





Sustainable Supply Chains in Operating Rooms: A Study
Sustainable Operating Room Supply Chains: A Case for Dynamic Physician Preference Cards
Robert Handfield¹, Amir Hossein Sadeghi², and Amirreza Sahebi-Fakhrabad²
- Department of Business Management, Poole College of Management, North Carolina State University, Raleigh, NC 27695, USA
- Department of Industrial and Systems Engineering, North Carolina State University, Raleigh, NC 27606, USA
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Handfield, R., et al., 2025. Sustainable Operating Room Supply Chains: A Case for Dynamic Physician Preference Cards. Medical Research Archives, [online] 13(4).
https://doi.org/10.18103/mra.v13i5.6508
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6508
ISSN 2375-1924
ABSTRACT
This paper presents a model that can be applied to improve the tracking of surgical instruments. At present hospitals are faced with a problem of underutilization and excess inventory leading to excess ordering of supplies without knowing their inventory at hand. A simulation was created for the hypothetical updating Physician Preference Cards (PPC) using dynamic PPCs, enabling healthcare facilities to transition towards a model of proactive, data informed supply planning that maximizes resource utilization while minimizing waste.
Keywords
- supply chain
- operating room
- physician preference cards
- inventory management
- sustainability
1. Introduction
The healthcare industry faces significant challenges related to the inefficient use of surgical supplies and equipment in operating rooms (ORs), contributing to both financial burdens and environmental impacts.¹² Studies estimate that operating rooms generate 70% of a hospital’s waste, driving up healthcare costs and posing significant environmental risks.³ For instance, a recent investigation into waste generated in a neurosurgical operating room revealed an average of $968 in OR waste per case, amounting to $242,968 per month and totaling $2.9 million annually for the neurosurgical department studied.⁴ Healthcare inefficiencies are compounded by a broader context of rising costs, with U.S. national healthcare spending reaching $4.3 trillion in 2021, accounting for nearly one fifth of the GDP.¹ Beyond financial losses, the environmental implications are severe. Operating rooms are major contributors to healthcare waste, generating one third of the sector’s waste and requiring energy intensive disposal processes. This environmental burden is exacerbated by climate change, which has already intensified extreme weather events, increased food insecurity, and worsened global health outcomes.⁵⁶
Optimizing OR supply chain management offers transformative opportunities. By minimizing waste, reducing costs, and streamlining operations, hospitals can enhance patient care and resource utilization simultaneously.² Effective supply chain strategies include the standardization of surgical instruments and supplies, improved inventory management, and the use of advanced data analytics to align resource planning with consumption patterns.² These approaches not only mitigate financial losses but also contribute to sustainability efforts, as reducing material waste directly impacts the carbon footprint of healthcare systems.⁸ Studies have demonstrated that removing unused instruments from trays and reducing supply variability among surgeons performing the same procedures can significantly lower costs without compromising patient outcomes.⁷⁸
Despite the potential benefits, many hospitals face persistent challenges in implementing efficient supply chain practice.⁹ Stockouts, administrative complexities, and resistance to change hinder progress. These issues are particularly evident in high resource environments like academic pediatric hospitals in metropolitan areas, where effective supply management is essential to ensure optimal care. Current practices often fail to leverage available data effectively, resulting in overspending, waste, and missed opportunities for improvement.¹⁰
This study seeks to address these challenges through a targeted focus on data driven solutions, leveraging digital twin and simulation techniques. By creating a virtual representation of the operating room environment, this approach enables precise modeling and analysis of supply utilization patterns. The implementation of dynamic physician preference cards (PPCs) tailored to actual utilization data offers a novel strategy for reducing variability and optimizing resource allocation. This methodology involves simulating and comparing static PPCs with updated PPCs that reflect the utilization rates of multiple surgeons, identifying opportunities for cost savings, waste reduction, and environmental impact mitigation.
The anticipated outcomes of this initiative are multi-faceted. From a financial perspective, optimized supply chain practices could significantly reduce inventory costs, freeing up resources to invest in patient care and research. Operationally, streamlined processes are expected to improve staff productivity and reduce administrative burdens. Environmentally, the reduction of unused supplies directly contributes to lowering the healthcare sector’s carbon footprint, aligning with broader sustainability goals. Ultimately, this study aims to demonstrate that data driven supply chain innovations can transform healthcare operations, delivering economic, environmental, and clinical benefits while paving the way for sustainable healthcare practices.
Ultimately, this research contributes to the growing body of literature advocating for data integration and analytics in healthcare supply chain management.
By focusing on surgical supplies, an area of healthcare that generates substantial waste and represents high costs, this study highlights the potential of advanced supply chain strategies in promoting financial efficiency and environmental sustainability in hospitals. Enhanced data integration between systems will be essential to fully realize the benefits of dynamic PPCs, enabling healthcare facilities to transition toward a model of proactive, data informed supply planning that maximizes resource utilization while minimizing waste.
