






Symptom Alleviation: Alcohol and Cannabis Use in Students
A Survey Study of Symptom Alleviation Motives for Alcohol and Cannabis Use among Students With and Without Chronic Health Conditions
Dana Balsink Krieg1, Paula M. Millin1, Megan Richards1, Delaney Klace1,
- Kenyon College, Department of Psychology, Gambier, OH 43022
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: KRIEG, Dana Balsink et al. A Survey Study of Symptom Alleviation Motives for Alcohol and Cannabis Use among Students With and Without Chronic Health Conditions. Medical Research Archives, [S.l.], v. 13, n. 10, oct. 2025. Available at: <https://esmed.org/MRA/mra/article/view/7038>. Date accessed: 03 nov. 2025.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.7038.
ISSN 2375-1924
Abstract
The purpose of this study was to examine cannabis and alcohol use patterns and self-medication motives in college students with and without a formally diagnosed chronic mental or physical health condition who are or are not taking prescription medication for their condition. To that end, college students were surveyed about their frequency of alcohol and cannabis use, as well as their motives for using alcohol and cannabis, including a direct assessment of intentional self-medication. They were also asked if they were taking prescription medication for their health condition. Results showed that more students had used alcohol than cannabis in the past 30 days, but that among users, cannabis was used on significantly more days than alcohol. Half of our sample reported chronic health conditions and nearly 40% of those students reported that they were taking prescription medication for their condition. Those with a physical health condition used alcohol and cannabis at similar rates as those without, while those with a mental health condition used cannabis (but not alcohol) at a higher rate. Those with a mental health condition reported intentionally using both alcohol and cannabis to alleviate their symptoms, while those with a physical condition reported using only cannabis to deliberately self- medicate. Taking prescription medication was associated with a marginally higher frequency of cannabis (but not alcohol) use. All participants, regardless of formal health diagnosis, endorsed cannabis more often than alcohol as a sleep aid, to relieve pain, to increase appetite, and to relax. Alcohol was endorsed more often “to party with friends” and to “get intoxicated”. Taken together, these results show that, like the general population of American adults, college students, and especially those with a chronic mental or physical health problem, use cannabis to self-medicate. Potential implications of this behavior are discussed.
Introduction
Chronic mental and physical health conditions are alarmingly common among United States (U.S.) adults. A 2025 study analyzing data from more than 2.5 million U.S. adults across ten years found that 76.4% were living with at least one chronic health condition in 2023 and that 51.4% were living with two or more of the following chronic conditions: arthritis, asthma, cancer (excluding skin cancer), chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), depressive disorder, diabetes (excluding gestational diabetes), heart disease, high blood pressure, high cholesterol, obesity, and stroke.¹ While adults aged 65 and older had the highest prevalence of chronic conditions (93% had at least one), the prevalence in younger adults, aged 18–34, was substantial and increased significantly from 52.5% in 2013 to 59.5% in 2023. Investigating the prevalence of mental health conditions, the Substance Abuse and Mental Health Services Administration (SAMHSA, the branch of the U.S. Department of Health and Human Services that tracks the mental health and substance use behaviors of American adults), found that 58.7 million (22.8%) of Americans over the age of 18 met the diagnostic criteria for one or more mental health conditions in 2023 (the most recent year for which they reported results of their annual National Survey of Drug Use and Health Study; NSDUH).² The rate of mental illness was highest in young adults aged 18–25 (33.8%). Many factors likely contribute to the high prevalence rate of mental illness in this cohort, including changes in brain structure and function,³ environmental factors, high levels of psychosocial stress,⁴ and a high incidence of interpersonal traumatic events.⁵
The widespread presence of chronic health problems necessitates the spending of trillions of dollars in healthcare in the U.S. each year. The National Institute of Health Care Management (NIHCM) reported that 90% of the 4.5 trillion dollars spent on healthcare in 2022 was spent on the treatment of chronic physical and mental health conditions.⁶ Although many Americans are satisfied with the cost and quality of their own healthcare, a recent Gallup poll showed that 29% rated the quality of their care as “only fair” or “poor” and 35% rated their healthcare coverage as “only fair” or “poor.”⁷ Further, a majority of Americans said they believed that the U.S. healthcare system is in crisis, citing cost and access as top problems.⁷ Given the high demand for and common dissatisfaction with conventional healthcare in the United States, it is perhaps not surprising that many Americans seek relief for chronic conditions by using alternative treatments available outside of the industrial medical complex.
In addition to vitamins, supplements, and herbal remedies, this includes the use of alcohol and other recreational drugs. In fact, one prominent theory for the etiology and maintenance of problematic drug and alcohol use is the self-medication (SM) hypothesis, which posits that negative reinforcement (relief from symptoms) motivates and sustains the drug use, as a primary driver of alcohol and other drug use for many people.⁸ Self-medication has long been recognized as a motivation for alcohol use in adults, including college students, suffering from mood and anxiety disorders,⁹ sleep problems,¹⁰ and physical pain conditions.¹¹ As legalization of medical and recreational cannabis continues to expand across the U.S., it will be interesting to observe the relative roles that cannabis and alcohol play in self-medication. This is a goal of the current study.
