






Social Support’s Role in Diabetes Distress and Quality of Life
The Moderating Role of Social Support in the Association between Diabetes Distress and Health-Related Quality of Life in Rural Adults with Type 2 Diabetes
Sweta Mahato1*, Sijin Wen2, Ranjita Misra3
- Department of Social and Behavioral Sciences, School of Public Health, West Virginia University, 64 Medical Center Dr., Morgantown, WV 26505-9190, United States of America
- Department of Epidemiology and Biostatistics, School of Public Health, West Virginia University, 64 Medical Center Dr., Morgantown, WV 26505-9190, United States of America
- College of Nursing; University of South Florida, 12901 Bruce B. Downs Blvd., Tampa, FL 33612
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION Mahato, S., et al., 2025. The Moderating Role of Social Support in the Association between Diabetes Distress and Health-Related Quality of Life in Rural Adults with Type 2 Diabetes. Medical Research Archives, [online] 13(9). https://doi.org/10.18103/mra.v13i9.6918
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.6918
ISSN 2375-1924
ABSTRACT
Introduction: West Virginia, a rural and entirely Appalachian state, has the highest prevalence of diabetes in the U.S., which is associated with higher diabetes distress and lower health-related quality of life (HRQoL). Yet, few studies have explored the nuanced role of social support as a buffer against distress, that is pivotal in designing effective interventions. Therefore, this study explored the moderating effect of social support between diabetes distress (total and its four domains) and HRQoL among individuals with type 2 diabetes mellitus (T2DM) in West Virginia.
Methods: This statewide cross-sectional study of T2DM individuals was conducted during the COVID-19 pandemic (September 2021- December 2022) using an online REDCap survey. Participants completed socio-demographic characteristics (age, gender, race, educational status, income, and rural residence) along with the Diabetes Distress Scale (DDS-17), the Patient-Reported Outcome Measurement Information System (PROMIS-10) and a single-item measure of social support. Linear regression analyses estimated the association between HRQoL (outcome variable), diabetes distress (exposure variable) and its four domains (regimen-related, physician-related, interpersonal, and emotional burden) and interaction of social support and diabetes distress, adjusting for age, gender, race, education, income, diabetes duration and rural residence.
Results: A total of 1,026 participants (mean age=58.40 ± 12.54; 63.20% female) were included in the analysis. About half of the participants resided in rural areas and had low socio-economic status (i.e., 25% reported an annual income below $25,000 and 19% had a college degree). Participants had lower mean T-scores for global physical health (40.70 ± 9.20) and global mental health (41.50 ± 10.10) compared to the general U.S. population. Most participants (92.90%) reported having social support and low to moderate diabetes distress. Multivariate analysis revealed a significant moderating effect of physician-related distress on global mental health with social support having a protective role that buffered the negative impact of physician-related distress on global mental health.
Conclusion: Findings indicated that HRQoL was lower than the US population average among individuals with T2DM in West Virginia. Additionally, social support ameliorated the negative effects of physician-related distress on global mental health highlighting its protective role.
Keywords:
Diabetes Distress, Health-Related Quality of Life, Social support, Appalachia, Diabetes
Introduction
Type 2 Diabetes Mellitus (T2DM), a widely prevalent and complex chronic illness, is associated with significant psychological burden. Diabetes distress refers to the emotional burden, fear, stress, and worries from managing the demanding long-term care and diabetes complications. Individuals with T2DM report that they are burdened and overwhelmed by the complex and demanding daily self-care activities required to manage their disease, including monitoring blood glucose levels, counting carbohydrates, adhering to medication regimens, and maintaining regular physical activity. Although, moderate to severe diabetes distress is reported in approximately 25% of individuals with T2DM, the prevalence is higher among vulnerable populations, particularly during the COVID-19 pandemic. Hence, diabetes distress is a pivotal psychosocial concern and encompasses emotional responses related to the diabetes diagnosis, the burden of a demanding diabetes self-care regimen, challenging in diabetes care access and service utilization, difficult interactions with healthcare providers and/or inadequate support received from interpersonal relationships. Studies have shown that diabetes distress is associated with poor adherence to diabetes self-care, suboptimal glycemic control and an increased risk of diabetes-related complications. In addition, individuals with diabetes distress report lower HRQoL, particularly in rural and underserved populations. Since diabetes distress and depression/anxiety have a bilateral relationship, assessment of HRQoL is an important patient-centered outcome as it captures disparities in diabetes management and outcomes and provides a holistic assessment of T2DM individuals experiences that extend beyond clinical measures like glycemic control.
A growing body of evidence suggests that social support is a key factor that positively influences HRQoL in individuals with T2DM. Defined as support from family, friends, and healthcare providers, the stress buffering hypothesis posits that such support can protect individuals from the adverse effects of stressors such as diabetes distress on health outcomes such as HRQoL. The moderating effect of social support may occur through the provision of emotional support, encouragement, and having a more positive outlook on life and diabetes management, improved coping strategies and/or practical assistance with diabetes care. While most research studies confirm the positive relationship between social support and HRQoL, the moderating effect of social support has not been well studied, especially in rural Appalachian population. While a prior study in Nigeria reported that social support moderated the association between diabetes distress and HRQoL, the findings may not be generalizable to the United States, particularly the rural and Appalachian populations of West Virginia, where socio-cultural and healthcare access factors differ substantially.
