

Sex-Based Insights in Aortic Valve Stenosis Research
Aortic Stenosis sexual dimorphism as a biological variable to decode the molecular mechanisms of aortic valve stenosis: The future toward sex-based precision therapies
Abdullah Alabdulgader ¹
PUBLISHED: 28 February 2025
CITATION Alabdulgader, A., 2025. Aortic Stenosis sexual dimorphism as a biological variable to decode the molecular mechanisms of aortic valve stenosis: The future toward sex-based precision therapies. Medical Research Archives, [online] 13(2). https://doi.org/10.18103/mra.v13i2.6259
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i2.6259
ISSN 2375-1924
Abstract
Aortic valve stenosis (AVS) exhibits significant sexual dimorphism, influencing its pathophysiology, clinical presentation, and outcomes. Despite growing recognition of sex as a biological variable in cardiovascular diseases, the molecular mechanisms underlying AVS remain inadequately explored through a sex-specific lens. This paper investigates the role of sexual dimorphism in AVS by analyzing a large cohort of congenital heart disease (CHD) cases in Saudi Arabia, utilizing a comprehensive dataset of over 3 million variables. Our findings confirm a strong male predominance in AVS cases, with a male-to-female ratio of 3:1 (p=0.003), suggesting intrinsic biological differences in disease development. This paper highlights key genetic, epigenetic, and hormonal factors contributing to these disparities, including X-chromosome inactivation escape genes, Y-chromosome-linked risk factors, and sex-specific variations in valvular interstitial cell behavior. Furthermore, transcriptomic analyses reveal distinct male and female responses to fibrotic and calcific remodeling, potentially guiding future sex-based precision therapies. These insights emphasize the need to incorporate sex-specific considerations into AVS diagnosis, treatment, and therapeutic development, promoting a shift toward personalized medicine in congenital and acquired cardiovascular diseases.
Keywords
- Aortic Stenosis
- Sexual Dimorphism
- Congenital Heart Disease
- Precision Medicine
- Valvular Interstitial Cells
Introduction
Aortic valve stenosis (AVS) is a significant cardiovascular disorder with a complex and multifactorial etiology. It remains a major cause of morbidity and mortality worldwide, particularly among congenital heart disease (CHD) cases. While congenital malformations of the heart constitute a substantial burden on global health, an often-overlooked factor in their pathogenesis is the role of sexual dimorphism. Emerging evidence suggests that sex-based differences influence not only the clinical presentation and progression of AVS but also its underlying molecular mechanisms. However, the exact biological pathways driving these disparities remain insufficiently characterized.
Sexual dimorphism in cardiovascular disease is well-documented in both congenital and acquired conditions, with AVS serving as a paradigm of these differences. Epidemiological data indicate that AVS is more prevalent in males than females, with a striking male-to-female ratio of approximately 3:1 in congenital cases. This imbalance has been attributed to various factors, including sex hormones, genetic determinants, and epigenetic modifications. Recent research suggests that estrogen may exert a protective effect against AVS progression, whereas testosterone is linked to increased fibrosis and calcification in the aortic valve. Furthermore, genes that escape X-chromosome inactivation (XCI) in females may provide an additional protective mechanism against the fibrotic remodeling characteristic of AVS. Conversely, specific Y-chromosome haplogroups have been implicated in an increased risk of cardiovascular disease in males, suggesting a potential genetic predisposition that warrants further investigation.
In addition to hormonal influences, cellular sex differences also contribute to AVS pathophysiology. Valvular interstitial cells (VICs), the predominant cell type within the aortic valve, exhibit sex-specific transcriptional profiles and responses to fibrotic stimuli. Recent transcriptomic analyses have demonstrated that male VICs are more prone to myofibroblast activation and extracellular matrix (ECM) disorganization, which are hallmark features of stenotic aortic valves. Moreover, Rho-associated protein kinase (ROCK) signaling has been identified as a key pathway driving these sex-specific responses, with female VICs exhibiting differential regulation of ROCK-associated genes. Such findings underscore the importance of considering cell-intrinsic sex differences when investigating AVS pathogenesis.
