





Stomas in CRS and HIPEC: Risks and Outcomes for Cancer
Stomas in Cytoreductive Surgery and Hyperthermic Intraoperative Peritoneal Chemotherapy for Colorectal and Appendiceal tumors: risk factors and outcomes
Teresa Moreno Djadou 1 MD PhD, Keat Seong Poh 1 MD, Shlomo Yellinek MD 1, Hana Fayazzadeh 3 MD, Kevin El-Hayek 4, MD, Conrad H. Simpfendorfer 2 MD, Giovanna DaSilva 1 MD, Steven D. Wexner 1 MD PhD (Hon)
- Departments of 1 Colorectal and 2General Surgery, Cleveland Clinic Florida, Weston, Florida;
- Department of Surgery, Cleveland Clinic, Cleveland, OH;
- Division of Surgical Oncology, Division of General Surgery, MetroHealth System, Cleveland, OH
OPEN ACCESS
PUBLISHED: 30 April 2026
CITATION: Moreno-Djadou, TM., Poh, KS., et al., 2026. Stomas in Cytoreductive Surgery and Hyperthermic Intraoperative Peritoneal Chemotherapy for Colorectal and Appendiceal tumors: risk factors and outcomes. Medical Research Archives, [online] 14(4).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Background: Cytoreductive surgery/hyperthermic intraperitoneal chemotherapy have evolved as promising treatments for peritoneal carcinomatosis of colorectal and appendiceal origin but are associated with high morbidity and mortality. For concomitant resections, stoma may mitigate against anastomotic leak or its adverse sequelae.
Objective Evaluate factors regarding decision-making and outcomes of stoma during cryoreductive/hyperthermic intraperitoneal chemotherapy.
Design: Retrospective review
Patients: All patients with appendiceal and colorectal neoplasms with peritoneal carcinomatosis who underwent cytoreductive surgery/hyperthermic intraperitoneal chemotherapy between 2009-2018. Patients were divided into those with and without a stoma.
Main outcomes: Surgical outcomes.
Results: 110 consecutive patients were identified. 78 (70.9%) did and 32 (29.1%) did not have a stoma: 46.9% loop ileostomies, 34.4% end ileostomies, 18.7% colostomies. 16.4% had diverting ileostomy. Preoperative factors associated with stoma formation included rectal tumor (p=0.031), body mass index <30 (p=0.023), hypoalbuminemia (p=0.036), and neoadjuvant chemotherapy (p=0.043). Peritoneal cancer index ≥10 (p=0.002), greater cytoreduction surgery (p<0.001), residual disease (p=0.002), more blood loss (p < 0.001), more blood transfusions (p<0.001), multiple small bowel resections (p<0.001), and multivisceral resections (p<0.001) also led to more stoma formation. Incidence of complications was 56.2% in patients with and 52.6% without a stoma (p=0.7). Patients with stomas had significantly more surgical site infections (p=0.006), severity of morbidity (Clavien-Dindo class 3/4; p =0.017), longer hospitalization (p=0.028), higher reoperation rate (p=0.010) and higher mortality (p<0.002). 8/32 (25%) patients underwent stoma reversal, one via laparotomy. Mean time to stoma closure was 5.3 ±2.8 months with a 4.5% morbidity rate. Limitations: Retrospective nature, heterogeneity of pathology/location, high-volume center with quaternary ancillary services leading to better resolution of complications but less generalizable results. Conclusions: Patient with appendiceal or colorectal neoplasms with higher carcinomatosis burden requiring extensive cytoreductive surgery and blood transfusion are more likely to have a stoma. Only 25% undergo stoma reversal, highlighting the importance of preoperative counselling.
Keywords: Stomas, Peritoneal carcinomatosis, Cytoreductive surgery, HIPEC, Intraperitoneal chemotherapy
THE EUROPEAN SOCIETY OF MEDICINE
Medical Research Archives, Volume 14 Issue 4
Background
Since the 1980s, studies on cytoreductive surgery (CRS) followed by hyperthermic intraperitoneal chemotherapy (HIPEC) have prompted a new treatment option for peritoneal carcinomatosis of several malignancies, including colorectal, appendiceal, ovarian, among others. Today, this multimodal approach is able to achieve long-term survival in select patients and has acceptable morbidity and mortality. Nonetheless, CRS with HIPEC is still considered a complex and high-risk procedure. This extensive surgery often requires multiple bowel resections and anastomoses in order to achieve complete cytoreduction (CC-0, CC-1), resulting in high complication rates. When a concomitant resection is performed, a stoma might be employed in an attempt to mitigate against anastomotic leakage or at least its major adverse sequelae, and a diverting loop ileostomy has been recommended in this setting. In one series, loop ileostomies were almost always reversed, whereas non-loop ileostomies were almost always permanent. Additionally, stoma reversal adds the additional morbidity associated with a future operation.