West Virginia, a rural and the only fully Appalachian state, ranks 1st in the nation in the prevalence of diabetes (17.7%). Likewise, diabetes distress burden is higher in West Virginia individuals due to adverse social determinants of health (SDOH) and access barriers since the region is characterized by striking high poverty rates, low literacy and low health literacy rates. The adverse SDOH along with limited access to healthcare specialists and diabetes self-care management education and services contribute to poor adherence to self-care (e.g., healthy diet, physical activity, blood glucose monitoring, medication adherence, and foot care), poor glycemic control and poor HRQoL. In this context, understanding the moderating role of social support on the association between diabetes distress and HRQoL is crucial given that prior studies have not studied the nuanced moderating role of social support in the rural Appalachian population of West Virginia. Therefore, the objective of this study was to explore the moderating role of social support on the association between diabetes distress and HRQoL among T2DM individuals in West Virginia. Findings will enhance our understanding of the moderating effects of social support and thereby address critical gaps for supportive implementation strategies to develop culturally tailored interventions for rural individuals.
Methods
STUDY DESIGN AND PARTICIPANTS
This cross-sectional study used secondary data collected during the COVID-19 pandemic (September 2021 to December 2022) from community-dwelling West Virginia individuals living with diabetes and comorbid conditions (n=1,026). Participants were recruited by sending messages via a patient portal to eligible individuals (aged 18 years and older with an established diagnosis of diabetes). The message included a link to an online survey, and an electronic consent form administered via a secure, web-based application – the Research Electronic Data Capture (REDCap) application. Participation was voluntary, and anonymity and confidentiality of the participants were ensured. To encourage participation, $50 raffle gift cards were given to ten randomly selected individuals who completed the survey and provided their contact information. The data from the online survey were extracted and encrypted for analysis. The study was approved by the Institutional Review Board of West Virginia University (IRB protocol number: 2207604554).
DATA COLLECTION AND MEASURES
As part of a larger project, this study included measures of socio-demographic characteristics, diabetes distress, HRQoL and social support. Demographic characteristics included age (in years), gender (female, male), race (Non-white, White), education level (high school or GED, some College or Technical degree, bachelor’s degree, master’s degree, professional education or PhD), income (< $25,000, $25,000 – $49,999, $50,000 – $74,999, $75,000 – $99,999, and $100,000), diabetes duration (in years) and rural residence. Race was condensed into two categories i.e. white and non-white since the sample size was unevenly distributed across the racial groups. The US Department of Agriculture’s census tract-level Rural-Urban Commuting Area (RUCA) codes were computed from participant’s zip codes to categorize participants as urban (0), large rural city/town (1) or rural dwellers (2).
Diabetes distress was measured by the 17-item Diabetes Distress Scale (DDS). The DDS assessed 4 domains of diabetes distress: emotional distress (5 items), regimen-related distress (5 items), interpersonal distress (3 items), and physician-related distress (4 items). Participants responded to the questions from 1 (not a problem) to 6 (very serious problem). Total and subdomain diabetes distress scores were calculated; higher score indicated higher diabetes distress. Average scores of <2.0 indicated little or no distress, 2.0-2.9 indicated moderate distress and ≥3.0 indicated high distress.
HRQoL was assessed using the 10-item Patient-Reported Outcome Measurement Information System (PROMIS-10) scale, which comprises two dimensions: namely Global Physical Health (GPH) and Global Mental Health (GMH). Items were reverse coded as guided by the scale scoring recommendations. Standardized T-scores were computed from the raw scores for GPH and GMH to facilitate meaningful interpretation and enable comparisons with the national average for Americans. Social support was assessed by 1-item question which asked participants who provided them with social support during the pandemic. The multiple choices included someone I live with, friend or family who comes by my place, friend or family who I talk with on the phone (or video chat), other and I do not have social support. Responses were grouped into two groups: 1 = any form of social support versus 0 = no social support.
STATISTICAL ANALYSIS
Descriptive statistics were conducted for sociodemographic information of participants along with diabetes distress, HRQoL and social support. Continuous variables were depicted via means and standard deviations (SD), and categorical variables were expressed as frequencies (% and n). Pearson’s correlation was used to measure associations among the variables and check for multicollinearity. Rural residence, income and education were transformed into binary variables before running correlation and regression analyses; rural residence was categorized into urban and rural; income was categorized to have two categories namely <$50,000 and $50,000 and education had two categories namely at least some college or technical school and bachelor’s degree and higher. Linear regression analyses were conducted to estimate the association between HRQoL (outcome variable) and diabetes distress (exposure variable) and interaction term (social support* diabetes distress) adjusting for covariates (age, gender, race, education, income, diabetes duration and rural residence). Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) (version 29.0, SPSS Inc, Chicago) and Stata (version 17.0). Statistical inferences were based on a significance level of p < 0.05 (two-sided).
Results
The sample size was 1,026. Participants socio-demographic characteristics are reported in Table 1. The mean age and diabetes duration were 58.40 ± 12.54 and 11.57 ± 8.38 years, respectively. Approximately half of the participants (49.9%) resided in suburban areas, 26.6% in urban areas and 23.5% in rural areas. The sample was predominantly female (63.2%) and almost exclusively non-Hispanic White (98.6%), reflective of the lack of racial and ethnic diversity in the state. Approximately 25% of participants reported an annual income below $25,000 and only 19% had a bachelor’s degree- also reflective of the lower socioeconomic status of West Virginians.
