






Selective Laser Trabeculoplasty Outcomes in Northern Ghana
Selective Laser Trabeculoplasty in Northern Ghana
J Simon¹, T Kenny², I Murdoch³*
- Director, Northern Community Eye Hospital, BA 108 Chinkara St, Rice City, Gumani, Tamale, Ghana NS-151-7998.
- Retired General Practitioner, United Kingdom.
- Honorary Associate Professor, Institute of Ophthalmology, University College London, UK.
[email protected]
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Simon, J., Kenny, T., et al., 2024. Selective Laser Trabeculoplasty in Northern Ghana. Medical Research Archives, [online] 13(1).
https://doi.org/10.18103/mra.v13i1.6141
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6141
ISSN 2375-1924
ABSTRACT
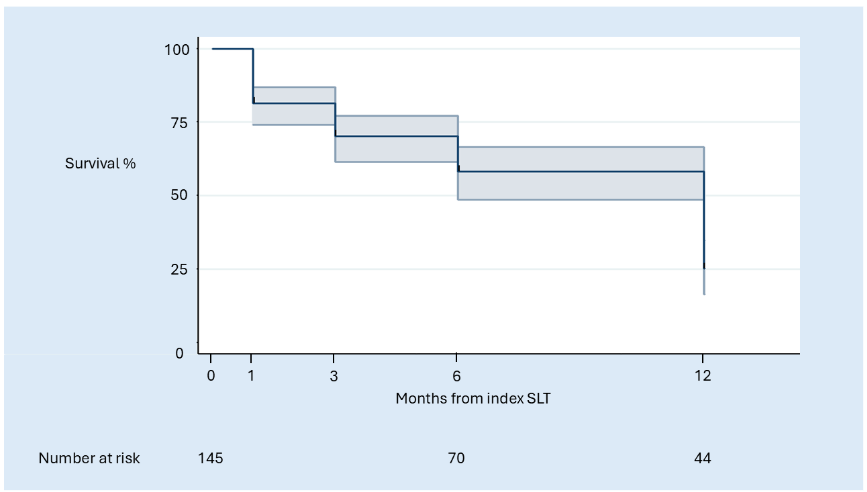
We report on a audit in Northern Ghana. A total of 283 selective laser trabeculoplasties (SLTs) were performed between September 2021 and September 2024. Because of co-linearity between right and left eye response therapy, 145 eyes individuals with primary open angle glaucoma were included in the analysis. Outcomes were assessed at 1, 3, and 12 months post index procedure. A success proportion of 75% (33/44) for a ≥20% reduction in IOP was achieved. No complications occurred in this cohort. This is comparable to other studies in the literature.
Keywords
Selective Laser Trabeculoplasty, Glaucoma, Intraocular Pressure, Northern Ghana
Introduction
Glaucoma, as a group of chronic ocular diseases characterized by progressive optic nerve damage and visual field loss. The most prevalent is primary open angle glaucoma, which is a significant public health concern worldwide, including in Ghana. The principal therapy for primary open angle glaucoma is the lowering of intraocular pressure. This can be done by medicine, surgery or laser. Selective Laser Trabeculoplasty (SLT) has emerged as a minimally invasive and effective treatment option for open angle glaucoma. Like its predecessor argon laser trabeculoplasty, SLT targets the trabecular meshwork. It uses a large spot size with low energy, which purportedly reduces the risk of damage to surrounding tissue. YAG it delivers a fraction (about 1%) of the energy. Both have similar mechanisms of action but SLT does not result in reduction of the intraocular pressure.
Inclusion criteria
1. Primary open angle glaucoma (POAG), pseudoexfoliative glaucoma, pigmentary glaucoma, secondary glaucoma (e.g. ischemic, diabetic, neovascular, steroid-induced, rubiosis, trauma, etc.)
