






Telehealth Collaboration: Enhancing Pharmacy Education
A Telehealth Collaboration Between a Regional Veterans Affairs Primary Care System and a School of Pharmacy: Key Outcomes from 2024
Sian M. Carr-Lopez, PharmD¹; Randell K. Miyahara, PharmD¹²; Rajul A. Patel, PharmD, PhD³⁴; Allen Shek, PharmD⁴⁵; Yvonne T. Mai, PharmD, MS⁴⁶; Elaine J. Law, PharmD⁴⁷; Jaime K. Chew, PharmD⁸
- Clinical Professor, Thomas J. Long School of Pharmacy, University of the Pacific, Stockton, CA
- Population Health Program Manager, Primary Care Service, VA Northern California Health Care System, Mather, CA
- Professor, Thomas J. Long School of Pharmacy, University of the Pacific, Stockton, CA
- Clinical Pharmacist, Population Health Program, Primary Care Service, VA Northern California Health Care System, Mather, CA
- Professor and Associate Dean, Thomas J. Long School of Pharmacy, University of the Pacific, Stockton, CA
- Associate Professor, Thomas J. Long School of Pharmacy, University of the Pacific, Stockton, CA
- Associate Clinical Professor, Thomas J. Long School of Pharmacy, University of the Pacific, Stockton, CA
- Associate Chief of Pharmacy, Primary Care Service, VA Northern California Health Care System, Mather, CA
OPEN ACCESS
PUBLISHED:31 May 2025
CITATION: Carr-Lopez, SM., Miyahara, RK., et al., 2025. A Telehealth Collaboration Between a Regional Veterans Affairs Primary Care System and a School of Pharmacy: Key Outcomes from 2024. Medical Research Archives, [online] 13(5).
https://doi.org/10.18103/mra.v13i5.6493
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6493
ISSN 2375-1924
Abstract
Background: The Veterans Health Administration is the largest integrated healthcare system in the United States, delivering services to more than 9.1 million Veterans across 1,380 facilities. We describe a partnership with a regional Veterans Affairs (VA) healthcare system and a health professional school.
Methods: The VA Northern California Health Care System, in collaboration with the University of the Pacific, Thomas J. Long School of Pharmacy, implemented a remote population health management course for pharmacy students. The course combined didactic and experiential learning, utilizing remote access to VA electronic health records and clinical dashboards to conduct telehealth activities focused on diabetes, cancer screenings, and opioid safety. A time and motion analysis evaluated the time the students saved the healthcare system. Pre- and post-course assessments evaluated students’ knowledge and confidence in performing telehealth activities.
Results: In 2024, 126 students participated in the course, collectively saving 377.5 hours of healthcare system labor. Analysis of pre- and post-course assessments revealed statistically significant improvements in students’ knowledge and confidence related to course activities and population health initiatives.
Conclusions: These findings demonstrate the effectiveness of a scalable telehealth course model in enhancing student learning while supporting population health management efforts within a healthcare system.
Keywords
Telehealth, Veterans Affairs, pharmacy education, population health, healthcare collaboration
Introduction
Summary of the Veterans Health Administration and Primary Care Practice Model
The Veterans Health Administration is the largest integrated healthcare system in the United States (U.S.), delivering services through 1,380 healthcare facilities, including 170 Veterans Affairs (VA) medical centers and 1,193 outpatient sites to more than 9.1 million Veterans enrolled in the VA healthcare program.
In 2010, the VA began implementing the Primary Care Medical Home model across all its primary care clinics.
The VA delivers primary care to Veterans through an interprofessional Patient Aligned Care Team (PACT), which consists of a primary care provider, registered nurse, licensed practical nurse or medical assistant, clinical pharmacist practitioner, social worker, dietitian, mental health professional, and administrative clerk.
Telehealth Services within the Veterans Health Administration and Interprofessional Training
The VA launched telehealth services in 2003. During the COVID-19 pandemic, the VA saw a dramatic surge in video visits, which increased by 3,000%. In 2024, approximately 40% of Veterans received at least a portion of their care from the VA via telehealth.
The VA operates one of the largest interprofessional training programs in the U.S., annually educating over 122,000 health professional trainees across more than 60 professions including physicians, nurses and associated health professions. A survey of 10,865 health professional trainees who trained within the VA during the 2023 academic year revealed generally neutral to positive perceptions of telehealth and virtual supervision in VA facilities. Among the associated health professions group, pharmacy had the highest number of respondents (n = 850), with 57% reporting involvement in telehealth services.
