

Surgical Approaches for Refractory Gluteus Medius Pathology
Contemporary Surgical Approaches for Refractory Gluteus Medius Pathology
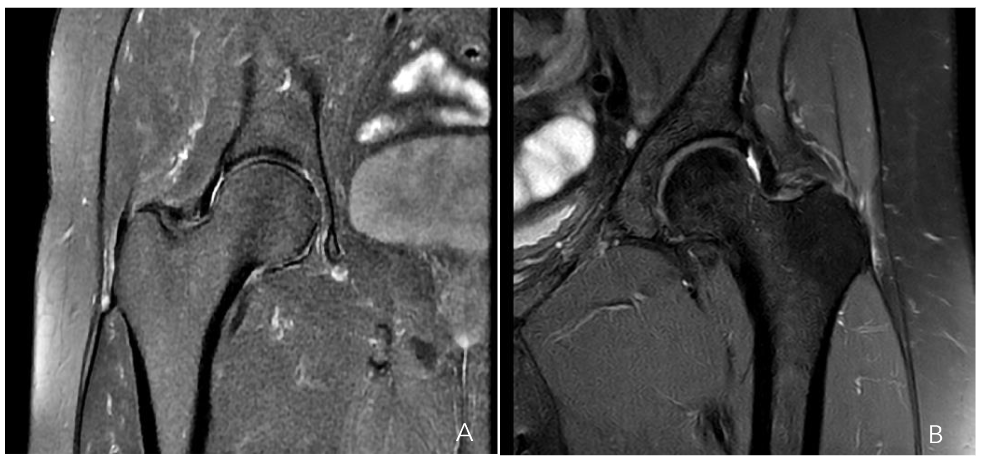


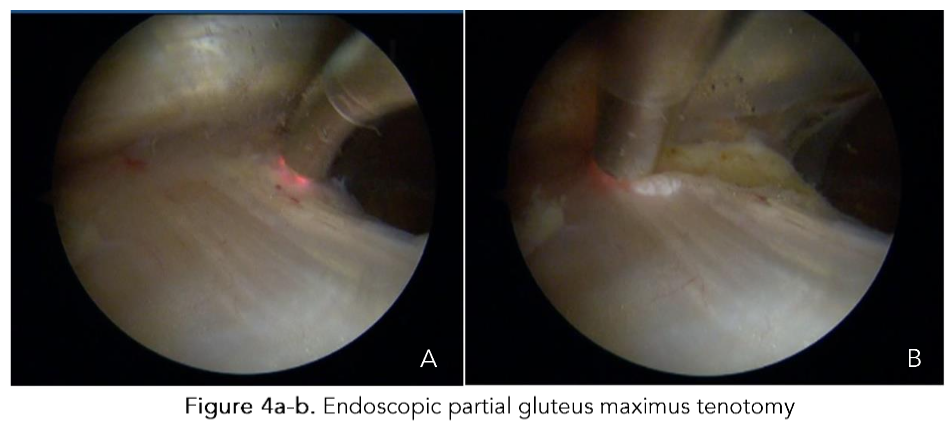
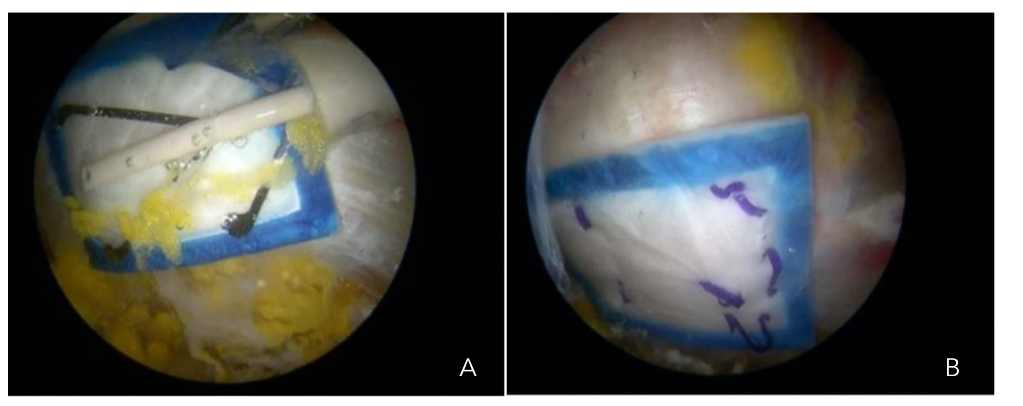
Figure 4a-b. Endoscopic partial gluteus maximus tenotomy
Given that this condition involves tendon insertion (enthesis) in an area with poor blood supply, we utilize the intermediate portal to perform transtendinous perforations in the degenerated tendon regions Figure 5. These perforations are directed towards the greater trochanter to encourage the development of new blood vessels and enhance blood flow, ultimately promoting healing of the lesion, indicating that this method has yielded exceptional results in both clinical evaluations and imaging examinations for partial tears of up to 25% of the total thickness, as illustrated in Figures 6a-b.