What do we know about cannabis self-medication, to date? It appears that cannabis self-medication for physical and mental health conditions has become a common phenomenon among U.S. adults. One study found that 27.4% of North American adults reported ever having used cannabis to self-medicate, and that the rate of self-medication was highest in U.S. states where recreational use of cannabis was legal (34%).¹² The top physical health-related reasons for self-medication were pain, sleep problems, and headaches, while the top mental health-related reasons were anxiety, depression, and PTSD/trauma.¹² Males were more likely than females to report self-medication, and people aged 26–36 years were more likely to report self-medication than other age cohorts.¹² In this study, the youngest participants were grouped into a single age bracket, ranging from 16–25 years, and college students were not differentiated from non-student age-matched young adults, precluding conclusions regarding the rate of self-medication among college students, specifically.¹² This is unfortunate because we suspect that college students represent a unique cohort for whom self-medication with cannabis may be particularly appealing since they often experience obstacles to conventional healthcare, such as a lack of knowledge or confidence required to navigate the healthcare system, lack of time, long wait times for appointments, and lack of transportation to off-campus doctors’ appointments.¹³ Moreover, cannabis is readily accessible to college students and they already use cannabis recreationally at very high rates.¹⁴ Additional research suggests that they increasingly view cannabis as a low-risk drug.¹⁴
While research on cannabis self-medication in college students is sparse, what exists is generally consistent with findings in the more general population of adults. For example, in a sample of frequent college cannabis users with high Cannabis Use Disorder Identification Test-Revised (CUDIT-R) scores (placing them in a “hazardous use” category), a recent study found that the top four most commonly endorsed self-medication motives were anxiety (81.7%), sleep problems (79%), depression (59.4%), and pain (40.6%).¹⁵ Other studies have likewise reported that a high percentage of cannabis-using college students report consuming cannabis as a sleep aid, at least occasionally.¹⁶ Moreover, college students with greater exposure to interpersonal trauma and trauma-related distress were more likely to use cannabis non-experimentally (defined as greater than six lifetime uses), supporting a self-medication hypothesis (though it is important to note that the relationship was correlational, as they did not explicitly ask participants if they were using cannabis to self-medicate).⁵ Investigating self-medication for an especially burdensome type of chronic health condition, a recent study from our laboratory found that college students with a diagnosed autoimmune disease were significantly more likely to have used cannabis in the past 30 days and to endorse therapeutic motives for cannabis consumption, including pain control, nausea control, improved sleep, and appetite stimulation than those without an autoimmune disease.¹⁷ We suspect that self-medication is an underappreciated motive for cannabis use in college students with diagnosed chronic health conditions not limited to autoimmune diseases; the current study was designed to investigate this possibility.
One likely reason for the paucity of data on self-medication is that few existing studies explicitly include self-medication. Early investigations into the motivations for cannabis use in college students typically employed the Marijuana Motives Measure (MMM) developed by Simons and colleagues.¹⁸ (Please note that the term “cannabis” is now generally preferred over “marijuana” because it is a more scientifically accurate and broadly encompassing term for products derived from the cannabis sativa L plant and because of concerns that the term marijuana has racist roots; however, in an attempt to avoid confusion, we will use the term marijuana when describing early research employing measures that utilized that term). This 25-item scale, which is an adaptation and extension of the four-factor alcohol motives measure pioneered by Cooper,¹⁹ investigates five categories of cannabis motives, including Enhancement (e.g., to get high, because I like the feeling, to have fun), Conformity (e.g., to be liked, so I won’t feel left out, to fit in with the group I like), Expansion (e.g., to know myself better, because it helps me be more creative and original, to expand my awareness), Coping (e.g., to cheer
me up when I am in a bad mood, to forget my worries, because it helps me when I feel depressed or nervous), and Social (e.g., because it makes social gatherings more fun, to be sociable, to celebrate a special occasion with friends). Subsequently, Lee et al.²⁰ explored additional motivations for cannabis use in college-bound, recent high school graduates using an open-ended questionnaire that asked participants to rank order their top five reasons for using cannabis, which resulted in the identification of nineteen unique categories of motives and formed the basis for an expanded marijuana motives measure known as the Comprehensive Marijuana Motives Measure (CMMM).²⁰ The nineteen motivations identified by Lee et al. overlapped substantially with those from the original MMM, but also included many novel motives, including boredom, experimentation, relaxation, sleep, perceived safety, availability, rebellion, and habit/routine motives.²⁰ In addition, 1.26% of respondents reported “medicinal” use as a motive,²⁰ however, this was not included in the final CMMM scale because it failed to emerge as a significant factor when subjected to factor analysis in a later study of 346 marijuana-using college students.²¹