Role of Pharmacists within the Veterans Health Administration
Until the introduction of Collaborative Drug Therapy Management (CDTM) in the 1960s and 1970s by the U.S. Public Health Service’s Indian Health Service, federal pharmacists primarily served in traditional roles, such as dispensing medications and providing patient education and drug information. Collaborative Drug Therapy Management can be defined as an agreement between one or more physicians and a clinical pharmacist, granting the pharmacist professional responsibility for performing patient assessments, ordering relevant laboratory tests, monitoring medication therapy, and initiating, modifying, and discontinuing medications. In the VA, CDTM is codified by a scope of practice. While all pharmacists within the VA can engage in traditional pharmacy activities such as dispensing medication, counseling patients, performing medication reconciliation and chart reviews, and monitoring and assessing drug therapy to provide recommendations, a scope of practice is required for pharmacists to independently manage chronic conditions through CDTM. This includes prescribing medications, ordering laboratory tests and diagnostic studies, performing physical measurements and objective assessments, making referrals, and carrying out other essential patient care functions. The VA utilizes this practice model to help mitigate the national shortage of primary care providers and to capitalize on published evidence showing that clinical pharmacist practitioners can improve clinical outcomes and reduce overall health care costs.
The Veterans Health Administration Population Health Initiatives
Opioid Safety
Veterans enrolled in VA programs experience chronic pain at higher rates than the general U.S. adult population. The presence of certain conditions is linked to high-dose opioid use and increased overdose risk compared to the general population; these conditions include posttraumatic stress disorder, major depressive disorder, alcohol use and a history of suicide attempts. Veterans face a significantly higher risk of accidental overdose, with rates nearly twice that of the non-Veteran population. The VA launched the Opioid Safety Initiative in 2013 to reduce inappropriate use of opioids and enhance the care of Veterans with chronic pain. This initiative takes a comprehensive, interdisciplinary approach, with pharmacists playing a key role in efforts to minimize pain and the risks linked to chronic opioid therapy. In alignment with these efforts, in 2022 the Centers for Disease Control and Prevention (CDC), along with the VA and Department of Defense, updated clinical guidelines for opioid prescribing. These guidelines emphasize thorough pain assessments, regular urine drug screenings, initial and periodic review of prescription drug monitoring program (PDMP) data, pharmacist collaboration, and referrals to specialists such as pain clinical pharmacists for advanced pain management. Given the evolving landscape of pain management, pharmacy students must be equipped to contribute meaningfully to the care of patients receiving chronic opioid therapy.
Diabetes Monitoring and Cancer Screening
Women are the fastest growing group of Veterans, with over 600,000 women (44% of women Veterans) using VA services. Women’s health initiatives such as screening for breast and cervical cancer are a priority for the VA. Diabetes monitoring is critical to ensure optimal disease management and to prevent micro- and macro-vascular complications. Within the VA, patients with diabetes require annual hemoglobin A1c, microalbuminuria, and LDL-cholesterol testing. Clinical dashboards assist clinicians in identifying patients needing laboratory monitoring for diabetes mellitus or cancer screenings. In addition to VA healthcare facilities, Veterans may receive health care at U.S. Department of Defense and/or non-federal healthcare systems. The Joint Longitudinal Viewer (JLV) is a clinical application that provides a read-only display of health data from participating healthcare systems. Clinicians access JLV to incorporate real-time medical data from other healthcare systems in the treatment of their patients. The use of JLV facilitates follow-up care and avoids duplication of tests and screenings, which is advantageous for the healthcare system as well as the patient. Priority initiatives such as diabetes monitoring and breast and cervical cancer screening are supported by searching JLV for testing and screening results conducted at non-VA facilities. These activities help the healthcare system prevent unnecessary testing and cancer screenings, leading to lower costs and reduced workload associated with ordering and interpreting these tests.
Rationale for Innovative Partnerships
As telehealth services become more widespread it is essential to equip health professional trainees with the skills needed to effectively provide virtual patient care. The Association of American Medical Colleges has identified core telehealth competencies in its publication Telehealth Competencies Across the Learning Continuum, which also includes curriculum frameworks. In pharmacy education, the 2022 revision of the American Association of Colleges of Pharmacy’s Curriculum Outcomes and Entrustable Professional Activities (COEPA) included “seek, analyze, integrate, and apply foundational knowledge of digital health.” This underscores the increasing importance of incorporating digital health into the education of future health professionals. Health professional education is typically divided into preclinical training, conducted at schools or universities, and clinical training, which occurs within healthcare settings. Telehealth technology enables students to engage in patient care remotely at the university, without traveling to a healthcare facility.
Herein, we present a telehealth program designed to enhance student learning while supporting a regional VA primary care system with population health management activities. The purpose of this paper is to describe the outcomes during a single year by a cohort of students using telehealth modalities on three specific initiatives: monitoring laboratory parameters for patients with diabetes, cancer screening in women, and opioid safety monitoring. We report the amount of time the program saved for the primary care team and the results of an analysis of pre- and post-course assessments evaluating students’ knowledge and confidence related to the course objectives.