Despite accumulating evidence supporting the influence of sex in AVS, current clinical approaches largely adopt a male-centric framework, overlooking potential sex-specific therapeutic strategies. Sex differences in pharmacokinetics and pharmacodynamics have long been recognized, yet most cardiovascular treatments remain standardized across sexes. The identification of molecular mechanisms underlying AVS sexual dimorphism presents an opportunity to develop targeted therapies that align with precision medicine principles. These could include sex-specific pharmacological interventions, biomaterial engineering for valve replacements tailored to the patient’s biological sex, and gene-based therapies designed to modulate sex-linked pathways in AVS progression.
Objectives
This paper aims to:
- Investigate the prevalence and sex distribution of AVS within a nationally representative cohort of CHD cases in Saudi Arabia.
- Identify genetic, epigenetic, and hormonal factors contributing to the sexual dimorphism observed in AVS progression.
- Analyze the role of VIC sex differences in ECM remodeling and fibrosis associated with AVS.
- Explore the implications of sex-based molecular mechanisms for future precision medicine approaches in AVS treatment and prevention.
By integrating epidemiological data with molecular insights, this paper seeks to advance the understanding of AVS sexual dimorphism, ultimately guiding the development of sex-specific precision therapies. Addressing these sex-based disparities is imperative for optimizing cardiovascular care and enhancing treatment efficacy in both congenital and acquired forms of AVS.
Materials and Methods
The investigation into aortic valve stenosis (AVS) as a sexually dimorphic condition was conducted within the broader framework of a nationwide study on congenital heart defects (CHD) across the Kingdom of Saudi Arabia. This extensive project included hospitals, primary healthcare centers, and specialized pediatric cardiology units focused on CHD management. CHD was defined as a significant structural abnormality of the heart or major intrathoracic vessels that affected functionality. Cases involving arrhythmias without associated structural abnormalities were excluded due to diagnostic uncertainties regarding their congenital nature.
Study Population and Data Collection: This paper encompassed a unique, nationally representative sample of live-born infants diagnosed with CHD within their first year of life over a five-year period. The primary objective was to identify potential genetic and environmental risk factors influencing the development of CHD, with a specific focus on AVS as a sexually dimorphic trait. For case identification, CHD status was coded as present (1) or absent (0). Data collection was meticulously designed, employing standardized data entry sheets

to capture over 3 million statistical variables across all cases, 40,000 of which were related to AVS.
Diagnosis and Classification: Each diagnosis was confirmed by certified pediatric cardiologists, following a hierarchical classification system that mapped 49 key morphogenetic landmarks to determine the precise timing of embryogenic disruptions
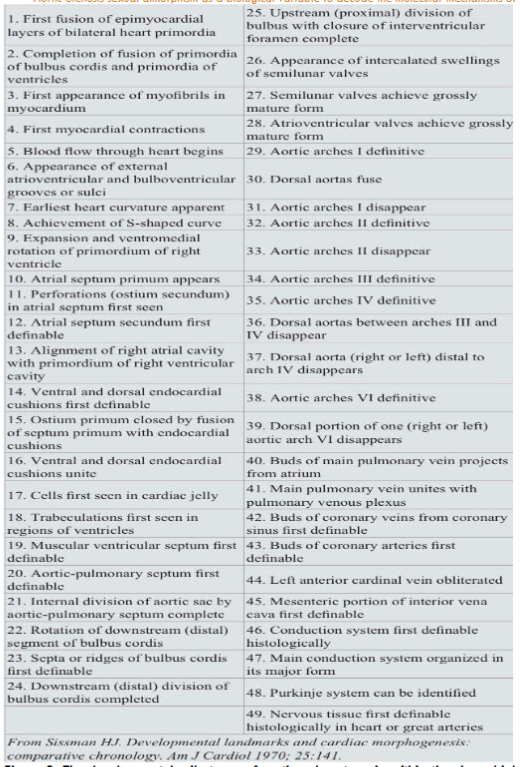
. This rigorous framework aimed to ensure the accuracy of the developmental stage associated with each case of AVS. Of the total 4,491 CHD cases included, 97 (2.6%) were identified as isolated AVS. Supra-valvular and sub-valvular aortic stenosis cases were excluded to maintain a specific focus on valvular pathology and its etiological (not hemodynamic) concerns.
Questionnaire and Exposure Assessment: Comprehensive questionnaires consisting of 412 variables per case were administered, addressing a wide range of potential genetic, physiological, and environmental risk factors. Parents, primarily mothers, were interviewed in person to ensure high data accuracy. These interviews explored exposure to environmental factors, medical history, and lifestyle practices during a defined six-month vulnerability period—three months pre-conception and three months post-conception.