2. Any contraindication to SLT (e.g. unable to sit at the laser-mounted slit-lamp, past history of or active uveitis, inadequate visualization of trabecular meshwork)
3. Congenital or early-onset glaucoma
4. Visually significant cataract with intention to undergo cataract surgery in the subsequent year
5. Recent cataract surgery within 3 months
6. Any active treatment for another ophthalmic disease
7. Any history of retinal ischemia, macular oedema, diabetic retinopathy, age-related macular degeneration
8. Any previous intraocular surgery, except uncomplicated cataract surgery more than 3 months prior to recruitment
9. Pregnancy at the time of recruitment, or intention to become pregnant within the duration of the trial
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Primary open angle glaucoma | Yes | No |
| Recent cataract surgery within 3 months | No | Yes |
| Any active treatment for another ophthalmic disease | No | Yes |
| Visually significant cataract | Yes | No |
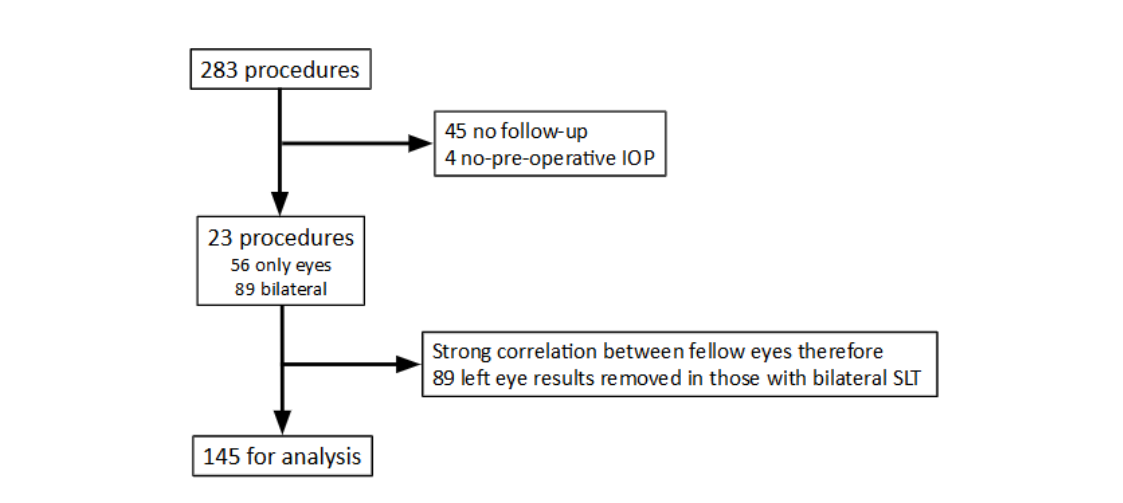
Of these 145, 61 eyes (figure 1) had pre-treatment IOP during the first year, where the mean (SD) pre-treatment IOP was 18.2 (±4.2) mmHg. The mean age at the time of SLT was 67 years (SD 16) ranging from 46-92 years. 22 eyes had repeat SLT during the first year (figure 1). The mean (SD) IOP at 1, 2 months, 5 months was 14.5 (±3.6), 12.5 (±3.2) and 12.5 (±3.3) mmHg respectively.
Discussion
Conclusion
We report an audit of SLT undertaken in Northern Ghana with a 75% success proportion comparable in an African context but lower than Caucasian studies. Our analyses showed a striking correlation in the response of fellow eyes in an individual to SLT which was not there when eyes from separate individuals were compared. This means any analysis of outcomes needs to either be of single eyes from individuals, or else random effects or other statistical techniques need to be applied to allow for the correlation and prevent an over estimation of sample size.
Conflict of Interest:
None
Funding Statement:
None.
Acknowledgements:
None.
References
1. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Burton, Matthew J et al., The Lancet Global Health, Volume 9, Issue 4, e489 – e551.
2. Glaucoma: now and beyond. Lancet, Jayaram H, Kolko M, Friedman DS, Gazzard G., 2023 Nov 11;402(10414):1788-1801.
3. Is laser trabeculoplasty the new star in glaucoma treatment? Töteberg-Harms, Marca; Meier-Gibbons, Francesb, Current Opinion in Ophthalmology 32(2):p 141-147, March 2021.
4. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Gazzard G., Ambler G. et al., The Lancet, Volume 393, Issue 10180, 1505 – 1516.
5. Selective laser trabeculoplasty versus 0·5% timolol eye drops for the treatment of glaucoma in Tanzania: a randomised controlled trial. Philippin H, Matayan E, Knoll KM, et al., Lancet Glob Health. 2021 Nov;9(11):e1589-e1599.
6. Physicians’ clinical experience and perspectives following a pilot, blended learning, point of care ultrasound course in Ghana- a mixed methods analysis. Pathak A, Limbani F, Awuku YA, Booth A, Joekes E. BMC Med Educ. 2024 Dec 4;24(1):1415.
7. Awareness of Glaucoma and Eye Health Services Among Faith-based Communities in Kumasi, Ghana. Murdoch C, Opoku K, Murdoch IJ Glaucoma. 2016 Oct;25(10):e850-e854.
8. Factors associated with adherence to treatment in patients with open angle glaucoma in Sierra Leone, West Africa: patient demographics and questionnaire. Kennedy A, Abosi U, Gilbert C, Mustapha J. Int Ophthalmol. 2022 Nov; 42(11):3479-3493.
9. Bridging the Language Barrier in Health Awareness. Opoku K, Murdoch IE. JAMA Ophthalmol. 2013;131(10):1367.
10. People and eyes: statistical approaches in ophthalmology. Murdoch IE, Morris SS, Cousens SN. Br J Ophthalmol. 1998 Aug;82(8):971-3.
11. Long-Term Safety and Outcomes of β-radiation for Trabeculectomy. Murdoch I, Puertas R, Hamedani M, Khaw PT. J Glaucoma. 2023 Mar 1;32(3):171-177