We present a scalable, collaborative model that allows health professional schools to introduce students to telehealth and population health training early in their education, leveraging university-based resources. Healthcare sites gain the advantage of student support on priority health initiatives without requiring space or onsite supervision at the healthcare facility.
Methods
Course Development and Design
A collaboration between the VA Northern California Health Care System Primary Care Service and the University of the Pacific, Thomas J. Long School of Pharmacy for population health management began in 2016. As part of this initiative, a remote telehealth course focusing on population health was established exclusively at the school, granting students and preceptors remote access to the VA’s electronic health record (EHR), Computerized Patient Record System (CPRS). To enhance clinical quality performance measures, the VA developed population management dashboards designed to identify Veterans in need of clinical interventions. The primary care dashboard includes features such as identifying patients who require PDMP reviews, diabetes monitoring, and cancer screenings.
Pharmacy students were assigned population management tasks typically performed by PACT members. Using university-issued laptops and VA-issued cell phones, students conducted PDMP activities, reviewed external medical records, ordered laboratory tests for prescriber approval, contacted patients to assess pain, and documented progress notes. To ensure proper supervision, the VA Primary Care Service hired and credentialed pharmacy practice faculty from the university, allowing students to be overseen by VA Clinical Pharmacist Practitioners.
Beginning in 2018, the telehealth introductory practice experience became a 1-unit required experiential course for second-year professional students, offered each semester within the tri-semester curriculum. In 2024, the course included approximately five hours of didactic and 25 hours of experiential learning, with enrollment ranging from approximately 40 to 50 students per semester. To accommodate these students, four 2-hour sessions were held weekly, each supervised by three to four pharmacist preceptors.
Before the start of each semester, students were processed as VA employees without compensation and completed necessary paperwork, fingerprinting for background checks, and online training in privacy, security, and the Health Insurance Portability and Accountability Act. Once the semester began, students received personal identity verification cards and remote access to CPRS using their university-issued laptops.
Students received an overview of the course, including expectations for professionalism, VA workflows, and navigation of the VA’s EHR and population management dashboards. These dashboards were utilized to identify patients requiring laboratory monitoring, cancer screening, opioid prescription drug monitoring, or pain assessments.
Didactic materials covered laboratory monitoring requirements for diabetes management, breast and cervical cancer screening recommendations and reporting, an overview of the VA Opioid Safety Initiative, the CDC guidelines for prescribing opioids for chronic pain, and the interpretation of PDMP and urine drug screen results. Additionally, students were trained to assess pain using a validated three-item questionnaire.
Student Activities
Students had both longitudinal (PDMP assessments) and intermittent (all other initiatives) patient care responsibilities throughout the semester.
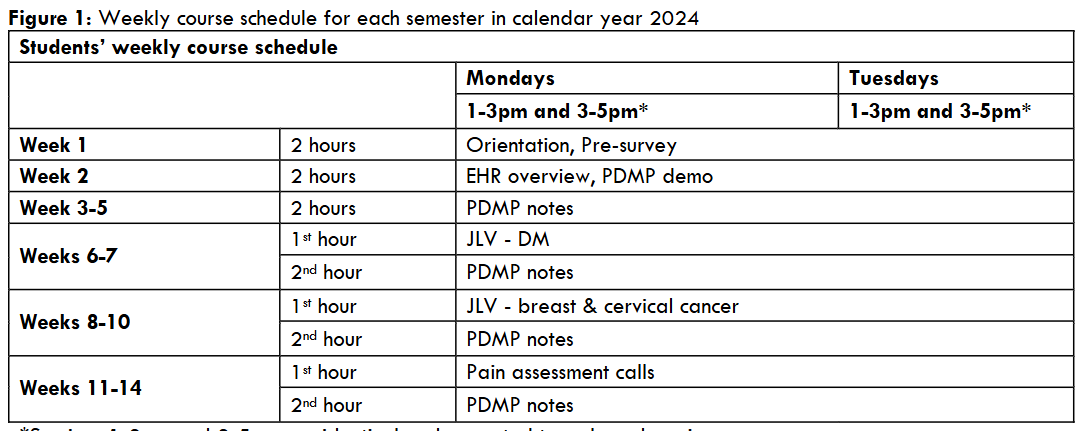
Students’ weekly course schedule
At the start of each class session, students were assigned patients requiring a PDMP assessment. They reviewed state PDMP records for prescriptions issued by non-VA providers, categorizing results as either positive or negative for non-VA controlled substance prescriptions. If positive, students reviewed health records to determine whether the prescription was appropriately indicated (e.g., documented in CPRS as being filled outside the VA) or if it raised concerns regarding adverse effects, aberrant behavior, overdose risk, substance use disorder, or potential diversion. As part of their assessment, students also reviewed the most recent urine drug screen results. Each patient case was discussed with a preceptor, after which students documented their findings in a standardized progress note. They included the preceptor and prescriber as co-signers before finalizing the note.
