






Serum Biomarkers for COVID-19 Mortality Prediction
Comparison of serum risk factors for mortality from COVID-19
Valeria Juárez García1, Gustavo Acosta Altamirano2, Monica Sierra Martínez3, Pedro José Curi-Curi4
- Zaragoza Higher School Faculty, National Autonomous University of Mexico, Mexico
- Research Direction of “Dr. Eduardo Liceaga” General Hospital of Mexico, Mexico
- Molecular Biology Laboratory of Regional High Specialty Hospital of Ixtapaluca, State of Mexico, Mexico
- Direction of Planning, Teaching and Research, Regional High Specialty Hospital of Ixtapaluca, State of Mexico, Mexico
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Juárez García, V., Altamirano, GA., et al., 2024. Comparison of serum risk factors for mortality from COVID-19. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5774
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5774
ISSN 2375-1924
Abstract
Background and Aims: Coronavirus disease 2019 (COVID-19) is associated with a proinflammatory state that causes elevation of multiple serum variables. It has been observed that some biochemical alterations in patients with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection can be prognostic markers of severity and mortality. This study aims to compare different serum biomarkers to determine whether their alteration is associated with mortality due to COVID-19.
Methods: A case-control clinical study was carried out including patients with COVID-19 which were divided into two groups: with clinical improvement and those who died. Sociodemographic, clinical and serum variables (blood count, blood chemistry, lipid profile, markers of acute inflammation and troponin I) were studied. The serum variables were analyzed using the Receiver Operating Characteristic (ROC) curve, the Odds Ratio (OR) value was analyzed and the predictive value of each one was evaluated using the area under the curve.
Results: Of the 285 patients included, 161 showed clinical improvement and 124 died. It was established that lactic dehydrogenase (LDH) has the best predictive value for mortality, followed by troponin I and IL-6.
Conclusions: Elevated LDH upon hospital admission was found to have the best predictive value for mortality, followed by troponin I and interleukin 6 (IL-6). It was determined that the serum variables with the best prognostic value for severity and mortality are associated with cardiovascular damage, so we infer that if the SARS-CoV-2 virus considerably affects the heart, patients have a higher risk of death during their hospital stay.
Keywords: COVID-19, SARS-CoV-2, prognosis, biomarkers, severity of illness
Introduction
Clinical presentation spectrum of Coronavirus disease 2019 (COVID-19) goes from the asyntomatic patient to severe acute respiratory distress syndrome with invasive mechanical ventilation requirement. The pathophysiology of COVID-19 is complex and not only involves the respiratory system, but generates a multisystemic condition associated with an uncontrolled pro-inflammatory state in critically ill patients caused by a cytokine storm that leads to a fatal outcome. This severe acute respiratory syndrome coronavirus 2 virus (SARS-CoV-2) pro-inflammatory state causes biochemical alterations and an increase in biomarkers associated with cellular damage and inflammation.
Severity of SARS-CoV-2 is related to the patient risk factors such as older age, male gender, chronic comorbidities, and increased serum chemical markers associated with inflammation such as interleukin 6 (IL-6), C-reactive protein (CRP), lactic dehydrogenase (DHL), D-dimer, procalcitonin, ferritin and troponin I. Troponin I is a biomarker that tends to increase when acute myocardial injury develops and can reflect also a severe condition.
Patients with severe COVID-19 present with different biochemical alterations and it is currently known that some biomarkers can serve as predictors of the disease upon hospital admission. Each marker has been studied separately and different studies have suggested which is the best prognostic biomarker for in-hospital mortality in patients with COVID-19, including troponin I, but it has not yet been possible to reach a consensus on which serum marker has the best mortality predictive value. The aim of this study is to compare several serum risk factors in order to know which one has the higher mortality predictive value for COVID-19.