The recent studies showing that self-medication with cannabis is common may suggest that a cultural shift in attitudes and perceptions about cannabis’ utility as an alternative medicine is driving an increase in therapeutic motives. The fact that many states legalized medical cannabis before it was made legal for recreational use may have encouraged the perception that cannabis has known medical benefits. Moreover, legalization has increased potential consumers’ exposure to cannabis marketing, which often promotes the “health benefits” of cannabis and is related to more positive perceptions and greater use of cannabis.²²–²³ Regardless of the reasons, we are glad to see increased attention being given to the role that self-medication motives play in driving cannabis use behaviors in college students. This is especially important because research has consistently shown that people who report coping motives for cannabis use (which might reasonably be considered a form of self-medication for negative affective states) are at increased risk for Cannabis Use Disorder (CUD).²⁴
The current survey study assessed the frequency of, and motivations for, cannabis and alcohol use in a sample of college students with and without a formal diagnosis of a chronic mental and/or physical health condition. We further examined whether those students who reported a formal diagnosis were taking prescription medication for their ailment(s) and whether their medication status was related to self-medication motives. Finally, we asked participants directly if they used cannabis to self-medicate their chronic condition. We did not ask participants about their specific diagnoses, as we were not attempting to discern which diagnoses were associated with which motives, but rather were interested in self-medication including students with ongoing health problems and whether their medication status was related to the likelihood that they self-medicated with cannabis. Breaking down motives by diagnosis is difficult without adequate targeted sampling due to small per-condition sample sizes, resulting in insufficient statistical power. This is a goal for future studies.
Methods
Participants
The sample was recruited from a small, residential, selective, liberal arts college in the midwestern United States. Participants (N = 44) were excluded if they reported never having used either alcohol or cannabis, leaving a sample of 209 participants with any history of alcohol or cannabis use. The majority (61.7%) of participants identified as female, 29.2% identified as male, 8.6% identified as non-binary or third gender. One participant preferred not to answer. Participants represented all four class years: 17.2% first years, 28.7% sophomores, 31.6% juniors, and 22.5% seniors. Students ranged in age from 18–23, with a mean of 19.95. Twenty-eight
participants chose not to share their age. This may be due to the age restrictions on alcohol use; participants may not have been comfortable disclosing under-age use. The majority of participants (65.1%) come from states where cannabis use is legal for both medicinal and recreational purposes, whereas relatively equal subgroups report that cannabis use is legal in their home state for medical purposes only (17.7%) or that it is illegal in their home state (16.3%). Note that at the time of this data collection, in the state where the participants attend college, cannabis use was only legal for individuals with a prescription from a medical professional. Only two respondents reported having what is commonly referred to as a medical marijuana card.
Measures
Participants were first asked to report whether they had been diagnosed with either a chronic physical or mental health condition and whether or not they were regularly taking prescription medication for that condition. Participants were then asked to describe their patterns of cannabis and alcohol use. They then selected from a list (see Table 1, in the Results section) their motives for use of alcohol and cannabis. Participants were also asked specifically whether they used cannabis or alcohol to reduce symptoms of their physical or mental health condition.
Procedure
Participants were recruited through the psychology department participant pool and through mass emails to the student body. The psychology participant pool includes undergraduate psychology majors and non-majors. Students recruited through the participant pool were all currently enrolled in a psychology class. Additional students not currently enrolled in psychology classes were recruited through the student email service. All participation was voluntary and, as a convenience sample, assumed to be fairly representative of the student body. All data were collected online via Qualtrics. Participants could complete the survey on any device, but were instructed to do so in a place that provided privacy. All data were collected during a two-week period in the Fall semester of the 2023/24 academic year, prior to which students had been on campus for at least the last month, as alcohol and cannabis use pattern items referred to the last 30 days. All statistical analyses were conducted using SPSS statistical software.
Results
Alcohol and Cannabis Use Patterns
The college students in the current study reported using alcohol and cannabis frequently. Participants were asked to report on how many of the last 30 days they used alcohol and cannabis. Of the 190 participants (91%) who reported alcohol use, the responses ranged from 1 day to 19 days, with an average of 5.25 days (SD = 3.28). For cannabis, 113 participants (54%) reported use. Their responses ranged from 1 day to 30 days, with an average of 8.88 days (SD = 9.44). Substantial percentages reported daily or near-daily use (23% used more than 15 days, 11.5% used every day). Many participants (N = 108; 51%) reported using both substances within the last 30 days. The number of days of alcohol and cannabis use were significantly correlated, r(106) = .28, p < .01. However, participants reported significantly more days of cannabis use than alcohol use, t(107) = 2.4, p < .05. Participants also reported their recency of use. The majority of alcohol users (56.5%) and a substantial percentage of cannabis users (26.2%) reported having last used within the past few days.
