





Telemedicine Adoption Model for Nigerian Clinicians
Telemedicine Adoption Among Nigerian Clinicians: Development and Validation of the Clinicians Telemedicine Adoption Model (CTAM)
Kayode I. Adenuga1, Noorminshah A. Iahad2, Suraya Miskon3
- University of Law Business School, Birmingham, United Kingdom
- Department of Applied Computing and Artificial Intelligence; Faculty of Computing, Universiti Teknologi Malaysia, UTM, Johor, Malaysia
- Department of Information Systems, Faculty of Management, Universiti Teknologi Malaysia, UTM, Johor, Malaysia
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: Adenuga, K. I., Jahad, N. A., & Miskon, S., 2025. Telemedicine Adoption Among Nigerian Clinicians: Development and Validation of the Clinicians’ Telemedicine Adoption Model (CTAM). Medical Research Archives, [online] 13(8).
https://doi.org/10.18103/mra.v13i8.6784
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6784
ISSN 2375-1924
Abstract
This study explores the key factors that influence the adoption of telemedicine among Nigerian clinicians. It introduces the Clinicians Telemedicine Adoption Model (CTAM), an extension of the Unified Theory of Acceptance and Use of Technology (UTAUT), developed through a cross-sectional survey of 302 clinicians across eight government hospitals in Ondo State, Nigeria. Using SmartPLS 2.0 for structural equation modelling, the study examined relationships among Clinicians Telemedicine Adoption Model (CTAM) variables and analysed demographic factors including age, gender, and profession as potential moderators. The findings show that Clinicians Telemedicine Adoption Model (CTAM) accounts for 45% of the variance in clinicians behavioural intention to use telemedicine systems. Specifically, Performance Expectancy, Effort Expectancy, Facilitating Conditions, Social Influence, and Reinforcement Factors significantly influenced clinicians’ intention to adopt telemedicine, consistent with the extended Unified Theory of Acceptance and Use of Technology (UTAUT) model. Furthermore, Human Factors were significantly moderated by younger clinicians, while the medical doctor profession significantly moderated the influence of Organisational Factors. Reinforcement Factors were also significantly moderated by age, gender, and profession. By understanding these determinants, hospital management boards and the Federal Ministry of Health can be better equipped to support the successful implementation of Nigeria’s national health ICT strategic framework, paving the way for more effective, technology-enhanced healthcare delivery in the near future.
Keywords
- Telemedicine
- Adoption
- Clinicians
1.0 Introduction
The introduction of information technology into hospital systems has significantly improved healthcare service delivery and management. It is also considered a vital component in reducing healthcare delivery costs for both healthcare organisations and policymakers. In Nigeria, a persistent shortage of clinicians has contributed to increased mortality among patients with chronic conditions requiring urgent medical attention. This pressing challenge has intensified the need to adopt innovative solutions such as telemedicine, particularly to bridge the healthcare delivery gap between urban centres and underserved rural hospitals. Across Nigeria, it is common for patients to travel long distances between states in search of specialised medical care. Similarly, specialists frequently travel from one government hospital to another on a weekly basis to offer consultations. This practice not only endangers the clinicians’ well-being but also compromises consistent care for patients at their primary workplaces. These logistical burdens could be substantially mitigated by harnessing the potential benefits of telemedicine systems, which offer a more sustainable and scalable solution for delivering specialist care.
Although telemedicine is not a new concept in Nigeria, its implementation has been limited. In 2007, the Nigerian government through the National Space Research and Development Agency (NASRDA) and the Federal Ministry of Health launched a pilot telemedicine project involving two teaching hospitals (University College Hospital, Ibadan and University Teaching Hospital, Maiduguri) and six federal medical centres across the country (Gombe, Makurdi, Yenagoa, Owo, Birnin Kebbi, and Owerri), alongside several private healthcare institutions. Despite this initiative, early investigations reveal that much of the pilot-phase equipment, including the telemedicine units, remains underutilised from a clinical standpoint. A recent systematic review by Agbeyangi and Lukose cited Obi-Jeff et al highlighting the low adoption of Nigeria’s mobile health application (IRISS) among caregivers and parents, primarily due to limited digital access and literacy barriers. In the same review, Onyeabor et al noted similarly low uptake of web-based healthcare applications among patients, with barriers including poor healthcare access, inadequate digital solutions, and limited patient engagement. Furthermore, long-standing challenges such as the absence of reimbursement policies, unstable internet connectivity, and inadequate infrastructure previously identified by Adenuga, Iahad, and Miskon remain largely unaddressed in Nigerian government hospitals.