Database Management and Statistical Analysis: The relational database, containing 3,018,724 variables, was managed using Oracle-SQL and interfaced with the SAS software package through ODBC connections. Data analysis utilized conditional logistic regression models, including stratified analyses that incorporated specialized macros to address matching and stratification needs effectively. This approach ensured that confounding factors were controlled for, enhancing the reliability of findings related to sex-based differences in AVS.
Cohorts for Comparative Studies: To further investigate AVS within the CHD context, two key cohorts were established. The first included 1,010 CHD-affected subjects paired with 1,010 controls, specifically examining extracardiac anomalies’ association with AVS. The second cohort consisted of 2,604 patients to assess the distribution of CHD types across Saudi Arabia’s four most populated regions. This strategy aimed to mitigate referral bias, given the concentration of cardiac care facilities in the central region.
Statistical Approach: The analysis strategy combined univariate and multivariate logistic regression methods, with maximum likelihood estimation as the primary algorithm. Descriptive statistics were reported as mean values with 95% confidence intervals (CIs), and associations between variables were tested using the Chi-square test. This robust approach aimed to quantify sex-based differences and establish AVS risk factors within the context of congenital heart disease.
Results
Isolated aortic valve (AS) pathology, mostly bicuspid aortic valve stenosis was found in 97 cases out of the project 4491 cases (2.16%)
| AS | Freq. | Percent | Cum. |
|---|---|---|---|
| NO | 4,394 | 97.84 | 97.84 |
| YES | 97 | 2.16 | 100.00 |
| TOTAL | 4,491 | 100.00 |
.
Percentage of cardiac defects in cohort of 2604 patients with congenital heart disease including AVS in the 4 most populated regions in Saudi Arabia is shown in table 2
| Lesion | Al Hassa | South | East | North | Central | West | Overall |
|---|---|---|---|---|---|---|---|
| VSD | 292 (39.5) | 109 (32.5) | 123 (38.4) | 359 (29.7) | 883 (33.9) | ||
| ASD | 85 (11.5) | 35 (10.4) | 37 (11.6) | 314 (26.0) | 471 (18.1) | ||
| PS | 66 (8.9) | 34 (10.1) | 29 (9.1) | 195 (16.1) | 324 (12.4) | ||
| PDA | 64 (8.6) | 53 (15.8) | 25 (7.8) | 159 (13.2) | 301 (11.6) | ||
| AVSD | 26 (3.5) | 12 (3.6) | 16 (5.0) | 38 (3.1) | 92 (3.5) | ||
| TOF | 31 (4.2) | 18 (5.4) | 15 (4.7) | 26 (2.2) | 90 (3.5) | ||
| AS | 26 (3.5) | 9 (2.7) | 9 (2.8) | 20 (1.6) | 64 (2.5) | ||
| COA | 20 (2.7) | 11 (3.3) | 6 (1.9) | 23 (1.9) | 60 (2.3) | ||
| D-TGA | 14 (1.9) | 5 (1.5) | 14 (4.4) | 22 (1.8) | 55 (2.1) | ||
| Other | 116 (15.7) | 49 (14.6) | 46 (14.4) | 53 (4.4) | 264 (10.1) | ||
| Total | 740 (100.0) | 335 (100.0) | 320 (100.0) | 1209 (100.0) | 2604 (100.0) |
.