Participants reported whether they had ever been diagnosed with a chronic physical health condition (17.7%, indicated yes) or chronic mental health condition (45.9%, indicated yes). There was considerable overlap in these two groups, wherein 75% of the participants reporting a physical health condition also had a mental health condition. As a result, 50% of the sample had either a physical or mental health condition or both. In addition, 39.7% reported regularly taking medication for their
chronic health condition. Alcohol users who reported regularly taking medication for their health condition did not differ from those who did not take medication in the number of days they use alcohol. However, cannabis users taking medication (N = 50, M = 10.66, SD = 10.91) reported a marginally higher number of days of cannabis use (N = 63, M = 7.11, SD = 8.66), t(92.1) = 1.88, p = .06.
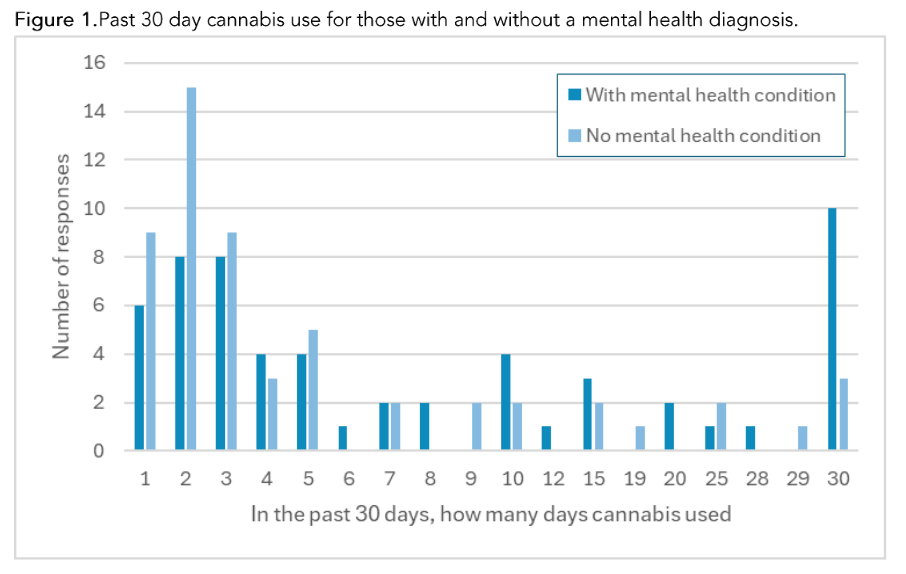
When comparing use patterns of individuals reporting a chronic physical health condition to those without, there were no differences in the number of reported days of alcohol or cannabis use. When comparing use patterns of individuals reporting a chronic mental health condition to those without, users with a mental health condition (N = 57, M = 10.67, SD = 10.76) used cannabis on more days than those without a mental health condition (N = 56, M = 6.66, SD = 8.42), t(105.76) = 2.21, p < .05 (correcting for unequal variance; see Figure 1). In contrast, there was no difference in days of alcohol use for those with and without mental health conditions.
Figure 1. Past 30 day cannabis use for those with and without a mental health diagnosis.
Motivations for Alcohol and Cannabis Use
We asked participants explicitly if they were using alcohol or cannabis to alleviate symptoms of their chronic, diagnosed health conditions. Chi-square analyses indicate that participants diagnosed with a chronic physical health condition were no more likely to use alcohol to alleviate the symptoms of their condition. However, those with a chronic mental health condition were more likely to indicate using alcohol to alleviate symptoms, χ² (N = 208, df = 1) = 20.62, p < .001.
Cannabis use, on the other hand, was associated with symptom alleviation for participants with physical and mental health conditions. Participants with a physical health condition were significantly more likely to report using cannabis to alleviate symptoms than those without a physical health condition, χ² (1, N = 208) = 23.15, p < .001. Participants with a mental health condition were significantly more likely to report using cannabis to alleviate symptoms than those without a mental health condition, χ² (1, N = 208) = 38.31, p < .001 (see Figure 2).

In general, among all participants, alcohol motivations are primarily social while cannabis motivations are more individual and potentially symptom-related (see Table 1). Specifically, using McNemar’s chi-square tests, we found that participants were significantly more likely to use cannabis than alcohol to alleviate pain, χ²(1, N = 209) = 11.25, p < .001, as a sleep aid, χ²(1, N = 209) = 34.57, p < .001, to increase appetite, χ²(1, N = 209) = 8.1, p < .01, and to relax, χ²(1, N = 208) = 24.81, p < .001. Participants were significantly more likely to use alcohol to get intoxicated, χ²(1, N = 209) = 4.7, p < .05, and to party with friends, χ²(1, N = 208) = 110.63, p < .001.
