

Serum NT-proBNP and Ferritin in COVID-19 Prognosis
Study on Evaluation of Serum Cardiac Marker and Ferritin Levels in COVID 19 Patients
Dr Manjula Halevooru Siddarajaiah ¹, Dr P. Vijayalakshmi ², Sharan Prasad Chandrashekarpura Shivaprasad, MBBS ³, Vishesh Siddesh, BE MBA ⁴
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION Halevooru Siddarajaiah,M., Vijayalakshmi, P., et al., 2025. Study on Evaluation of Serum Cardiac Marker and Ferritin Levels in COVID 19 Patients. Medical Research Archives, [online] 13(6). https://doi.org/10.18103/mra.v13i6.6611
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i6.6611
ISSN 2375-1924
ABSTRACT
Background: COVID 19 pandemic is a systemic inflammatory condition caused by novel severe acute respiratory syndrome (SARS)CoV 2 virus infecting humans. The role of pro inflammatory cytokines such as interleukin (IL) 6, IL 12, IL 8 and tumour necrosis factor alpha causing dysfunctional immune response during the disease progression leads to acute respiratory distress syndrome and systemic organ failure. Ferritin is linked with COVID as a feature of respiratory oxidative stress (ROS) generation and secondary tissue damage. On the other side NTproBNP (N terminal pro brain natriuretic peptide) a heart failure marker also carries prognostic value in noncardiac conditions such as lung disease like in chronic obstructive pulmonary disease. However, its role in patients with COVID-19 and its prognostic value is still not well-established. Also, the relationship of ferritin an inflammatory marker with NTproBNP released in widespread alveolar damage or multi‑organ failure, and eventually death is not available widely.
Aim: The aim of the study is to evaluate the possible association between the N-terminal pro-brain type natriuretic peptide (NT-proBNP) levels and ferritin as a prognostic or diagnostic marker in COVID19 cases.
Methods and Material: This is a institutional record based cross sectional study, collected from records of patients admitted over a period of 4 months (July 2020-October 2020) at Jayadeva Institute of Cardiac sciences, Bengaluru, Karnataka, India. A total of 100 covid-19 patients were selected as per convenient sampling with CI-95% from the MRD case chart. Descriptive statistical analysis of data was done. Categorical variables such as age and gender were presented in (n)%. Continuous variables were expressed as mean±SD. ANOVA test was used to compare the parameters between quartiles (Q1- Q4) of Ferritin, p<0.05 was considered to be statistically significant. Pearson’s correlation coefficient was applied to analyse the correlation between study variables. The p-value <0.05 was considered statistically significant.
Results: The Random Blood glucose (RBG) was 117±60 which is on a higher range. Age is positively correlated with ferritin though minimal with r value 0.26 with p<0.01. Correlation with NTproBNP and age was r value 0.13 with p 0.19 with no statistical significance. Correlation between ferritin and NTproBNP was statistically significant with r value 0.56 with p <0.001. Analysis of variance across the quartiles was statistically significant for NTproBNP with p0.04, the other being close with p<0.06 however the other variables didn’t show statistical significance.
Conclusions: From the current study we conclude that serum NT pro BNP levels could be a marker of increasing severity of disease as it is seen with increasing quartiles of ferritin. A positive relationship exists between them Hence the cardiac stress marker elevated with inflammatory marker ferritin shows that both can be routinely used as a prognostic marker of COVID-19 or one can act as a surrogate marker for other in resource deficient conditions.
Key words: Inflammation, cardiac marker, prognosis, cascade, lung disease
INTRODUCTION
COVID19 which had a global outbreak is a systemic inflammatory condition caused by novel SARS CoV2 virus infecting humans. Covid 19 is associated with release of pro inflammatory cytokines such as IL6, IL12, IL 8 and TNF alpha. The cytokine storm is cascade of dysfunctional immune response presenting similar to influenza. The massive release of cytokines during the disease progression leads to acute respiratory distress syndrome and systemic organ failure.
For reasons still not completely understood some patients have poor outcomes and the factors responsible for determining these unfavourable factors are unclear. ROS generation and secondary tissue damage are postulated to be the association of increased ferritin levels in COVID cases.
As an indicator of disease progression and risk of mortality the levels of serum ferritin, d-dimer, lactate dehydrogenase, and IL-6 are found increasing during the worsening of the disease. Serum ferritin, has been found to be a feature of complication of viral infection, and those with compromised lung function seem more likely to have increased ferritin levels.
The presence of cardiac manifestations with or without previous history has been found in COVID 19 and also their association with mortality shown as altered cardiac biomarkers been reported in patients with COVID-19 related to disease severity and mortality.