2. Literature Review
Effective management of surgical resources and healthcare supply chains is critical for improving operational efficiency and reducing costs in healthcare organizations.¹¹–¹³ ORs, as high cost and resource intensive environments, present significant opportunities for optimization through innovative strategies and technologies.¹⁴ The integration of physician preference cards (PPCs), automated processes, and big data analytics has been widely discussed as a means to address inefficiencies, minimize waste, and enhance decision making in healthcare management.¹⁵ This literature review examines the current body of research, focusing on surgical resource utilization, the role of PPCs, the impact of big data analytics in healthcare supply chains, and the financial implications of supply management in the OR.
2.1. SURGICAL RESOURCES UTILIZATION
Recent studies highlight the inefficiency in surgical resource utilization, particularly in operating rooms (ORs), which generate up to 70% of hospital waste.¹⁶ Rigante et al. (2017) found that unused disposable supplies accounted for 95% of surgical waste costs in neurointerventional procedures.³ Likewise, Brauer et al. (2015) emphasized the potential for improved resource utilization without compromising care quality, citing significant opportunities for cost savings.¹⁷ Albert and Rothkopf (2015) recommended revising surgical instrument sets to minimize waste, which could lead to financial savings and environmental benefits.¹⁶ Chasseigne et al. (2018) conducted a prospective study observing 55 surgeries in a French university hospital, revealing that wasted surgical supplies accounted for up to 20.1% of the total cost allocated to surgical materials, with an estimated annual cost savings potential of €100,000 across 8,000 procedures in three surgical departments. The primary cause of waste was the anticipation of surgeons’ needs, while circulating nurses spent up to 26.3% of operative time outside the operating room, primarily to fulfill additional surgeon requests (30%).¹⁰ Millet et al. (2020) demonstrated the benefits of automation in reducing supply costs. Their study of 1,023 knee replacement surgeries found that surgeries utilizing automated processes saved an average of $2,216 in billable supply costs compared to traditional methods. Additionally, these procedures showed reduced length of stay and more consistent cost outcomes, underscoring the value of digitizing surgical processes.¹⁸ Magno-Pardon et al. (2022) conducted a retrospective cohort study using the American College of Surgeons National Surgical Quality Improvement Program database to analyze resource utilization by elective and nonelective surgeries performed between 2017 and 2018. The study revealed that elective surgeries constituted 79.8% of the total procedures and were associated with significantly lower rates of resource consumption compared to nonelective surgeries.¹⁹
2.2. PHYSICIAN PREFERENCE CARDS
Surgeon preference cards play a critical role in the management of operative supply chains, influencing the purchase, packing, and utilization of surgical instruments and supplies. Harvey et al. (2017) conducted a quality improvement study to assess the impact of updating PPCs on cost efficiency within a gynecologic surgery suite. The study involved 21 surgeons reviewing preference cards for their most frequently performed procedures, leading to changes in 39 of 48 returned cards. This intervention resulted in the removal of 109 disposable supplies, with a total cost savings of $767.67, and the elimination of three reusable instrument trays, saving an additional $925 in processing costs over three months.
Furthermore, 22 items were flagged for availability upon request rather than routine stocking, further optimizing resource use and saving $6,293.54. Post intervention, the average number of unused instruments returned to storage per case decreased from 10.1 to 9.6. These findings underscore the importance of surgeon engagement in preference card management as a practical strategy to reduce waste and enhance the cost efficiency of surgical supply chains.²⁰ Scheinker et al. (2021) developed and evaluated a novel algorithm that automates the optimization of PPCs using an informatics based approach. By cross referencing supplies used in surgical procedures and listed on PPCs, the algorithm identified inaccuracies through timeseries regression analysis. The difference in differences analysis confirmed significant cost reductions exclusively in the intervention group. The intervention in their study led to an 8.38% reduction in average direct supply costs per case, equivalent to $352 per procedure, compared to a 13.21% increase in the control group.²¹ Dreyfus et al. (2019) showed that changes to PPCs exhibited a curvilinear relationship with unplanned costs: costs initially increased with more changes but decreased beyond a certain threshold, likely reflecting improved supply accuracy. Additionally, higher communication density among operating room team members correlated with reduced unplanned costs. By employing methods such as participant observation, surveys, and data analysis, the study emphasized the interplay between PPC revisions and communication patterns in reducing waste. These findings highlight the importance of strategic PPC updates and fostering effective team communication to enhance efficiency and resource utilization in surgical settings.¹⁵ Schmidt et al. (2018) emphasized the significant role of inventory management and preference card optimization in reducing OR costs.²² Their study targeted the inventory repository in ORs and explored how inefficient processes can lead to high levels of waste. Their findings underline the critical impact of a lean preference card program in minimizing supply waste and reducing overall supply chain expenditures in surgical settings. By updating the preference card system at a Level 1 Trauma Center, they implemented a strategy to only pull items explicitly required to be opened during surgical cases. Items deemed necessary but not routinely used were no longer pre-pulled for procedures. Data collected over a month revealed a substantial potential savings of $1.18 to $1.45 million annually without extending the average surgical time per case.²²
The literature highlights the pivotal role of PPC’s in optimizing operating room efficiency, reducing supply waste, and achieving significant cost savings. Studies demonstrate that interventions ranging from manual surgeon led updates to algorithm driven automation can lead to measurable reductions in disposable and reusable supply usage, as well as overall supply chain expenditures. Effective PPC management not only decreases unplanned costs but also minimizes inefficiencies caused by inaccurate or outdated supply lists. Moreover, fostering communication and collaboration among surgical teams, combined with strategic updates to PPCs, enhances the alignment between planned and actual resource utilization. As hospitals face increasing financial and operational pressures, refining PPC processes emerges as a scalable and impactful approach to improve resource stewardship and streamline OR operations.