| Socio-demographic characteristic | % | n (Total n=1,026) | Mean (Std. deviation) |
|---|---|---|---|
| Age (years) | 58.40 (12.54) | ||
| Diabetes duration (years) | 11.57 (8.38) | ||
| Rural residence | Urban | 26.60 | 261 |
| Large Rural city/town | 49.90 | 491 | |
| Rural | 23.50 | 231 | |
| Gender | Female | 63.20 | 639 |
| Male | 36.80 | 372 | |
| Race | Non-white | 1.40 | 14 |
| White | 98.60 | 999 | |
| Income | Less than $25,000 | 24.20 | 241 |
| $25,000 – $49,999 | 26.50 | 263 | |
| $50,000 – $74,999 | 20.50 | 204 | |
| $75,000 – $99,999 | 13.80 | 137 | |
| $100,000 or more | 15.00 | 149 | |
| Educational status | High School Graduate or GED | 25.10 | 255 |
| Some College or Technical School | 40.10 | 407 | |
| College Graduate (Bachelor’s Degree) | 19.30 | 196 | |
| Graduate Degree (Master’s, Professional Degree, or Doctoral Degree) | 15.60 | 158 |
The psychosocial characteristics of the participants are summarized in Table 2. The mean GPH and GMH T-scores were 40.7 ± 9.2 and 41.5 ± 10.1, which were below the US national averages, indicating lower HRQoL in West Virginia. The mean total diabetes distress score was 1.9 ± 0.9, indicating little or no distress among participants. The mean domain scores were: emotional burden (2.1 ± 1.2), physician-related distress (1.3 ± 0.7), regimen-related distress (2.2 ± 1.1), and interpersonal distress (1.8 ± 1.1). These scores suggest that, on average, participants experienced moderate or clinically significant levels of emotional burden and regimen-related distress while little or no physician-related distress and interpersonal distress. Most participants (92.9%) reported having social support, suggesting that the majority had access to assistance and support from family, friends, cohabiting partner or others.
| Psycho-social variables | % (n) | Mean | Std. Deviation |
|---|---|---|---|
| HRQoL | Global Physical Health | 12.20 | 3.20 |
| Global Mental Health | 12.50 | 3.50 | |
| Global Mental Health T-score | 41.50 | 10.10 | |
| Global Physical Health T-score | 40.70 | 9.20 | |
| Diabetes distress | Total Diabetes Distress | 1.90 | 0.90 |
| Emotional Burden | 2.10 | 1.20 | |
| Physician Distress | 1.30 | 0.70 | |
| Regimen Distress | 2.20 | 1.10 | |
| Interpersonal Distress | 1.80 | 1.10 | |
| Social Support | Yes | 92.90 (953) | |
| No | 7.10 (73) |
<td<0.01
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Age | 1 | ||||||||||||||
| 2 Diabetes duration | 0.31** | 1 | |||||||||||||
| 3 Rural residence | 0.03 | -0.06 | 1 | ||||||||||||
| 4 Income | 0.08* | 0.04 | -0.04 | 1 | |||||||||||
| 5 Education | 0.10** | 0.01 | -0.07* | 0.34** | 1 | ||||||||||
| 6 Race | -0.01 | -0.07 | 0.08** | 0.03 | 0.01 | 1 | |||||||||
| 7 Gender | 0.13** | 0.10** | -0.04 | 0.20** | 0.08* | <0.01 | 1 | ||||||||
| 8 Global Physical health | 0.11** | -0.01 | -0.04 | 0.40** | 0.29** | 0.03 | 0.19** | 1 | |||||||
| 9 Global mental health | 0.20** | 0.04 | -0.03 | 0.30** | 0.21** | 0.04 | 0.18** | 0.67** | 1 | ||||||
| 10 Total diabetes distress | -0.28** | -0.07* | 0.05 | -0.17** | -0.06 | -0.01 | -0.11** | -0.46** | -0.46** | 1 | |||||
| 11 Emotional burden | -0.27** | -0.03 | 0.02 | -0.15** | -0.07* | -0.02 | -0.07 | -0.45** | -0.44** | 0.92** | 1 | ||||
| 12 Physician distress | -0.06 | 0.10 | -0.10** | -0.01 | -0.04 | -0.03 | -0.22 | -0.23** | 0.61** | 0.45** | 1 | ||||
| 13 Regimen distress | -0.30** | -0.12** | 0.07* | -0.16** | -0.06 | <0.01 | -0.14** | -0.42** | -0.42** | 0.88** | 0.75** | 0.36** | 1 | ||
| 14 Interpersonal distress | -0.21** | -0.06 | 0.05 | -0.17** | -0.06 | 0.01 | -0.10** | -0.34** | -0.36** | 0.78** | 0.64** | 0.41** | 1 | ||
| 15 Social support | 0.07* | -0.01 | 0.01 | 0.08* | 0.07* | <0.01 | -0.05 | 0.10** | 0.14** | -0.13** | -0.13** | -0.01 | -0.11** | -0.18** |
Table 4: Linear Regression Model of HRQoL and Total Diabetes Distress
| Global Mental Health | Global Physical Health | |
|---|---|---|
| Variables | β coefficients [95% CI] p-values | β coefficients [95% CI] p-values |
| Total diabetes distress score | -2.80 [-4.79, -0.81] 0.01 | -3.32 [-5.12, -1.52] <0.001 |
| Rural residence (rural+large rural city) | 0.01 [-1.44, 1.47] 0.99 | -0.21 [-1.55, 1.12] 0.75 |
| Income (≥$50,000) | 3.96 [2.57, 5.34] <0.001 | 4.12 [2.83, 5.40] <0.001 |
| Education (bachelor’s degree and higher) | 1.91 [0.48, 3.33] 0.01 | 3.76 [2.45, 5.06] <0.001 |
| Race (White) | 0.61 [-4.53, 5.75] 0.82 | -0.20 [-5.76, 5.35] 0.94 |
| Gender (Male) | 1.59 [0.23, 2.95] 0.02 | 1.81 [0.56, 3.06] 0.01 |
| Social support (has social support) | 7.81 [2.28, 13.35] 0.01 | 2.64 [-2.53, 7.81] 0.32 |
| Diabetes duration | 0.003 [-0.08, 0.08] 0.93 | -0.03 [-0.10, 0.04] 0.39 |
| Age | 0.02 [-0.04, 0.07] 0.53 | -0.04 [-0.09, 0.01] 0.11 |
| Total diabetes distress * social support | -2.11 [-4.25, 0.03] 0.05 | -1.08 [-3.02, 0.85] 0.31 |