ProBNP is released from ventricular myocytes which breakdown to give active peptide B-type natriuretic peptide (BNP) and the inactive N-terminal proBNP (NT-proBNP). The analyte is increased in response to high ventricular filling pressures, and hence it is routinely used as a marker for heart failure includes some cases of ischaemic insults.
NT-proBNP also carries prognostic value in noncardiac conditions such as lung disease like in chronic obstructive pulmonary disease However, its role in patients with COVID-19 and data on its prognostic value is still not well-established.
The excessive activation of inflammatory and immune-modulating pathways in patients with increasing severity of the disease, mandates the need for specific biomarkers of inflammation and immuno-activation in order to assist with management. The laboratory tests combined with the clinical evaluation can allow a rapid assessment of the patient’s condition for the optimal approach in these COVID-19 patients. Serum ferritin is studied due to its potential diagnostic and prognostic role.
Studies have shown that the NT-proBNP levels are independently linked with the in-hospital mortality rates in subjects with COVID-19 pneumonia and without HF. NTproBNP was reported to be very high even in non severe cases. Thus, we believe that this biomarker can be used as a valuable prognostic parameter in such cases.
The objective of the present study was to evaluate the possible association between the N-terminal pro-brain type natriuretic peptide (NT-proBNP) levels and ferritin as a prognostic or diagnostic marker in COVID19 cases.
MATERIALS AND METHOD:
STUDY POPULATION
This is an institutional record based cross sectional study, collected from records of patients admitted for over a period of 4 months (July 2020-October 2020) at Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bengaluru, Karnataka, India. A total of 100 covid-19 patients were selected as per convenient sampling with CI-95%.
Inclusion criteria: RT PCR Diagnosed case of COVID 19 admitted in the hospital for treatment and where patients’ laboratory investigations are available were selected for the study. The cases were discharged with treatment.
Exclusion criteria: Pregnant women, death of patient and non-availability of required biochemical laboratory data were excluded from our study.
DATA COLLECTION
The details of patients through case sheets were collected from medical records section, and biochemical investigation data was collected from central laboratory records. Sample size of 100 patients were collected. Data from random blood sample investigated at the time of admission were used for analysis. The sample collection was done with the red top clot activator tube which was centrifuged at 4000 rpm for 5 minutes after 25-30 mins for sample clotting. The biochemical parameters, random blood glucose, urea, creatinine, NTproBNP and ferritin were analysed using Cobas analyser.
Estimation of blood glucose was done by Glucose oxidase and peroxidase method in cobas 8000 c702 module. NTproBNP and ferritin was analysed by immune assay method on Cobas 8000 E602 module-automated analyser and commercial kit as per manual’s instructions. Serum Urea estimated by urease GLDH method as per kit protocol on in cobas 8000 c702 module instrument. Serum creatinine was measured using modified Jaffe’s kinetic method without deproteinization as per kit’s protocol.
STATISTICAL ANALYSIS:
Descriptive statistical analysis of data was done. Categorical variables such as age and gender were presented in (n)%. Continuous variables were expressed as mean±SD. Analysis of variance (ANOVA)test was used to compare the parameters between quartiles (Q1-Q4) of ferritin, a p value <0.05 was considered to be statistically significant. Pearson’s correlation coefficient was applied to analyse the correlation between study variables. A p-value <0.05 was considered statistically significant.
RESULTS
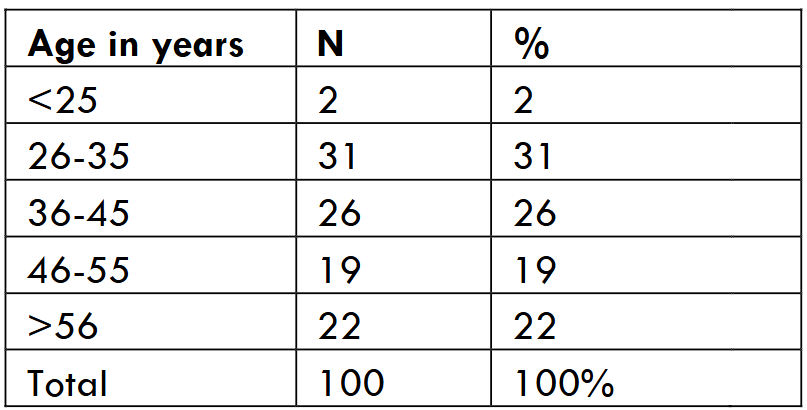
The demographic characteristics of study groups are presented in Table/Fig-1 for sex distribution and Table/Fig-2 for age distribution. In our study, the average age was 44.7 ± 15 years, Majority of patients ie. 31% were within 26 to 35 years. With a male-female distribution of 48% and 52% respectively.