Methodology
A case-control clinical study was designed in order to compare serum mortality risk factors for COVID-19. Inclusion criteria were patients of both genders over 16 years of age, with clinical diagnosis of COVID-19 confirmed by polymerase chain reaction with reverse transcriptase (RT-PCR), who were admitted from January to December at a third level hospital during 2020 pandemia. Cases with clinical background of ischemic heart disease, acute heart failure and acute myocardial infarction within the previous 48 hours were excluded. All cases recruited at the above described period of time, were divided into two groups: those who had a favorable clinical outcome (control group) and the ones who died during their hospital stay (problem group).
Sociodemographic, clinical and serum data during hospital admission were obtained from the electronic clinical record of each patient. Data on blood count, blood chemistry, lipid profile and systemic markers of inflammation (CRP, D-dimer, ferritin, IL-6) were recorded out of a blood serum sample from peripheral vein. For the analysis of serum samples, the enzyme-linked fluorescent assay (ELFA) and the enzyme-linked immunosorbent assay (ELISA) were used. The established reference values correspond to those indicated by the supplier of each method used. This study was approved by the Institutional Research and Research Ethics Committees.
Statistic analysis
The information collected was recorded in an electronic Excel spreadsheet. Analysis was performed using SPSS statistical software (version 25.0). Numerical variables are expressed as mean ± standard deviation with minimum and maximum values of variability. Categorical variables are expressed as frequency and percentage in relation to the population at risk of each study group. Student t test was used to compare numerical variables with normal distribution, and Chi Square test was used to compare categorical variables, calculating the odds ratio with a 95% confidence interval. Mann Whitney U test was used to compare numerical variables without normal distribution. The serum values that presented statistically significant differences between the two studied groups, were analyzed using a Receiver Operating Characteristic (ROC) curve in order to determine the best sensibility and sensitivity cut-off point value expressed by the higher Area Under the Curve (AUC). Finally, we dicotomized each serum risk factor by means of the cut-off point obtained, and analyzed with a Chi Square test the one that had the best Odds ratio (OR) value (95% confidence Interval). A p <0.05 was considered statistically significant.
Results
A total sample of 285 cases was obtained, which were distributed into two groups. The cases recruited in the problem group were 124 (43.5%), while in the control group were 161 (56.5%). Table 1 shows the sociodemographic variables. Age and type 2 diabetes (DM-2) presented statistically significant differences between both groups (24.8% vs 40.3%, p=0.0057). Age was higher in cases at the problem group (51 years vs 55 years, p=0.017). In both groups DM-2 was the most prevalent chronic degenerative disease, although in the problem group the number of cases with this pathology was greater. In both groups, the most frequent comorbidities were systemic arterial hypertension followed by DM-2, and smoking history. In both groups, male gender represented more than half of the cases. According to the average body mass index (BMI), we observed overweight in both groups (29.3 vs 29.25).
Table 2 shows clinical variables of the studied groups. We can see that the respiratory rate upon admission was significantly higher in the problem group (27 vs 29, p<0.001) as well as the heart rate (99 vs 104, p=0.011). Oxygen saturation (SO2) was significantly lower in the problem group (81% vs 67%, p<0.0001), as was the assessment of the state of consciousness using the Glasgow scale (15 vs 14, p=0.003). Capillary refill in the problem group was slower compared to the control group (2sec vs 3sec, p=0.023). The use of oxygen (O2) was significantly higher (126 vs 110, p=0.0205) in the problem group, as was the use of a reservoir mask (59 vs 66, p=0.0052), since more than half of the cases required this device to achieve optimal SO2 levels. Regarding the use of nasal prongs, simple mask and invasive mechanical ventilation (IMV), there were no significant differences in their use in both groups. Dyspnea occurred in a significantly greater number of cases in the problem group (121 vs 112, p=0.0015).