Table 1: Percentage of All Participants Identifying Specific Motivations for Substance Use
| Motivations | Alcohol | Cannabis | |||
|---|---|---|---|---|---|
| N | % | N | % | χ² | |
| Alleviate Physical Pain | 5 | 2.4 | 21 | 10.0 | 11.25*** |
| Insomnia/Sleep Aid | 2 | 1.0 | 42 | 20.1 | 34.57*** |
| Anxiety/Stress Relief | 61 | 29.2 | 80 | 38.3 | 3.81 |
| Relieve Nausea | 0 | 0.0 | 2 | 1.0 | — |
| Increase Appetite | 1 | 0.5 | 11 | 5.3 | 8.10** |
| Get Intoxicated | 126 | 60.3 | 107 | 51.2 | 4.70* |
| Party with Friends | 190 | 90.9 | 69 | 33.0 | 110.63*** |
| Relax | 66 | 31.6 | 118 | 56.5 | 24.81*** |
| Fit in with Friends | 41 | 19.6 | 28 | 13.4 | 3.35 |
There are also differences in motivations depending on mental or physical health conditions. Participants with physical health conditions were significantly more likely to endorse pain alleviation as a motive for cannabis use than those without, χ²(1, N = 209) = 3.92, p < .05; those with mental health conditions are more likely to endorse relaxation as a motive for alcohol use than those without, χ²(1, N =209) = 3.99, p < .05.
Within these groups, there were different motivations for using each substance (see Table 2). Those with physical health conditions were more likely to endorse cannabis use than alcohol use to alleviate physical pain, χ²(1, N = 37) = 4.17, p < .05, and to relax, χ²(1, N = 36) = 4.05, p < .05. They were more likely to endorse alcohol use to party with friends, χ²(1, N = 36) = 14.09, p < .001. Those reporting mental health conditions were more likely to use cannabis than alcohol as a sleep aid, χ²(1, N = 96) = 13.47, p < .001, and to relax, χ²(1, N = 95) = 6.02, p < .05.
Like those reporting physical health conditions, those with mental health conditions were more likely to use alcohol than cannabis to party with friends, χ²(1, N = 96) = 42.48, p < .001. Similar results were also seen among participants who reported no chronic health conditions. These participants were also more likely to use cannabis as a sleep aid, χ²(1, N = 104) = 18.38, p < .001 and to relax, χ²(1, N = 104) = 17.42, p < .001. They were more likely to use alcohol than cannabis to party with friends, χ²(1, N = 104) = 68.01, p < .001 and to get intoxicated, χ²(1, N = 104) = 4.36, p < .05.
While all three groups were more likely to report their cannabis use as motivated by relaxation, all groups were equally likely to use cannabis and alcohol to relieve stress/anxiety, indicating a clear distinction between these related motives. Comparisons could not be made across these three groups as the mental and physical health groups are not mutually exclusive. However, the patterns of endorsement are sufficiently similar to suggest that these are the more important factors.
Table 2: Percentage of Participants Identifying Specific Motivations for Substance Use Across Health Status
| Motivations | Chronic Physical Health Condition (N=37) | Chronic Mental Health Condition (N = 96) | No Chronic Health Condition (N = 104) | |||
|---|---|---|---|---|---|---|
| Alcohol | Cannabis | Alcohol | Cannabis | Alcohol | Cannabis | |
| N | % | N | % | N | % | |
| Alleviate Physical Pain | 1 | 2.7 | 7 | 18.9* | 0 | 0.0 |
| Insomnia/Sleep Aid | 1 | 2.7 | 5 | 13.5 | 1 | 1.0 |
| Anxiety/Stress Relief | 14 | 37.8 | 16 | 43.2 | 31 | 32.3 |
| Relieve Nausea | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Increase Appetite | 0 | 0.0 | 3 | 8.1 | 0 | 0.0 |
| Get Intoxicated | 24 | 64.9 | 22 | 59.5 | 57 | 59.4 |
| Party with Friends | 34 | 91.9 | 14 | 37.8** | 85 | 88.5 |
| Relax | 12 | 32.4 | 21 | 56.8* | 37 | 38.5 |
| Fit in with Friends | 7 | 18.9 | 6 | 16.3 | 17 | 17.7 |
* p < .05, ** p < .001
Discussion
Our study appears to be the first to directly compare use rates and self-medication motives for alcohol and cannabis in college students with and without a diagnosed chronic mental or physical health condition. Having a physical health condition was not associated with greater consumption of alcohol or cannabis in our sample. And while students with a diagnosed mental health condition used alcohol at similar rates to those without, they used cannabis, on average, four more times per week. This is concerning not only because greater use is associated with the development of CUD, but also because people with pre-existing mental health conditions, including anxiety, depression, psychosis, and bipolar disorder are at increased risk for cannabis-induced psychosis, a rare, but serious condition that often requires hospitalization.²⁵ Importantly, the relationship between cannabis use and psychosis does not seem to be the result of people who already have psychosis using cannabis as a form of self-medication for their symptoms.²⁶ Moreover, although the literature is mixed, some studies suggest that, despite the common perception by college students that cannabis has anxiolytic properties,²⁷ it may actually exacerbate anxiety.²⁸ Taken together, these findings suggest that psychoeducation regarding the risks of cannabis use in those with certain mental health conditions is warranted.
