






Surgical Policy Action in Sub-Saharan Africa
Surgical healthcare: How Sub-Saharan Africa is translating global, regional, and national policy into action
Joshua Gazzetta1, Erika Gazzetta1, Mwamba Josephine Chiteba Mulenga1, Mutimba Bernard Mpabalwani1, Cyrus Phiri, Emmanuel Malabo Makasa1
- Centre for Surgical Healthcare Research
OPEN ACCESS
PUBLISHED: 28 February 2025
CITATION: Gazzetta, J., Gazzetta, E., et al., 2025. Surgical healthcare: How Sub-Saharan Africa is translating global, regional, and national policy into action. Medical Research Archives, [online] 13(2). https://doi.org/10.18103/mra.v13i2.6238
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i2.6238
ISSN 2375-1924
ABSTRACT
Nearly one-third of the global burden of disease is due to surgical diseases. In low and middle-income countries, nine out of ten people are unable to access safe, timely, and affordable surgical care. While more global policies are focused on building surgical capacity in low-resource settings, there have been limited ways to implement these policies in Sub-Saharan Africa. This research describes a novel model designed to accommodate the collaborative effort required to translate global and regional surgical policies into action throughout the Southern Africa Development Community (SADC) Member-States. Through innovative platforms, national surgery policies have been developed, revised, and implemented in several SSA countries. Additionally, policy advisement, research opportunities, and diverse stakeholder opportunities have been created to improve surgical care where it is needed most. This model may provide a framework that may be used or modified in other regions of the world.
Keywords
Sub-Saharan Africa, surgery, policy, NSOAP
Background
The Lancet Commission on Global Surgery (LCoGS) estimates that 5 billion people across the world lack access to life-saving surgical care. While surgical diseases are responsible for approximately 28% of the global burden of disease, the lack of infrastructure, equipment and qualified personnel limits the ability to provide safe, timely, and affordable surgical care in many low- and middle-income countries (LMICs). Over the last decade, there has been a robust effort to scale up surgical healthcare in LMICs through multiple World Health Assembly (WHA) resolutions and decisions spurred by the LCoGS Report and the World Bank’s “Essential Surgery” publication from Disease Control Priorities, Third Edition (DCP3). The commitments contained in the WHA resolution WHA68.15 (2015) and decisions WHA70.22 (2017) and WHA76.2 (2023) urge the United Nations Member-States to strengthen and integrate emergency and essential surgical and anesthesia care into universal health coverage, ultimately contributing to the global action plan to meet the 2030 agenda for Sustainable Development. In 2024, action points to improve surgical care were interwoven throughout the WHA agenda, including the commitment to develop an emergency, critical, and operative (ECO) care strategy plan for 2026 to 2035.
In Sub-Saharan Africa (SSA), the Southern African Development Community (SADC), founded in 1992 and comprising 16 Member-States, supports objectives enhancing the quality of life of the 379 million people of Southern Africa. To domesticate the WHA resolutions and decisions, the SADC adopted Decision 1 (2018), Decision 21 (2019) at two consecutive SADC Health Ministers Conferences. The Decisions are policy mandates that underscore SADC’s support of surgical healthcare as a component of primary healthcare and Universal Health Coverage. The SADC Member-States have committed to developing and implementing National Surgical Obstetric and Anesthesia Plans (NSOAP) as a roadmap for surgical advancement at each country level. While political commitments were made to improve surgical healthcare, there was no mechanism to carry these commitments forward in SSA. Progress on actualizing the global and regional policies has been slow and the financial investments have been intangible. An innovative model to coordinate the necessary and collaborative efforts was imperative to facilitate the adoption of the WHA and SADC decisions at the national levels. Additionally, a platform to involve local and regional healthcare workers, community members, and surgical patients was necessary to understand the true frontline community needs. In Africa, there has been an increasing need for sub-national planning and increased engagement of stakeholder partnerships to carry policy implementation forward.
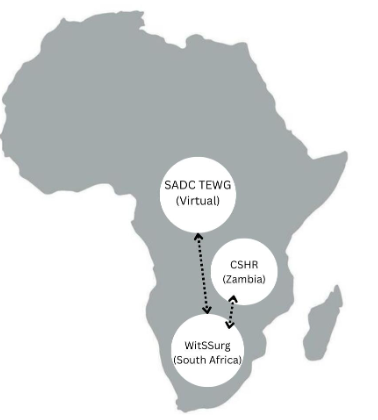
Stemming from these needs, a new model was designed to accommodate the broad and collaborative effort required to translate policy into action throughout the SADC Member-States. This model includes the following regional and national entities: (1) the SADC Surgical Healthcare Technical Experts Working Group (TEWG), (2) the Wits-SADC Regional Collaboration Centre for Surgical Healthcare (WitSSurg), and (3) the Centre for Surgical Healthcare Research (CSHR) in Zambia, the first satellite country hub of WitSSurg.