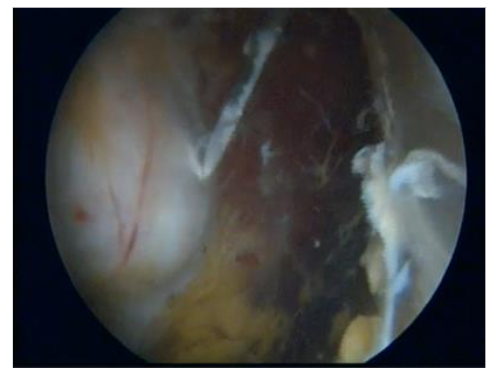
Figure 5. Endoscopic greater trochanter perforations
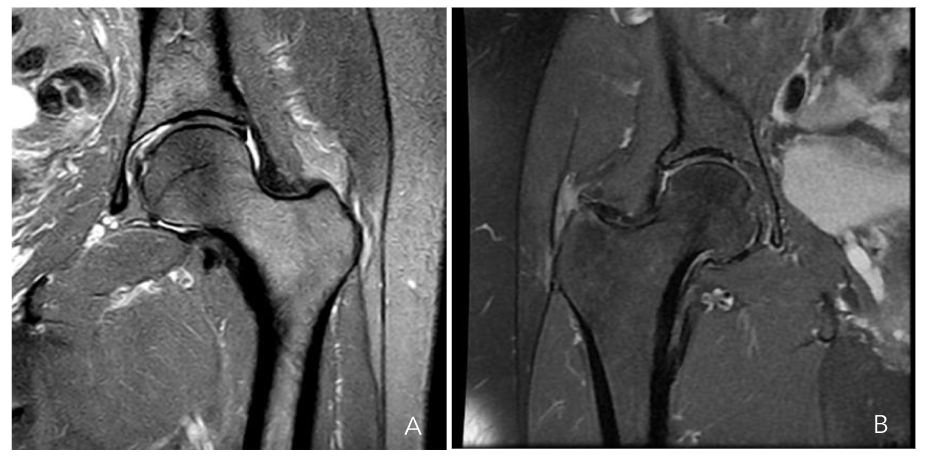
Figure 6a-b. Hip MRI scan showing a partial gluteus medius tear (a) and a gluteus minor tear (b)
The selection of an appropriate treatment modality becomes more complex when lesions affect between 25% and 50% of the thickness Figure 7. As previously noted, these lesions are situated medial to the gluteus medius tendon, demonstrating tendon continuity in the most lateral region. Direct repair of this lesion would require the disinsertion of a healthy gluteus medius tendon, which is suboptimal. Cutting one healthy tendon to repair another would, at best, result in scar tissue formation, which would not possess the same functionality as native tissue. Consequently, in this subset of lesions, augmentation with a biological collagen patch is employed, in addition to the technique described for the two previous groups.
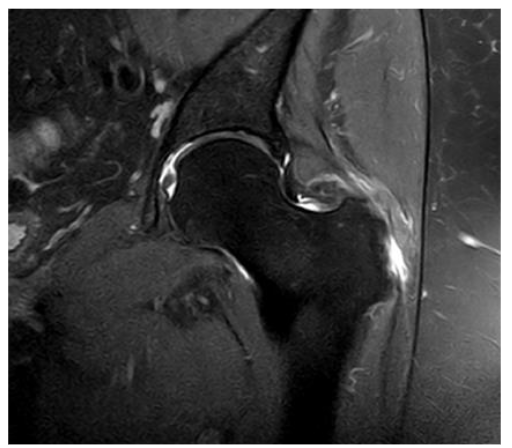
Figure 7. Hip MRI scan showing a 30% rupture of the gluteus medius and minor tendons
This patch stimulates tissue regeneration, promoting collagen deposition and enhancing the recovery of the gluteus minimus tendon Figure 8a-b. We have achieved favorable outcomes with this technique, which we published in 2024³⁴⁴. The REGENETEN® bioinductive patch (Smith & Nephew) is a highly porous type 1 collagen implant with oriented fibers that stimulate and guide the body’s natural healing response. It supports new tendon growth by interrupting disease progression and promoting cell and blood vessel migration⁴⁵⁴⁷, ultimately resulting in increased tendon thickness.