Much of the prior research on “self-medication” motives seems to have conflated coping motives with self-medication. While the “coping” subscale of the MMM and the “sleep”, “coping”, and “social anxiety” subscales of the CMMM likely capture instances of self-medication for diagnosed cases of anxiety, depression, and sleep disturbances, they also likely capture many instances of cannabis use for the amelioration of subclinical mood and sleep disturbances due to everyday worries and stressors. An advantage of the current study is that, unlike previous studies that inferred self-medication motives through correlations between health conditions and coping motives, we asked participants explicitly if they were using alcohol or cannabis to alleviate symptoms of their chronic, diagnosed health conditions. We found that students with a mental health condition intentionally use both alcohol and cannabis to alleviate or reduce their symptoms, while those with a physical health condition self-medicate with cannabis but not alcohol. All participants, regardless of whether they had a formal health diagnosis, were more likely to use cannabis than alcohol therapeutically as a sleep aid, to increase appetite, and for pain relief.
Considering use patterns and motives in combination, we see that cannabis and alcohol seem to serve different purposes. Participants use alcohol infrequently (about once per week) and usually with friends; When describing their motives for using alcohol, participants endorsed “to get intoxicated” and “to party with friends” at high rates. On the other hand, students use cannabis nearly twice as often and for a broader range of reasons, as indexed by a larger number of motives being selected, but with a lower probability of being used to get intoxicated or to party with friends. This suggests that cannabis may not be viewed as a party drug in the same way that alcohol is, and instead (or in addition) is viewed as a therapeutically useful drug, especially by people with chronic mental and physical health conditions. Intentional therapeutic use of cannabis may contribute to its relatively frequent use compared to alcohol. Future studies should continue to explore the unique circumstances under which each substance is likely to be used.
Interestingly, cannabis users taking conventional pharmaceuticals for a chronic condition used cannabis (but not alcohol) marginally more frequently than those not taking medication. We might have hoped that those taking medication would report using significantly less of both substances since they are contraindicated with many medications. Moreover, we had speculated
that lack of access to conventional medical care might increase the appeal of self-medication with cannabis, which would have been associated with the opposite relationship between taking prescription medication and self-medication with cannabis. Of course, the severity of many chronic conditions exists on a continuum, and it is possible that those who take prescription medications for their chronic conditions are living with more severe conditions than those who are not, and that their symptoms are not fully alleviated by conventional treatments. It is also the case that many chronic conditions have multiple symptoms and that the prescription medication our participants were taking did not adequately address them all. Another possibility still is that conventional medications are causing unpleasant side effects from which people seek relief with cannabis. For example, stimulant medications used to treat Attention Deficit Hyperactivity Disorder (ADHD) are known to interfere with sleep, as might antidepressants for those on cannabis as a sleep aid. In any case, lack of access to conventional medical care does not neatly explain the high rate of cannabis self-medication in our sample, nor the positive relationship between prescription medication use and cannabis self-medication. A goal of future studies will be to inquire specifically about the symptoms participants are seeking to relieve through cannabis self-medication to determine if they are the same ones for which they administer prescription pharmaceuticals.
If not for lack of access to traditional healthcare, then why are the college students in our sample willing to self-medicate their chronic conditions despite there being little empirical evidence of its safety and efficacy? Perhaps it is due to the same developmental and contextual factors that lead to higher than average rates of all substance use in people this age. Adolescence and early adulthood are developmental periods marked by sensation seeking, risk taking, and feelings of invincibility.²⁹ ³⁰ At the same time, college provides less parental oversight and increased access to drugs and alcohol. This combination creates conditions that are highly conducive to drug and alcohol use; Perhaps students discover incidentally through frequent recreational cannabis use that it alleviates symptoms of their mental and physical health issues. Another factor may be the relatively greater exposure that young adults have to cannabis advertising, which is associated with positive expectations of cannabis and the perception that cannabis has proven medical benefits.²³ Since expectancies fuel behavior, future research ought to explore this. Moreover, because coping motives are predictive of problematic cannabis use,²⁴ ³¹ and because coping is closely related to self-medication (it might reasonably be seen as a specific instance of self-medication in an effort to alleviate negative affect), it will be important to determine if self-medication motives are related to the likelihood of developing a CUD and what variables (apart from a chronic health diagnosis) are related to a college student’s likelihood of self-medicating with cannabis.