Table/Fig-3 shows the mean ±SD of variables. The Random Blood glucose (RBG) was 117±60 which is on a higher range showing the patients had comorbid condition such as impaired glucose tolerance, Urea was 22.8±18.9. Creatinine values were within normal range 0.9±1.4 whereas creatinine in Q4 showed a above normal range which could indicate that the rise in ferritin levels has an effect on renal function or patients with compromised renal condition have increased inflammation and complications.
| Variable | Mean±SD | 95%CI |
|---|---|---|
| Age (years) | 44.7±15 | 41.76-47.64 |
| RBS (mg/dl) | 117.3±60 | 105.5-129 |
| Urea (mg/dl) | 22.8±18.9 | 19-26.5 |
| Creatinine (mg/dl) | 0.9±1.4 | 0.62-1.17 |
| NTproBNP (pg/ml) | 107.2±174.4 | 73-141.3 |
| Ferritin (µ/L) | 249.6±397 | 171.7-327.4 |
Table/Fig-4 shows the correlation among variables such as age with Biochemical parameters and between biochemical parameters. Age is positively correlated with ferritin though minimal r value 0.26 with p<0.01. Correlation with NTproBNP and age was r value 0.13 with p 0.19 with no statistical significance.

Correlation between ferritin and NTproBNP was statistically significant with r value 0.56 with p <0.001.
Table/Fig-5 Shows variable comparision across ferritin quartiles (Q1-Q4). FerritinQ1 (<39.5), Q2 (39.6 -102), Q3 (103-234), Q4(>235). The values expressed in mean ±SD. Analysis of variance across the quartiles was statistically significant for NTproBNP with p0.04, the other being close with p<0.06 however the other variables didn’t show statistical significance.
| Q1(<39.5) | Q2(39.6-102) | Q3(103-234) | Q4(>235) | p value | |
|---|---|---|---|---|---|
| Age | 40±12.9 | 47±15 | 42±10 | 50±19 | 0.06 |
| RBS | 105.5±47.2 | 112±60 | 123±57 | 129±74 | 0.52 |
| Urea | 18.7±13.3 | 22±9 | 21±9 | 30±33 | 0.18 |
| Creatinine | 0.8±0.3 | 0.72±0.2 | 0.77±0.2 | 1.42±2.7 | 0.24 |
| NT pro BNP | 60±65.8 | 93.4±96 | 84.7±111 | 191±299 | 0.04* |
Results expressed as Mean±SD;
Gender distribution male female Ferritin p value NTproBNP p value Age 0.26 <0.01* 0.13 0.19 NTproBNP 0.56 <0.001*
DISCUSSION
It is shown that up to 15% of COVID-19 patients have severe clinical manifestation, resulting in acute respiratory distress (ARDS) leading to death. The burden was huge and limited resources in developing countries like India, created a shift on to the role of laboratory medicine to aid in clinical decision making and risk stratification.
In the present study we found that serum level of NT proBNP was positively correlated with ferritin levels and which was also shown across the quartiles of ferritin. Study by Selcuk M et al. concluded that NTproBNP levels were linked with in hospital mortality in COVID 19 pneumonia and without heart failure. Similar conclusion was found in Juan Caro-Codón et al. study. A meta analysis study by Sorrentino et al also showed that NTproBNP was related with critically ill and patients who succumbed to.
Study by Ahmed et al showed that ferritin concentration to be a promising predictor of mortality, though, might not reliably predict severity but due to its availability it can be a useful marker for risk stratification and treatment plan in combination with other biochemical markers. This could be emphasised as we found a positive correlation between NTproBNP and ferritin in our study.
The combination of cTnI and NT-proBNP seemed to show superior predictive value for the composite events compared with each individual component. Study by Lalani K et al showed that age was independent predictors of mortality in COVID‑19 patients similarly our study has shown age to be positively correlated with both ferritin and NTproBNP. The mean age in Q4 was higher than other quartiles. Our study also had 22% of patients >56 years. A feedback mechanism exists between cytokines and ferritin which is shown as Ferritin, an acute-phase protein to be elevated in inflammation of both infectious and non infectious nature as it is associated with cell damage, oxidative stress, and the severity of chronic disease processes.
It is believed to be the role of pro-inflammatory cytokines that through liver produce several proteins like C-reactive protein (CRP) and ferritin. Also ferritin may have an active pathogenic role by stimulating pro-inflammatory pathways. Thus, both are interconnected.