Figures 8a-b. Endoscopic placement of a REGENETEN® bioinductive patch over the gluteus medius insertion
Our group conducted a prospective study by incorporating the REGENETEN® patch as a single augmentation technique from 2019 to 2024 with a minimum follow-up of 6 months⁴³. The study population comprised patients who underwent hip surgery for tendinopathy refractory to conservative treatment, defined as failure to respond to NSAIDs, three courses of physiotherapy, and a symptom duration exceeding 6 months. In patients with a symptom duration of less than 6 months, surgical intervention was indicated in the presence of 30% to 50% rupture of the gluteus medius minimus tendon complex. All patients underwent preoperative MRI, which was subsequently compared with imaging performed 6 months postoperatively, demonstrating complete healing of the tendon.
Surgical technique
The procedure is conducted on an outpatient basis for all patients utilizing an anesthetic protocol comprising epidural block with sedation, and prophylactic antibiotics administered 30 minutes prior to the start of the surgical procedure. The patient is positioned in the supine decubitus position, with the ipsilateral leg in the surgical field, facilitating abduction, adduction, internal and external rotations, as well as hip flexion and extension movements.
Subsequently, the portals for surgical access are determined through individualized measurements for each patient. Initially, the width of the femur is outlined with a sterile marker at the level of the most lateral prominence of the greater trochanter, which is projected proximally and distally, in the posterior third of the femur (proximal posterolateral accessory portal (PPLA), and distal posterolateral accessory portal (DPLA). Finally, a posterior accessory portal is utilized at the level of the most lateral portion of the greater trochanter using half of the previously defined measurement⁴².
The initial portal established is the DPLA, which is utilized to access the virtual space between the vastus lateralis and the iliotibial band. This space is distended using normal saline solution (NSS) with epinephrine at a concentration of 1 mg per 3 liters of NSS, maintained at a temperature of 30°C⁴⁸. The PPLA is subsequently established utilizing a guide wire under direct visualization with a 70° optic through the DPLA portal. A bursectomy and resection of fibrous bands are performed to identify the gluteus maximus as a landmark. A partial tenotomy of the proximal portion of the distal insertion of the gluteus maximus, approximately 3 cm in length, is executed, which enhances the working space and reduces pressure in the lateral compartment⁴⁹. The proximal end of the greater trochanter and the gluteus medius tendon are identified, and tendon lesions are examined. Subsequently, the greater trochanter is drilled in the areas of gluteus medius tendon degeneration utilizing a 2.3 mm drill through the PPLA.
In patients previously identified with lesions exceeding 30%, the bio-inductive collagen patch is applied after the perforations through the DPLA, which is secured with resorbable anchors through the PPLA, with the arthroscopic lens positioned in the PPLA. Internal and external rotation maneuvers are executed to facilitate perforations, placement, and fixation of the collagen inductive patch. The stability of the fixation is evaluated by conducting flexion and extension, abduction and adduction movements, and rotational movements.
Complete rupture of the gluteus medius tendon presents a significant challenge for surgeons, as the tendon has been displaced from its anatomical position in the greater trochanter, which is typically sclerotic and is associated with a tendon of poor quality. Poor outcomes have been reported with conventional open surgical treatments in such cases. Consequently, we have developed an endoscopic surgical technique, as described for partial tendon lesions, with the notable distinction that in these cases it is crucial to examine the continuity of the tendon with the bone tissue and assess its adherence or detachment. If the tendon is detached, it must be incised longitudinally to identify the sclerotic zone of the bone at the greater trochanter, which is then removed, typically with a 5.5 mm burr drill, to create a bleeding bed where the tendon can heal. The tendon is subsequently fixed with one or two 5.5 mm titanium anchors loaded with double sutures to close the incision and secure the tendon to the bleeding bed of the greater trochanter Figure 9a-c and 10a-d.