Students utilized JLV, a clinical application that integrates health data from the Department of Defense, the VA, and private health system partners, to search for outside medical records. The process for required laboratory monitoring varied depending on whether recent laboratory results were available in JLV. Similarly, JLV was searched for outside mammogram and cervical cancer screenings test results. For both diabetes and cancer initiatives, students entered relevant results found in JLV into CPRS. For the diabetes initiative, if outside results were unavailable, students reviewed CPRS for pending tests and if absent, ordered necessary laboratory tests for prescriber approval and sent laboratory reminder letters to Veterans.
For pain assessments, students contacted Veterans using VA-issued cell phones under the guidance of a preceptor. Before initiating calls, they rehearsed the pain assessment script with their preceptors who also reviewed the facility’s “urgent symptoms” list to ensure appropriate escalation of any concerning findings to the facility’s call center. During the calls, students administered a validated three-item questionnaire and documented responses in CPRS.
All student work was conducted under close preceptor supervision, with no laboratory orders or progress notes finalized without preceptor review and approval. Furthermore, all calls to Veterans were made with a preceptor directly supervising the interaction. All approved and completed notes had the patient’s primary care provider or prescriber added as an additional signer to notify them of the additional information found.
Student Outcomes
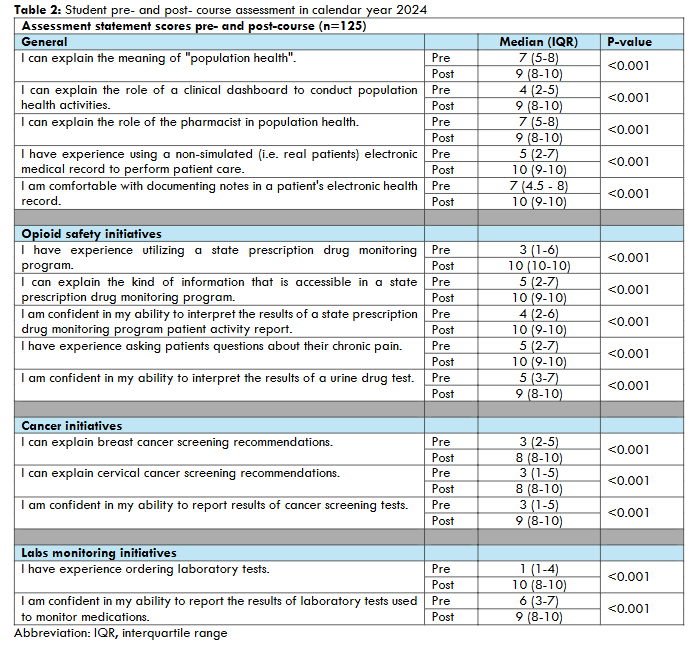
Students completed both pre- and post-course assessments containing statement-based questions aimed at evaluating their knowledge, attitudes, and experiences related to population health activities. Responses were measured using a 10-point Likert scale (1 = Strongly Disagree to 10 = Strongly Agree). Changes in student self-assessment responses from baseline (pre) to course completion (post) were analyzed using Wilcoxon signed-rank tests. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered statistically significant.
Data Collection and Analysis
Students were required to log all patient care activities performed. For each assigned patient, students recorded their activities such as successfully completing a pain assessment call or identifying whether the PDMP review yielded positive or negative findings. This was in addition to documenting progress notes within the electronic health record. Students recorded the number and outcomes of PDMP reviews, the number of completed pain assessments, the results from outside record reviews from JLV, number of laboratory tests ordered, and number of reminder letters sent to patients to complete laboratory tests. All entries were verified by a pharmacist preceptor. Pharmacy student activities were documented throughout the 2024 calendar year.
A time and motion study was performed, whereby the PACT team member was timed while conducting the activities that would be assigned to students. The average time it took PACT team members to complete each activity was recorded. A detailed description of the time and motion study is reported elsewhere. We calculated the time the students saved for the PACT team in calendar year 2024. To estimate the total time saved for each activity, the frequency of each student-completed activity was multiplied by its corresponding average time to complete. Time saved for each activity was totaled; this calculation reflects the total time saved by having students perform these activities in lieu of the PACT team members. One activity was excluded from the time and motion study. Reviewing outside records in JLV did not always produce results. If results were not found, the time spent on the activity was not included in the analysis. This project was submitted to the VA Northern California Health Care System’s Institutional Review Board who determined that reporting this data is not research based and was exempt from Research Service approval or monitoring.