2.3. BIG DATA ANALYTICS AND DIGITAL TWIN TECHNOLOGY
Big Data Analytics (BDA) is emerging as a transformative tool in healthcare supply chain management. Cozzoli et al. (2022) conducted a systematic literature review on BDA in healthcare organizations, identifying its growing adoption from 2016 to 2021. They highlighted the potential of BDA based management systems to revolutionize decision making processes and improve patient care. However, the rapid evolution of BDA poses challenges for standardization and staying current with technological advancements.²³ Dash et al. (2019) highlight that the vast volumes of data generated by hospital records, medical examinations, and IoT devices present significant opportunities for enhancing healthcare outcomes. However, they note that the proper management and analysis of this data are critical, as raw data alone does not provide actionable insights. The authors emphasize the importance of high end computing solutions to overcome challenges in data handling, and they argue that with effective infrastructure and data integration, healthcare providers can unlock substantial benefits.²⁴ Olaronke and Oluwaseun (2020) also highlight that traditional methods of managing healthcare data are insufficient due to the sheer scale and diversity of information.²⁵ They stress the importance of technologies like cloud computing and virtualization for processing and analyzing large datasets securely and efficiently. However, the authors also point out several obstacles, including data fragmentation, security concerns, ethical issues, and usability challenges.²⁵ Hermon and Williams (2014) explore the growing role of big data analytics in healthcare, noting its potential to provide valuable insights despite ongoing challenges related to managing the volume, variety, velocity, veracity, and value of data. The authors highlight that while the accuracy, integrity, and interpretation of data remain key concerns in clinical applications, the exploration of big data as a tool for improving healthcare outcomes continues to progress. Through a systematic review, they identify four primary categories for big data use in healthcare: administration and delivery, clinical decision support (with a focus on clinical information), consumer behavior, and support services. Importantly, they note that big data applications in healthcare often span multiple areas, rather than being limited to a single domain, underscoring the versatility and broad applicability of big data in optimizing healthcare systems, reducing costs, and enhancing patient care.²⁶
Digital twins, when integrated with big data analytics, enable advanced simulation capabilities that can model and predict real time scenarios in healthcare, facilitating improved decision making, resource optimization, and personalized treatment strategies. Alazab et al. (2020) discuss the growing importance of digital twins in the context of Healthcare 4.0, a framework incorporating advanced technologies such as personalized healthcare, intelligent rehabilitation, and telemedicine. Digital twins, which are virtual replicas of physical entities, play a crucial role in facilitating proactive analytics and ensuring the self sustainability of healthcare networks. These capabilities allow for efficient resource management and real time decision making, responding to dynamic patient needs with minimal interaction from operators.²⁷ These systems enable better decision making by simulating complex interactions and dynamic healthcare environments. The integration allows for more efficient management of healthcare processes, such as severe trauma care, by simulating and predicting outcomes, enhancing both the personalization and responsiveness of treatments.²⁸ By leveraging AI, digital twins can process and integrate vast amounts of heterogeneous data from various sources, enabling more accurate and personalized clinical decision making.²⁹ However, the application of AI driven digital twins in healthcare faces certain barriers, which must be addressed for successful implementation and widespread adoption.²⁹
In recent years, several efforts have been made to improve the efficiency and sustainability of surgical resource utilization, as explored in the literature. Studies on surgical resource utilization have highlighted the need for better planning and tracking of resources in the OR to minimize waste and reduce unnecessary costs. The role of PPC has emerged as a significant factor in optimizing resource use, with several studies illustrating the benefits of regularly updating these cards to reflect actual usage patterns. The literature on PPCs, particularly those involving physician engagement in reviewing and updating these cards, suggests that surgeon involvement can lead to considerable reductions in supply waste and cost. However, many of the studies in this area focus on static PPCs, which do not account for real time data and actual utilization rates. In parallel, the integration of big data analytics and digital twin technology has gained attention in the healthcare supply chain domain. Big data
analytics allows for the collection and analysis of large volumes of data, which can be used to optimize various aspects of healthcare operations, including inventory management and supply chain optimization. Meanwhile, the application of digital twins in healthcare presents an innovative approach to real time monitoring and predictive analytics, offering opportunities for enhancing decision making processes. These technologies have the potential to improve the accuracy of data used to track resource utilization in the OR, leading to better informed decisions regarding inventory and supply planning.