Distribution of congenital heart disease defects among 2,604 patients based on sex
| Defects | Total | Males | Females | M:F |
|---|---|---|---|---|
| VSD | 883 | 442 (50.1) | 441 (49.9) | 1:1 |
| ASD | 471 | 224 (47.6) | 247 (52.4) | 0.9:1 |
| PS | 324 | 155 (47.8) | 169 (52.2) | 0.9:1 |
| PDA | 301 | 122 (40.5) | 179 (59.5) | 0.7:1 |
| AVSD | 92 | 44 (47.8) | 48 (52.2) | 0.9:1 |
| TOF | 90 | 45 (50.0) | 45 (50.0) | 1:1 |
| AVS | 64 | 48 (75.0) | 16 (25.0) | 3:1 |
| COA | 60 | 43 (71.7) | 17 (28.3) | 2.5:1 |
| D-TGA | 55 | 39 (70.9) | 16 (29.1) | 2.4:1 |
| Other | 264 | 137 (51.9) | 127 (48.1) | 1.1:1 |
| Total | 2604 | 1299 (49.9) | 1305 (50.1) | 1:1 |
. Male constitute 60.4% of AS cases, there is statistically significant difference (60.4% vs.39.6; P=0.003) with Pearson Chi square = 4.7227. Having a female baby has an Odd Ratio (OR =0.63) as predictor to AS compared to male, table 4
| Robust | AS | Odds Ratio | Std Err. | Z | P<IzI | [95% Conf. Interval] |
|---|---|---|---|---|---|---|
| Gender | Female | 0.6346228 | 0.133881 | -2.16 | 0.031 | 0.4197056 – 0.9595917 |
| _Cons | 0.027619 | 0.0036767 | -26.96 | 0.000 | 0.0212762 – 0.0358528 |
.
Discussion
Strong male predominance was observed in our population with congenital aortic valvular stenosis (AVS) as detailed in results section. A cohort of 2604 children with congenital heart disease was carried out to overcome any bias in referral as our total population showed dominance of central region where major cardiac centers are located. Analysis of this cohort is in concordance with total project population in incidence and sex dimorphism of AVS. Having a female baby has an Odd Ratio of (OR =0.63) and considered as protective predictor to AS compared to male (Table 4). This significant finding of male dominance of AVS is in concordance with worldwide reports.
In addition, AVS is sexually dimorphic, with sex differences in clinical presentation, pathophysiology, and postoperative outcomes. Sex hormones partially regulate cardiovascular disease, but there are other major players in the field as gonadectomized animal models show sexually dimorphic disease progression. Cardiovascular diseases control may be encoded in biological sex. Research shows that hormonal, genetic, and anatomical differences between sexes can lead to variations in how cardiovascular disease (CVD) develops and is managed. The primordia of mature valve leaflets during embryogenesis are the endocardial cushions (EC) which are composed of a highly organized extracellular matrix (ECM). The valve ECM is consisting of 3 distinct layers made of collagens, proteoglycans and elastin that together represent all the essential biomechanical properties to withstand constant changes in the hemodynamic environment.
Superficial valve endothelial cells (VECs) create uninterrupted protective endothelial protective layer over the leaflets and communicate at the molecular level with the underlying valvular interstitial cells (VICs) to modulate their behavior in response to shifts in the hemodynamic environment. Turnover of the valvular ECM is tightly regulated by valve interstitial cells (VICs) which are precursors to profibrotic myofibroblasts. In a healthy, non-diseased state, VICs are largely dormant and exhibit a fibroblast-like phenotype, contributing to the extracellular matrix and maintaining the integrity of the valve. However, in response to injury or disease, VICs can become activated and differentiate into profibrotic myofibroblasts. This activation is associated with increased production of ECM components and pro-fibrotic factors, which can lead to fibrosis and dysfunction of the heart valves. This process is crucial in the pathophysiology of various cardiovascular diseases, including aortic stenosis. Spatiotemporal coordination of ECM organization and VIC compartmentalization is characteristic of normal valve development which is disrupted in patients with diseased bicuspid aortic valve. Increased ECM Production, ECM Disorganization, and VIC disarray are cardinal features of the stenotic aortic valve in pediatric patients. It has been shown that male and female VICs have different gene expression profiles and phenotypes. Genetic and epigenetic alterations attributable to X and Y chromosomes which cause phenotypic differences between cells, have been thought to be due to intrinsic “sex” potentials of the somatic cells.
