and calculated. The density value was obtained using Planmeca Romexis software from the Planmeca Pro-Max x-ray machine. The space on the extraction side is the diameter of the root of the 1st bicuspid plus residual alveolar bone in the cervical area. The diameter of the cervix of the 1st bicuspid ranges from 4 to 5 mm at most. The result of accumulating and processing the data is the statistical mean and the standard deviation.Material and methods:
Sample of 21 patients from Japan. The study involved patients who received orthodontic treatment with premolar tooth extractions and were monitored during post-extraction space closure. The inclusion criteria included individuals aged 12 to 50 years, without systemic diseases that could affect bone healing or dental mobility, with complete medical records including pre- and post-extraction CBCT radiographs, and comprehensive data on root length, bone density, and the duration of space closure. Patients with dental or bone trauma in the evaluated area, severe periodontal disease, active infections in the extraction site, or incomplete or interrupted orthodontic treatment were excluded from the study.STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS software version 26.0. The Pearson correlation test was used to assess relationships between bone density, root length, and space closure time. Independent samples t-tests compared group means, while linear regression analysis identified predictive factors in the space-closure process. The ANOVA test was employed to evaluate differences among groups with varying orthodontic characteristics. A p-value below 0.05 was regarded as statistically significant.RESULTS.
The average age of the participants is 23.71 years, ranging from 12 to 49 years (SD = 9.65). Regarding gender, most participants are female (76.2%), with 23.8% being male. In terms of malocclusion classification, Class I is the most common, accounting for 66.7% of cases, while Class II is found in 33.3% of participants.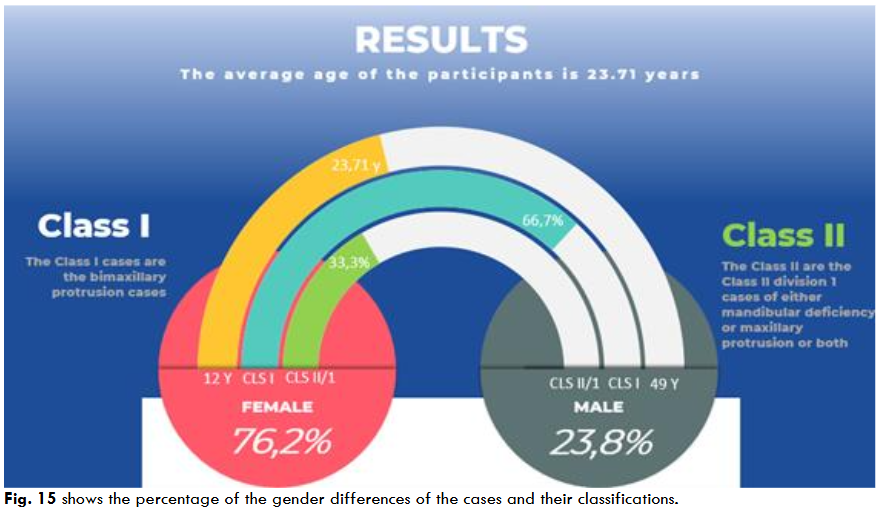 Fig. 15 shows the percentage of the gender differences of the cases and their classifications.
Class I cases involve bimaxillary protrusion.
Class II includes Class II division I cases, which may involve either mandibular deficiency, maxillary protrusion, or both. A few cases of Class II division 2 (two instances) are also included.
Fig. 15 shows the percentage of the gender differences of the cases and their classifications.
Class I cases involve bimaxillary protrusion.
Class II includes Class II division I cases, which may involve either mandibular deficiency, maxillary protrusion, or both. A few cases of Class II division 2 (two instances) are also included.