Since there are limited data on how LMICs are translating surgical healthcare policy into tangible actions, this report’s objective is to detail the SADC region’s approach to improve surgical healthcare and to fill this knowledge gap. This research aims to explain the model and platforms created to translate global, regional, and national surgical healthcare policies to real-world action plans in SSA. Additionally, this report aims to provide a framework that may be used in other regions of the world.
Methods
This is a narrative report on the development of platforms implementing surgical healthcare policy in SSA by an interdisciplinary team of global health experts, global surgery experts, surgeons, and medical educators. The research team is experienced in national surgical health planning and the team lead contributed to WHA 68.15. All members are based at the Centre for Surgical Healthcare Research which is housed in the University Teaching Hospital’s (UTH) Department of Surgery in Lusaka, Zambia. UTH is the largest teaching and referral hospital in the Republic of Zambia.
The creations of the SADC Surgical Healthcare Technical Experts Working Group, hereafter referred to as the “Technical Experts Working Group,” WitSSurg, and the Centre for Surgical Healthcare Research, hereafter referred to as the “Centre for Research” platforms were direct outcomes of the SADC decisions. The SADC secretariat, which is the executive institution of SADC responsible for the planning, coordination, and management of SADC programs, engaged professional society and academic stakeholders from each Member-State to create the Technical Experts Working Group. The SADC secretariat then partnered with the University of Witwatersrand to finance and establish the regional collaboration centre, WitSSurg, and the first national hub, the Surgical Research Centre. Each entity was created with the guiding principles of (1) translating global and regional political commitments into country-level intervention, (2) cross-border collaboration of SADC countries, and (3) facilitating partnerships to advance surgical care within the region. To empower communication and collaboration, the Technical Experts Working Group has a bidirectional relationship with the SADC secretariat and WitSSurg, and WitSSurg has a bidirectional relationship with Technical Experts Working Group and the Surgical Research Centre.
SADC SURGICAL HEALTHCARE TECHNICAL EXPERTS WORKING GROUP (TEWG)
In 2019, The SADC Technical Experts Working Group was created as a platform for open dialogue, collaboration, and strategic planning within the SADC region. The group is composed of a diverse array of individuals from each of the 16 Member-States, including Ministry of Health (MOH) representatives, professional societies, academic institutions, civil society organizations, communication professionals such as news outlets, private sector investors, and patient representatives. This group meets on a virtual platform monthly to deliberate on surgical healthcare matters and to share knowledge, resources, and technology. Additionally, the Technical Experts Working Group is responsible for key deliverables by providing technical support to countries and through policy advisory. With the Technical Experts Working Group as an appendage of the SADC secretariat, each action point is easily relayed to health ministries for appraisal.
Wits-SADC REGIONAL COLLABORATION CENTRE FOR SURGICAL HEALTHCARE (WitSSurg)
In 2019, WitSSurg was founded at South Africa’s University of Witwatersrand within the School of Clinical Medicine and hosted in the Department of Surgery. WitSSurg was created with a dual role, (1) to serve as the Centre for Global Health/Global Surgery for the university and (2) to serve as SADC’s regional collaboration centre for surgical healthcare policies and practices. Members of WitSSurg are university-affiliated and work directly with the Universities Advisory Board and with the Centre’s Executive Director who maintains the bidirectional relationship with the SADC Technical Experts Working Group. WitSSurg serves as secretariat to the SADC Technical Experts Working Group and assists with scheduling, chairing, and recording meetings. Further, WitSSurg consolidates minutes into policy documents that go to SADC and then to individual Member-States. This platform functions as the regional hub to mobilize and coordinate country support for surgical healthcare policy planning and implementation on behalf of the SADC Secretariat and SADC Member-States.