Results
In the 2024 calendar year, a total of 126 students participated in the telehealth course.
| Activity type | Total frequency of activity in 2024 | Total time saved (hours) | ||
|---|---|---|---|---|
| Opioid safety | ||||
| PDMP initiative (31 weeks) | Negative PDMP notes | 3677 | 122.6 | |
| Positive PDMP notes | 328 | 32.8 | ||
| Phone pain assessment (10 weeks) | 840 | 84.0 | ||
| JLV queries | ||||
| Cancer screening initiatives (7 weeks) | Breast cancer data notes documented | 90 | 39.0 | |
| Cervical cancer data notes documented | 170 | |||
| Lab monitoring initiatives (8 weeks) | JLV labs found* | 365 | 25.1 | |
| JLV lab notes documented | 167 | |||
| Ordering labs for providers if not found in JLV | Lab tests ordered* | 1535 | 74.0 | |
| Patient lab reminder letter sent | 634 | |||
| Total | 377.5 |
Of the 126 students, 125 (99.2%) completed both the pre- and post-course assessment. Table 2 presents the 15 statement-based assessment questions, categorized by initiative type, along with the median score for each question at both baseline and course completion. A comparison of pre- and post-course survey responses revealed improvements in students’ understanding of population health, as well as their knowledge and confidence related to key initiatives. There was a significant increase in student agreement for all statements (p <0.001), including those related to confidence in performing specific skills and explaining specific concepts. The most notable change occurred for the statement “I have experience ordering laboratory tests” which had a median score of 1 at baseline and 10 at course completion. Other notable changes included the statements “I have experience utilizing a state prescription drug monitoring program” which had a median score of 3 at baseline and 10 at course completion, and “I am confident in my ability to report results of cancer screening tests” which had a median score of 3 at baseline and 9 at course completion.
Discussion
The Role of Telehealth in the Era Following the Coronavirus Disease 2019 (COVID-19) Pandemic
In the U.S., telemedicine use among office-based physicians rose dramatically during the COVID-19 pandemic. Data from the National Electronic Health Record Survey (2018-2021) show that by 2021, nearly 87% of office-based physicians had adopted some form of telemedicine, a sharp rise from just 15% in the two years prior. Office-based physicians working in medical or academic health centers reported the highest adoption rate at 98%. Among specialties, primary care physicians led with 91% utilization, followed by medical specialists at 87%, and surgical specialists at 75%. Notably, over 80% of office-based physicians planned to continue using telemedicine beyond the pandemic.
A systematic review of 102 peer-reviewed articles examined the global adoption of telehealth and telemedicine in the post-COVID-19 era. From 2019 to 2023, there has been a significant global effort to implement and expand these services. Among 77 countries analyzed out of 195 countries worldwide, 27 (13.8%) were identified as being in the advanced stage of adoption, 20 (10.3%) had reached a developed level and 24 (12.3%) were in the developing stage of utilization.
Gullseltt et al summarized findings from the Telehealth Programmes section of the 2022 World Health Organization (WHO) Survey on Digital Health (2022 WHO/Europe DH Survey). Among the 53 Member States in the WHO European Region, the COVID-19 pandemic catalyzed the rapid adoption of various telehealth modalities. By 2022, the most well-established telehealth services, defined as operational for at least two years with continued use expected for at least another two years, included teleradiology, telepsychiatry, telemedicine and teledermatology. Telemedicine demonstrated the most rapid growth reportedly offered in 37/48 (77%) of responding countries. The widespread use of telemedicine technologies across the WHO European Region reflects increasing acceptance of remote health care delivery. Systematic reviews evaluating telemedicine’s effectiveness have consistently shown clear benefits in the screening, diagnosis, management, treatment, and long-term follow-up of various chronic diseases.
The Importance of Teaching the Next Generation of Telehealth Providers
The WHO defines telehealth as the delivery of health care services, where patients and providers are separated by distance. The WHO highlights the importance of establishing clear telehealth policies and strategic frameworks to support its integration into existing healthcare systems. As part of this integration, we advocate for the development of a pipeline of healthcare professionals trained in telehealth as a component of their professional education. To our knowledge, the telehealth experiential course described in this manuscript represents the longest-running preclinical population health experience of its kind offered at a health professions school in the U.S.
The U.S. Food and Drug Administration describes digital health categories such as mobile health, health information technology, wearable devices, telehealth and telemedicine, and personalized medicine. The regional digital health action plan for the WHO European Region 2023–2030 emphasizes the importance of collaboration with academic institutions and other stakeholders to ensure that digital health policies are evidence-based, adaptive and innovative. The goal is to improve health outcomes, promote sustainability of efforts and resources, and foster a culture of continuous learning to inform decision-making. One of the strategic priorities outlined in the plan is to explore how digital technologies can improve disease prevention and management. In alignment with this priority, our telehealth initiatives support cancer screening for women and aid in the management of common health conditions such as chronic pain and diabetes. The regional action plan further acknowledges that, when effectively implemented, these technologies can enhance the work of health professionals and align with national health system priorities.