Time to close the extraction spaces
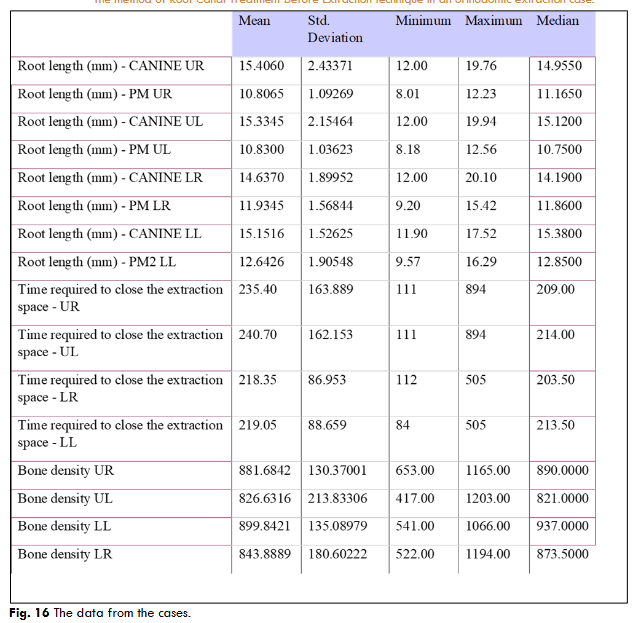
The time needed for post-extraction space closure is shorter in the mandible (about 218 days) than in the maxilla (235–240 days), and bone density is greater in the lower regions, especially in LL (899.8 HU), compared to the upper areas (UR – 881.7 HU, UL – 826.6 HU). These differences may affect orthodontic treatment planning, suggesting faster mandibular space closure, which is associated with higher bone density.Discussion
The time needed to close the maxilla extraction gap was longer than that for the mandible. This might initially raise a question; however, when we consider most of the Class I and Class II cases in the maxilla, despite having lower bone density than the mandible, we see larger and longer teeth. We need to retract more distance compared to the mandible, where we often require less anchorage loss to move the posterior teeth mesially after the anterior teeth have been uprighted to their normal angulation and inclination according to the treatment plan. The maxillary teeth then moved to consolidate the mandible teeth. Correlation analysis was performed between bone density and variables related to root length and post-extraction space closure time. The factors that lead to quicker tooth movement during a delayed extraction:- The Regional Acceleratory Phenomenon (RAP) is a biological response in which tissue repair and remodeling speed up after a harmful stimulus, such as surgical injury or mechanical force. In orthodontics, RAP is intentionally triggered to shorten treatment time by increasing bone turnover and improving tooth movement efficiency.
- During active orthodontic movement, the tooth may temporarily become more mobile due to bone remodeling and changes in the Periodontal Ligament (PDL). This increased mobility is normal, and the rise in ICPT (“type I collagen cross-linked C-terminal telopeptide”) is directly linked to the rate of tooth movement, which is also related to the rate of bone remodeling. Therefore, a proportional force, such as the MEAW, can help maintain a consistent rate.
- The amount of space that needs to be closed has been significantly reduced in this Root Canal Before Extraction method, which could be a significant benefit.
Result.
The study revealed moderate variation in the root length of canines and premolars across dental regions (maxillary and mandibular), with significant differences between the upper and lower areas. The time required for post-extraction space closure is shorter in the mandible than in the maxilla, which is linked to higher bone density in the lower regions, especially in the LL area. The correlation analysis revealed that bone density is not a significant predictor of root length across the studied regions. However, bone density in the lower areas (LR and LL) shows a moderate, inversely proportional, and statistically significant correlation with the time required for post-extraction space closure, suggesting that higher bone density may help reduce the duration of the closure process. These results highlight the importance of assessing bone density when planning orthodontic treatment, especially in cases involving post-extraction mandibular spaces, thereby providing a foundation for optimizing treatment strategies based on local bone properties. Comparison with the previous closing time of the extraction site study showed significant differences. However, the treatment technique and environmental factors could also have affected the results, making it difficult to judge. The extraction site in this maxillary study was closed without the use of mini screws or Temporary Anchorage Devices. Instead, en-masse retraction was employed, based on the anchorage of the posterior teeth, to close the extraction site. The duration of this process was 235 days. The previous study by Schneider et al found that the retraction process took approximately 12.1 months, or 363 days. This shows that the Root Canal Before Extraction method helps close extraction spaces after removing the bicuspids. The key question for many orthodontists is: “Orthodontic treatment time: can it be shortened?” This research might help cut down the overall length of orthodontic treatment.Limitations of the study
- Small sample size (n=21)
- Population selection (excluding patients from Japan):
- Results may reflect ethnic, genetic, or lifestyle factors that might not be relevant to other populations.
- Measurements performed by a single examiner:
- Although consistency is maintained, the absence of inter-examiner assessment may add subjectivity and reduce external validity.
- Single imaging tool (CBCT only):
- Partial monitoring of clinical variables:
- Other variables relevant to space closure, such as oral hygiene quality, patient cooperation, or applied orthodontic forces, were not quantified.
- Globally assessed closure time per region:
- No distinction was made between space closure caused by distal/mesial tooth movement and that caused by biological regeneration mechanisms.
- Unequal distribution across genders and malocclusion types.
- The bone density (Hounsfield Unit) may vary during tooth movement treatment; therefore, it is not a static measurement.