Predicting factors for stoma formation has been assessed by comparing patients who underwent stoma formation to those who did not. Creation of a stoma during CRS/HIPEC has been correlated with a higher peritoneal carcinomatosis index (PCI) score, larger number of organs resected, greater number of anastomoses, prolonged operative time (OT), and longer hospital stay (LOS). In fact, in procedures requiring >2 anastomoses, formation of a stoma reduced the anastomotic leak (AL) rate, morbidity, and reoperation rate, therefore, a protective diverting loop ileostomy has been previously recommended for extensive CRS/HIPEC procedures. Analyzing the various factors leading to stoma formation in this setting and the short-term outcome of this group of patients may improve both preoperative assessment and intraoperative decisions.
The primary aim of this study was to evaluate factors regarding the decision-making process and outcomes of performing a stoma during CRS and HIPEC for colorectal and appendiceal tumors and to examine whether fecal diversion reduces postoperative morbidity.
Materials and Methods
STUDY POPULATION
A retrospective analysis of an IRB-approved prospective registry was performed. All patients >18 years of age who underwent CRS and HIPEC for appendiceal and CRC between November 2009 and February 2018 at our institution were included. Patients were divided into two groups: those with and those without a stoma. A protective stoma was defined as any stoma with at least one distal anastomosis. The two groups were compared for demographics, preoperative baseline characteristics, operative details, and postoperative outcomes. This retrospective study was approved by the Institutional Review Board.
DATA COLLECTION
Patient demographics including age, gender, body mass index (BMI), albumin level, preoperative carcinoembryonic antigen (CEA), tumor location, and neoadjuvant chemotherapy were retrieved from the patient’s medical record. Peritoneal cancer index (PCI), intraoperative complications, estimated blood loss (EBL), major cytoreductive surgery, small bowel resection, multivisceral resection, type of anastomosis, and type of stoma creation were obtained from the operative report. Outcome measures including length of hospital stay (LOS), overall and specific complications, reoperation, pathology, residual disease, and mortality were obtained from the patient’s medical record. Complications included ileus, small bowel obstruction (SBO), abscess, surgical site infection (SSI), anastomotic leak, enterocutaneous fistula, perforation, pulmonary edema, and blood transfusion. Ileus was defined as a failure to pass gas or stool or the inability to tolerate a diet at postoperative day four or later. SBO was defined as any of the above-described symptoms with radiologic confirmation of mechanical obstruction. Abscess was confirmed by radiologic imaging and anastomotic leak was defined as any disruption of the anastomosis proven by radiology at reoperation. Morbidity was graded according to the Clavien–Dindo (CD) classification: Grades I–II were considered minor and grades III–V were considered major.
SURGICAL TECHNIQUE
The abdominal cavity was evaluated as to establish the extent of the peritoneal spread using the PCI score, as described by Sugarbaker. Lesions were resected by sharp dissection or ablation using a variety of thermal methods (cautery, bipolar, or argon beam). The abdominal cavity was carefully inspected for peritoneal carcinomatosis in all quadrants, diaphragm, on the surface of the small bowel, lesions on the serosal surface of the small bowel mesentery, and in the pelvis, after which surgery was initiated. Complete omentectomy was performed, as was additional organ resection when indicated. Following irrigation, the HIPEC cannulas were placed, after which the skin was closed with a watertight seal. After filling the abdomen with 3 L of sterile lactated Ringer’s, HIPEC was undertaken with 40 mg/m2 of mitomycin C (MMC) circulated at 42-43 degrees Celsius for 60-110 minutes with a perfusion flow rate of 1000 mL/min. At the completion of HIPEC, irrigation of the abdominal cavity, removal of the inflow and outflow cannulas, reintroduction of trocars, and further suction of fluid was undertaken after which the anastomoses and/or stoma formation were performed. Assessment of the CC score was performed according to the residual tumor size.
