





Segmental Bioimpedance Myography in Neuromuscular Diseases
Segmental electrical bioimpedance myography in normals and in patients with neuromuscular diseases: a case series
T Bertorini¹*, LA Talbot¹, EJ Metter¹, M Fagan¹ and W Mays¹*
¹UTHSC
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Bertorini, T., Talbot, L.A., et al., 2025. Segmental electrical bioimpedance myography in normals and in patients with neuromuscular diseases: a case series. Medical Research Archives, [online] 13(9).
https://doi.org/10.18103/mra.v 13i9.6982
COPYRIGHT: © 2025 European Society of Medicine. This is an open- access article distributed under the Terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v 13i9.6982
ISSN 2375-1924
ABSTRACT
Background: Bioimpedance myography is a useful nontraumatic, simple technique that assists in determining muscle mass and is increasingly used to assess muscle atrophy and disease progression. Studies indicate the results are reproducible and show strong correlation with DEXA scans and muscle ultrasound. This technique employs high-frequency, low-intensity electrical stimulation to measure the reactance and resistance of tissue, thereby determining muscle mass.
Methods: We conducted tests on forty-one normal subjects as well as patients with various neuromuscular diseases.
Results: Our study established normal values with variability less than 0.5%, providing examples of several disorders where decreased muscle mass was apparent in patients experiencing atrophy and weakness across different regions of the body. In conclusion, bioimpedance myography is a reliable, non-invasive method for assessing muscle mass, showing strong correlation with DEXA scans. It effectively identifies reduced muscle mass in neuromuscular diseases, aiding clinical evaluations and progression monitoring.
Keywords
bioimpedance myography, muscle mass, neuromuscular diseases, atrophy, DEXA scans
Introduction
Understanding muscle mass is important for assessing the impact of exercise in athletes and in monitoring neuromuscular diseases and sarcopenia. Accurate measurement not only aids in evaluating disease progression but also in gauging treatment responses. Among various techniques, electrical bioimpedance myography stands out as a simple, non-invasive method that effectively measures muscle mass. By applying high frequency, low intensity currents to the skin, this technique allows currents to penetrate the muscle tissue. The resulting responses are recorded using surface electrodes providing data on resistance and reactance. Resistance reflects changes related to the surrounding tissue such as water, fat, and connective tissue, while reactance provides insights into muscle fiber properties. The correlation between these parameters facilitates precise calculations of both regional and total muscle mass across different regional areas.
Electrical bioimpedance myography results correlate well with DEXA scan and ultrasound to determine the muscle mass in sarcopenia. This technique has been applied in various neuromuscular diseases, with pioneering studies initiated by Rutkove SB. It has also been extensively studied in axonal disorders such as ALS, spinal muscular atrophy, muscular dystrophy, and nerve radiculopathies. Additionally, it has been shown to help determine disease progression. Studies have found the technique to be quite easy and the results to be reproducible.
Different methods of bioelectric myography use either total body measurements or focus on individual muscle areas. The drawback of total body measurement is its inability to account for segmental atrophy, whereas individual muscle testing can be time consuming and fails to provide comprehensive total body results. This paper aims to study segmental bioimpedance myography, revealing those clinical findings of atrophy and wasting correlate well with decreased muscle mass as measured by bioimpedance.
Materials and Methods
We studied segmental bioimpedance myography using the FDA-approved Quantum RJL analyzer to determine muscle mass using eight electrodes. We assessed forty-one normal subjects and retested them on another day with the same examiner to evaluate variability. Additionally, we applied this technique to determine the characteristics of muscle atrophy and various disorders associated with decreased muscle mass through case examples, illustrating the correlation between clinical findings and measured decreases in muscle mass by bioimpedance. The Ethics Committee of the University of Tennessee Health Science Center approved this study.
Normal subjects included forty-one controls, which were tested and retested at different times by the same investigator to determine variability. Patients included four adults with familial spinal muscular atrophy, a patient with slowly progressive non-SMN I mutation spinal muscular atrophy affecting only the legs, one patient with amyotrophic lateral sclerosis, one patient with limb-girdle muscular dystrophy 2B, one patient with adult-onset Pompe disease, one patient with inclusion body myositis, one patient with distal muscular dystrophy, and one patient with myotonic dystrophy.
We assessed changes in the right and left upper and lower extremities, alongside measurements of the torso and total body. Given the limited number of cases available, statistical analysis was not performed; however, we provided illustrative examples that clearly demonstrated segmental atrophy corresponding to decreased muscle mass.
Results
We determined the normal values for each body segment as well as total body mass. We measured reactance, resistance, and calculated the phase, which corresponds to the muscle mass. Additionally, we reported the ratio of total muscle mass versus no muscle mass to establish normal muscle mass values for various segments of the body.