THE CENTRE FOR SURGICAL HEALTHCARE RESEARCH (CSHR)
In 2023, WitSSurg supported the Republic of Zambia to create its first country hub, the Surgical Research Centre. The Surgical Research Centre objectives include advocating for evidence-based national surgical healthcare improvement, coordinating country-level surgical healthcare policy efforts, providing technical support for policy development and implementation around surgical healthcare, and training the next generation of physician-scientists. The Surgical Research Centre is the implementing partner for Zambia’s MOH for policy-to-service delivery. Members of the Surgical Research Centre include global surgery experts, students, researchers, community members, professional societies, and members from the civil society and private sectors. The Surgical Research Centre was created as a Non-Governmental Organization (NGO) to encourage multi-stakeholder involvement from all parties invested in equitable surgical care. As a non-profit, the Surgical Research Centre is more inclusive of all stakeholders, especially the community, and is free of political and bureaucratic influence. Importantly, the Zambian community is given a voice through the centre since it functions as an open platform, combatting the “top-down” approach, which limits input from the community and surgical patients who should be the center of all policies.
Results
POLICY DEVELOPMENT AND IMPLEMENTATION
The Technical Experts Working Group conducted an NSOAP Barriers Survey to identify surgical policy barriers for formulation and implementation within the 16 SADC Member-States and subsequently provided policy recommendations to accelerate NSOAP development within the region. Together, the Technical Experts Working Group and WitSSurg have successfully supported the Republic of Zimbabwe (2022) and the Republic of Namibia (2023) in developing their national healthcare policies and are now supporting the Republic of Zambia, through the Centre for Research, to revise its NSOAP. Additionally, the Technical Experts Working Group and WitSSurg are monitoring and evaluating the implementation of the United Republic of Tanzania’s, Madagascar’s, and Malawi’s NSOAP.
The SADC Technical Experts Working Group supported the establishment of the Pan-African Surgical Healthcare Forum (PASHeF) for African Union (AU) Member States. The Republic of Rwanda hosted the inaugural and subsequent forum for Ministries of Health of African Union Member States in Kigali in July 2023 and Sept 2024 on the “Status of Surgical Healthcare Policies in Africa.” PASHef is a country-owned and country-led collaborative platform that aims to improve surgical systems and services in Africa, for Africans, by Africans. Members of the SADC Technical Experts Working Group are among the founding members of PASHef, PASHef scientific committee, and subcommittees. In fact, the PASHeF was created using the SADC model. With the aim of bringing key stakeholders together to improve surgical healthcare in Africa, the PASHef forum provides another avenue for sharing practical experiences, new approaches to policy implementation, and resource mobilization. PASHef conferences have successfully identified collective solutions to local problems with minimal external influence. For example, adjustment of healthcare insurance schemes to cover surgical diseases and the incorporation of community-based prevention programs into national surgical healthcare plans and policies have been topics emphasized to strengthen surgical systems.
The Surgical Research Centre is now a trusted partner that has been mandated by the MOH of the Republic of Zambia to carry out the country’s first NSOAP revision and support the policy’s implementation. In collaboration with the WHO-Zambia, nursing groups, professional societies, and patient groups, the Centre for Research developed and completed a baseline surgical capacity assessment using a revised WHO tool, The Emergency and Essential Surgical (Peri-Operative) Healthcare Health Facility Assessment Tool (ZAMSAT). The rapid assessment successfully captured data from 116 surgical healthcare facilities in all ten provinces to inform the NSOAP revision. As an NGO, the Surgical Research Centre was then able to partner with external funders to carry the revision and implementation process forward. In September of 2024, the Centre for Research hosted the weeklong stakeholder’s meeting to revise Zambia’s NSOAP. One of the major outcomes of the stakeholder’s meeting was a change in the implementation process. To overcome some of the barriers associated with low resources, three district-level hospitals have been chosen to pilot the revised implementation process which will be used to structure further implementation projects across the nation over time.
At the onset of the COVID-19 pandemic, the Technical Experts Working Group provided policy advisory and protocols on how to manage patients with suspected or confirmed COVID-19 across the SADC region. Additionally, the Technical Experts Working Group examined how the diversion of resources, safety protocols, and lockdowns affected surgical procedures and patients and formulated strategies to minimize pandemic-related disruptions of surgical care. Following the pandemic, surgical staff and equipment needs were mapped out by the Technical Experts Working Group to fight the backlog of surgical cases in each SADC country.
RESEARCH AND MENTORSHIP
WitSSurg and the Centre for Research have provided a stage for researchers and learners to come together to share ideas and start collaborative projects in surgical healthcare systems and services. The Centre for Research has seen tremendous growth in research projects including funded and prospective studies evaluating emergency surgeries and surgical patient barriers to care. Interns associated with Surgical Research Centre have been assigned mentorship and are exposed to the field global health through the relationship with WitSSurg. The Surgical Research Centre has become a highly competitive centre with dozens of applications each year. Additionally, strategies for training healthcare professionals in surgical techniques through WitSSurg and the Surgical Research Centre have culminated in opportunities for medical students and young professionals interested in surgery.