Our study was not without limitations. Our sample had a high percentage of people with mental health problems — higher than the percentage found for young adults in the most recent SAMHSA report.² The SAMHSA study included young adults who are not in college, and that could make a difference given the sociocultural differences that exist between those two groups. Additionally, our participants attend a small, selective liberal arts school, and thus the participant pool includes a disproportionate number of students who come from a privileged socioeconomic background. It is possible that this privilege gives them greater access to mental health care, and thus diagnoses. Moreover, due to the low professor to student ratio, institutions of this nature may attract students who desire greater support from faculty, which might coincide with mental health problems.
Conclusion
Results from the current study suggest that college students living with a chronic mental health condition may turn to cannabis to help ameliorate their symptoms even when they are taking prescription medications for their ailment. While the patterns of and motivations for use varied among participants with and without chronic health conditions, cannabis was endorsed much more often than alcohol as a sleep aid, for appetite stimulation, for pain control, and to help students relax. Alcohol emerged as a less therapeutic and more social drug, being endorsed much more often than cannabis as the substance of choice for partying with friends and getting intoxicated.
Because the rate of chronic mental illness for those aged 18–34 is high, it is crucial to continue examining how young adults cope with the difficult mental health symptoms they face. By further clarifying the motivations for self-medicating with alcohol and cannabis, we may come closer to discovering therapeutic gaps in commonly used prescriptions to treat mental illnesses. Addressing these gaps could help to decrease the incentive for young adults to use alcohol and cannabis as a form of self-medication, ultimately protecting them from the harmful consequences of frequent and prolonged substance use.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
No financial disclosure.
Acknowledgements:
No acknowledgements
References
1. Watson KB, Wiltz JL, Nhim K, Kaufmann RB, Thomas CW, Greenlund KJ. Trends in Multiple Chronic Conditions Among US Adults, By Life Stage, Behavioral Risk Factor Surveillance System, 2013–2023. Prev Chronic Dis. 2025;22. doi:10.5888/pcd22.240539
2. Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2023 National Survey on Drug Use and Health. 2023 NSDUH Annual National Report. July 30, 2024. Accessed July 21, 2025. https://www.samhsa.g. ov/data/report/2023-nsduh-annual-national-report.
3. Paus T, Keshavan M, Giedd JN. Why Do Many Psychiatric Disorders Emerge During Adolescence? Nat Rev Neurosci. 2008;9(12):947-957. doi:10.1038/nrn2513
4. Qiu A, Liu C. Pathways link environmental and genetic factors with Structural Brain Networks and psychopathology in Youth. Neuropsychopharmacol. 2023;48(7):1042-1051. doi:10.1038/s41386-023-01559-7
5. Hicks TA, Bountress KE, Adkins AE, et al. A longitudinal mediational investigation of risk pathways among cannabis use, interpersonal trauma exposure, and trauma-related distress. Psychol Trauma. 2023;15(6):969-978. doi:10.1037/tra0001207
6. The Growing Burden of Chronic Diseases. NIHCM. April 3, 2025. Accessed July 21, 2025.
https://nihcm.org/publications/the-growing-burden-of-chronic-diseases.
7. Brenan M. View of U.S. Healthcare Quality Declines to 24-Year Low. Gallup.com. December 6, 2024. Accessed July 21, 2025.
https://news.gallup.com/poll/654044/view-healthcare-quality-declines-year-low.aspx.
8. Blume AW, Schmaling KB, Marlatt GA. Revisiting the self-medication hypothesis from a behavioral perspective. Cogn Behav Pract. 2000;7(4):379-384. doi:10.1016/s1077-7229(00)80048-6
9. Turner S, Mota N, Bolton J, Sareen J. Self-medication with alcohol or drugs for mood and anxiety disorders: A narrative review of the epidemiological literature. Depress Anxiety. 2018;35(9):851-860. doi:10.1002/da.22771
10. Goodhines PA, Gellis LA, Kim J, Fucito LM, Park A. Self-Medication for Sleep in College Students: Concurrent and Prospective Associations With Sleep and Alcohol Behavior. Behav Sleep Med. 2017;17(3):327-341. doi:10.1080/15402002.2017.1357119