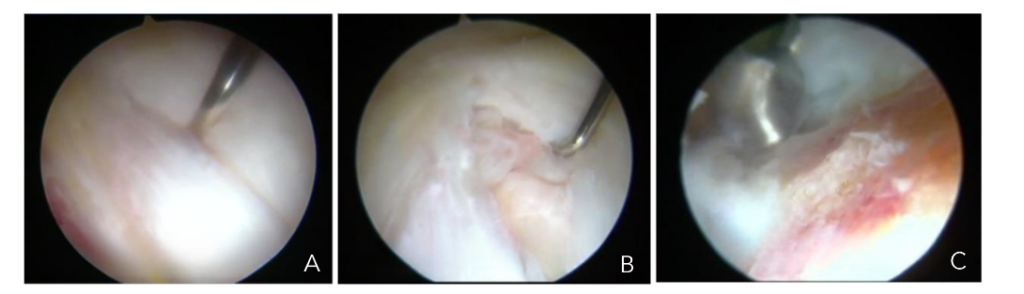
Figures 9a-c. Endoscopic view of a longitudinal incision of the gluteus medius tendon (A), exposure of sclerotic bone beneath the tendon (B), bone bed preparation under tendon (C).
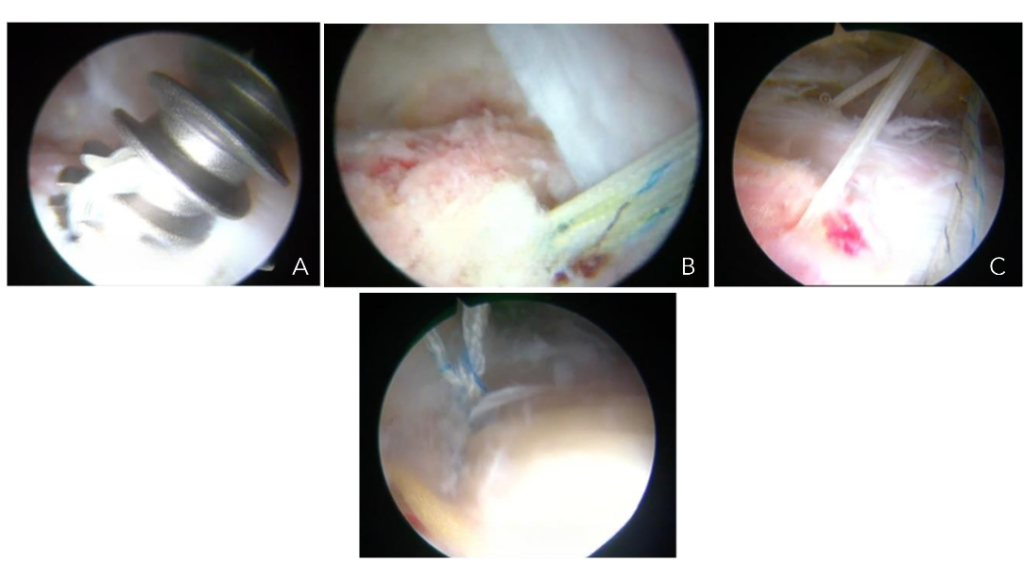
Figures 10a-d. Endoscopic view of a gluteus medius tear repair. Placement of a titanium anchor (A) Anchor in bone with sutures (B). Anchor sutures through tendon closing longitudinal incision/ tear (C). Final suture-anchor construct (D).