This paper builds upon the existing literature by addressing a key gap—utilizing dynamic PPCs that are regularly updated based on real time data to optimize surgical supply chain operations. The proposed simulation model showcases the potential of integrating big data analytics and digital twin technology to monitor and predict resource usage, allowing for continuous updates to PPCs. This approach is novel in that it not only improves the accuracy of PPCs but also introduces a dynamic element that aligns supply orders with actual utilization rates, offering substantial potential for cost savings and waste reduction. By leveraging these innovative technologies, healthcare systems can achieve a more sustainable and efficient OR supply chain, surpassing the limitations of the traditional static PPC model highlighted in the reviewed literature.
3. Methodology
Our methodology involved processes that can be applied in any hospital operating rooms (OR) setting. This included process mapping of current practices for OR surgical kits and the development of a revised process map. Additionally, we created a simplified model to estimate potential savings in terms of supply costs and inventory costs for the hospital by implementing a dynamic PPC system.
3.1. CURRENT PROCESS WITH STATIC PHYSICIAN PREFERENCE CARD
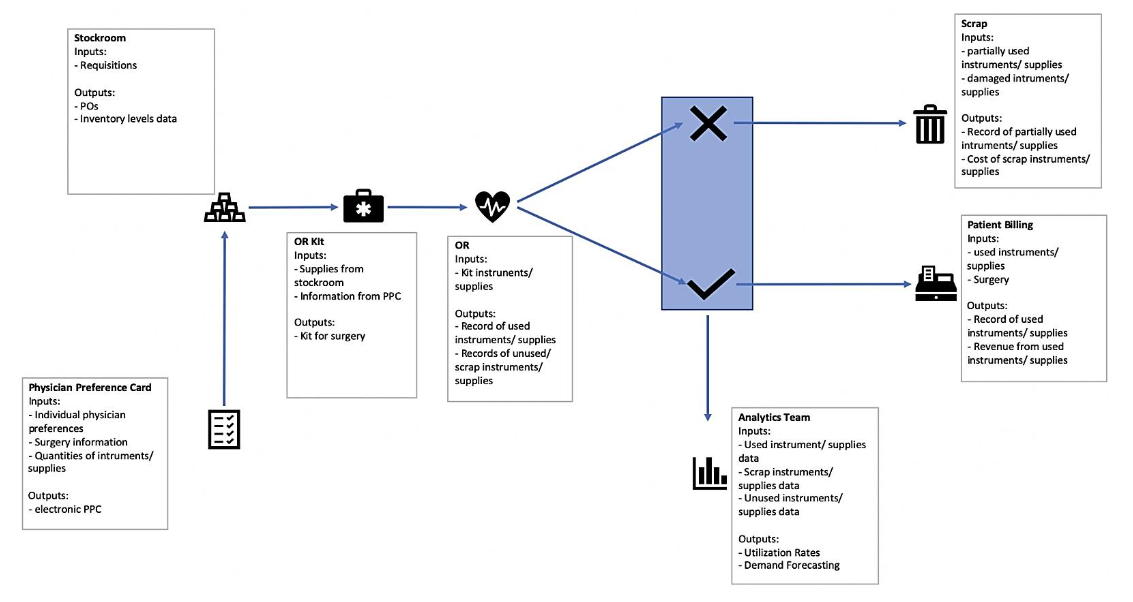
Based on conversations with a large non-profit hospital with approximately 900 beds, we gained key insights into the structure of the supply chain for surgical supplies from stockroom to scrap or billing. The process map shown in Figure 1 highlights that there are multiple discrete information systems currently that are not well-integrated. The flow of information and materials is unidirectional, culminating in excessive material and supplies waste. The following are primary systems in the process:
-
Stockroom – physical storage location for all the hospital’s supplies which uses a dedicated inventory management system to determine the distribution of supplies across the various hospital departments and to replenish supplies are required based on requisitions received.
-
Physician Preference Card (PPC) – document with individual physician preferences to facilitate customized, quality patient care. The items are custom ordered for each physician and lists all the specific items a surgeon requires to be packed into their OR kit for surgeries.
-
OR Kit – a kit prepared by nurses for each specific surgery based on the PPC for the surgeon performing that surgery. The nurse ensures that the correct supplies by specification and correct quantities are sent to the OR.
-
OR – where the actual surgery takes place and a record of used quantities of equipment and supplies is created to prepare for patient billing.
-
Analytics Team – a team has been convened to look into utilization rates but has largely not been integrated into the process to transform practices to drive up utilization.
-
Scrap – all partially used, unused, soiled and damaged supplies are sent to scrap. Some instruments may be sent back to the stockroom after sterilization.
-
Patient Billing – patients are billed through the EPIC system for any instruments used and supplies consumed during the surgery.
3.2. ANALYTICAL MODEL
Based on our understanding of the processes at data from the hospital that we had access to, we created an analytical model to highlight the importance of regularly updating Physician Preference Card (PPC) using input from surgical supplies utilization as a metric to better inform supplies purchasing and creation of surgical kits for operating room (OR). The model built brings to attention the potential cost-savings and waste reduction benefits of using dynamic PPCs instead of the current method of using static PPCs that do not take actual usage of materials and supplies into consideration. In the current process, the key cost components include the actual unit cost of the instruments and consumable materials, inventory holding costs, and reordering costs, and sterilization costs for items to be re-entered into the stockroom.