As shown in Table 4, individuals experiencing higher diabetes distress (total) had significantly poorer HRQoL as reflected by lower scores of GPH (β= -3.32, p<0.001) as well as GMH (β= -2.80, p=0.01). Socioeconomic factors were associated with better HRQoL; men and individuals with income > $50,000 and a bachelor’s degree reported higher GPH (β= 1.81, p=0.01; β= 4.12, p<0.001; β= 3.76, p<0.001) and GMH (β= 1.59, p=0.02; β= 3.96, p<0.001; β= 1.91, p=0.01) compared to women and those with lower socioeconomic status. Additionally, those with social support had significantly higher GMH (β= 7.81, p=0.01) compared to those without support. However, social support was not significantly associated with GPH. While no moderating effects of social support were observed for either GPH or GMH, the interaction term approached significance for GMH (p=0.05), suggesting that social support may moderate the relationship between total diabetes distress and GMH.
Emotional burden
As shown in Table 5, individuals with higher emotional burden had significantly lower GMH (β=-1.96, p=0.02) and GPH (β=-2.77, p<0.001). Similar to total diabetes distress, higher income, male gender and having a bachelor’s degree were positively and significantly associated with GMH (β= 4.22, p<0.001; β= 1.78, p=0.01; β= 1.83, p=0.01) as well as GPH (β= 4.32, p<0.001; β= 1.99, p=0.01; β= 3.64, p<0.001). Men and individuals with higher socioeconomic status (i.e., income > $50,000 and bachelor’s degree) reported higher GPH and GMH compared to women and those with lower socioeconomic status. Individuals with social support had higher GMH than those without social support (β=7.34, p=0.01), although social support was not significantly associated with GPH. Furthermore, social support did not moderate the association between emotional burden and GMH or GPH. In addition, the moderating effect of social support on the emotional burden-GMH relationship approached statistical significance (p=0.06) indicating a potential moderating role that warrants further investigation.
Table 5: Linear Regression Model of HRQoL and Emotional Burden
| Global Mental Health | Global Physical Health | |
|---|---|---|
| Variables | β coefficients [95% CI] p-values | β coefficients [95% CI] p-values |
| Emotional burden score | -1.96 [-3.53, -0.40] 0.02 | -2.77 [-4.17, -1.37] <0.001 |
| Rural residence (rural+large rural city) | -0.24 [-1.70, 1.22] 0.75 | -0.37 [-1.71, 0.96] 0.58 |
| Income (≥$50,000) | 4.22 [2.83, 5.61] <0.001 | 4.32 [3.04, 5.60] <0.001 |
| Education (bachelor’s degree and higher) | 1.83 [0.40, 3.26] 0.01 | 3.64 [2.33, 4.94] <0.001 |
| Race (White) | 0.49 [-4.69, 5.66] 0.85 | 0.08 [-5.48, 5.64] 0.98 |
| Gender (Male) | 1.78 [0.41, 3.14] 0.01 | 1.99 [0.74, 3.24] 0.01 |
| Social support (has social support) | 7.34 [2.19, 12.51] 0.01 | 1.50 [-3.26, 6.27] 0.53 |
| Diabetes duration | 0.02 [-0.06, 0.10] 0.62 | -0.02 [-0.09, 0.05] 0.58 |
| Age | 0.02 [-0.04, 0.08] 0.49 | -0.04 [-0.09, 0.01] 0.13 |
| Emotional burden * social support | -1.62 [-3.31, 0.06] 0.06 | -0.51 [-2.02, 0.99] 0.51 |
Table 6: Linear Regression Model of HRQoL and Physician-related Distress
| Global Mental Health | Global Physical Health | |
|---|---|---|
| Variables | β coefficients [95% CI] p-values | β coefficients [95% CI] p-values |
| Physician-related distress score | 0.81 [-2.28, 3.89] 0.61 | 0.12 [-2.63, 2.88] 0.93 |
| Rural residence (rural+large rural city) | -0.40 [-1.96, 1.16] 0.61 | -0.37 [-1.82, 1.08] 0.62 |
| Income (≥$50,000) | 4.58 [3.10, 6.06] <0.001 | 5.00 [3.61, 6.39] <0.001 |
| Education (Bachelor’s degree and higher) | 1.82 [0.30, 3.35] 0.02 | 3.79 [2.38, 5.21] <0.001 |
| Race (White) | 0.93 [-4.58, 6.44] 0.74 | 0.76 [-5.28, 6.80] 0.80 |
| Gender (Male) | 2.02 [0.56, 3.47] 0.01 | 2.19 [0.83, 3.55] <0.01 |
| Social support (has social support) | 10.07 [4.99, 15.15] <0.001 | 5.78 [1.17, 10.38] 0.01 |
| Diabetes duration | 0.01 [-0.08, 0.09] 0.98 | -0.03 [-0.11, 0.05] 0.45 |
| Age | 0.01 [0.04, 0.15] <0.01 | 0.03 [-0.02, 0.08] 0.30 |
| Physician-related distress * social support | -3.91 [-7.16, -0.65] 0.02 | -2.69 [-5.61, 0.22] 0.07 |
Unlike other domains of diabetes distress, physician-related distress was not significantly associated with either GMH or GPH. However, key sociodemographic variables continued to show significant and positive associations with both GPH and GMH as shown in table 6: higher income, having at least bachelor’s degree and male gender were positively and significantly associated with both GPH (β= 5.00, p<0.001; β= 3.79, p=<0.001; β= 2.19, p<0.01) and GMH (β= 4.58, p<0.001; β= 1.82, p=0.02; β= 2.02, p= 0.01). Men and individuals with higher socioeconomic status (i.e., income > $50,000 and bachelor’s degree) reported higher GPH and GMH compared to women and those with lower socioeconomic status. Additionally, older participants reported higher GMH (β= 0.01, p<0.01) while rural residence, race and diabetes duration were not significant predictors in the model. Likewise, individuals with social support had higher GMH (β=10.07, p<0.001) as well as GPH (β=5.78, p=0.01) as compared to those who reported no social support. Most importantly, results showed a significant moderating effect of social support for GMH (p=0.02) implying that the relationship between physician-related distress and GMH differed based on the presence of social support.