Conclusion
This approach focuses solely on the timing of extraction in orthodontic treatments and is not linked to any specific philosophies or techniques used by orthodontic specialists. Therefore, it can be applied to any fixed appliance, whether labial or lingual brackets, and is also suitable for aligner orthodontics. Delaying extraction allows time to prepare the arches, both upper and lower, before beginning to close the extraction gap. Extraction can occur once all preparations, such as aligning, leveling the Curve of Spee, and setting up for gap closure, are complete. After extraction, the process can proceed. Take advantage of the RAP once the tooth is removed. Before extraction, brackets are placed on the tooth to eliminate the bowing effect. Applying Root Canal Treatment before extraction (RBE) is feasible across all areas of orthodontics.Conflicts of Interest Statement
Non-financial conflict of any kind.Funding Statement
This is a purely individual research project without any funding from any bodies or companies.Acknowledgements
Thank you to Dr. Cristina Gena Dascalu, Associate, for providing the statistical analysis for this paper.Bibliography:
- Rothe, L. E., Bollen, A., Little, R. M., Herring, S. W., Chaison, J. B., Chen, C. S. K., & Hollender, L. G. (2006). Trabecular and Cortical Bone as Risk Factors for Orthodontic Relapse. American Journal of Orthodontics and Dentofacial Orthopedics, 130(4), 476-484. https://doi.org/10.1016/j.ajodo.2005.03.023
- Tan, W. L., T. Wong, T. L., M. Wong, M. C., & Lang, N. P. A systematic review of post-extraction alveolar hard and soft tissue dimensional changes in humans. Clinical Oral Implants Research, 23, 1-21. https://doi.org/10.1111/j.1600-0501.2011.02375.x
- Jahangiri L, Devlin H, Ting K, Nishimura I. Current perspectives in residual ridge remodeling and its clinical implications: a review. J Prosthet Dent. 1998 Aug;80(2):224-37. doi: 10.1016/s0022-3913(98)70116-7. PMID: 9710828.
- Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin Oral Implants Res. 2013 Nov;24(11):1231-7. doi: 10.1111/j.1600-0501.2012.02535.x. Epub 2012 Jul 12. PMID: 22784417.
- John G. Edwards, The prevention of relapse in extraction cases, AJO, Volume 60, Issue 2, 1971, Pages 128-141, ISSN 0002-9416, https://doi.org/10.1016/0002-9416(71)90029
- Priya D, Sundareswaran S, Mishra N, Sathyanathan S, Shibin M, Jisha B. Timing of Therapeutic Extractions Can Affect En Masse Anterior Retraction: A Split Mouth Randomized Clinical Trial. Turk J Orthod. 2024 Dec 31;37(4):213-220. doi: 10.4274/TurkJOrthod.2024.2023.6. PMID: 39743844; PMCID: PMC11705195.
- Verna C. Regional Acceleratory Phenomenon. Front Oral Biol. 2016;18:28-35. doi: 10.1159/000351897. Epub 2015 Nov 24. PMID: 26599115.
- Mathews DP, Kokich VG. Accelerating tooth movement: the case against corticotomy-induced orthodontics. Am J Orthod Dentofacial Orthop. 2013 Jul;144(1):5-13. doi: 10.1016/j.ajodo.2013.04.008. PMID: 23810039.
- Park, H., Lee, Y., Jeong, S., & Kwon, T. (2007). Density of the alveolar and basal bones of the maxilla and the mandible. American Journal of Orthodontics and Dentofacial Orthopedics, 133(1), 30-37. https://doi.org/10.1016/j.ajodo.2006.01.044
- Yu JH, Huang HL, Liu CF, Wu J, Li YF, Tsai MT, Hsu JT. Does Orthodontic Treatment Affect the Alveolar Bone Density? Medicine (Baltimore). 2016 Mar;95(10):e3080. doi: 10.1097/MD.0000000000003080. PMID: 26962841; PMCID: PMC4998922.
- Hsu JT, Chang HW, Huang HL, Yu JH, Li YF, Tu MG. Bone density changes around teeth during orthodontic treatment. Clin Oral Investig. 2011 Aug;15(4):511-9. doi: 10.1007/s00784-010-0410-1. PMID: 20393863.
- Daraqel B, Mheissen S, Li J, Khan H, Allan S, Zheng L. The effect of early versus delayed space closure on the rate of orthodontic tooth movement: a systematic review and meta-analysis. Eur J Orthod. 2023 Nov 30;45(6):680-689. doi: 10.1093/ejo/cjad015. PMID: 37203234.