STATISTICAL ANALYSIS
Statistical analyses were performed using SPSS 24.0 software. Simple descriptive analyses were performed including mean and standard deviation (SD) for normally distributed factors. Univariate analysis comparing patients with stoma and without stoma were undertaken using the cross-table Pearson χ2 test or Fisher exact test, when appropriate, was used for categorical factors, while the Student’s t-test was applied for continuous factors. In order to assess the impact of stoma creation at the HIPEC surgery setting among other perioperative factors, we performed a multivariate regression analysis to the preoperative and intraoperative factors statistically significant after univariate analysis. Stoma reversal analysis was calculated using the Fischer’s exact test. Survival probabilities were calculated using the Kaplan–Meier method. p value < 0.05 was considered statistically significant.
Results
PATIENTS
A total of 110 patients underwent CRS/HIPEC for colorectal and appendiceal neoplasms; 32 (29.1%) with stoma and 78 (70.9%) without stoma (Figure 1). Mean age for patients with stoma was 53.3 ± 13.3; 16.4% were female versus 12.7% males (p = 0.114). Three types of stomas were performed: 15 (46.9%) loop ileostomies, 11 (34.4%) end ileostomies, and 6 (18.7%) end colostomies. In 18/110 (16.4%) patients, the ileostomy was diverting a colorectal or small bowel anastomosis. Preoperative factors associated with stoma creation are shown in Table 1 and included rectal tumor (21.9% vs. 7.7%, p = 0.031), body mass index (BMI) < 30 (81.3% vs. 58.4%, p = 0.023), hypoalbuminemia (12.5% vs. 2.6%, p = 0.036), carcinoembryonic antigen (CEA) (67.8 ± 241.2 vs. 17.6 ± 49.1, p = 0.021), and neoadjuvant chemotherapy (78.1% vs. 57.7%, p = 0.043).
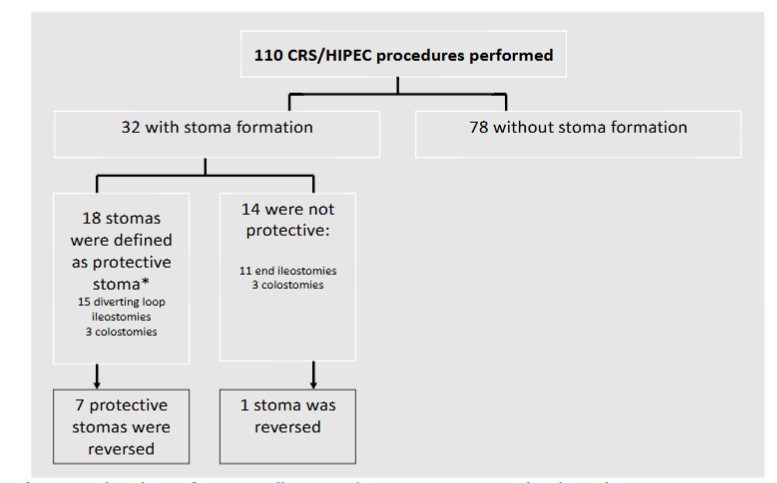
Table 1. Univariate analysis of perioperative factors associated with stoma creation at cytoreductive surgery and hyperthermic intraperitoneal chemotherapy procedure
| Variable | Stoma N = 32 | No stoma N = 78 | P value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 53.3 ± 13.3 | 55.8 ± 11.3 | 0.315 | |
| Male, n (%) | 14 (12.7) | 47 (42.7) | 0.114 | |
| BMI ≥ 30 (kg/m²), n (%) | 6 (18.7) | 32 (41.0) | 0.023 | |
| Albumin < 3.5 gr/dL, n (%) | 4 (12.5) | 2 (2.6) | 0.036 | |
| Preoperative CEA, mean ± SD | 67.8 ± 241.2 | 17.6 ± 49.1 | 0.021 | |
| Preoperative chemotherapy, n (%) | 25 (78.1) | 45 (57.7) | 0.043 | |
| Colorectal location, n (%) | – Right colon | 6 (18.7) | 25 (32.0) | 0.031 |
| – Left colon | 0 (0) | 1 (1.3) | ||
| – Sigmoid colon | 8 (25.0) | 6 (7.7) | ||
| – Rectum | 7 (21.9) | 6 (7.7) | ||
| PCI ≥ 10, n (%) | 19 (59.4) | 23 (29.5) | 0.002 | |
| EBL (cc), mean ± SD | 662.5 ± 687.4 | 250.0 ± 305.6 | 0.000 | |
| Major CRS, n (%) | 28 (87.5) | 25 (32.0) | 0.000 | |
| Multivisceral resection, n (%) | 19 (59.4) | 20 (25.6) | 0.000 | |
| Small bowel resection, n (%) | 23 (71.9) | 27 (34.6) | 0.000 | |
| Resection with hypaque, n (%) | 27 (84.4) | 30 (38.5) | 0.000 |
Results
SURGERY PARAMETERS
The intraoperative factors that significantly led to more stoma formation were peritoneal cancer index (PCI) ≥ 10 (59.4% vs. 29.5%, p = 0.002), a more extensive cytoreductive surgery (CRS) (87.5% vs. 32%, p < 0.001), residual disease (50% vs. 20.5%, p = 0.002), a higher estimated blood loss (EBL) (662.5 ± 687.4 vs. 250.0 ± 305.6, p < 0.001), more red blood cells (RBC) transfusions (43.7% vs. 11.5%, p < 0.001), multiple small bowel resections (71.9% vs. 34.6%, p < 0.001), and multivisceral resections (59.4% vs. 25.6%, p < 0.001).