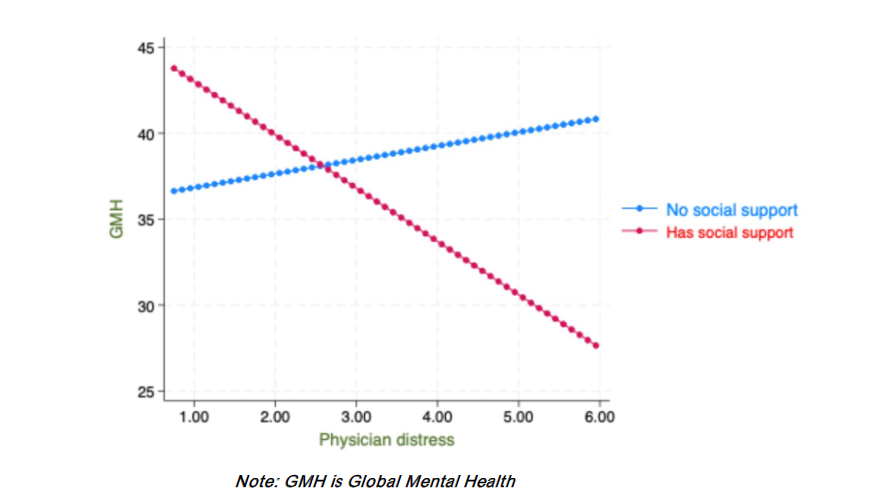
As illustrated in Figure 1, lower physician-related distress was significantly associated with higher GMH among individuals who had social support (β=-3.10, p<0.001). However, this association was not significant for individuals without social support (β=1.58, p=0.31). These findings suggest the protective role of social support for GMH.
Regimen-related distress
As shown in table 7, individuals with higher regimen-related distress had poorer GMH (β=-2.25, p<0.01) as well as GPH (β=-2.27, p<0.01). Higher income and having at least bachelor’s degree were positively associated with both GMH (β=4.27, p<0.001; β=1.69, p= 0.02) and GPH (β=4.42, p<0.001; β=3.54, p<0.001) indicating that individuals with higher socioeconomic status reported better HRQoL. Male gender was associated with GPH (β=1.63, p=0.01) but not GMH, suggesting that gender-based differences may be more pronounced in GPH rather than GMH. Participants rural residence, race, diabetes duration and age were not associated with both GMH or GPH. However, social support correlated with GMH (β=6.27, p=0.01) suggesting that individuals with social support had higher GMH. No moderating effects of social support were observed for either GPH or GMH.
Table 7: Linear Regression Model of HRQoL and Regimen-related Distress
| Global Mental Health | Global Physical Health | |
|---|---|---|
| Variables | β coefficients [95% CI] p-values | β coefficients [95% CI] p-values |
| Regimen-related distress score | -2.25 [-3.76, -0.75] <0.01 | -2.27 [-3.64, -0.91] <0.01 |
| Rural residence (rural+large rural city) | 0.21 [-1.28, 1.70] 0.78 | -0.06 [-1.42, 1.29] 0.93 |
| Income (≥$50,000) | 4.27 [2.86, 5.68] <0.001 | 4.42 [3.11, 5.72] <0.001 |
| Education (Bachelor’s degree and higher) | 1.69 [0.24, 3.14] 0.02 | 3.54 [2.21, 4.86] <0.001 |
| Race (White) | 1.11 [-4.14, 6.36] 0.68 | 0.76 [-4.90, 6.41] 0.79 |
| Gender (Male) | 1.36 [-0.03, 2.75] 0.05 | 1.63 [0.36, 2.91] 0.01 |
| Social support (has social support) | 6.27 [1.32, 11.22] 0.01 | 2.88[-1.76, 7.51] 0.22 |
| Diabetes duration | -0.02 [-0.10, 0.06] 0.61 | -0.06 [-0.13, 0.02] 0.13 |
| Age | 0.03[-0.03, 0.08] 0.32 | -0.04 [-0.09, 0.01] 0.14 |
| Regimen-related distress * social support | -1.04 [-2.66, 0.58] 0.21 | -0.84 [-2.31, 0.62] 0.26 |
Interpersonal distress
As shown in table 8, individuals with higher interpersonal distress had poorer GMH (β=-2.04, p=0.01) as well as GPH (β=-2.16, p<0.01). Socioeconomic status and male gender remained strong predictors of better GMH and GPH. Higher income, having a college degree and male gender were significantly (positively) associated with both GPH (β=4.46, p<0.001; β= 3.67, p<0.001; β= 1.93, p<0.01) as well as GMH (β= 4.18, p<0.001; β= 1.74, p=0.02; β= 1.74, p= 0.02). In contrast, rural residence, race, diabetes duration and social support were not associated with either HRQoL. Age was significantly associated with only GMH (β= 0.06, p= 0.05) indicating that older participants had better GMH. No moderating effects of social support were observed for either GPH or GMH.