- Abu Alhaija ES, Al Shayeb RA, Al-Khateeb S, Daher HO, Daher SO. A comparative assessment of the amount and rate of orthodontic space closure toward a healed vs recent lower premolar extraction site. Angle Orthod. 2022 Jul 1;92(4):463-470. doi: 10.2319/102921-797.1. PMID: 35344007; PMCID: PMC9235382.
- Proffit, William R., Henry W. Fields, and David M. Sarver. Contemporary Orthodontics. St. Louis, MO: Elsevier/Mosby, 2013.
- Mapare S, Mundada R, Karra A, Agrawal S, Mahajan SB, Tadawalkar A. Extraction or Nonextraction in Orthodontic Cases: A Review. J Pharm Bioallied Sci. 2021 Jun;13(Suppl 1):S2-S5. doi: 10.4103/jpbs.JPBS_549_20. Epub 2021 Jun 5. PMID: 34447032; PMCID: PMC8375952.
- Edwards, J. G. (1971). The prevention of relapse in extraction cases. American Journal of Orthodontics, 60(2), 128-141. https://doi.org/10.1016/0002-9416(71)90029-7
- Schreiber JJ, Anderson PA, Rosas HG, Buchholz AL, Au AG. Hounsfield units for assessing bone mineral density and strength: a tool for osteoporosis management. J Bone Joint Surg Am. 2011 Jun 1;93(11):1057-63. doi: 10.2106/JBJS.J.00160. PMID: 21655899.
- Vitral RW, Fraga MR, da Silva Campos MJ. Use of Hounsfield units in cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2015 Aug;148(2):204. doi: 10.1016/j.ajodo.2015.05.005. PMID: 26232821.
- Kuruthukulam RM, Patil AS. The center of resistance of a tooth: a review of the literature. Biophys Rev. 2023 Jan 17;15(1):35-41. doi: 10.1007/s12551-023-01042-z. PMID: 36909954; PMCID: PMC9995625.
- Yoshida N, Jost-Brinkmann PG, Koga Y, Mimaki N, Kobayashi K. Experimental evaluation of initial tooth displacement, center of resistance, and center of rotation under the influence of an orthodontic force. Am J Orthod Dentofacial Orthop. 2001 Aug;120(2):190-7. doi: 10.1067/mod.2001.115036. PMID: 11500662.
- Chang HW, Huang HL, Yu JH, Hsu JT, Li YF, Wu YF. Effects of orthodontic tooth movement on alveolar bone density. Clin Oral Investig. 2012 Jun;16(3):679-88. doi: 10.1007/s00784-011-0552-9.
- Ritwiroon, Nawaporn & Suzuki, Boonsiva & Suzuki, Eduardo Yugo. (2021). Effects of Alveolar Bone Width and Density on the Rate of Orthodontic Tooth Movement Introduction Material and Methods. The Journal of the Dental Association of Thailand. 71. 53-63. 10.14456/jdat.2021.6.
- Frost HM. The regional acceleratory phenomenon: a review. Henry Ford Hosp Med J. 1983;31(1):3–9.
- Danz, J. C., & Degen, M. (2025). Selective modulation of the bone remodeling regulatory system through orthodontic tooth movement—A review. Frontiers in Oral Health, 6, 1472711. https://doi.org/10.3389/froh.2025.1472711
- Gadhia A, Pepper T. Oral Surgery, Extraction of Teeth. [Updated 2023 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
- Schneider PP, Kim KB, da Costa Monini A, Dos Santos-Pinto A, Gandini LG Júnior. Which one closes extraction spaces faster: en masse retraction or two-step retraction? A randomized prospective clinical trial. Angle Orthod. 2019 Nov;89(6):855-861. doi: 10.2319/101618-748.1. Epub 2019 Jul 1. PMID: 31259616; PMCID: PMC8109172.
- Moresca R. Orthodontic treatment time: can it be shortened? Dental Press J Orthod. 2018 Nov-Dec;23(6):90-105. doi: 10.1590/2177-6709.23.6.090-105.sar. PMID: 30672990; PMCID: PMC6340199.
- Jiang F, Liu SS, Xia Z, Li S, Chen J, Kula KS, Eckert G. Hounsfield unit change in root and alveolar bone during canine retraction. Am J Orthod Dentofacial Orthop. 2015 Apr;147(4):445-53. doi: 10.1016/j.ajodo.2014.11.027. PMID: 25836004; PMCID: PMC4385197.
Interested in publishing your own research?
ESMED members can publish their research for free in our peer-reviewed journal.
Learn About Membership