| Variable | CONTROL Group (n=161) | PROBLEM Group (n=124) | p |
|---|---|---|---|
| Age (years) | 51 ± 15 (21-84) | 55 ± 13 (16-81) | 0.017 |
| Gender | Male 101 (62.7%) | 91 (73.4%) | NS |
| Female 60 (37.3%) | 33 (26.6%) | NS | |
| Comorbidity | SAH 37 (23%) | 40 (32.3%) | NS |
| DM-2 40 (24.8%) | 50 (40.3%) | 0.0057 | |
| Asthma 3 (1.9%) | 0 (0%) | NS | |
| COPD 2 (1.2%) | 2 (1.6%) | NS | |
| Smoking 27 (16.8%) | 23 (18.5%) | NS | |
| Somatometry | Weight 79 ± 19 (43-120) | 78 ± 19 (40-142) | NS |
| Size 1.64 ± 0.09 (1.40-1.87) | 1.60 ± 0.8 (1.40-1.80) | NS | |
| BMI 29.3 ± 5.41 (47.47-18.20) | 29.25 ± 5.81 (49.31-17.78) | NS |
| Variable | CONTROL Group (n=161) | PROBLEM Group (n=124) | p |
|---|---|---|---|
| Temperature (°C) | 37.2 ± 0.94 (35-39.9) | 37.2 ± 0.9 (35.5-39.3) | NS |
| Blood pressure (mmHg) | Systolic 114 ± 16 (60-160) | 116 ± 17 (69-162) | NS |
| Diastolic 70 ± 9 (40-96) | 70 ± 11 (33-95) | NS | |
| HR (bpm) | 99 ± 19 (60-195) | 104 ± 17 (55-149) | 0.011 |
| RR (bpm) | 27 ± 7 (15-42) | 29 ± 7 (15-48) | 0.001 |
| SO2 (%) | 81 ± 13 (25-100) | 67 ± 16 (30-98) | < 0.0001 |
| Capillary refill(s) | 2 ± 1 (1-4) | 3 ± 1 (1-6) | 0.023 |
| Glasgow | 15 ± 1 (6-15) | 14 ± 1 (9-15) | 0.003 |
| Oxygen therapy | 126 (78.3%) | 110 (88.7%) | 0.0205 |
| Oxygen supply | Nasal prongs 62 (38.6%) | 40 (32.3%) | NS |
| Simple mask 3 (1.9%) | 1 (0.8%) | NS | |
| Reservoir mask 59 (36.6%) | 66 (53.2%) | 0.0052 | |
| IMV 2 (1.2%) | 3 (2.4%) | NS | |
| Tachypnea | 44 (27.3%) | 45 (28%) | NS |
| Polypnea | 19 (9.9%) | 26 (16.1%) | 0.0354 |
| Dyspnea | 121 (75.2%) | 112 (90.3%) | 0.0015 |
Table 3 presents serum variables, where it is observed that the problem group compared with the control group have significantly higher values of neutrophils (9.29 cell/mm3 vs 11.87 cell/mm3, p<0.0001), serum glucose (142 mg/dl vs 187 mg/dl, p<0.0001), and urea nitrogen (BUN) (19.61 mg/dl vs 28.1 mg/dl, p<0.0001) are significantly higher in the problem group. On the contrary, there were significantly higher values in the control group of lymphocytes (2.02 cell/mm3 vs 1.04 cell/mm3, p=0.037) and cholesterol (140 mg/dl vs 129 mg/dl, p=0.023). Regarding the markers associated with severity of COVID-19 disease, CRP, troponin I, D-dimer, lactic dehydrogenase (DHL), Interleukin-6 (IL-6) and ferritin, it is observed that their serum levels are significantly higher in the problem group.