Discussion
The development of this novel, multi-country, model for regional and country surgical healthcare policy formulation and implementation is, to our knowledge, the first of its kind. This model establishes a clear and feasible system through which policy mandates can be directed and countries can seek support from the appropriate partners. These platforms also allow for engagement with stakeholders from the region and from around the world. The intimate relationships of SADC Member-States through the Technical Experts Working Group, WitSSurg, and the Surgical Research Centre are mutually profitable with the ability to share technology, financial, and human resources.
The importance of collaborative efforts to strengthen surgical systems can be seen globally. The Western Pacific Region has developed an action framework for surgical planning to address the challenges of surgical policy implementation. The Western Pacific Region model aims to identify actionable items that can be placed into short-, medium- and long-term national health and development plans. Using multisectoral stakeholders and both traditional and non-traditional partners is part of their process to identify gaps in surgical service delivery and redesign ways to strengthen surgical services. In the Pan-American Region, a regional cooperative model is also accelerating Ecuador’s NSOAP development. Ecuador is the first Latin country to begin NSOAP development and they are partnering with the public health system, Pan American Health Organization, and frontline surgical providers to identify top priorities for surgical services strengthening. In South Asia, Pakistan successfully created their national healthcare plan in 2020 in collaboration with government officials, the private sector, donor agencies, and international experts. While progress is being made in several world regions, the only country who has successfully performed an audit of the surgical healthcare improvement policy process is Ethiopia.
Using the SADC region model has been successful in translating WHA and SADC resolutions and decisions into meaningful actions at the country level through NSOAP developments, surgical capacity survey administration to inform policy, pandemic response initiatives, and providing a platform for knowledge-sharing and research capacity building.
CHALLENGES
Challenges these platforms face include funding and resource limitations. The Surgical Research Centre is now a highly competitive entity and due to limited funding, the centre is unable to accommodate many qualified applicants. With continued growth, funding for administrative tasks, recruitment, and research is necessary. Administrative demands also remain challenging. The platforms currently rely on a few individuals with a growing set of responsibilities. Administrative support for advocacy endeavors, recruitment of collaborators, and publicity is a priority, and increased human capital is needed to keep up with the growth.
STRENGTHS
These collaborative and open platforms provide opportunities for leadership and stakeholder engagement at all levels providing a diverse array of local, regional, and international participants. The community and patients are also given a voice in healthcare policy and provide a necessary window into frontline needs. The model provides efficient communication to streamline information and the cross-border collaboration leads to knowledge and resource sharing while reducing duplicative efforts. This model is also well situated to add new spokes and, using Surgical Research Centre as a model, scale growth throughout the SADC Member-States.
Table 1 Strengths and Challenges of the TEWG, WitSSurg, and CSHR
| Strengths | Challenges |
|---|---|
| Knowledge, resource, and technology sharing | Funding |
| Cross-border collaborations | Administrative workloads |
| Diverse stakeholder participation | Time commitments |
| Research and education capacity building | Available data to quantify progress |
| Structured for expansion | Resource constraints |
FUTURE DIRECTION
The SADC Technical Experts Working Group aims to recruit and include more stakeholders, including professional societies, biomedical engineers, paramedics, and community members, to harness expertise from all groups dedicated to mitigating surgical disparities. WitSSurg is working to extend its collaboration with other academic institutions within the SADC region and aims to place a country-spoke, similar to the Surgical Research Centre, in each of the 16 SADC Member-States. As country spokes expand among the SADC Member-States, the addition of provincial spokes within each country will further strengthen the model and overall collaboration. With an emphasis on cross-border collaboration, the addition of external partners will increase the model’s visibility, resources, and external funding. To diversify the research portfolio, the model also aims to recruit more students and scientists to engage in the efforts to advance surgical care. Finally, the Technical Experts Working Group and WitSSurg will continue to support additional SADC Member-States with their NSOAP developments and implementations.
Conclusion
This model arose from the need to translate and implement policy and generate an innovative and collaborative ecosystem to make the realization of global policy at the country level possible. The platforms have proven a way to translate global and regional policy into action in SSA and may provide a framework that may be used in other regions of the world.