To simplify the model, we decided to focus on a particular type of spine surgery, lumbar discectomy, and created a list of commonly used instruments and consumable materials in a typical lumbar discectomy surgery by speaking to several surgeons.
We also made several assumptions regarding the number of surgeries, the costs associated with the supplies and the usage rates of these supplies:
-
120 lumbar discectomy surgeries happen per year with each surgery having the exact same total cost
-
Unit cost of each instrument or consumable supply was arbitrarily determined. Inventory carrying cost was taken to be 18% of the unit cost and total unit cost was a sum of the unit cost and inventory carrying cost
-
All instruments and consumable materials partially used, unused, soiled or damaged in the OR will be sent to scrap – nothing will be resterilized and put back into the stockroom. As such, there are no costs associated with sterilization in this model
-
For the common PPC, quantities used and scrapped per item per surgery were randomly generated
-
Beginning inventory levels were randomly generated
-
Reorder point and reorder quantity were arbitrarily determined – reorder point was set at 70 for all three selected supplies, reorder quantity was 30 for the Mastoid Self-Retaining Retractor, 50 for the Right C Retractor and 66 for the Bone Nibbler
-
Reorder cost was determined to be a fixed amount per transaction at a rate of $500 for the Mastoid Self-Retaining Retractor, $400 for the Right C Retractor, and $200 for the Bone Nibbler
-
For updated PPCs scenario, doctor 1 does 48 surgeries and doctors 2 and 3 do 36 surgeries each over a year
Based on the surgery supplies list and our assumptions, a surgery inventory master was created that showed an estimated cost per surgery and the total cost of unused/scrap materials. That data was then extrapolated to simulate 120 surgeries for the entire year and was then fed into the inventory master. This scenario depicts the usage of a common PPC with low utilization rates. Three more PPCs were created to mimic 3 individual physician PPCs with updates to surgical supply quantities closer to their actual usage rate. For each of these scenarios, utilization per year for each surgical supply item was calculated. This allowed us to compare the cost of surgical supply materials for a year period between using a common PPC and an updated PPC.
The next part of the model simulates surgical supplies reordering throughout the year depending on the common PPC utilization as well as updated PPCs utilization rates. The Mastoid Self-Retaining Retractor, Right C Retractor, and Bone Nibbler were selected to model this reordering process. Beginning inventory was set at 100 units, reorder point was fixed at 70 units, and reorder quantity was 30 for the Mastoid Self-Retaining Retractor, 50 for the Right C Retractor and 66 for the Bone Nibbler. This model was able to show the net impact on inventory costs over a year period.
4. Results
The outcomes of our analytical model clearly demonstrate the financial and operational benefits of transitioning from a static, common Physician Preference Card (PPC) system to a dynamic, utilization-informed PPC framework. By simulating a year’s worth of lumbar discectomy surgeries under both scenarios, we were able to quantify cost savings across multiple dimensions.
The model revealed that using updated PPCs based on individual physician utilization data significantly reduces the total quantity of surgical supplies required per procedure. When aggregated over 120 surgeries annually, this reduction translated into a 47% decrease in surgical supply expenditures compared to the static PPC approach. These savings stem from the elimination of routinely overstocked or unnecessary items, many of which were either underutilized or consistently discarded in the static model.
This improvement not only reduces costs but also minimizes wasteful overconsumption of medical-grade instruments and materials. In addition to reducing supply usage, updated PPCs also impacted inventory dynamics. Lower quantities per surgery mean that existing stock is depleted more slowly, delaying the need for reorder triggers.
As a result, the model simulated 58% savings in inventory holding and reorder costs across the year. The slower inventory turnover directly translates into fewer replenishment transactions, which under the static PPC scenario, were frequent due to inflated supply quantities and faster depletion rates. These savings are especially relevant in hospital systems where high reordering costs are incurred due to fixed transaction fees and logistical complexities.
When considering both the reduction in surgical supply expenses and inventory-related costs, our model projects a 52% total annual cost saving by moving to updated PPCs. This figure reflects the combined benefit of better-aligned supply preparation and more efficient inventory management.
Importantly, the benefits extend beyond mere financial savings. Less scrap, fewer expired or soiled items, and more precise OR kit composition support broader sustainability and quality improvement goals within the hospital.
A secondary outcome of using dynamic PPCs is the substantial improvement in utilization efficiency. The customized PPCs for each of the three surgeons resulted in item lists more accurately reflecting what is actually used during surgery. As a result, waste is
dramatically reduced. Items no longer routinely discarded or sent to scrap unnecessarily contribute to a more sustainable OR process. While we assumed that no items were sterilized and returned to inventory, incorporating sterilization loops could lead to even greater reductions in waste and costs, making this an important area for future study.