References
1. Antonio S, Wolfgang G, Robert H, Fullerton B, Carla S. The anatomical and functional relation between gluteus maximus and fascia lata. Journal of Bodywork and Movement Therapies. 2013;17 (4):512-517. doi:10.1016/j.jbmt.2013.04.004
2. Tsutsumi M, Nimura A, Akita K. The Gluteus Medius Tendon and Its Insertion Sites: An Anatomical Study with Possible Implications for Gluteus Medius Tears. J Bone Joint Surg Am. 2019;101(2):177-184. doi:10.2106/JBJS.18.00602
3. Lequesne M, Mathieu P, Vuillemin-Bodaghi V, Bard H, Djian P. Gluteal tendinopathy in refractory greater trochanter pain syndrome: diagnostic value of two clinical tests. Arthritis Rheum. 2008;59(2): 241-246. doi:10.1002/art.23354
4. Thomassen PJB, Basso T, Foss OA. Endoscopic Treatment of Greater Trochanteric Pain Syndrome – A Case Series of 11 Patients. J Orthop Case Rep. 2019;9(1):6-10. doi:10.13107/jocr.2250-0685.1284
5. Williams BS, Cohen SP. Greater trochanteric pain syndrome: a review of anatomy, diagnosis and treatment. Anesth Analg. 2009;108(5):1662-1670. doi:10.1213/ane.0b013e31819d6562
6. Cormier G, Berthelot JM, Maugars Y; SRO (Société de Rhumatologie de l’Ouest). Gluteus tendon rupture is underrecognized by French orthopedic surgeons: results of a mail survey. Joint Bone Spine. 2006;73(4):411-413. doi:10.1016/j.jbs pin.2006.01.021
7. Lachiewicz PF. Abductor tendon tears of the hip: evaluation and management. J Am Acad Orthop Surg. 2011;19(7):385-391. doi:10.5435/00 124635-201107000-00001
8. LaPorte C, Vasaris M, Gossett L, Boykin R, Menge T. Gluteus medius tears of the hip: a comprehensive approach. Phys Sportsmed. 2019;47 (1):15-20. doi:10.1080/00913847.2018.1527172
9. Lindner D, Shohat N, Botser I, Agar G, Domb BG. Clinical presentation and imaging results of patients with symptomatic gluteus medius tears. J Hip Preserv Surg. 2015;2(3):310-315. Published 2015 May 19. doi:10.1093/jhps/hnv035
10. Ganderton C, Semciw A, Cook J, Pizzari T. Demystifying the Clinical Diagnosis of Greater Trochanteric Pain Syndrome in Women. J Womens Health (Larchmt). 2017;26(6):633-643. doi:10.1089/j wh.2016.5889
11. Long SS, Surrey DE, Nazarian LN. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. AJR Am J Roentgenol. 2013; 201(5):1083-1086. doi:10.2214/AJR.12.10038
12. Ramírez J, Pomés I, Sobrino-Guijarro B, Pomés J, Sanmartí R, Cañete JD. Ultrasound evaluation of greater trochanter pain syndrome in patients with spondyloarthritis: are there any specific features?. Rheumatol Int. 2014;34(7):947-952. doi:10.1007/s00296-014-2947-9
13. Redmond JM, Chen AW, Domb BG. Greater Trochanteric Pain Syndrome. J Am Acad Orthop Surg. 2016;24(4):231-240. doi:10.5435/JAAOS-D-14-00406
14. Meghpara MB, Bheem R, Shah S, et al. Prevalence of Gluteus Medius Pathology on Magnetic Resonance Imaging in Patients Undergoing Hip Arthroscopy for Femoroacetabular Impingement: Asymptomatic Tears Are Rare, Whereas Tendinosis Is Common. Am J Sports Med. 2020;48(12):2933-2938. doi:10.1177/0363546520952766
15. Cvitanic O, Henzie G, Skezas N, Lyons J, Minter J. MRI diagnosis of tears of the hip abductor tendons (gluteus medius and gluteus minimus). AJR Am J Roentgenol. 2004;182(1):137-143. doi:10.2214/ajr.182.1.1820137
16. Christofilopoulos P, Kenanidis E, Bartolone P, Poultsides L, Tsiridis E, Kyriakopoulos G. Gluteus maximus tendon transfer for chronic abductor insufficiency: the Geneva technique. Hip Int. 2021; 31(6):751-758. doi:10.1177/1120700020924330
17. Robertson WJ, Gardner MJ, Barker JU, Boraiah S, Lorich DG, Kelly BT. Anatomy and dimensions of the gluteus medius tendon insertion. Arthroscopy. 2008;24(2):130-136. doi:10.1016/j.arthro.2007.11.015