POSTOPERATIVE OUTCOMES
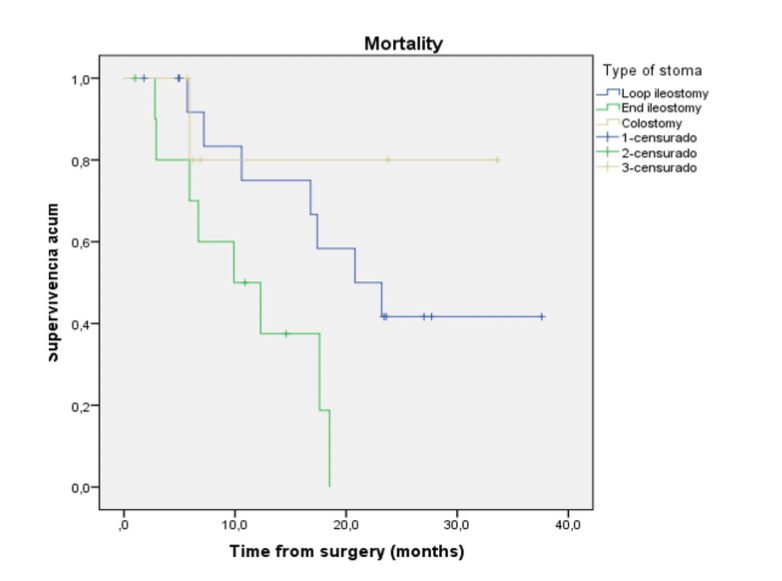
The incidence of complications was 56.2% in patients with stoma versus 52.6% in those without stoma (p = 0.7). Patients with stomas had significantly more surgical site infections (25% vs. 6.4%, p = 0.006), severity of morbidity (Clavien-Dindo class 3 and 4: 25% vs. 7.7%, 21.9% vs. 7.7%, respectively, p = 0.017), longer hospitalization (10.5 ± 4.6 vs. 7.1 ± 3.7, p = 0.028), higher reoperation rate (12.5% vs. 1.3%, p = 0.010) and mortality (50% vs. 20.5%, p < 0.002). Among diverted patients, 7 had dehydration, 3 had small bowel obstruction, one intraabdominal abscess, and one pulmonary complication. All patients with anastomotic leak (AL) were non-stoma patients. Eight of 32 patients (25%) underwent stoma reversal, one by laparotomy. The mean time to stoma closure was 5.3 ±2.8 months with a morbidity rate of 4.5%. As noted in Table 2, multivariate analysis among perioperative factors, multiple small bowel resections and multivisceral resections were significantly associated with stoma creation. Figure 2 demonstrates Kaplan-Meier curves of overall survival (OS) after CRS/HIPEC for appendiceal and colorectal cancer based on stoma and no stoma patients. Stoma patients had more mortality at 12 months (40% vs. 20%, p < 0.001). OS after CRS/HIPEC based on end ileostomy, loop ileostomy, and colostomy creation was 38%, 75%, and 80%, respectively (p < 0.029) as noted in Figure 3.