X chromosome inactivation (XCI) (also called Lyonization, after English geneticist Mary Lyon) is a process by which one of the copies of the X chromosome is inactivated. The inactive X chromosome is silenced by being packaged into heterochromatin (transcriptionally inactive structure). Escape from XCI results in sex-biased expression of at least 60 genes, potentially contributing to sex-specific differences in health and disease. The 15% to 25% of genes that escape X-chromosome inactivation (XCI) in female individuals is thought to be responsible about the sex-dependent variability in cellular phenotypes. On the other hand, increased risk of coronary artery disease in specific haplogroups of men has been linked to the Y chromosome. This critical biological differentiated cell line behavior is heralding new era for investigating sex dimorphism of VICs as strategic move toward decoding the secrets of dimorphic behavior of AVS progression with an eye on potential preventive and therapeutic measures. In addition to hormones, it seems that cell sex by itself is a potent contributor to healthy and diseased cellular phenotypes. Dimorphysm is not restricted to VICs. Other cell types that exhibit sexually dimorphic cellular behaviors include human umbilical vein endothelial cells, cardiac myocytes, skeletal muscle cells, and pluripotent stem cells. Various transcriptional factors mediate sex-biased regulatory programs independently of sex hormone receptor activity. Myofibroblasts can be defined as fibroblasts that assume some of the properties of smooth muscle cells and are able to contract the extracellular matrix. Rho-associated protein kinase signaling was found as a potential driver of sex-dependent myofibroblast activation. This was revealed using transcriptomic analysis of male and female porcine VICs. The elevated female myofibroblast activation through Rho associated protein kinase signaling is partially regulated by genes that escape X-chromosome inactivation such as BMX and STS (encoding for Bmx nonreceptor tyrosine kinase and steroid sulfatase, respectively).
In the clinical arena incorporating this new knowledge to treat congenital and acquired AVS with medication is phenomenal scientific fantasy reflecting marvelous scientific ambition. As a matter of fact, sex differences in pharmacokinetics and pharmacodynamics related to differences in drug absorption, distribution, and metabolism in vivo have long been recognized, but not implemented in therapeutics. Male centric approach is the rule and the bias toward males as the default norm prevail in today medical practice. The identification of sex-based protective factors, such as the lower odds of AVS in females, could be used to refine predictive models for AVS. Knowing a patient’s sex-related risk could help healthcare providers develop more effective prevention strategies, including earlier screening and lifestyle interventions. Another shrewd observation is the astute insight that cell sex regulates cellular responses to several small molecules. Cell responses to small molecule inhibition is affected by X-linked and Y-linked gene expression and epigenetic modifiers. World Health Organization (WHO) and other national as well as international leading authorities with the common goal to fight against human cardiovascular diseases needed to expedited the research aiming to provide the international arena with drugs that target sex-specific cardiovascular mechanisms. This new research direction underlines the potential for developing drugs that target sex-specific pathways in AVS. With increased understanding of how sex hormones and sex chromosomes influence AVS progression, pharmaceutical companies could design medications that consider differences in drug absorption, distribution, metabolism, and cellular response between men and women. This could improve efficacy and reduce adverse effects. Since sex hormones and X-chromosome-linked genes influence the progression of AVS, therapies that modulate hormone levels or target specific genes (e.g., genes that escape X-chromosome inactivation in females) could be developed. By focusing on the cellular mechanisms linked to each sex, such therapies might slow the disease’s progression or even prevent AVS in susceptible populations. Based on the differing cellular responses in male and female valvular interstitial cells (VICs), personalized biomaterials could be engineered for valve replacements. These materials could be optimized to match the patient’s sex-specific cellular environment, improving compatibility, durability, and reducing complications in AVS patients undergoing valve replacement surgery. Since male and female VICs have distinct gene expression profiles and phenotypic behaviors, isolating and potentially modifying these cells, gene and cell-based therapies could be tailored to address the specific cellular dysfunctions in AVS that are unique to each sex. This could include strategies to modulate Rho-associated protein kinase (ROCK) signaling, which influences myofibroblast activation differently in males and females. Small molecules that influence cellular responses can differ in efficacy based on the sex of the cells. This new knowledge could encourage research into small molecule inhibitors specifically designed for male or female VICs, providing targeted treatments that leverage sex-based cellular responses to achieve optimal therapeutic outcomes. Medical education, research protocols, and healthcare policies might need adjustment to incorporate sex as a significant biological variable in AVS and other cardiovascular diseases. Emphasizing sex-based approaches could accelerate the adoption of precision medicine, leading to more nuanced and effective treatment plans across patient populations. These advances are part of a broader movement toward individualized medicine, which tailors healthcare to each patient’s unique genetic, molecular, and phenotypic characteristics, including sex.