Patients with comorbid condition like hypertension, diabetes, cerebrovascular illness are more likely to suffer from acute cardiac damage and mortality as a result of COVID‑19 infection. ACS is a well‑known COVID‑19 consequence, and its pathophysiology might be linked to the virus’s hypercoagulable condition, which causes coronary artery thrombosis. The cytokine storm is caused by unchecked and overreactive immune responses, resulting in widespread alveolar damage or multi‑organ failure, and eventually death from COVID‑ 19. Study by Lei Gao et al showed plasma NT-proBNP was positively correlated with age, similarly our observation saw a weak positive correlation with NTproBNP and age with r value 0.13 with p 0.19 but with no statistical significance.
Lalani K et al study reported serum creatinine levels in the severe disease group were substantially greater than those in the milder group which was also seen in our study as creatinine of 1.42 ±2.7 was found in Q4 whereas in Q1to Q3 was <1mg/dl though the features cannot be compared with disease severity as severity levels were not considered in the current study. Report by Lippi et al found creatinine and urea to be increased in non survivors. N-terminal natriuretic peptide (NT-proBNP) is associated with a worse prognosis in patients with ARDS. Cardiovascular manifestations play a significant role in predicting mortality among COVID‑19 patients. Whereas study by Lalani K et al reported that in the multivariable regression analysis, ferritin was not an independent predictor of mortality. Study by Chen et al reported that serum ferritin levels were significantly higher in the severe COVID‑19 group compared to the mild disease group. A similar relationship may exist between COVID-19 and NT-proBNP.
Key information connecting routinely performed clinical and analytical markers can be provided by assessment of NT-proBNP. In particular, a high level of NT-proBNP may suggest clinicians to be precautious and to timely perform a more accurate cardiac evaluation. Assessing NT-proBNP may represent a surrogate of invasive monitoring in poor resource setting and support the medical therapy.
Limitation
Relatively small sample size. A larger prospective study will be required to establish the clinical utility of NT proBNP in flu like disease like COVID. In addition, Other cardiac markers like troponin were not studied. The association with severity of disease were not studied.
Conclusion
From the current study we conclude that serum NT pro BNP levels could be a marker of increasing severity of disease as it is seen with increasing quartiles of ferritin. A positive relationship exists between them Hence the cardiac stress marker elevated with inflammatory marker ferritin shows that both can be routinely used as a prognostic marker of COVID-19 or one can act as a surrogate marker for other in resource deficient conditions.
Acknowledgement
We express our sincere thanks to the patients who helped us contribute to the study. Also our sincere thanks to our institution for their support.
References
- Kaushal K, Kaur H, Sarma P, et al. Serum ferritin as a predictive biomarker in COVID-19. A systematic review, meta-analysis and meta-regression analysis. J Crit Care. 2022;67:172-181. doi:10.1016/j.jcrc.2021.09.023
- Cheng L, Li H, Li L, et al. Ferritin in the coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J Clin Lab Anal. 2020;34(10). doi:10.1002/JCLA.23618
- Lino K, Guimarães GMC, Alves LS, et al. Serum ferritin at admission in hospitalized COVID-19 patients as a predictor of mortality. Brazilian Journal of Infectious Diseases. 2021;25(2). doi:10.1016/j.bjid.2021.101569
- Ziaie N, Ezoji K, Ziaei SG, et al. The relationship between N-terminal pro-brain natriuretic peptide (NT-proBNP) levels and diastolic heart failure in patients with COVID-19. Int J Cardiovasc Imaging. 2022;38(6):1289. doi:10.1007/S10554-021-02513-8
- Nguyen Trung ML, Tridetti J, Ancion A, Oury C, Lancellotti P. Natriuretic peptides in heart failure. Rev Med Liege. 2020;75(10):644-648. doi:10.1016/J.HFC.2017.08.002
- AZ, SS, CC, AA M. B-Type Natriuretic Peptide Concentrations, COVID-19 Severity, and Mortality: A Systematic Review and Meta-Analysis With Meta-Regression. Front Cardiovasc Med. 2021;8. doi:10.3389/FCVM.2021.690790