Although the model employs several simplifying assumptions, such as fixed numbers of surgeries, randomly generated inventory levels, and static reorder points, its findings are directionally consistent with actual hospital inefficiencies reported in literature and practice. For instance, many hospitals still rely on outdated PPCs and lack feedback loops to adjust them based on usage data. Even with arbitrary utilization rates, our model shows that aligning PPCs with real-world use can yield significant benefits. Future studies can refine this model using hospital-specific data, potentially unveiling even larger financial and operational improvements.
5. Discussion
The analytical model developed in this study offers compelling evidence in support of a dynamic, utilization-driven approach to managing Physician Preference Cards (PPCs). By explicitly demonstrating the cost inefficiencies inherent in the continued use of static PPCs, this research underscores the need for hospitals to transform how they approach surgical kit preparation and inventory management.
While the model itself is based on a simplified case involving a single type of spine surgery, the core insights and operational principles are highly generalizable across other surgical domains. Transitioning to dynamic PPCs is not merely a matter of reordering supplies. It demands a foundational reconfiguration of processes, systems integration, and cultural norms within hospitals.
At the heart of this shift is the establishment of a robust, interdisciplinary feedback loop capable of driving continuous improvement. This feedback loop, as shown in the recommended process map (Figure 2), integrates data from the operating room, inventory systems, and supply utilization records to inform the ongoing refinement of PPCs.
Such a system requires that unused but unopened supplies be routed back into inventory rather than discarded, emphasizing not only cost efficiency but also environmental sustainability.
Figure 2. Recommended Process with Dynamic PPC.
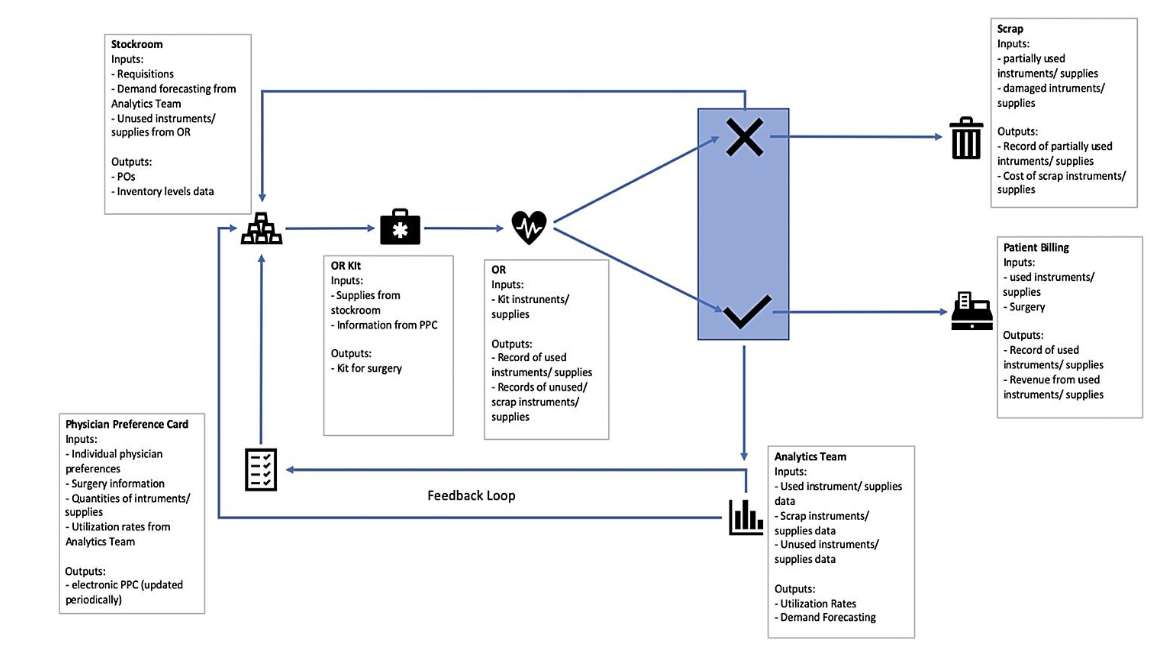
Figure 2. Enhanced Process with Dynamic PPC.
Central to achieving this vision is the strategic empowerment of the hospital’s Analytics Team. Currently, analytics functions are often siloed and underutilized, lacking the visibility and authority to influence core supply chain decisions. To realize the benefits of dynamic PPCs, the Analytics Team must be embedded within the operational fabric of the hospital. This includes establishing formal data pipelines that capture real-time usage data from surgical teams, billing systems, and stockroom inventories. With access to these data streams, analysts can develop actionable metrics such as utilization variance, reorder frequency, and scrap rates to inform PPC revisions and procurement strategies.
Additionally, collaboration between stakeholders is critical. Cross-functional teams composed of surgeons, nurses, supply chain staff, and analysts should be formed to co-design PPC updates and interpret utilization data. Beyond internal collaboration, there is also a pressing need for physician engagement and cultural change. Surgeons often default to highly individualized supply preferences, influenced by training, past experience, or vendor relationships. Encouraging standardization such as through hospital-level agreements on preferred brands or consolidated product lists can dramatically simplify supply logistics and reduce the variability that undermines inventory efficiency. Regular forums or workshops where physicians review aggregated usage data and share best practices could promote greater buy-in and facilitate consensus-building.