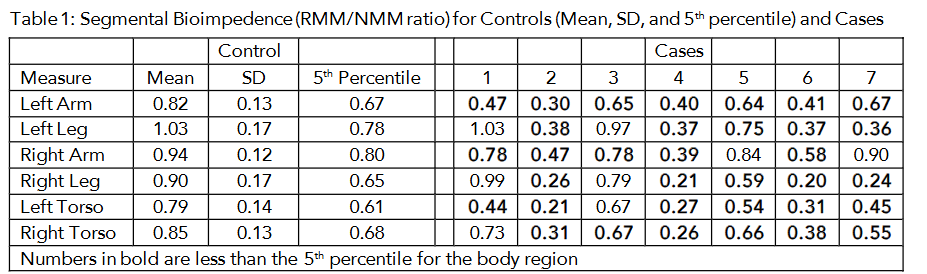
We found the variability among normal subjects was less than 0.5%. Further, we also discovered the technique to be quite easy to perform, taking less than 10 minutes per patient, and was nonpainful and comfortable.
Case Examples
Case #1 was a 63-year-old man with bibrachial diplegia form of ALS with very prominent atrophy and decreased muscle mass in the upper extremities, and minimal involvement of the legs. There was also decreased muscle mass in the torso. Bioimpedance demonstrated the atrophy in the arm and left torso.
Case #2 was a 48-year-old man with familial spinal muscular atrophy type 4, who demonstrated profound weakness in the lower extremities and decreased muscle mass in the torso. There was mild-to-moderate weakness and atrophy in the arms, with mildly decreased muscle mass. Bioimpedance demonstrated muscle loss in both arms, legs, and torso.
Case #3 was a 60-year-old man with classical ALS who had weakness and atrophy in the arms and legs, along with hyperreflexia. He had decreased muscle mass, primarily in the arms and torso. The bioimpedance was consistent with these findings.
Case #4 was a 72-year-old man with inclusion body myositis exhibited prominent weakness and atrophy in the legs, more prominent decreased mass in the right leg. He also had decreased muscle mass in the torso. The bioimpedance found decreased muscle mass in all areas.
Case #5 was a 76-year-old female with adult-onset Pompe disease. She exhibited moderate proximal wasting and weakness in the arms and legs, along with decreased muscle mass in the arms and legs, and torso. The bioimpedance found decreased mass in all areas except the right arm.
Case #6 was a 25-year-old female with limb-girdle muscular dystrophy type 2b. She exhibited weaknesses and atrophy more severe in the legs, with decreased muscle mass more profoundly in the legs and torso. The bioimpedance found decreased muscle mass in all areas.
Case #7 was a 45-year-old man with quadriceps-sparing distal muscular dystrophy. The patient exhibited severe weakness and atrophy in the distal legs, with more pronounced decreased muscle mass in the legs and torso. The bioimpedance found decreased muscle mass in all areas except the right arm. The bioimpedance test did not differentiate between proximal and distal weakness.
Discussion
Our study demonstrated that bioimpedance myography (BIM) is easy to perform, safe, with results that were reproducible with a variability of 0.5% in test-retest scenarios. In clinical practice, there is a need for objective parameters to monitor disease progression and response to treatment.
SIMPLICITY AND SAFETY
Bioimpedance myography is characterized by its simplicity and non-invasive nature. The procedure involves placing electrodes on the skin surface, making it easy to use without causing discomfort to the patient. This aspect is particularly beneficial in clinical settings where patient comfort and safety are essential.
REPRODUCIBILITY OF RESULTS
In our study, we observed reproducibility with a variability of 0.5% in test-retest scenarios. This level of consistency ensures that clinicians can utilize BIM for accurate monitoring over a period of time, making it a reliable tool for tracking disease progression or response to treatment.
CLINICAL RELEVANCE IN NEUROMUSCULAR DISEASES
One of the advantages of BIM is its ability to provide objective parameters for evaluating neuromuscular diseases. Traditional methods often rely heavily on subjective assessments, which can vary between practitioners. BIM offers quantifiable data on muscle mass and atrophy, providing clinicians with precise information about the extent and location of muscle loss. Our findings demonstrated that patients with segmental areas of muscle loss experienced decreased muscle mass in those regions. These results were consistent with classical clinical observations but provided additional quantitative insights necessary for informed medical decision-making.
COMPARISON WITH OTHER TECHNIQUES
When compared to other techniques like DEXA (Dual-Energy X-ray Absorptiometry) and ultrasound, bioimpedance myography proves more straightforward, cost-effective, and less time-consuming. Unlike DEXA scans which require specialized equipment and personnel, BIM can be performed quickly with minimal training. This makes it accessible for a wider range of clinical settings. Additionally, the equipment needed for BIM is relatively inexpensive compared to DEXA machines, allowing for more frequent monitoring without an excessive financial burden. The quick setup and measurement process make BIM suitable for routine clinical use without significantly adding to consultation times. This efficiency benefits both patients and healthcare providers by streamlining the diagnostic process.