11. Alford DP, German JS, Samet JH, Cheng DM, Lloyd-Travaglini CA, Saitz R. Primary Care Patients with Drug Use Report Chronic Pain and Self-Medicate with Alcohol and Other Drugs. J Gen Intern Med. 2016;31(5):486-491. doi:10.1007/s11606-016-3586-5
12. Leung J, Chan G, Stjepanović D, Chung JY, Hall W, Hammond D. Prevalence and self-reported reasons of cannabis use for medical purposes in USA and Canada. Psychopharmacology (Berl). 2022;239(5):1509-1519. doi:10.1007/s00213-021-06047-8
13. Tran D-MT, Silvestri-Elmore A. Healthcare-seeking behaviours in college students and Young Adults: A Review. J Res Nurs. 2020;26(4):320-338. doi:10.1177/1744987120951594
14. Chambers J, Keyhani S, Ling PM, et al. Perceptions of Safety of Daily Cannabis vs Tobacco Smoking and Secondhand Smoke Exposure. JAMA Netw Open. 2023;6(8). doi:10.1001/jamanetworkopen.2023.28691
15. Wallis D, Coatsworth JD, Mennis J, et al. Predicting Self-Medication with Cannabis in Young Adults with Hazardous Cannabis Use. Int J Environ Res Public Health. 2022;19(3):1850. doi:10.3390/ijerph19031850
16. Drazdowski TK, Kliewer WL, Marzell M. College students’ using marijuana to sleep relates to frequency, problematic use, and sleep problems. J Am Coll Health. 2019;69(1):103-112. doi:10.1080/07448481.2019.1656634
17. Millin P, Klace F, Krieg D. A Comparative Analysis of the Frequency and Motivations for Cannabis Use in College Students With & Without an Autoimmune Disease. Med Res Arch. 2023;11(11). doi:10.18103/mra.v11i11.4674
18. Simons J, Correia CJ, Carey KB, Borsari BE. Validating a five-factor marijuana motives measure: Relations with use, problems, and alcohol motives. J Couns Psychol. 1998;45(3):265-273. doi:10.1037//0022-0167.45.3.265
19. Cooper ML. Motivations for Alcohol Use Among Adolescents: Development and Validation of a Four-Factor Model. Psychol Assess. 1994;6(2):117-128. doi:10.1037/1040-3590.6.2.117
20. Lee CM, Neighbors C, Woods BA. Marijuana motives: Young adults’ reasons for using marijuana. Addict Behav. 2007;32(7):1384-1394. doi:10.1016/j.addbeh.2006.09.010
21. Lee CM, Neighbors C, Hendershot CS, Grossbard JR. Development and preliminary validation of a comprehensive marijuana motives questionnaire. J Stud Alcohol Drugs. 2009;70(2):279-287. doi:10.15288/jsad.2009.70.279
22. Han B, Shi Y. Associations of recreational cannabis dispensaries’ availability, storefront signage and health benefit signs with cannabis use: findings from a representative adult sample in California, United States. Addiction. 2023;118(7):1270-1279. doi:10.1111/add.16132
23. Cohn AM, Alexander AC, Ehlke SJ, et al. Seeing is believing: How cannabis marketing exposure is associated with cannabis use attitudes and behavior in a permissive medical cannabis policy environment. Am J Addict. 2023;32(4):333-342. doi:10.1111/ajad.13390
24. Moitra E, Christopher PP, Anderson BJ, Stein MD. Coping-motivated marijuana use correlates with DSM-5 cannabis use disorder and psychological distress among emerging adults. Psychol Addict Behav. 2015;29(3):627-632. doi:10.1037/adb0000083
25. Schoeler T, Ferris J, Winstock AR. Rates and correlates of cannabis-associated psychotic symptoms in over 230,000 people who use cannabis. Transl Psychiatry. 2022;12(1). doi:10.1038/s41398-022-02112-8
26. Hall W, Degenhardt L. Cannabis use and the risk of developing a psychiatric disorder. World Psychiatry. 2008;7(2)68-71. doi: 10.1002/j.2051-5545.2008.tb00158.x
27. Blyth LG, Seal C, Sorkhou M, Lowe DJ, George TP. A Systematic Review of Cannabis and Anxiety: Chicken or Egg? Curr Addict Rep. 2025;12(1). doi:10.1007/s40429-025-00650-x
28. Lowe DJ, Sasiadek JD, Coles AS, George TP. Cannabis and Mental Illness: A Review. Eur Arch of Psychiatry Clin Neurosci. 2018;269(1):107-120. doi:10.1007/s00406-018-0970-7
29. Kennedy S, Millin P, Kennedy GJ. A Preliminary Study Examining Self-Reported Invincibility, Alcohol Problems, and the Nonmedical Use of Prescription Stimulants in College Students. J Drug Issues. 2021;52(1):3-14. doi:10.1177/00220426211037267
30. Ravert RD, Schwartz SJ, Zamboanga BL, Kim SY, Weisskirch RS, Bersamin M. Sensation seeking and danger invulnerability: Paths to college student risk-taking. Pers Individ Dif. 2009 Nov;47(7):763-768. doi: 10.1016/j.paid.2009.06.017.
31. Brammer WA, Conn BM, Iverson E, Lankenau SE, Dodson C, Wong CF. Coping Motives Mediate the Association of Trauma History with Problematic Cannabis Use in Young Adult Medical Cannabis Patients and Non-Patient Cannabis Users. Subst Use Misuse. 2022;57(5):684-697. doi: 10.1080/10826084.2022.2026970