- O’donnell C, Ashland MD, Vasti EC, et al. N‑Terminal Pro‑B‑Type Natriuretic Peptide as a Biomarker for the Severity and Outcomes With COVID‑19 in a Nationwide Hospitalized Cohort. Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease. 2021;10(24):e022913. doi:10.1161/JAHA.121.022913
- Selçuk M, Keskin M, Çinar T, et al. Prognostic significance of N-Terminal Pro-BNP in patients with COVID-19 pneumonia without previous history of heart failure. J Cardiovasc Thorac Res. 2021;13(2):141-145. doi:10.34172/JCVTR.2021.26
- Chehrazi M, Yavarpour H, Jalali F, et al. Optimal cut points of N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) in patients with COVID-19. Egyptian Heart Journal. 2022;74(1). doi:10.1186/S43044-022-00253-1
- Trinder P. Determination of Glucose in Blood Using Glucose Oxidase with an Alternative Oxygen Acceptor. Ann Clin Biochem. 1969;6(1):24-27. doi:10.1177/000456326900600108
- Blackmore S, Hamilton M, Lee A, et al. Automated immunoassay methods for ferritin: Recovery studies to assess traceability to an international standard. Clin Chem Lab Med. 2008;46(10):1450-1457. doi:10.1515/CCLM.2008.304
- Prontera C, Zucchelli GC, Vittorini S, Storti S, Emdin M, Clerico A. Comparison between analytical performances of polyclonal and monoclonal electrochemiluminescence immunoassays for NT-proBNP. Clinica Chimica Acta. 2009;400(1-2):70-73. doi:10.1016/J.CCA.2008.10.011
- Osmic–Husni A, Hukic F, Saric MP. Comparison of Jaffe Method and Enzymatic Method at Measuring Serum Creatinine Level, Creatinine Clearance and Estimated Glomerular Filtration Rate. Mater Sociomed. 2023;35(2):113. doi:10.5455/MSM.2023.35.113-117
- Sorrentino S, Cacia M, Leo I, et al. B-type natriuretic peptide as biomarker of COVID-19 disease severity—a meta-analysis. J Clin Med. 2020;9(9):1-7. doi:10.3390/JCM9092957
- Ahmed S, Ansar Ahmed Z, Siddiqui I, Haroon Rashid N, Mansoor M, Jafri L. Evaluation of serum ferritin for prediction of severity and mortality in COVID-19- A cross sectional study. Annals of Medicine and Surgery. 2021;63. doi:10.1016/J.AMSU.2021.02.009
- Caro-Codón J, Rey JR, Buño A, et al. Characterization of NT-proBNP in a large cohort of COVID-19 patients. Eur J Heart Fail. 2021;23(3):456-464. doi:10.1002/EJHF.2095
- Wang L, Chen F, Bai L, Bai L, Huang Z, Peng Y. Association between NT-proBNP Level and the Severity of COVID-19 Pneumonia. Cardiol Res Pract. 2021;2021. doi:10.1155/2021/5537275
- Lalani K, Seshadri S, Samanth J, et al. Cardiovascular complications and predictors of mortality in hospitalized patients with COVID-19: a cross-sectional study from the Indian subcontinent. Trop Med Health. 2022;50(1):1-11. doi:10.1186/S41182-022-00449-W/TABLES/6
- Gómez-Pastora J, Weigand M, Kim J, et al. Hyperferritinemia in critically ill COVID-19 patients −Is ferritin the product of inflammation or a pathogenic mediator? Clinica Chimica Acta. 2020;509:249-251. doi:10.1016/j.cca.2020.06.033
- Kappert K, Jahić A, Tauber R. Assessment of serum ferritin as a biomarker in COVID-19: bystander or participant? Insights by comparison with other infectious and non-infectious diseases. Biomarkers. 2020;25(8):616-625. doi:10.1080/1354750X.2020.1797880
- Ruscitti P, Berardicurti O, Barile A, et al. Severe COVID-19 and related hyperferritinaemia: more than an innocent bystander? Ann Rheum Dis. 2020;79(11):1515-1516. doi:10.1136/ANNRHEUMDIS-2020-217618
- Marhaeni W, Felicia FV, Sumadi Jap AL, Hartoyo E, Andayani P. Comparing serum ferritin levels during COVID-19 infection and recovery period in pediatric patients with transfusion-dependent thalassemia, a single-center study. Front Med (Lausanne). 2023;10. doi:10.3389/FMED.2023.1056599
- Gao L, Jiang D, Wen XS, et al. Prognostic value of NT-proBNP in patients with severe COVID-19. Respir Res. 2020;21(1). doi:10.1186/S12931-020-01352-W
- Lippi G, Plebani M. Laboratory abnormalities in patients with COVID-2019 infection. Clin Chem Lab Med. 2020;58(7):1131-1134. doi:10.1515/CCLM-2020-0198
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet. 2020;395(10223):507-513. doi:10.1016/S0140-6736(20)30211-7