Table 8: Linear Regression Model of HRQoL and Interpersonal Distress
| Global Mental Health | Global Physical Health | |
|---|---|---|
| Variables | β coefficients [95% CI] p-values | β coefficients [95% CI] p-values |
| Interpersonal distress score | -2.04 [-3.52, -0.55] 0.01 | -2.16 [-3.52, -0.80] <0.01 |
| Rural residence (rural+large rural city) | -0.17 [-1.70, 1.35] 0.82 | -0.22 [-1.63, 1.19] 0.76 |
| Income (≥$50,000) | 4.18 [2.73, 5.63] <0.001 | 4.46 [3.10, 5.81] <0.001 |
| Education (Bachelor’s degree and higher) | 1.74 [0.25, 3.23] 0.02 | 3.67 [2.29, 5.05] <0.001 |
| Race (White) | 1.63 [-3.75, 7.01] 0.55 | 0.93 [-4.94, 6.79] 0.76 |
| Gender (Male) | 1.74 [0.31, 3.16] 0.02 | 1.93 [0.60, 3.25] <0.01 |
| Social support (has social support) | 4.56 [-0.11, 9.23] 0.06 | 0.72 [-3.72, 5.15] 0.75 |
| Diabetes duration | -0.001 [-0.08, 0.08] 0.97 | -0.03 [-0.11, 0.04] 0.38 |
| Age | 0.06 [0.0003, 0.11] 0.05 | -0.003 [-0.06, 0.05] 0.91 |
| Interpersonal distress * social support | -0.59 [-2.21, 1.03] 0.47 | -0.13 [-1.61, 1.35] 0.87 |
Discussion
The primary aim of this study was to examine whether social support moderates the relationship between diabetes distress and HRQoL among individuals with T2DM in the rural state of West Virginia. Our findings showed that social support significantly moderated the association between physician-related distress and GMH. Specifically, individuals with social support experienced a weaker negative impact of diabetes distress on GMH as compared to those without social support. Additionally, it was also observed that individuals reported significantly lower GPH and GMH scores compared to the general United States population. These findings align with prior evidence showing that HRQoL is lower in rural individuals with T2DM compared to the United States population. West Virginia is a rural and the only fully Appalachian state in the nation with disproportionate burden of diabetes and related distress. In addressing the challenges faced by individuals with T2DM, our findings demonstrate that social support can play a protective role by buffering the negative effect of physician-related distress on GMH, consistent with the stress-buffering theory of social support.
Diabetes distress affects GPH and GMH and differences were noted in this rural population by gender and socioeconomic status. Since managing diabetes requires ongoing daily self-care that can present significant challenges, it is crucial to address psychosocial factors and promote healthy coping mechanisms to improve HRQoL in those living with T2DM. Hence, T2DM self-management interventions aimed at improving diabetes self-care and outcomes in rural individuals with T2DM may integrate social support while addressing psychosocial factors that promote healthy coping to improve overall HRQoL. More specifically, stress management sessions may focus on how to seek and cultivate support systems such as peer support groups or community networks to reduce challenges and address diabetes distress. Additionally, awareness and training of healthcare providers to address diabetes distress through improved patient-provider communication, recognizing the signs of distress and providing appropriate counseling, and connecting them with resources such as behavioral health services and emotional support is crucial. This can also improve a patient-centered care and empathetic communication and encouragement by providers that focus on physical, mental, and behavioral health.
There was a near-significant moderating effect of social support for emotional burden and total diabetes distress. This suggests that social support can provide a protective role in various domains of distress that warrants further investigation. Although the sample size of the study was large, detecting moderation effects can be challenging due to the need for sufficient variability in both the predictor and moderating variables. Alternatively, the trends toward moderating the association between emotional burden and total diabetes distress could be a reflection of this complexity rather than a lack of true moderation.
The findings of our study partly differs from a prior study conducted in Nigeria that indicated that social support moderated the association between diabetes distress and HRQoL for total diabetes distress as well as all domains of diabetes distress except emotional burden. The discrepancies between our study findings and those of Onu et al. may be explained by differences between the Eastern and Western cultures and the populations studied (i.e., West Virginia vs. Nigeria), as well as variations in how social support was conceptualized and measured. First, cultural differences between people in West Virginia and Nigeria may significantly influence how they perceive, understand, and use social support for chronic disease management. Social support can vary across populations depending on how families are involved, strength of family relationships and how connected people are within their local communities and community networks. Second, the differences in how social support was measured i.e., 1-item in this study versus Onu et al. (Brief Chronic Illness Resources Survey (BIRS); 22-items) could be a contributing factor for the discrepancies noted. Since social support has several domains, use of validated tools, such as the BIRS, for assessing an individuals available social support to manage their chronic illness, can provide better context and is recommended for future research.