Table 2. Multivariate analysis of perioperative factors associated with stoma formation at cytoreductive surgery and hyperthermic intraperitoneal chemotherapy
| Prognostic factor | OR | Lower 95%CI | Upper 95%CI | P value |
|---|---|---|---|---|
| BMI > 30 kg/m2 | 1.136 | 0.089 | 1.153 | 0.082 |
| Albumin <3.5 gr/dL | 1.471 | 0.459 | 41.322 | 0.200 |
| Preoperative chemotherapy | 0.358 | 0.360 | 5.682 | 0.611 |
| PCI >10 | 0.696 | 0.617 | 6.526 | 0.247 |
| EBL | 0.001 | 0.999 | 1.002 | 0.239 |
Figure 2
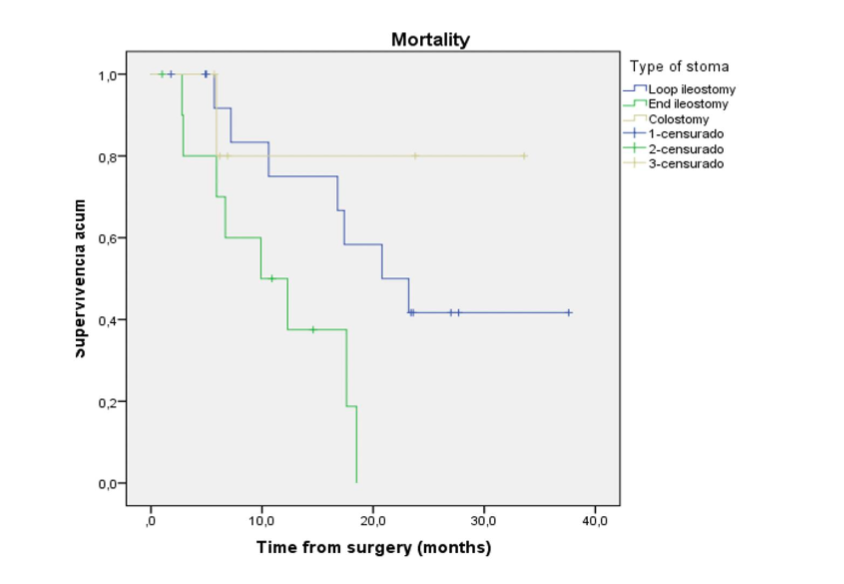
Figure 3
Discussion
Peritoneal carcinomatosis of gastrointestinal primary origin has been considered a fatal clinical entity to be treated palliatively in the past 40 years. Currently, the development of surgical techniques such as CRS/HIPEC have provided new hope for a potential increase in overall survival in select patients. Although CRS/HIPEC is still considered a complex and high-risk procedure, it is associated with an acceptable morbidity and mortality. Achieving complete cytoreduction (CC-0, CC-1) is crucial as it has been shown to correlate with prognosis.
Formation of stoma via diverting loop ileostomy or colostomy as part of CRS/HIPEC is a technique frequently used to protect a high-risk anastomosis and may be an effective tool in reducing leaks, thus decreasing the postoperative morbidity. In the past, colorectal anastomoses required a diverting ileostomy in 50% of these patients, and its incidence was reduced to 7%. In our series, we identified 29.1% of patients with stoma formation, higher than some studies in the literature at 17% and 4.8%, but in keeping with what other authors have described. The majority of stoma patients in our study had rectosigmoid colon resection (46.9%) with ileorectal, colorectal or coloanal anastomoses. The majority of our patients with right colon or appendiceal neoplasms underwent CRS/HIPEC with ileocolic anastomosis and no diversion, similar to what other studies have described.
In pelvic cytoreduction with rectal resection, the resection margin usually is just below the peritoneal surface; therefore, rectal resections in CRS/HIPEC are more likely high anterior resection than low anterior resections. With this in mind, a colostomy may not be necessary in all cases. In our study, we identified 18.7% of colostomies, lower than previously published (21%). Loop ileostomy was 46.9%, also lower than other studies (67%) and end ileostomy 34.4%, higher than other studies (12%). Verwaal et al. performed a protective colostomy in 42% of their patients, but complications occurred in almost 18% of them despite the stoma. Furthermore, Sugarbaker suggested that preservation of a 10–15 cm length of rectum allows a two-layered anastomosis which may reduce the need for diverting ileostomy in patients who undergo CRS and HIPEC.