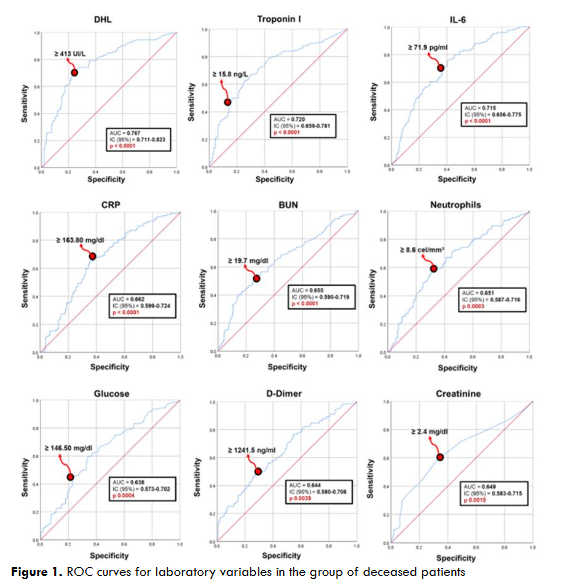
Figure 1 shows the ROC curves of the serum risk factors that were used to explore the predictive cut-off value for mortality from COVID-19. We can see that the serum variable with the greatest area under the curve (AUC) is DHL at a value of ≥413 IU/L, followed by troponin I at the level of ≥15.8 ng/l, and IL-6 at a value of ≥71.9 pg/ml. The AUC of the serum variables studied ranged between 0.6 and 0.7, indicating a high predictive value for clinical severity. Serum variables that presented statistically significant differences are summarized in Table 4. The serum values with the highest OR were DHL (7.5), troponin I (5.6) and IL-6 (4.9). Both DHL and troponin I are biomarkers associated with cardiac injury and have the greatest potential for predicting mortality at the cut-off points of ≥ 413 IU/L and ≥ 15.8 ng/l respectively, established in cases with COVID-19. The risk of death when presenting high concentrations is 7.5 times for DHL and 5.6 for troponin I, which indicates that if the SARS-CoV-2 virus considerably affects the heart, the risk of progressing to severe disease and death during the hospital stay is high.
| Variable | CONTROL Group (n=161) | PROBLEM Group (n=124) | p | OR (95% CI) |
|---|---|---|---|---|
| DHL (≥ 413 IU/L) | 37 (21.1%) | 86 (69.4%) | < 0.0001 | 7.5 (IC 0.08-0.22) |
| Troponin I (≥ 15.8 ng/l) | 26 (16.1%) | 60 (48.4%) | < 0.0001 | 5.6 (IC 0.12-036) |
| IL-6 (≥ 71.9 pg/ml) | 59 (36.6%) | 83 (66.9%) | < 0.0001 | 4.9 (IC 0.17-0.47) |
| CRP (≥ 163.80 mg/dl) | 62 (38.5%) | 81 (65.3%) | < 0.0001 | 4.4 (IC 0.20-0.54) |
| BUN (≥ 19.7 mg/dl) | 47 (29.2%) | 67 (54%) | < 0.0001 | 4.2 (IC 0.21-0.57) |
| Neu (≥ 8.6 cells/mm³) | 62 (38.5%) | 75 (60.5%) | 0.0003 | 3.6 (IC 0.25-0.66) |
| Glucose (≥ 146.50 mg/dl) | 38 (23.6%) | 54 (43.5%) | 0.0004 | 3.5 (IC 0.24-0.67) |
| D-dimer (≥ 1241.5 ng/ml) | 58 (36%) | 66 (53.2%) | 0.0039 | 2.8 (IC 0.30-0.80) |
| Creatinine (≥ 2.4 mg/dl) | 4 (2.5%) | 12 (9.7%) | 0.0015 | 2.4 (IC 0.07-0.76) |
Discussion
Identifying the risk factors in a patient with COVID-19 allows health personnel to detect the cases who are most likely to progress to a serious illness and thus provide timely treatment to reduce potential complications and prevent mortality. Advanced age in many infectious diseases is a determining factor for progression towards a serious condition, since the immune system response is compromised and comorbidities are more prevalent in this age group. In our study, the cases who had a fatal outcome of the disease (problem group) were significantly older compared to those who were discharged due to improvement, which agrees with what is reported in the literature. DM-2 was observed more frequently in both studied groups, mainly in cases of the problem group. It has been shown that this chronic degenerative disease increases the risk of death up to 3 times in cases with COVID-19, which is why it is considered an important risk factor. SAH was the second most frequent comorbidity in both groups. In the literature, SAH has been reported as the comorbidity that occurs most frequently in severely ill cases, contrary to what was reported in this study. DM-2 as the main comorbidity is associated with the fact that the study population is Hispanic and, due to genetic issues of insulin resistance, this chronic degenerative disease has a higher prevalence and incidence in our population. It has been shown that male gender is another factor that predisposes to complicated SARS-CoV-2 infection, which has been associated with the protective effect of hormones against an inflammatory state in females. On the other hand, the increase in converting enzyme receptors of angiotensin 2 (ACE2) in men facilitates the entry of the virus into a greater number of cells and a higher viral load.