Academia and Telehealth
The World Federation for Medical Education develops and updates Global Standards for Quality Improvement for Basic Medical Education. The 2015 Standards, as part of the quality development standards, emphasized the Clinical Sciences and Skills portion of medical school curriculum should evolve in response to technological developments and the changing needs of health systems, and that clinical skills training should be appropriately structured for each stage of education. The 2020 Revision further reinforced the value of incorporating well-designed digital and distance learning methods and experiences into medical education.
In the U.S., accreditation requirements stipulate the development of clear policies regarding the supervision of medical students during patient care activities, including the use of telemedicine where applicable. Similarly, the American Association of Colleges of Pharmacy’s 2022 Curriculum Outcomes and Entrustable Professional Activities (COEPA) includes the competency to “seek, analyze, integrate, and apply foundational knowledge of digital health.”
Mutual Benefits of Partnering with Academia
Telehealth course offers flexible learning options, including asynchronous chart review and direct patient contact. While working remotely at the school under the direct supervision of VA clinical pharmacists, students accessed electronic health records to review patient charts, ordered laboratory tests under a prescriber’s name, documented clinical notes, and sent laboratory reminder letters to patients. These activities are adaptable and can be adjusted in response to shifting healthcare system priorities.
At the height of the COVID -19 pandemic, the university transitioned to virtual learning, prompting modifications to the telehealth course. While the course is typically conducted at the university, students completed it from their homes for two semesters due to pandemic-related restrictions. They were granted remote access privileges to the VA’s EHR system and received supervision from VA clinical pharmacists via Microsoft Teams. Because faculty were not physically co-located with students and therefore unable to take over a phone call with a Veteran if needed, pain assessments by phone were temporarily suspended. This activity was replaced with women’s health initiatives, which involved chart reviews of breast and cervical cancer screenings conducted through the Department of Defense, other VA facilities, or private health system partners. These women’s health-focused efforts have remained a core component of our telehealth program beyond the COVID-19 pandemic.
Sharing of resources Funding, infrastructure and workforce limitations are cited as major barriers to the sustained delivery of telehealth services. Collaborating with academic partners can help mitigate some of these challenges through shared resources. The telehealth course was delivered remotely from the healthcare system, with the university contributing key infrastructure and personnel support. This included providing classroom space for course activities, laptops for student access to the EHR system, internet connectivity, and university faculty who taught the course and supervised student work.
The VA supported the initiative by supplying a limited number of phones that were shared for patient outreach, remote access to EHR systems, and access to clinical dashboards and the JLV. The VA clinical dashboards enable population health management by using EHR data to identify patients who may benefit from evidence-based care but have not yet received it. The VA also employed university faculty to oversee student activities, and provided online training in Privacy and Health Insurance Portability and Accountability Act and VA Privacy and Information Security Awareness and Rules of Behavior for all participating students.
Collaboration between healthcare systems and health professional schools ensures that initiatives are mutually relevant and beneficial. Telehealth activities should align with the priorities of the healthcare system and be appropriate for the students’ level of education. Our telehealth course is required for second-year pharmacy students, designed to reflect their current knowledge and abilities. The skills they develop include team-based interprofessional care, applied population health, medication monitoring, documentation in electronic health records, and effective patient communication using telehealth methods. These initiatives are flexible, aiming to both enhance student learning and meet the evolving needs of the healthcare system. This telehealth course primarily focused on two critical clinical areas, the opioid epidemic and the high prevalence of diabetes, along with an economic initiative to reduce the costly duplication of screening and monitoring tests across different healthcare institutions.
Students receive hands-on, experiential training in telehealth at the school, eliminating the need to travel and occupy limited space at a healthcare facility. Analysis of pre- and post-course assessments revealed statistically significant improvements in students’ knowledge and confidence related to course activities and population health initiatives. Similar positive outcomes have been reported in another study involving a telehealth course for health professional students. The VA received support for its population health activities through student involvement. As part of the opioid safety initiative, students completed over 4,000 PDMP notes and conducted 840 pain assessments over the phone. These activities would typically be carried out by the primary care team. Students also reviewed external health records in JLV and intervened in 1,061 cases, either documenting test results or screening outcomes from outside healthcare facilities. These activities helped the health system avoid redundant testing and cancer screenings, reducing both the costs and workload of ordering and interpreting these tests. Students also ordered required laboratory tests when indicated and notified patients about the need for additional laboratory tests. By performing these tasks, students alleviated pressure on an already burdened healthcare workforce. Alami et al highlight the positive attributes of telehealth services as clinically relevant, efficient, and mutually beneficial for all stakeholders including shared costs and benefits. Our academic partnership model aligns with these positive attributes, emphasizing collaboration and resource sharing.