Conclusion
This paper highlights the critical role of sexual dimorphism in aortic valve stenosis (AVS), shedding light on the molecular, genetic, and cellular mechanisms that contribute to sex-specific differences in disease prevalence, pathophysiology, and outcomes. Our findings confirm a significant male predominance in AVS cases, with epidemiological data supporting a strong association between biological sex and disease risk. The differential regulation of valvular interstitial cells (VICs), extracellular matrix remodeling, and fibrotic progression suggests that intrinsic cellular sex characteristics, beyond hormonal influences, play a crucial role in AVS pathogenesis. Genetic and epigenetic analyses further reveal that X-chromosome inactivation escape genes may confer protective effects in females, while Y-chromosome-linked pathways contribute to increased disease susceptibility in males. The involvement of Rho-associated protein kinase (ROCK) signaling and other transcriptional regulators in sexually dimorphic VIC activation underscores the importance of targeting these pathways for potential therapeutic interventions. From a clinical perspective, this advocates for the integration of sex-based precision medicine into AVS management. Current diagnostic and therapeutic strategies remain largely male-centric, failing to consider the distinct molecular mechanisms underlying AVS in each sex. Recognizing these disparities could lead to significant advancements in early detection, risk stratification, and personalized therapeutic approaches. Future research should focus on developing sex-specific pharmacological treatments, bioengineered valve replacements tailored to sex-based cellular responses, and gene-based interventions that modulate sex-linked pathways involved in AVS progression. The broader implications of this paper extend beyond AVS, emphasizing the need for a paradigm shift in cardiovascular research and clinical practice. Incorporating sex as a fundamental biological variable will not only enhance our understanding of congenital and acquired heart diseases but also contribute to the development of more effective, equitable, and personalized treatments. This paper serves as a call to action for the scientific and medical communities to prioritize sex-based research in cardiovascular diseases, fostering a future where precision medicine addresses the unique biological differences between men and women.
References
- Alabdulgader A. Congenital heart disease in Saudi Arabia: current epidemiology and future projections. East Mediterr Health J. 2006;12:157-167.
- Simard L, Côté N, Dagenais F, et al. Sex-related discordance between aortic valve calcification and hemodynamic severity of aortic stenosis: is valvular fibrosis the explanation? Circ Res. 2017;120:681-691. doi:10.1161/CIRCRESAHA.116.309306
- Voisine M, Hervault M, Shen M, et al. Age, sex, and valve phenotype differences in fibro-calcific remodeling of calcified aortic valve. J Am Heart Assoc. 2020;9:e015610. doi:10.1161/JAHA.119.015610
- Sritharen Y, Enriquez-Sarano M, Schaff HV, Casaclang-Verzosa G, Miller JD. Pathophysiology of aortic valve stenosis: is it both fibrocalcific and sex specific? Physiology (Bethesda). 2017;32:182-196. doi:10.1152/physiol.00025.2016
- Fuchs C, Mascherbauer J, Rosenhek R, et al. Gender differences in clinical presentation and surgical outcome of aortic stenosis. Heart. 2010;96:539-545. doi:10.1136/hrt.2009.186650
- Ji H, Zheng W, Wu X, et al. Sex chromosome effects unmasked in angiotensin II-induced hypertension. Hypertension. 2010;55:1275-1282. doi:10.1161/hypertensionaha.109.144949
- Pessôa BS, Slump DE, Ibrahimi K, et al. Angiotensin II type 2 receptor- and acetylcholine-mediated relaxation: essential contribution of female sex hormones and chromosomes. Hypertension. 2015;66:396-402. doi:10.1161/HYPERTENSIONAHA.115.05303
- Hinton RB Jr, Lincoln J, Deutsch GH, et al. Extracellular matrix remodeling and organization in developing and diseased aortic valves. Circ Res. 2006;98:1431-1438.