18. Kenanidis E, Kyriakopoulos G, Kaila R, Christofilopoulos P. Lesions of the abductors in the hip. EFORT Open Rev. 2020;5(8):464-476. Published 2020 Sep 10. doi:10.1302/2058-5241.5.190094
19. Ebert JR, Bucher TA, Ball SV, Janes GC. A review of surgical repair methods and patient outcomes for gluteal tendon tears. Hip Int. 2015; 25(1):15-23. doi:10.5301/hipint.5000183
20. Moalli PA, Talarico LC, Sung VW, et al. Impact of menopause on collagen subtypes in the arcus tendineous fasciae pelvis.Am J Obstet Gynecol. 2004;190(3):620-627. doi:10.1016/j.ajog.2003.08.040
21. Greising SM, Baltgalvis KA, Lowe DA, Warren GL. Hormone therapy and skeletal muscle strength: a meta-analysis. J Gerontol A Biol Sci Med Sci. 2009; 64(10):1071-1081. doi:10.1093/gerona/glp082
22. Rosinsky PJ, Diulus SC, Walsh JP, et al. Development of a Predictive Algorithm for Symptomatic Hip Abductor Tears in Patients Undergoing Primary Hip Arthroscopy. Am J Sports Med. 2021;49(2):497-504. doi:10.1177/036354652 0980461
23. Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001;44(9):2138-2145. doi:10.1002/1529-0131(200109)44:9<2138::AID-ART367>3.0.CO;2-M
24. Guermazi A, Neogi T, Katz JN, et al. Intra-articular Corticosteroid Injections for the Treatment of Hip and Knee Osteoarthritis-related Pain: Considerations and Controversies with a Focus on Imaging-Radiology Scientific Expert Panel. Radiology. 2020;297(3):503-512. doi:10.1148/radiol.2020200771
25. Kong A, Van der Vliet A, Zadow S. MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome. Eur Radiol. 2007;17(7):1772-1783. doi:10.1007/s00330-006-0485-x
26. Pan J, Bredella MA. Imaging of soft tissue abnormalities about the hip. Radiol Clin North Am. 2013;51(3):353-369. doi:10.1016/j.rcl.2012.10.003
27. Woodley SJ, Nicholson HD, Livingstone V, et al. Lateral hip pain: findings from magnetic resonance imaging and clinical examination. J Orthop Sports Phys Ther. 2008;38(6):313-328. doi:10.2519/jospt.2 008.2685
28. Rice MW, Browning RB, Nho SJ. Surgical Treatment of Gluteus Medius Tears. Arthroscopy. 2022;38(7):2115-2117. doi:10.1016/j.arthro.2022.0 5.002
29. Longstaffe R, Dickerson P, Thigpen CA, et al. Both open and endoscopic gluteal tendon repairs lead to functional improvement with similar failure rates: a systematic review. J ISAKOS. 2021; 6(1):28-34. doi:10.1136/jisakos-2020-000474
30. Ebert JR, Jain M, Janes GC. Good clinical outcomes, a high level of patient satisfaction and an acceptable re-operation rate are observed 7-10 years after augmented hip abductor tendon repair. Knee Surg Sports Traumatol Arthrosc. 2023;31 (6):2131-2139. doi:10.1007/s00167-023-07382-3
31. Chandrasekaran S, Lodhia P, Gui C, Vemula SP, Martin TJ, Domb BG. Outcomes of Open Versus Endoscopic Repair of Abductor Muscle Tears of the Hip: A Systematic Review. Arthroscopy. 2015;31 (10):2057-67.e2. doi:10.1016/j.arthro.2015.03.042
32. Rai S, Jin S, Meng C, et al. Arthroscopic release using F and C method versus conventional open release method in the treatment of gluteal muscle contracture: a comparative study [published correction appears in BMC Musculoskelet Disord. 2018 Jun 7;19(1):187. doi: 10.1186/s12891-018-2119-2.]. BMC Musculoskelet Disord. 2017;18(1): 113. Published 2017 Mar 16. doi:10.1186/s12891-017-1484-6
33. Kenanidis E, Lund B, Christofilopoulos P. A roadmap to develop clinical guidelines for open surgery of acute and chronic tears of hip abductor tendons. Knee Surg Sports Traumatol Arthrosc Off J ESSKA. 2021;29(5):1420-31.