More than half of the study population in both groups belonged to the male gender. Because COVID-19 presented high morbidity and mortality worldwide, we tried to identify the risk factors that contributed to a worse prognosis of the disease. Among the clinical factors already mentioned, serum risk factors were studied and it was observed that cases with COVID-19 present with different biochemical alterations. Among them, markers associated with inflammation stand out, since COVID-19 is closely related to a systemic pro-inflammatory state. In the most severe states of the disease, complement activation and the uncontrolled secretion of proinflammatory molecules lead to a cytokine storm that generates a serious pro-inflammatory state that not only affects the respiratory system, but also produces kidney, neurological and cardiovascular damage, generating fatal complications in cases.
IL-6 is a glycoprotein that is secreted during an acute inflammatory response and acts as an immunomodulator, activating T cells and promoting the differentiation of B cells to give way to the innate and adaptive response. High concentrations of IL-6 in cases with COVID-19 are associated with a greater probability of developing severe disease. In this study, it was determined that elevation of IL-6 above ≥ 71.9 pg/ml increases the risk of death in cases hospitalized with COVID-19 by 4.9 times. CRP is a protein that is synthesized in the liver in response to IL-6, so the increase in this protein is directly proportional to IL-6 concentrations. Both are markers of acute inflammation and their increase is associated with systemic inflammation and severe COVID-19 disease. CRP concentrations ≥163.80 mg/dl increase the risk of mortality 4.4 times and are significantly associated with severe disease and can be used as a prognostic indicator.
Among the serum variables studied, it was observed that the elevation in LDH concentrations predicts the risk of mortality to a greater extent compared to the other variables analyzed. LDH is a catalytic enzyme and is expressed in multiple tissues of the body, mainly in skeletal and cardiac muscle. This protein is released into the bloodstream in severe infections that cause tissue damage. Therefore, it has been proposed that LDH can be used as a prognostic marker of severity in COVID-19, since it has been determined that LDH is significantly higher in cases with severe COVID-19. In our study, elevated LDH upon hospital admission increases the risk of mortality 7.5 times in cases hospitalized with COVID-19. This enzyme is a very sensitive marker for tissue damage, but it is very nonspecific, since it is not only elevated by COVID-19, but also damage to any tissue or organ due to an etiology other than SARS-CoV-2 infection can generate release of this marker. For the use of this enzyme as a prognostic marker of severity, it is recommended to perform a more complete analysis where the isoforms of LDH are measured, especially LDH3, which is predominantly found in lung tissue and is what could be used as a prognostic marker of severity in cases with COVID-19.
The cut-off point for total LDH to predict severity has been estimated at 425 IU/L while in our population the cut-off point was determined at ≥413 IU/L, which is very similar to what has already been established. Another biomarker studied, was the increase in troponin I above the 99th percentile which correlates with in-hospital mortality 5.6 times, so it can be considered an independent prognostic marker. Troponin I is a protein found mainly in cardiac muscle cells and when they present functional damage this protein is significantly elevated, which is why it has been used as a biomarker of acute myocardial injury. Severe SARS-CoV-2 infection has been related to acute myocardial injury, so troponin I can be used as a prognostic marker of severity. It has been shown that elevated troponin I increases the mortality associated with acute myocardial injury up to 4.7 times and even in this study the risk of mortality is higher, since it increases the risk of in-hospital death by up to 5.6 times with a calculated cut-off value of ≥ 15.8 ng/L. Cardiac injury is a common complication that occurs as a consequence of COVID-19, since the viral infection spreads beyond the respiratory system, the tropism of the virus and the large number of ACE2 receptors in the heart promote significant myocardial injury due to an increase in free radicals, which has been associated with a high in-hospital mortality rate. Both DHL and troponin I are biomarkers associated with cardiovascular damage, which means that if the SARS-CoV-2 virus significantly compromises the heart, COVID-19 acquires severity criteria and a higher risk of mortality during the hospital stay.