References
- Meara JG, Leather AJ, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. Aug 8 2015;386(9993):569-624. doi:10.1016/S0140-6736(15)60160-X
- Shrime MG, Sleemi A, Ravilla TD. Charitable platforms in global surgery: a systematic review of their effectiveness, cost-effectiveness, sustainability, and role training. World J Surg. Jan 2015;39(1):10-20. doi:10.1007/s00268-014-2516-0
- Ologunde R, Maruthappu M, Shanmugarajah K, Shalhoub J. Surgical care in low and middle-income countries: burden and barriers. Int J Surg. 2014;12(8):858-63. doi:10.1016/j.ijsu.2014.07.009
- Alkire BC, Raykar NP, Shrime MG, et al. Global access to surgical care: a modelling study. Lancet Glob Health. Jun 2015;3(6):e316-23. doi:10.1016/S2214-109X(15)70115-4
- Mock CN, Donkor P, Gawande A, et al. Essential surgery: key messages from Disease Control Priorities, 3rd edition. Lancet. May 30 2015;385(9983):2209-19. doi:10.1016/S0140-6736(15)60091-5
- Assembly TS-EWH. WHA68.15 Strengthening emergency and essential surgical care and anaesthesia as a component of universal health coverage. 2015.
- Assembly TSWH. WHA 70.22 Progress in the implementation of the 2030 Agenda for Sustainable Development. 2017.
- Assembly TS-SWH. WHA 76.2 Integrated emergency, critical and operative care for universal health coverage and protection from health emergencies. 2023.
- Hyman GY, Park KB. Surgical Care In The Global Health Agenda: The Role Of Frontline Academic And Clinical Practitioners In Implementing World Health Assembly Recommendations [Opinion]. 2024. Journal of Global Surgery (ONE).
- SADC I. Communication and Public Relations Unit of the SADC Secretariat. 2018. SADC Secretariat Monthly Newsletter. https://www.sadc.int/sites/default/files/2021-08/Inside_SADC_October_2018_mail…pdf
- SADC I. Communication and Public Relations Unit of the SADC Secretariat. 2019. SADC Secretariat Monthly Newsletter. https://www.sadc.int/sites/default/files/2021-08/Inside_SADC_-_November_2019.pdf
- Makasa EM. Access to emergency and essential surgery obstetrics trauma and anaesthesia healthcare: a contemporary overview. Journal of Public Health and Emergency. 2021;5(8):8. doi:10.21037/jphe-2020-gs-12
- Peters AW, Pyda J, Menon G, ESuzuki E, Meara JG. The World Bank Group: Innovative financing for health and opportunities for global surgery. Surgery. 2019;165(2):10. doi:10.1016/j.surg.2018.07.040
- Reddy CL, Peters AW, Jumbam DT, et al. Innovative financing to fund surgical systems and expand surgical care in low-income and middle-income countries. BMJ Glob Health. Jun 2020;5(6)doi:10.1136/bmjgh-2020-002375
- Peters AW, Roa L, Rwamasirabo E, et al. National Surgical, Obstetric, and Anesthesia Plans Supporting the Vision of Universal Health Coverage. Global Health: Science and Practice 2020;31(8):9. doi:10.9745/GHSP-D-19-00314
- Truche P, Shoman H, Reddy CL, et al. Globalization of national surgical, obstetric and anesthesia plans: the critical link between health policy and action in global surgery. Global Health. Jan 2 2020;16(1):1. doi:10.1186/s12992-019-0531-5
- Alayande BT, Seyi-Olajide JO, Fenta BA, et al. The Pan-African Surgical Healthcare Forum: An African qualitative consensus propagating continental national surgical healthcare policies and plans. PLOS Glob Public Health. 2024;4(11):e0003635. doi:10.1371/journal.pgph.0003635
- Organization WH. Action framework for safe and affordable surgery in the Western Pacific Region (2021-2030). 2021. https://apps.who.int/iris/handle/10665/340914
- Torres Perez-Iglesias C, Hill SK, Jhunjhunwala R, et al. Strengthening surgical, obstetric, and anesthesia care in the Americas: a call to action. Lancet Reg Health Am. Jun 2023;22:100499. doi:10.1016/j.lana.2023.100499
- Pakistan MoNHSRCGo. National Vision for Surgical Care 2020-2025 The Official Launch fo Pakistan’s National Surgical Plan. 2021. https://static1.squarespace.com/static/5c838b3aab1a621eed7c5c41/t/61b70ccab53991068763c42c/1639386319817/Pakistan+NSOAP_report.pdf
- Burssa D, Teshome A, Iverson K, et al. Safe Surgery for All: Early Lessons from Implementing a National Government-Driven Surgical Plan in Ethiopia. World J Surg. Dec 2017;41(12):3038-3045. doi:10.1007/s00268-017-4271-5