The absence of a moderating effect of social support on the relationship between diabetes distress and GPH may have several explanations. One possibility is that social support tends to offer emotional and psychological benefits to individuals, which are more directly linked to improvements in GMH rather than GPH. In contrast, GPH often depend on adherence to diabetes self-care behaviors that necessitate instrumental social support. These includes tangible assistance with transportation to medical appointments, support with eating healthy and encouragement or shared participation in physical activity. This suggests research should differentiate the types and domains of social support and their specific effects on domains of diabetes distress and HRQoL.
In our sample, a higher proportion of participants had rural residence and low socio-economic status, reflective of the state’s rural and medically underserved population. In addition, a higher proportion of participants had elevated regimen-related distress and emotional burden as compared to interpersonal and physician-related distress. However, moderating effect of social support was observed only for physician-related distress. This may be attributed to several factors. One plausible explanation is that the type of social support available to participants may be better suited to address physician-related distress. For example, family and friends may provide support to help individuals navigate the healthcare system, remind them to ask questions, accompany them to appointments for emotional support, and share experiences and tips about communicating effectively that may effectively buffer physician-related distress. However, these forms of support might not be as relevant to other domains of diabetes distress. Likewise, some domains of distress (e.g., emotional burden and interpersonal distress) may be more internalized and personal and thus may necessitate more intensive psychosocial support from behavioral health providers such as counseling, therapy or sustained close relationships, unlike physician-related and regimen-related distress. Hence, patients may require specific support from trained providers or health coaches for emotional burden and interpersonal distress. Furthermore, the buffering effect of social support may be diminished when there is a mismatch between perceived and received social support. For example, while the sources of social support (family or friends) may express sympathy with good intentions, that may not help individuals feel supported.
Individuals with T2DM experience regimen-related distress from the burden and frustration from daily demands of managing their complex lifestyle and treatment regimens. This includes the stress associated with following a strict medication schedule, monitoring blood glucose levels regularly, adhering to a diet plan, and maintaining consistent physical activity. Individuals with T2DM often benefit from instrumental social support and informational social support. Instrumental support can include assistance with grocery shopping and cooking healthy meals and reminders to take medications, financial support or support with transportation for healthcare visits while informational support can include practical and relevant information pertaining to diabetes management and care including information on counting calories, information on diabetic friendly meal plans, local support groups for individuals with T2DM. While an individual may have a large social network, this does not necessarily guarantee access to instrumental or informational support. This disconnect can be especially pronounced in individualistic cultures, such as that of the United States, where individuals may be less likely to seek and receive, especially instrumental support.
Although social support can play an important role in reducing interpersonal distress, when individuals perceive that encounters and interactions with family and friends are the source of their distress, it creates a complex and often painful paradox. Instead of being a buffer, negative interactions can trigger stress, misunderstanding, or conflict. Therefore, social support to reduce interpersonal distress often calls for a more nuanced or external sources of support. These sources may include professional counseling and peer support groups where people share similar experiences. Thoits argues that, in addition to significant others (encompassing family), experientially similar others – individuals with similar experiences with managing diabetes- also serve as important sources of social support. She proposes that empathy, active coping assistance, and role modeling are key mechanisms through which social support buffers stress. Peer support groups offer individuals the opportunity to talk and listen without judgment and provided advice and guidance. Peer support groups are an integral component of group-based diabetes self-management programs that have been shown to effectively buffer the negative effects of interpersonal distress.
This study has several strengths. To our knowledge, this study was the first state-wide investigation into the moderating effects of social support using a large sample of T2DM individuals in a predominantly rural Appalachian state. Due to the large sample size, the estimates of population parameters have greater precision. Likewise, it increased the statistical power of hypothesis tests, thereby reducing the risk of Type II errors (i.e., false negatives) and enhancing the likelihood of detecting significant results when they exist. Additionally, our study used validated diabetes distress and HRQoL measures that allowed us to contextualize the domain-specific variations. However, several limitations should be noted. This is a cross-sectional study that limits causal inferences based on the findings. The self-reported measures used to assess diabetes distress, HRQoL and social support may have social desirability bias. Additionally, survey recruitment via an online patient portal and completion of online REDCap surveys and e-consent forms may have excluded participants with low digital literacy. In addition, the findings may not be generalizable outside of West Virginia because of the lower representation of racial and ethnic minority groups (3%) in the state. Additionally, using a single-item social support question may not have captured the multifaceted nature of social support and overlooked important dimensions such as tangible support, informational support, emotional support and appraisal support. In addition, data were collected during the COVID-19 pandemic when individuals with T2DM may have faced significant challenges to not only their routine diabetes clinical care but also self-care challenges and diabetes distress may have been more pronounced, especially for individuals living in rural and medically underserved areas in West Virginia. There is a possibility that pandemic related uncertainty and social isolation may have worsened individuals diabetes distress and HRQoL during the study period. Nevertheless, the study population was representative of the patient demographics in West Virginia. Although we cannot draw causal inferences from this cross-sectional study, our recruitment success highlights online patient portal and survey tools can be successfully used to track behavioral and EHR data for chronic disease care.