Analytical tools are imperative for improving hospital operations, especially in the area of utilization. Some of the representative challenges we discovered in interviewing hospital supply chain managers included the following:
-
“As I reduce our costs, we are being paid less by both commercial payors and the government. I’m not making any more money, because reimbursements keep dropping and there is no control over the belief that healthcare is too expensive.”
-
“We struggle with the day-to-day operational details of charge capture, clinical documentation, and product replacement. So we don’t really know if we are making a profit on any given patient or operation on any given day.”
-
“Our working capital is bloated, but we can’t seem to get control over how much inventory we have, the utilization of those materials, or the prices we are being billed for them. The nurses don’t want to run out for fear of the doctor’s wrath, yet the product version itself changes every two months. Because we’re not ever allowed to run out, we overcompensate by having more than we need, but we end up wasting a lot of materials that is never charged back to the payor.”
-
“We are consumed with rolling out Electronic Health Records, which have no link back to materials consumed. We are spending millions on EPIC but aren’t seeing any benefit in terms of cost reduction or revenue generation.”
-
“In the operating room during procedure, nurses will put a sticker on a sheet showing an item was consumed, and they know they must document that they used one stent (for example). But often they don’t know the size or the item number, as the search function in EPIC is limited. But nurses aren’t trained to know the upstream and downstream effects of data inaccuracy. So the health record ends up being inaccurate, and so does the invoicing to the patient, as well as the material tracking record in the inventory system.”
These challenges faced by hospitals are leading to a situation of increasing financial instability and losses, as a result of no visibility to performance data, on-going financial losses, and increasingly frustrated personnel who are leaving the profession. This has led to the saying that healthcare is a “Seven trillion $ cottage industry”, due to the inept handling of data, analytics, and performance outcomes.
One tactical approach to mitigating loss of visibility without compromising clinical flexibility is the implementation of a two-tiered PPC system. In this
structure, each physician’s PPC would be divided into a “required” list, containing essential supplies, and a “standby” list, featuring items that are occasionally used. Standby kits would only be opened if clinically necessary, and unopened kits could be returned directly to stock, thereby avoiding unnecessary waste. While this approach may initially add operational complexity for nursing staff responsible for kit preparation, the long-term reductions in waste, reordering costs, and environmental impact present a compelling case for its adoption. Moreover, the model supports strategic prioritization in PPC updates. Given the wide variation in surgical volume across procedures, a phased implementation that targets the most frequently used PPCs can produce significant early returns. As suggested by industry experts, focusing on the top 20 percent of PPCs by volume whether by department or overall hospital usage can address up to 80 percent of the total supply cost base, thereby maximizing the impact of initial efforts before scaling further.
From a systems-level perspective, the discussion highlights a broader issue of fragmentation in hospital operations. The lack of integration between supply chain, analytics, clinical staff, and IT systems results in inefficiencies that are difficult to resolve without systemic change. Hospitals looking to implement dynamic PPCs should consider investing in enterprise-wide platforms that enable interoperability between data sources and support advanced analytics capabilities. In the long term, this integration will be crucial not only for supply management but also for other strategic initiatives such as value-based care, sustainability reporting, and predictive modeling of clinical and operational outcomes. Ultimately, this study illustrates how relatively modest changes, rooted in better data, more frequent feedback, and collaborative governance, can yield substantial financial and operational benefits. While our model employs simplifying assumptions and does not capture the full range of surgical and institutional variability, it clearly demonstrates that aligning supply decisions with actual usage patterns can drive significant cost savings, reduce environmental waste, and improve operational resilience. As healthcare systems continue to face increasing pressure to do more with less, models like this offer a practical blueprint for operational transformation which is both economically and ethically compelling.
6. Conclusion
Our analytical model considers two scenarios: one utilizing static Physician Preference Cards (PPCs) and another employing dynamic PPCs based on updated utilization data from three different surgeons. By comparing the cost and inventory outcomes of each scenario, this study quantifies the potential savings from using dynamic PPCs, providing evidence to support data-driven surgical supply management. Modeling offers a valuable method for analyzing these complex systems, as it allows for the examination of multiple variables and interdependencies that impact operating room (OR) resource utilization.
We also believe that more complex simulation models that are based on actual data collected in OR procedures could provide a much richer set of conclusions. We believe that future research in this vein can produce some important insights for improved utilization of hospital supplies, in an era where healthcare is under pressure to reduce costs of procedures.
References
1. Sathe TS, Sorrentino TA, Wang K, et al. Instrument and supply variability: an opportunity to reduce the carbon footprint of the operating room. Journal of Surgical Research. 2024;295:732-739.
2. Estrera SL. Improving Operating Room Supply Chain Efficiency and Cost-Reduction Using Data Analytics. UCLA; 2024.
3. Rigante L, Moudrous W, de Vries J, Grotenhuis AJ, Boogaarts HD. Operating room waste: disposable supply utilization in neurointerventional procedures. Acta Neurochir (Wien). 2017;159:2337-2340.