Conclusion
Troponin I and DHL cardiac biomarkers are the ones that had the highest predictive value for mortality, so we can infer that when the great cardiac damage caused by COVID-19, the mortality is higher. IL-6 and CRP were the inflammatory markers that were also associated with mortality but to a lesser extent, increasing the risk of death 4.9 times and 4.4 times respectively. Both markers are related, since the secretion of IL-6 promotes the synthesis of CRP. In cases with SARS-CoV-2 infection, the integrity of the cardiovascular system must be monitored, because when cardiac damage is detected, these cases are at greater risk of complications and death. Therefore, serum variables analyzed in this study predict the risk of severe disease and mortality to different extents.
References
- Parasher A. COVID-19: Current understanding of its Pathophysiology, Clinical presentation and Treatment. Vol. 97, Postgraduate Medical Journal. BMJ Publishing Group; 2021. p. 312–20.
- Gusev E, Sarapultsev A, Solomatina L, Chereshnev V. Sars‐Cov‐2‐Specific Immune Response and the Pathogenesis of COVID‐19. Vol. 23, International Journal of Molecular Sciences. MDPI; 2022.
- Tjendra Y, Al Mana AF, Espejo AP, Akgun Y, Millan NC, Gomez-Fernandez C, et al. Predicting disease severity and outcome in COVID-19 patients: A review of multiple biomarkers. Vol. 144, Archives of Pathology and Laboratory Medicine. College of American Pathologists; 2020. p. 1465–74.
- De Michieli L, Babuin L, Vigolo S, Berti De Marinis G, Lunardon A, Favretto F, et al. Using high sensitivity cardiac troponin values in patients with SARS-CoV-2 infection (COVID-19): The Padova experience. Clin Biochem. 2021 Apr 1;90:8–14.
- Pitamberwale A, Mahmood T, Ansari AK, Ansari SA, Limgaokar K, Singh L, et al. Biochemical Parameters as Prognostic Markers in Severely Ill COVID-19 Patients. Cureus. 2022 Aug 30;
- Dubey DB, Mishra S, Reddy HD, Rizvi A, Ali W. Hematological and serum biochemistry parameters as a prognostic indicator of severally ill versus mild Covid-19 patients: A study from tertiary hospital in North India. Clin Epidemiol Glob Health. 2021 Oct 1;12.
- Endeshaw Y, Campbell K. Advanced age, comorbidity and the risk of mortality in COVID-19 infection. J Natl Med Assoc. 2022 Oct 1;114(5):512–7.
- Kang SJ, Jung SI. Age-Related Morbidity and Mortality among Patients with COVID-19. Infect Chemother. 2020 Jun 1;52(2):154–64.
- Pérez-Sastré MA, Valdés J, Ortiz-Hernández L. Características clínicas y gravedad de COVID-19 en adultos mexicanos. Gac Med Mex. 2020;156(5):373–81.
- Gao Y dong, Ding M, Dong X, Zhang J jin, Kursat Azkur A, Azkur D, et al. Risk factors for severe and critically ill COVID-19 patients: A review. Vol. 76, Allergy: European Journal of Allergy and Clinical Immunology. Blackwell Publishing Ltd; 2021. p. 428–55.
- Aguayo-Mazzucato C, Diaque P, Hernandez S, Rosas S, Kostic A, Caballero AE. Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Vol. 35, Diabetes/Metabolism Research and Reviews. John Wiley and Sons Ltd; 2019.
- Zhang J jin, Dong X, Liu G hui, Gao Y dong. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Vol. 64, Clinical Reviews in Allergy and Immunology. Springer; 2023. p. 90–107.
- Chauhan AJ, Wiffen LJ, Brown TP. COVID-19: A collision of complement, coagulation and inflammatory pathways. Vol. 18, Journal of Thrombosis and Haemostasis. Blackwell Publishing Ltd; 2020. p. 2110–7.
- Unver N, McAllister F. IL-6 family cytokines: Key inflammatory mediators as biomarkers and potential therapeutic targets. Vol. 41, Cytokine and Growth Factor Reviews. Elsevier Ltd; 2018. p. 10–7.