The study findings are important as it improves our understanding of the impact of social support on reducing diabetes distress and improving wellbeing of T2DM patients. Additionally, the findings can inform and support interventions and strategies to reduce distress and improve health outcomes. Our findings suggest that public health practitioners and educators should prioritize the development and implementation of targeted interventions designed to enhance social support for individuals with T2DM in order to attenuate the negative effect of diabetes distress on HRQoL; such interventions can be mobilization of health coaches or community health workers or peer support groups who are trained to provide them with various forms of social support such as appraisal support, informational support, emotional support and instrumental support. Future research should examine the role of different types of social support such as appraisal or informational support to guide more targeted interventions. Likewise, in-depth qualitative studies should be conducted to explore how social support can be mobilized in the context of diabetes distress, especially physician-related distress.
Conclusions
The study findings emphasize the protective role of social support in buffering the negative effect of diabetes distress, particularly physician-related distress, on GMH among T2DM individuals in West Virginia. In addition, lower GPH and GMH than the average US population were noted emphasizing the poor HRQoL in rural population of West Virginia. These findings underscore the importance of social support as a vital psychosocial resource to help individuals cope with challenges and stressors in rural and underserved areas of West Virginia. The findings also emphasize the need for interventions that integrate strategies to strengthen social support especially for individuals with elevated diabetes distress and low social support.
Conflicts of Interest Statement: The authors declare no conflict of interest.
Funding Statement: The authors declare no funding source used for this study.
Acknowledgements: We would like to acknowledge and thank all the study participants.
References
- Gonzalez JS, Hood KK, Esbitt SA, Mukherji S, Kane NS, Jacobson A. Psychiatric and psychosocial issues among individuals living with diabetes. 2021.
- Riise HK, Haugstvedt A, Igland J, et al. Diabetes distress and associated psychosocial factors in type 2 diabetes. A population-based cross-sectional study. The HUNT study, Norway. Diabetology & Metabolic Syndrome. 2025;17(1):62.
- Moawd SA. Quality of life in university students with diabetes distress: Type 1 and type 2 of diabetes differences. Journal of Diabetes Research. 2022;2022.
- Onu DU, Ifeagwazi CM, Prince OA. Social support buffers the impacts of Diabetes distress on health-related quality of life among type 2 diabetic patients. Journal of Health Psychology. 2022;27(10):2305-2317.
- Berry E, Lockhart S, Davies M, Lindsay JR, Dempster M. Diabetes distress: understanding the hidden struggles of living with diabetes and exploring intervention strategies. Postgraduate medical journal. 2015;91(1075):278-283.
- Dunn S, Smartt H, Beeney L, Turtle J. Measurement of emotional adjustment in diabetic patients: validity and reliability of ATT39. Diabetes Care. 1986;9(5):480-489.
- Nakahara R, Yoshiuchi K, Kumano H, Hara Y, Suematsu H, Kuboki T. Prospective study on influence of psychosocial factors on glycemic control in Japanese patients with type 2 diabetes. Psychosomatics. 2006;47(3):240-246.
- McCoy MA, Theeke LA. A systematic review of the relationships among psychosocial factors and coping in adults with type 2 diabetes mellitus. International journal of nursing sciences. 2019;6(4):468-477.
- Shayeghian Z, Aguilar-Vafaie ME, Besharat MA, et al. Self-care activities and glycated haemoglobin in Iranian patients with type 2 diabetes: can coping styles and social support have a buffering role? Psychology & Health. 2015;30(2):153-164.
- DS A, R S, B R, AK K, YJ C, Tang S ea. Diabetes Distress Among US Adults with Diagnosed Diabetes. https://www.cdc.gov/pcd/issues/2025/24_0287.htm. Published 2021. Accessed May 18, 2025.
- Mommersteeg PM, Herr R, Zijlstra WP, Schneider S, Pouwer F. Higher levels of psychological distress are associated with a higher risk of incident diabetes during 18 year follow-up: results from the British household panel survey. BMC public health. 2012;12:1-10.
- Wojujutari AK, Idemudia ES, Ugwu LE. Psychological resilience mediates the relationship between diabetes distress and depression among persons with diabetes in a multi-group analysis. Scientific Reports. 2024;14(1):6510.
- Beverly EA, Osowik F. Clinically significant depressive symptoms and high diabetes distress in adults with type 1 and type 2 diabetes in Appalachian Ohio. Journal of Osteopathic Medicine. 2021;121(10):813-824.
- Tareen RS, Tareen K. Psychosocial aspects of diabetes management: dilemma of diabetes distress. Translational pediatrics. 2017;6(4):383.
- Skinner TC, Joensen L, Parkin T. Twenty-five years of diabetes distress research. Diabetic Medicine. 2020;37(3):393-400.
- Fisher L, Polonsky WH, Hessler D. Addressing diabetes distress in clinical care: a practical guide. Diabetic Medicine. 2019;36(7):803-812.
- Abd El Kader AI, Ibrahim ME, Mohamed HS, Osman BM. Diabetes distress and self-care activities among patients with diabetes type II: a correlation study. SAGE Open Nursing. 2023;9:2377960823189944.
- Fisher L, Mullan JT, Arean P, Glasgow RE, Hessler D, Masharani U. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes care. 2010;33(1):23-28.
- Park H-S, Cho Y, Seo DH, et al. Impact of diabetes distress on glycemic control and diabetic complications in type 2 diabetes mellitus. Scientific Reports. 2024;14(1):5568.
- Zhu Y, Fish AF, Li F, Liu L, Lou Q. Psychosocial factors not metabolic control impact the quality of life among patients with type 2 diabetes in China. Acta diabetologica. 2016;53:535-541.
- Chew B-H, Mohd-Sidik S, Shariff-Ghazali S. Negative effects of diabetes related distress on health-related quality of life: an evaluation among the adult patients with type 2 diabetes mellitus in three primary healthcare clinics in Malaysia. Health and quality of life