4. Zygourakis CC, Yoon S, Valencia V, et al. Operating room waste: disposable supply utilization in neurosurgical procedures. Journal of neurosurgery. 2017;126:620-625.
5. Yates EF, Bowder AN, Roa L, et al. Empowering surgeons, anesthesiologists, and obstetricians to incorporate environmental sustainability in the operating room. Annals of surgery. 2021;273(6):1108-1114.
6. Wu S, Cerceo E. Sustainability initiatives in the operating room. The Joint Commission Journal on Quality and Patient Safety. 2021;47(10):663-672.
7. Park KW, Dickerson C. Can efficient supply management in the operating room save millions? Current Opinion in Anesthesiology. 2009;22(2): 242-248.
8. Ahmadi E, Masel DT, Metcalf AY, Schuller K. Inventory management of surgical supplies and sterile instruments in hospitals: a literature review. Health Systems. 2019;8(2):134-151.
9. Man LC, Lin Y, Pang G, Sanderson J, Duan K. Digitalization to achieve greener healthcare supply chain. Journal of Cleaner Production. Published online 2024:142802.
10. Chasseigne V, Leguelinel-Blache G, Nguyen TL, et al. Assessing the costs of disposable and reusable supplies wasted during surgeries. International Journal of Surgery. 2018;53:18-23.
11. Kwon IWG, Kim SH, Martin DG. Healthcare supply chain management; strategic areas for quality and financial improvement. Technological forecasting and social change. 2016;113:422-428.
12. Moons K, Waeyenbergh G, Pintelon L. Measuring the logistics performance of internal hospital supply chains–a literature study. Omega. 2019;82:205-217.
13. Avinash B, Joseph G. Reimagining healthcare supply chains: a systematic review on digital transformation with specific focus on efficiency, transparency and responsiveness. Journal of Health Organization and Management. 2024;38(8):1255-1279.
14. Baltera RM. How to Run a Cost-Effective Operating Room: Opportunities for Efficiency and Cost-Savings. Hand Clinics. Published online 2024.
15. Dreyfus D, Nair A, Rosales C. The impact of planning and communication on unplanned costs in surgical episodes of care: implications for reducing waste in hospital operating rooms. Journal of Operations Management. 2020;66(1-2):91-111.
16. Albert MG, Rothkopf DM. Operating room waste reduction in plastic and hand surgery. Plastic Surgery. 2015;23(4):235-238.
17. Brauer DG, Hawkins WG, Strasberg SM, et al. Cost variation in a laparoscopic cholecystectomy and the association with outcomes across a single health system: implications for standardization and improved resource utilization. HPB. 2015;17(12): 1113-1118.
18. Millet C, Chimento G, Barrette W, Dasa V. Can automating surgical processes reduce operating room supply costs? A pilot study of a novel OR based technology. Journal of Orthopaedic Experience & Innovation. 2020;1(1).
19. Magno-Padron DA, Holoyda KA, Moss W, et al. Elective surgery resource utilization. Langenbeck’s Archives of Surgery. Published online 2022:1-5.
20. Harvey LFB, Smith KA, Curlin H. Physician engagement in improving operative supply chain efficiency through review of surgeon preference cards. Journal of minimally invasive gynecology. 2017;24(7):1116-1120.
21. Scheinker D, Hollingsworth M, Brody A, et al. The design and evaluation of a novel algorithm for automated preference card optimization. Journal of the American Medical Informatics Association. 2021;28(6):1088-1097.
22. Schmidt RN, Posteraro RH, Lopez M. Reducing Waste in the Operating Room Through Inventory-Based Supply Chain Optimization. ASBBS Proceedings. 2019;26:476-483.
23. Cozzoli N, Salvatore FP, Faccilongo N, Milone M. How can big data analytics be used for healthcare organization management? Literary framework and future research from a systematic review. BMC health services research. 2022;22(1): 809.
24. Dash S, Shakyawar SK, Sharma M, Kaushik S. Big data in healthcare: management, analysis and future prospects. Journal of big data. 2019;6(1):1-25.
25. Olaronke I, Oluwaseun O. Big data in healthcare: Prospects, challenges and resolutions. In: 2016 Future Technologies Conference (FTC). ; 2016:1152-1157.
26. Hermon R, Williams PAH. Big data in healthcare: What is it used for? Published online 2014.
27. Alazab M, Khan LU, Koppu S, et al. Digital twins for healthcare 4.0—Recent advances, architecture, and open challenges. IEEE Consumer Electronics Magazine. 2022;12(6):29-37.
28. Croatti A, Gabellini M, Montagna S, Ricci A. On the integration of agents and digital twins in healthcare. Journal of Medical Systems. 2020;44 (9):161.
29. Kaul R, Ossai C, Forkan ARM, et al. The role of AI for developing digital twins in healthcare: The case of cancer care. Wiley Interdisciplinary Reviews: Data Mining and Knowledge Discovery. 2023;13 (1):e1480.
30. Saver C. Manage physician preference cards to boost efficiency and patient safety. OR manager. 2016;32(3):14-16.