Conclusions
Academic telehealth partnerships offer benefits to both health professional students and healthcare systems. By conducting telehealth activities remotely at the university, students gain early clinical experience, while leveraging resources from both the academic institution and the healthcare system. This partnership has significantly enhanced students’ perceptions of their learning and helped develop the next generation of telehealth providers, addressed prioritized population health initiatives, and reduced the workload for practitioners at healthcare facilities.
Conflict of Interest
The authors have no conflict of interest to disclose.
References
- Veterans Health Administration-About VHA. US Department of Veterans Affairs Website. Published January 20, 2025. Accessed March 27, 2025. https://www.va.gov/health/aboutVHA.asp
- Rosland AM, Nelson K, Sun H, et al. The patient-centered medical home in the Veterans Health Administration. Am J Manag Care. 2013;19(7):e263-e272.
- Rodriguez HP, Giannitrapani KF, Stockdale S, Hamilton AB, Yano EM, Rubenstein LV. Teamlet structure and early experiences of medical home implementation for Veterans. J Gen Intern Med. 2014;29 Suppl 2(Suppl 2):S623-S631. doi:10.1007/s11606-013-2680-1
- VA Telehealth Services celebrates 20 years – VA News. news.va.gov. Published May 1, 2023. Accessed April 7, 2025. https://news.va.gov/118570/va-telehealth-services-celebrates-20-years/
- Heyworth L, Shah N, Galpin K. 20 years of telehealth in the Veterans Health Administration: Taking stock of our past and charting our future. J Gen Intern Med. 2024;39(Suppl 1):5-8. doi:10.1007/s11606-024-08617-w
- US Department of Veterans Affairs Veterans Health Administration Office of Academic Affiliations. Health professions trainee satisfaction survey: AY 2023-2024. Accessed April 7, 2025. https://www.va.gov/OAA/docs/OAA_Stat_Sheet_AY23-24.pdf
- Harada ND, Falco K, Bowman M, Byrne JM. Telehealth and virtual supervision practices for health professions education in the Department of Veterans Affairs. BMC Med Educ. 2025;25(1):314. doi:10.1186/s12909-025-06698-7
- Ourth H, Groppi J, Morreale AP, Quicci-Roberts K. Clinical pharmacist prescribing activities in the Veterans Health Administration. Am J Health Syst Pharm. 2016;73(18):1406-1415. doi:10.2146/ajhp150778
- Hammond RW, Schwartz AH, Campbell MJ et al. Collaborative drug therapy management by pharmacists—2003. Pharmacotherapy. 2003;23(9):1210-1225. doi:10.1592/phco.23.10.1210.32752
- McFarland MS, Buck ML, Crannage E, et al. Assessing the impact of comprehensive medication management on achievement of the quadruple aim. Am J Med. 2021;134(4):456-461. doi:10.1016/j.amjmed.2020.12.008
- Perez A, Doloresco F, Hoffman JM, et al. ACCP: economic evaluations of clinical pharmacy services: 2001-2005. Pharmacotherapy. 2009;29(1):128. doi:10.1592/phco.29.1.128.
- Talon B, Perez A, Yan C, et al. Economic evaluations of clinical pharmacy services in the United States: 2011-2017. J Am Coll Clin Pharm. 2019;3:793–806. https://doi.org/10.1002/jac5.1199
- US Department of Veterans Affairs Pharmacy Benefits Management Services, Clinical Pharmacy Practice Office. Optimizing the Clinical Pharmacist Practitioner (CPP) to Improve Access and Quality Care. Accessed April 7, 2025. https://www.pbm.va.gov/PBM/CPPO/Documents/ExternalFactSheet_OptimizingtheCPPToImproveAccess_508.pdf
- Kerns RD, Otis J, Rosenberg R, Reid MC. Veterans’ reports of pain and associations with ratings of health, health-risk behaviors, affective distress, and use of the healthcare system.J Rehabil Res Dev. 2003;40(5):371-379. doi:10.1682/jrrd.2003.09.0371
- Gellad WF, Good CB, Shulkin DJ. Addressing the opioid epidemic in the United States: lessons from the Department of Veterans Affairs. JAMA Intern Med. 2017;177(5):611-612. doi:10.1001/jamainternmed.2017.0147
- Gallagher RM. Advancing the pain agenda in the Veteran population. Anesthesiol Clin. 2016;34(2):357-378. doi:10.1016/j.anclin.2016.01.003
- Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain – United States, 2022. MMWR Recomm Rep. 2022;71(3):1-95. doi:10.15585/mmwr.rr7103a1
- US Department of Veterans Affairs and Department of Defense. Clinical Practice Guideline for the Use of Opioids in the Management of Chronic Pain. May 2022. Accessed April 7, 2025. https://www.healthquality.va.gov/guidelines/Pain/cot/VADODOpioidsCPG.pdf
- US Department of Veterans Affairs. About Us – Women Veterans Health Care. Accessed April 7, 2025. https://www.womenshealth.va.gov/WOMENSHEALTH/about-us.asp