In the current series, preoperative factors significantly associated with stoma formation included rectal tumor (21.9%), non-obese patients (BMI <30), malnutrition defined as hypoalbuminemia (albumin <3.5 gr/dL), higher CEA, and neoadjuvant chemotherapy. Even though a defunctioning stoma is feasible in most cases, it may be difficult in edematous small bowel after a prolonged procedure such as CRS/HIPEC or in obese patients. Although patients with stoma were slightly younger than patients without stoma, and they are more likely to be female, it was not statistically significant as other authors have reported.
On univariate analysis we found that operations with stoma formation were more extensive. In fact, procedures requiring two or more number of anastomoses, formation of stoma reduced the anastomotic leak (AL) rate, the morbidity, and reoperation rate, therefore, protective diverting loop ileostomy should be considered in extensive CRS/HIPEC procedures. In our study, patients with PCI ≥ 10, greater cytoreduction, residual disease (CC-2, CC-3), a higher estimated blood loss (EBL), more red blood cells (RBC) transfusions, multiple small bowel resections, multivisceral resections, and re-do anastomosis were intraoperative factors that significantly led to more stoma formation. This finding is in keeping with other reports; however, prolonged operative time (OT) was not correlated and it is similar for both groups as seen in another report. On multivariate logistic regression analysis among perioperative factors, multiple small bowel resections and multivisceral resections are significant factors predicting stoma formation. Our findings also raise the question of the exact impact of organs resection on patient outcome. Otherwise, a study regarding this issue showed that PCI was the single most dominant factor for stoma formation.
Intuitively, patients with higher PCI undergo more extensive surgery (more bowel and solid organ resections) in order to render the patient CC-0 status, and thus these patients are at higher risk of complications. In the present study, the incidence of complications was slightly higher among patients who required stoma, although it was not statistically significant. Overall, AL occurred in 3 cases (2.7%) which is lower than other reported series (7.5%-12.3). CRS with HIPEC can take up to 12 hours and frequently requires large-volume resuscitation during and after the operation. After CRS and HIPEC, patients often have significant fluid shifts, development of pleural effusions, and requirement of peritoneal drains.
Nonetheless, within the body of CRS and HIPEC literature, the anastomotic leak rate is reported to be as high as 10%, but most of the studies included all intestinal anastomoses and did not focus on high-risk pelvic anastomoses. Our patients with stomas had significantly more intra-abdominal abscess and surgical site infections, as well as higher severity of morbidity (Clavien-Dindo class 3 and 4) and reoperation rate. Surprisingly, postoperative ileus was not significantly lower for stoma patients. Patients in the present series received a mitomycin C-based regimen for HIPEC, and the literature contains evidence that intraperitoneal administration of this drug may reduce postoperative adhesion formation. Conversely, a 1996 study by Jacquet and Sugarbaker showed increased intraabdominal adhesions after intraperitoneal chemotherapy with mitomycin C. Consequently, we assume that the difference in stoma-related morbidity rate is attributable to higher volume of disease in the stoma group that required multiple organs resections and GI anastomoses, and not to the creation of the stoma itself. Previous studies on extreme CRS/HIPEC (defined as either resection of ≥5 organs or ≥3 bowel anastomoses) showed that extensive CRS/HIPEC procedures are associated with higher major morbidity, including greater rate of intra-abdominal abscess/leak, and inferior oncological outcomes, whereas other studies have shown lower rate of severe morbidity (41 vs. 6%) and lower reoperation rate (28 vs. 0%) for patients who underwent stoma creation. Unlike our study, other reports established that loop ileostomy may be omitted for patients with low risk for AL after colorectal resection in experienced centers with adequate postoperative care, possibilities for postoperative assessment and radiological intervention to avoid stoma-related complications and increase the quality of life of patients with peritoneal metastases.
Overall, 8 of our patients (25%) underwent stoma reversal, which is not on par with previous studies reporting stoma closure rates of approximately 70% for colorectal cancer. However, other studies of CRS and HIPEC patients have reported lower rates of stoma reversal although still higher than ours (44%). They grouped both loop and end stomas (colostomy and ileostomy) together, which likely explains the low reported closure rates. Only one bowel continuity restored required a laparotomy for reversal due to dense adhesions, much lower than 18% of previous publications. Among patients with stoma reversal, only one was non-loop ileostomy and 5 of whom had complications treated non-operatively; four patients had postoperative ileus, one patient fistula, and anastomotic leak rate of 0% after ileostomy closure, lower than other publications, reporting a morbidity rate for stoma reversal up to 50% which is similar to other publications. Overall morbidity rate of stoma reversal was 4.5%, more than 1.6% reported by other authors. No patients died due to stoma reversal, whereas other authors reported a 30-day mortality rate of 4.7%. Avoiding excess of intestinal discontinuity, mean time to stoma closure in our series was 23 weeks, which is similar to what other authors have reported. As expected, factors to avoid stoma reversal were formation of non-loop ileostomy and evidence of disease progression.