Conclusion
Given these advantages—ease of use, safety, reproducibility, clinical relevance in neuromuscular diseases, simplicity compared to other techniques—we recommend considering the integration of segmental bioimpedance myography into routine clinical practice for monitoring neuromuscular diseases.
Funding
The bioimpedance assay instrument and equipment were donated by RJL systems (RJL systems 33945 Harper Ave, Clinton Township, MI 48035) the authors received no funding and have no financial conflicts of interest to declare.
Study Approval
This study was reviewed and approved by the University of Tennessee Health Science Center Institutional Review Board (14-03167-XP)
Conflict of Interest Statement:
None.
Acknowledgements:
None.
References:
- Kyle UG, Bosaeus I, DeLorenzo AD, et al. Bioelectrical impedance analysis? Part I: review of principles and methods. Clin. Nutr. 2004; 23:1226-1243.
- Rutkove SB. Electrical impedance myography: Background, Current state, and future directions. Muscle Nerve 2009;40(6):936-946.
- Janssen I, Maymsfield S, Baumgartner R, Ross, R. Estimation of skeletal muscle mass bioelectrical impedance analysis. J Appl. Physiol, 2000;89(2): 463-471.
- Rutkove SB, Kyoungmouk SL, Schiffman CA, Aaron R. Test-Retest Reproducibility of 50kHz Linear-Electrical Impedance Myography. Clin. Neurophys. 2006;117:1244-1248. Doi. 10.1016/j.clinph.2005.
- Rutkove SB, Geishbush TR, Mijailovic A., et al. Cross-sectional evaluation of electrical impedance myography and quantitative ultrasound for the assessment of Duchenne muscular dystrophy in a clinical trial setting. Pediat Neurol. 2014; 51:88-92. Doi:10.1016/j.pediatneurol.2014;02.015.12.029
- Roy B, Darras BT, Zaidman CM, Wu JS, Kapur K, Rutkove SB. Exploring the relationship between electrical impedance myography and quantitative ultrasound parameters in Duchenne muscular dystrophy. Clin Neurophysiol. 2019;130-:515-520.
- Iannuzzi-Sucich M, Prestwood KM, Kenny AM. Prevalence of sarcopenia and predictors of skeletal muscle mass in healthy, older men and women. J Gerontol A Biol Sci Med Sci. 2002;57:M772- M777
- Zaidman CM, Wang LL, Connolly AM, et al. Electrical impedance myography in Duchenne muscular dystrophy and healthy controls: a multi-center study of reliability and validity. Muscle Nerve. 2015; 52:592-597.
- Rutkove SB, Shefner JM, Gregas M, et al. Characterizing spinal muscular atrophy with electrical impedance myography. Muscle Nerve. 2020;42: 915-921.doi:10.1001/mus.21784.
- Rutkove SB, Caress JB, Cartwright MS, et al. Electrical impedance myography as a biomarker to assess ALS progression. Amyotroph Lateral Scler. 2012; 13:439-445.
- Spieker AJ, Narayanaswami P, et al. Electrical impedance myography in the diagnosis of radiculopathy. Muscle Nerve 2013;48:800–805.
- Offit MB, WU T, Floeter MK, Lehky TJ. Electrical impedance myography (EIM in a natural history study of C90RF72 mutation carriers. Amyotrophic Lateral Scler Frontotemporal Degener. 2020; 21:445-451.
- Li J, Sung M, et al. Electrophysiologic biomarkers for Assessing Disease Progression and the Effect of Riluzole in SOD1 G93A ALS mice. PLOS ONE. 2013;8:e65976
- Offit MB, Mohammad, Khanli H, Wu T, Lehky TJ. Electrical impedance myography in healthy volunteers. Muscle Nerve. 2024;69(3):288-294. Doi:10.1002/mus.27978.
- Sanchez B, Rutkove SB. Electrical Impedance Myography and its Applications in Neuromuscular Disorders. Neurotherapeutics. 2017;17:107-118 Doi: 10.1007/s1331-016-0491-x
- Bertorini Bertorini T, Knickerbocker J, Anwar H, Mays W, Carter K, Metter EJ, Talbot LA. A Case Series Examining Clinic, Laboratory, and Physical Function After Administration of Nusinersen in Adults With Spinal Muscular Atrophy, a Single-Center Study. J Clin Neuromuscul Dis. 2024 Dec 1;26(2):82-89. doi: 10.1097/CND.0000000000000512. PMID: 39590926.