- Liu F, Li L, Xu M Da, Wu J, Luo D, Zhu YS, et al. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. Journal of Clinical Virology. 2020 Jun 1;127.
- Pepys MB. C-reactive protein predicts outcome in COVID-19: is it also a therapeutic target? Vol. 42, European Heart Journal. Oxford University Press; 2021. p. 2280–3.
- Serrano-Lorenzo P, Coya ON, López-Jimenez A, Blázquez A, Delmiro A, Lucia A, et al. Plasma LDH: A specific biomarker for lung affectation in COVID-19? Pract Lab Med. 2021 May 1;25.
- Ergenc I, Capar E, Sengel BE, Bahramzade G, Atalah F, Kocakaya D, et al. DIAGNOSTIC PERFORMANCE OF LACTATE DEHYDROGENASE (LDH) ISOENZYMES LEVELS FOR THE SEVERITY OF COVID-19. J Med Biochem. 2023;42(1):16–26.
- Capraru ID, Vulcanescu DD, Bagiu IC, Horhat FG, Popescu IM, Baditoiu LM, et al. COVID-19 Biomarkers Comparison: Children, Adults and Elders. Medicina (Lithuania). 2023 May 1;59(5).
- Zhang Y, Xiao LS, Li P, Zhu H, Hu C, Zhang WF, et al. Clinical Characteristics of Patients With Progressive and Non-progressive Coronavirus Disease 2019: Evidence From 365 Hospitalised Patients in Honghu and Nanchang, China. Front Med (Lausanne). 2020 Nov 16;7.
- Abbasi B Al, Torres P, Ramos-Tuarez F, Dewaswala N, Abdallah A, Chen K, et al. Cardiac Troponin-I and COVID-19: A Prognostic Tool for In-Hospital Mortality. Cardiol Res. 2020 Dec 1;11(6):398–404.
- Lippi G, Lavie CJ, Sanchis-Gomar F. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): Evidence from a meta-analysis. Vol. 63, Progress in Cardiovascular Diseases. W.B. Saunders; 2020. p. 390–1.
- Azevedo RB, Botelho BG, Hollanda JVG de, Ferreira LVL, Junqueira de Andrade LZ, Oei SSML, et al. Covid-19 and the cardiovascular system: a comprehensive review. Vol. 35, Journal of Human Hypertension. Springer Nature; 2021. p. 4–11.
- Wibowo A, Pranata R, Akbar MR, Purnomowati A, Martha JW. Prognostic performance of troponin in COVID-19: A diagnostic meta-analysis and meta-regression. International Journal of Infectious Diseases. 2021 Apr 1;105:312–8.
- Juárez V, Curi-Curi PJ. Acute myocardial injury as an independent factor of poor prognosis in severe COVID 19 disease. Indian Journal of Research. 2023;12(12).
- Lashgari R, Jabeen G, Prakash J, Kumal P, Rehman S. Inflammatory biomarkers and cardiac injury in COVID-19 patients.
- Del Prete A, Conway F, Della Rocca DG, Biondi-Zoccai G, De Felice F, Musto C, et al. COVID-19, Acute Myocardial Injury, and Infarction. Vol. 14, Cardiac Electrophysiology Clinics. W.B. Saunders; 2022. p. 29–39.
- Dawson D, Dominic P, Sheth A, Modi M. Prognostic value of Cardiac Biomarkers in COVID-19 Infection: A Meta-analysis. Res Sq [Internet]. 2020 June 13; Available from: http://www.ncbi.nlm.nih.gov/pubmed/32702736
- Sheth A, Modi M, Dawson D, Dominic P. Prognostic value of cardiac biomarkers in COVID-19 infection. Sci Rep. 2021 Dec 1;11(1).
- Walker CP, Deb S, Ling H, Wang Z. Assessing the Elevation of Cardiac Biomarkers and the Severity of COVID-19 Infection: A Meta-analysis [Internet]. Vol. 23, J Pharm Pharm Sci (www.cspsCanada.org). 2020