This study has some limitation including its retrospective nature and the heterogeneity of the pathology/location. In addition, these patients were treated at a high-volume center with quaternary ancillary services, which leads to better resolution of complications and makes the results less generalizable with other lower volume centers.
Conclusions
Patients with appendiceal or colorectal neoplasms with higher carcinomatosis burden requiring major cytoreductive surgery and RBC transfusion are more likely to have stoma constructed in CRS/HIPEC procedure. Only one quarter of the patients with a diverting ileostomy in this study had bowel continuity restored within 6 months after their index operation highlighting the importance of preoperative counselling. Diverting ileostomy reversal required a laparotomy in one case due to dense adhesions and had an associated overall morbidity rate of 4.5%. The use of protective stoma should be considered in extensive CRS/HIPEC procedures requiring multiple bowel resections although additional studies are needed to evaluate risk factors for anastomotic leak.
Poster presentation at the annual meeting of the American Society of Colon and Rectal Surgeons, June 1-5, 2019, Cleveland, OH
Podium presentation at the International Colorectal Disease Symposium, February 25-28,2020, Jerusalem, Israel
Funding: None
Disclosures: Drs. Moreno Djadou, Poh, Yellinek, Fayazzadeh, El-Hayek, Simpfendorfer and Dasilva have not disclosures. Dr. Wexner receives consulting fees from ICON Language Services, Intuitive Surgical, Stryker, Medtronic, Takeda, ARC / Corvus, Astellas, Baxter, Olympus, AISChannel, Livsmed, GI Supply, and Leading BioSciences; stock options from Regentys, LifeBond, Pragma /GibLib, and Renew Medical; and royalties from Medtronic, Intuitive Surgical, Karl Storz Endoscopy America Inc, and Unique Surgical Innovations LLC.
References
- Sugarbaker PH, Van der Speeten K. Surgical technology and pharmacology of hyperthermic perioperative chemotherapy. J Gastrointest Oncol. 2016;7(1):29-44.
- Elias D, Lefevre JH, Chevalier J, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. J Clin Oncol. 2009;27(5):681-685.
- Cao C, Yan TD, Black D, Morris DL. A systematic review and meta-analysis of cytoreductive surgery with perioperative intraperitoneal chemotherapy for peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol. 2009;16(8):2152-2165.
- Glehen O, Gilly FN, Boutitie F, et al. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy: a multi-institutional study of 1,290 patients. Cancer. 2010;116(24):5608-5618.
- Cortes-Guiral D, Elias D, Cascales-Campos PA, et al. Second-look surgery plus hyperthermic intraperitoneal chemotherapy for patients with colorectal cancer at high risk of peritoneal carcinomatosis: Does it really save lives? World J Gastroenterol. 2017;23(3):377-381
- Colombo N, Sessa C, du Bois A, Ledermann J, et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann Oncol. 2019;30(5):672-705.
- Goéré D, Passot G, Gelli M, Levine EA, Bartlett DL, Sugarbaker PH, Glehen O. Complete cytoreductive surgery plus HIPEC for peritoneal metastases from unusual cancer sites of origin: results from a worldwide analysis issue of the Peritoneal Surface Oncology Group International (PSOGI). Int J Hyperthermia. 2017;33(5):520-527.
- Chouliaras K, Levine EA, Fino N, Shen P, Votanopoulos KI. Prognostic Factors and Significance of Gastrointestinal Leak After Cytoreductive Surgery (CRS) with Heated Intraperitoneal Chemotherapy (HIPEC). Ann Surg Oncol. 2017;24(4):890-897.
- Hübner M, Kusamura S, Villeneuve L, et al. Guidelines for Perioperative Care in Cytoreductive Surgery (CRS) with or without hyperthermic IntraPEritoneal chemotherapy (HIPEC): Enhanced Recovery After Surgery (ERAS®) Society Recommendations – Part II: Postoperative management and special considerations. Eur J Surg Oncol. 2020;46(12):2311-2323.