- Legler A, Price M, Parikh M, et al. Effect on VA patient satisfaction of provider’s use of an integrated viewer of multiple electronic health records. J Gen Intern Med. 2019;34(1):132-136. doi:10.1007/s11606-018-4708-z
- Yuan Y, Price M, Schmidt DF, Ward M, Nebeker J, Pizer S. Integrated health record viewers and reduction in duplicate medical imaging: Retrospective observational analysis. JMIR Med Inform. 2022;10(5):e32168. doi: 10.2196/32168
- The Association of American Medical Colleges. New and emerging areas in medicine series. Telehealth competencies across the learning continuum. March 2021. Accessed April 7, 2025. https://store.aamc.org/downloadable/download/sample/sample_id/412/
- American Association of Colleges of Pharmacy. AACP Curriculum Outcomes and Entrustable Professional Activities (COEPA) 2022. Accessed April 7, 2025. https://www.aacp.org/sites/default/files/2022-11/coepa-document-final.pdf
- Krebs EE, Lorenz KA, Bair MJ, et al. Development and initial validation of the PEG, a three-item scale assessing pain intensity and interference. J Gen Intern Med. 2009;24(6):733-738. doi:10.1007/s11606-009-0981-1
- Carr-Lopez SM, Strohecker LA, Miyahara RK, et al. Impact of a Veterans Affairs primary care collaboration to provide remote team-based care and telehealth introductory pharmacy practice experiences. J Am Coll Clin Pharm. 2021;4(9):1109–1116. https://doi.org/10.1002/jac5.1474
- Pylypchuk Y, Barker W. Use of Telemedicine among office-based physicians, 2021. In: ASTP Health IT Data Brief. Washington (DC): Office of the Assistant Secretary for Technology Policy; March 2023.1-16.
- Ndwabe H, Basu A, Mohammed J. Post pandemic analysis on comprehensive utilization of telehealth and telemedicine. Clin eHealth. 2024;7:5-14. doi:10.1016/j.ceh.2023.12.002
- Gullslett MK, Ronchi E, Lundberg L, et al. Telehealth development in the WHO European Region: Results from a quantitative survey and insights from Norway. Int J Med Inform. 2024;191:105558. doi: 10.1016/j.ijmedinf.2024.105558
- Saigí-Rubió F, Borges do Nascimento IJ, Robles Net al. The current status of telemedicine technology use across the World Health Organization European Region: An Overview of systematic reviews. J Med Internet Res. 2022;24(10), e40877. doi.org/10.2196/40877
- World Health Organization. The ongoing journey to commitment and transformation. Digital health in the WHO European Region 2023. 2023. Accessed April 7,2025. https://cdn.who.int/media/docs/librariesprovider2/data-and-evidence/english-ddh-260823_7amcet.pdf?sfvrsn=4c674522_2&download=true
- U.S. Food and Drug Administration. What is digital health? September 22, 2022. Accessed April 7, 2025. https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health
- World Health Organization. Regional digital health action plan for the WHO European Region 2023-2030. 2022. Accessed April 7, 2025. https://iris.who.int/bitstream/handle/10665/360950/72wd05e-DigitalHealth-220529.pdf?sequence=2
- World Federation for Medical Education. Basic Medical Education: WFME Global Standards for Quality Improvement. 2015. Accessed April 7, 2025. https://wfme.org/wp-content/uploads/2015/01/BME_2015_v2.pdf
- World Federation for Medical Education. Basic Medical Education: WFME Global Standards for Quality Improvement. 2020. Accessed April 7, 2025. https://wfme.org/wp-content/uploads/2020/12/WFME-BME-Standards-2020.pdf
- American Osteopathic Association. Commission on Osteopathic College Accreditation. Accreditation of Colleges of Osteopathic Medicine: COM Continuing Standards. 2023. Accessed April 7, 2025. https://osteopathic.org/index.php?aam-media=/wp-content/uploads/COCA-2023-COM-Continuing-Standards.pdf
- Carmichael JM, Meier J, Robinson A, Taylor J, Higgins DT, Patel S. Leveraging electronic medical record data for population health management in the Veterans Health Administration: Successes and lessons learned. Am J Health Syst Pharm. 2017;74(18):1447-1459. doi:10.2146/ajhp161048
- Mariño RJ, Capurro D, Merolli M. Pilot implementation of a telehealth course for health professions students. BMC Med Educ. 2024;24(1):963. Published 2024 Sep 4. doi:10.1186/s12909-024-05931-z
- Alami H, Shaw SE, Fortin JP, Savoldelli M, Fleet R, Têtu B. The ‘wrong pocket’ problem as a barrier to the integration of telehealth in health organisations and systems. Digit Health. 2023;9:20552076231169835. Published 2023 Apr 16. doi:10.1177/20552076231169835