34. Widler KS, Glatthorn JF, Bizzini M, et al. Assessment of hip abductor muscle strength. A validity and reliability study. J Bone Joint Surg Am. 2009;91(11):2666-2672. doi:10.2106/JBJS.H.01119
35. Myers CA, Laz PJ, Shelburne KB, et al. Simulated hip abductor strengthening reduces peak joint contact forces in patients with total hip arthroplasty. J Biomech. 2019;93:18-27.
doi:10.1016/j.jbiomech.2019.06.003
36. Kahlenberg CA, Nwachukwu BU, Jahandar H, Meyers KN, Ranawat AS, Ranawat AS. Single- Versus Double-Row Repair of Hip Abductor Tears: A Biomechanical Matched Cadaver Study. Arthroscopy. 2019;35(3):818-823. doi:10.1016/j.arthro.2018.10.146
37. Whiteside LA, Roy ME. Incidence and treatment of abductor deficiency during total hip arthroplasty using the posterior approach: repair with direct suture technique and gluteus maximus flap transfer. Bone Joint J. 2019;101-B(6_Supple_B): 116-122. doi:10.1302/0301-620X.101B6.BJJ-2018-1511.R1
38. Howell GE, Biggs RE, Bourne RB. Prevalence of abductor mechanism tears of the hips in patients with osteoarthritis. J Arthroplasty. 2001;16(1):121-123. doi:10.1054/arth.2001.19158
39. Chandrasekaran S, Gui C, Hutchinson MR, Lodhia P, Suarez-Ahedo C, Domb BG. Outcomes of Endoscopic Gluteus Medius Repair: Study of Thirty-four Patients with Minimum Two-Year Follow-up. J Bone Joint Surg Am. 2015;97(16):1340-1347. doi:10.2106/JBJS.N.01229
40. Dai Z, Chen Z, Liao Y, Tang Z, Cui J. Comparison of arthroscopic versus open surgery on external snapping hip caused by gluteal muscle contracture. Hip Int. 2018;28(2):173-177. doi:10.1177/1120700017754013
41. Gulledge CM, Makhni EC. Open Gluteus Medius and Minimus Repair With Double-Row Technique and Bioinductive Implant Augmentation. Arthrosc Tech. 2019;8(6):e585-e589. Published 2019 May 17. doi:10.1016/j.eats.2019.01.019
42. Parodi D, Villegas D, Escobar G, Bravo J, Tobar C. Deep Gluteal Pain Syndrome: Endoscopic Technique and Medium-Term Functional Outcomes. J Bone Joint Surg Am. 2023;105(10):762-770. doi:10.2106/JBJS.22.00394
43. Parodi D, Bravo JT, González I, Villegas D, Tobar C. Endoscopic gluteus medius partial tear repair with collagen patch augmentation. Clinical and imaging results. IPMRJ. 2024;9(1):26-35. doi:10.15406/ipmrj.2024.09.00369
44. Seidel D, Parodi D. Retrograde Acetabular Micro Perforations, for Treatment of Chondral Lesions Grade 1 and 2 in Patients with Femoroacetabular Impingement. In: Ozcan ProfG, ed. Achievements and Challenges of Medicine and Medical Science Vol. 10. BP International; 2025:95-103. doi:10.9734/bpi/acmms/v10/3622
45. Schlegel TF, Abrams JS, Bushnell BD, Brock JL, Ho CP. Radiologic and clinical evaluation of a bioabsorbable collagen implant to treat partial-thickness tears: a prospective multicenter study. J Shoulder Elbow Surg. 2018;27(2):242-251. doi:10.1016/j.jse.2017.08.023
46. Bokor DJ, Sonnabend D, Deady L, et al. Preliminary investigation of a biological augmentation of rotator cuff repairs using a collagen implant: a 2-year MRI follow-up. Muscles Ligaments Tendons J. 2015;5(3):144-150. Published 2015 Oct 20. doi:10.11138/mltj/2015.5.3.144
47. Bokor DJ, Sonnabend D, Deady L, et al. Evidence of healing of partial-thickness rotator cuff tears following arthroscopic augmentation with a collagen implant: a 2-year MRI follow-up. Muscles Ligaments Tendons J. 2016;6(1):16-25. Published 2016 May 19. doi:10.11138/mltj/2016.6.1.016
48. Parodi D, Tobar C, Valderrama J, et al. Hip Arthroscopy and Hypothermia. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2012; 28(7):924-928. doi:10.1016/j.arthro.2011.12.012
49. Parodi D, Castrillo J, Seidel D. Peritrochanteric Decompression Via Endoscopic Release of the Proximal Insertion of the Gluteus MAjor. Poster presented at: ISHA Annual Scientific Meeting; October 17-19, 2024; Washington DC, USA