- Jacoby H, Berger Y, Barda L, Sharif N, Zager Y, Lebedyev A, Gutman M, Hoffman A. Implications of Stoma Formation as Part of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. World J Surg. 2018;42(7):2036-2042.
- Sugarbaker PH. Avoiding Diverting Ileostomy in Patients Requiring Complete Pelvic Peritonectomy. Ann Surg Oncol. 2016;23(5):1481-1485.
- Whealon MD, Gahagan JV, Sujatha-Bhaskar S, et al. Is Fecal Diversion Needed in Pelvic Anastomoses During Hyperthermic Intraperitoneal Chemotherapy (HIPEC)? Ann Surg Oncol. 2017;24(8):2122-2128.
- Pakraftar S, Ramalingam L, Shuai Y, et al, Choudry HA. Institutional Experience with Ostomies Created During Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemoperfusion. Ann Surg Oncol. 2017;24(13):3811-3817.
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-213.
- Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res. 1996;82:359-374.
- Sugarbaker PH. Management of peritoneal-surface malignancy: the surgeon’s role. Langenbecks Arch Surg. 1999;384(6):576-587.
- Brandl A, Raue W, Aigner F, Arroyave MC, Pratschke J, Rau B. Safety of extraperitoneal rectal resection and ileo- or colorectal anastomosis without loop ileostomy in patients with peritoneal metastases treated with CRS and HIPEC. Colorectal Dis. 2018 Jan 6. doi: 10.1111/codi.14004. Epub ahead of print. PMID: 29316159.
- Hamilton TD, Taylor EL, Cannell AJ, McCart JA, Govindarajan A. Impact of Major Complications on Patients’ Quality of Life After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann Surg Oncol. 2016;23(9):2946-2952.
- Riss S, Chandrakumaran K, Dayal S, Cecil TD, Mohamed F, Moran BJ. Risk of definitive stoma after surgery for peritoneal malignancy in 958 patients: comparative study between complete cytoreductive surgery and maximal tumor debulking. Eur J Surg Oncol. 2015;41(3):392-395.
- Jaehne J. Cytoreductive procedures-strategies to reduce postoperative morbidity and management of surgical complications with special emphasis on anastomotic leaks. J Surg Oncol. 2009;100(4):302-305.
- Verwaal VJ, van Tinteren H, Ruth SV, Zoetmulder FA. Toxicity of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. J Surg Oncol. 2004;85(2):61-67.
- Doud AN, Levine EA, Fino NF, Stewart JH, Shen P, Votanopoulos KI. Stoma Creation and Reversal After Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy. Ann Surg Oncol. 2016;23(2):503-510.
- Lee L, Alie-Cusson F, Dubé P, Sideris L. Postoperative complications affect long-term outcomes after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for colorectal peritoneal carcinomatosis. J Surg Oncol. 2017;116(2):236-243.
- Casado-Adam A, Alderman R, Stuart OA, Chang D, Sugarbaker PH. Gastrointestinal complications in 147 consecutive patients with peritoneal surface malignancy treated by cytoreductive surgery and perioperative intraperitoneal chemotherapy. Int J Surg Oncol. 2011;2011:468698. doi: 10.1155/2011/468698. Epub 2011 Oct 16.
- Jacquet P, Stephens AD, Averbach AM, et al. Analysis of morbidity and mortality in 60 patients with peritoneal carcinomatosis treated by cytoreductive surgery and heated intraoperative intraperitoneal chemotherapy. Cancer. 1996;77(12):2622-2629.
- Liu Y, Li H, Shu XZ, Gray SD, Prestwich GD. Crosslinked hyaluronan hydrogels containing mitomycin C reduce postoperative abdominal adhesions. Fertil Steril. 2005;83 Suppl 1:1275-1283.
- Jacquet P, Sugarbaker PH. Effects of postoperative intraperitoneal chemotherapy on peritoneal wound healing and adhesion formation. Cancer Treat Res. 1996;82:327-335.
- Waterland P, Goonetilleke K, Naumann DN, Sutcliff M, Soliman F. Defunctioning Ileostomy Reversal Rates and Reasons for Delayed Reversal: Does Delay Impact on Complications of Ileostomy Reversal? A Study of 170 Defunctioning Ileostomies. J Clin Med Res. 2015;7(9):685-689.
- de Cuba EM, Verwaal VJ, de Hingh IH, et al. Morbidity associated with colostomy reversal after cytoreductive surgery and HIPEC. Ann Surg Oncol. 2014;21(3):883-890.