- Lincoln J, Garg V. Etiology of valvular heart disease-genetic and developmental origins. Circ J. 2014;78(8):1801-1807. doi:10.1253/circj.cj-14-0510
- McCoy CM, Nicholas DQ, Masters KS. Sex-related differences in gene expression by porcine aortic valvular interstitial cells. PLoS One. 2012;7:e39980. doi:10.1371/journal.pone.0039980
- Masjedi S, Lei Y, Patel J, Ferdous Z. Sex-related differences in matrix remodeling and early osteogenic markers in aortic valvular interstitial cells. Heart Vessels. 2017;32:217-228. doi:10.1007/s00380-016-0909-8
- Shah K, McCormack CE, Bradbury NA. Do you know the sex of your cells? Am J Physiol Cell Physiol. 2014;306:C3-18. doi:10.1152/ajpcell.00281.2013
- Porras AM, McCoy CM, Masters KS. Calcific aortic valve disease: a battle of the sexes. Circ Res. 2017;120:604-606. doi:10.1161/CIRCRESAHA.117.310440
- Tukiainen T, Villani AC, Yen A, et al. Landscape of X chromosome inactivation across human tissues. Nature. 2017;550(7675):244-248. doi:10.1038/nature24265
- Wainer Katsir K, Linial M. Human genes escaping X-inactivation revealed by single-cell expression data. BMC Genomics. 2019;20:201. doi:10.1186/s12864-019-5507-6
- Charchar FJ, Bloomer LD, Barnes TA, et al. Inheritance of coronary artery disease in men: an analysis of the role of the Y chromosome. Lancet. 2012;379:915-922. doi:10.1016/S0140-6736(11)61453-0
- Maan AA, Eales J, Akbarov A, et al. The Y chromosome: a blueprint for men’s health? Eur J Hum Genet. 2017;25:1181-1188. doi:10.1038/ejhg.2017.128
- Witt E, Lorenz M, Völker U, et al. Sex-specific differences in the intracellular proteome of human endothelial cells from dizygotic twins. J Proteomics. 2019;201:48-56. doi:10.1016/j.jprot.2019.03.016
- Addis R, Campesi I, Fois M, et al. Human umbilical endothelial cells (HUVECs) have a sex: characterisation of the phenotype of male and female cells. Biol Sex Differ. 2014;5:18. doi:10.1186/s13293-014-0018-2
- Hartman RJG, Kapteijn DMC, Haitjema S, et al. Intrinsic transcriptomic sex differences in human endothelial cells at birth and in adults are associated with coronary artery disease targets. Sci Rep. 2020;10:12367. doi:10.1038/s41598-020-69451-8
- Lorenz M, Blaschke B, Benn A, et al. Sex-specific metabolic and functional differences in human umbilical vein endothelial cells from twin pairs. Atherosclerosis. 2019;291:99-106. doi:10.1016/j.atherosclerosis.2019.10.007
- Trexler CL, Odell AT, Jeong MY, Dowell RD, Leinwand LA. Transcriptome and functional profile of cardiac myocytes is influenced by biological sex. Circ Cardiovasc Genet. 2017;10:e001770. doi:10.1161/CIRCGENETICS.117.001770
- Lindholm ME, Huss M, Solnestam BW, et al. The human skeletal muscle transcriptome: sex differences, alternative splicing, and tissue homogeneity assessed with RNA sequencing. FASEB J. 2014;28:4571-4581. doi:10.1096/fj.14-255000
- Ronen D, Benvenisty N. Sex-dependent gene expression in human pluripotent stem cells. Cell Rep. 2014;8:923-932. doi:10.1016/j.celrep.2014.07.013
- Aguado BA, Walker CJ, Grim JC, et al. Genes that escape X chromosome inactivation modulate sex differences in valve myofibroblasts. Circulation. 2022;145(7):513-530. doi:10.1161/CIRCULATIONAHA.121.054108
- Soldin OP, Mattison DR. Sex differences in pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2009;48:143-157. doi:10.2165/00003088-200948030-00001
- Franconi F, Brunelleschi S, Steardo L, Cuomo V. Gender differences in drug responses. Pharmacol Res. 2007;55:81-95. doi:10.1016/j.phrs.2006.11.001
- Penaloza C, Estevez B, Orlanski S, et al. Sex of the cell dictates its response: differential gene expression and sensitivity to cell death inducing stress in male and female cells. FASEB J. 2009;23:1869-1879. doi:10.1096/fj.08-119388
- James BD, Guerin P, Allen JB. Let’s talk about sex: biological sex is underreported in biomaterial studies. Adv Healthc Mater. 2021;10:e2001034. doi:10.1002/adhm.202001034
- Forte E. How sex matters to aortic valves. Nat Cardiovasc Res. 2022;1:107. doi:10.1038/s44161-022-00024-w
- Alabdulgader A. Intelligent insights for noninvasive aortic valve stenosis therapeutics. Med Res Arch. 2024;12(8). Web. 5 Nov. 2024.