These realities underscore the continued relevance of developing a telemedicine adoption model specifically tailored to Nigerian clinicians. This study, therefore, focuses on clinicians defined here as physicians and nurses actively involved in inpatient care and medical responsibilities as they serve as the primary users and implementers of telemedicine in Nigeria. In contrast, patients typically do not engage directly with the technology in their healthcare management. Addressing the technology adoption behaviour of clinicians is essential in filling a significant research gap and supports healthcare organisations striving to manage telemedicine effectively, particularly in environments where information technology investment and utilisation are on the rise. Although several studies have explored factors influencing telemedicine adoption using established theoretical frameworks such as the Diffusion of Innovation Theory (DIT), Technology Acceptance Model (TAM), Theory of Planned Behaviour (TPB), and Unified Theory of Acceptance and Use of Technology (UTAUT), few have focused on voluntary (non-mandatory) healthcare settings. Even fewer have addressed complex health information systems such as telemedicine, particularly in the Nigerian context.
To date, no study has proposed a theoretical model explaining Nigerian clinicians’ behavioural intention to adopt telemedicine. Therefore, the aim of this study is to identify and examine the factors that influence clinicians in Nigeria to adopt telemedicine. For the purposes of this study, telemedicine is defined as the enhancement of medical practice using telecommunication and multimedia technologies, combined with user-related attributes that support its effective utilisation.
2.0 Factors Influencing the Adoption of Telemedicine
To explore the factors influencing the adoption of telemedicine, the researchers conducted a comprehensive review of existing literature. A manual search of peer-reviewed articles indexed in Web of Science, ScienceDirect, Scopus, and Medline databases was carried out using Boolean combinations of keywords such as Telemedicine AND Adoption, Telemedicine AND Factors, Telemedicine AND Developed Countries, and Telemedicine AND Developing Countries. A Quality Assessment Criteria (QAC) metric guided the inclusion and exclusion of sources. Included studies covered various dimensions of telemedicine, such as feasibility assessments, healthcare management, clinical implementation, and review articles. The review revealed a diverse range of influences on telemedicine adoption, which the researchers have synthesised into five interconnected categories: Technological, Human, Organisational, Social, and Reinforcement factors.
Although telemedicine has been widely implemented in several developed countries and some developing contexts, its adoption remains limited particularly in Nigeria. While the benefits of telemedicine are well-documented, a range of persistent barriers continues to hinder its full-scale use. Zakaria et al categorised these barriers into technological, human, and organisational domains. Similarly, Hu et al emphasised the interplay of individual, technological, and organisational characteristics in technology adoption. Social influence, as discussed by Isabalija et al and Maarop and Win, also plays a significant role in shaping individual decisions about whether to engage with telemedicine services. Researchers such as Lasierra et al and Zanaboni and Wootton have also emphasised the need for further exploration of financial and professional incentives that may motivate clinicians. Despite the compelling case for telemedicine, these barriers if not adequately addressed are likely to continue limiting its uptake, especially in resource-constrained healthcare environments. Consequently, this study investigates these five key dimensions within the Nigerian healthcare context.
Technology, particularly information and communication technologies (ICT), continues to reshape healthcare delivery by enabling services to transcend geographic boundaries. Telemedicine is one such application of ICT that can significantly improve access and quality of care. However, its success largely depends on clinicians’ actual engagement with the technology. Research suggests that perceived benefits, usefulness, ease of use, and compatibility are vital in determining whether a user will adopt a new system. Systems perceived as user-friendly are more likely to be embraced, while those viewed as complex often face resistance, particularly when users are accustomed to existing methods. As such, it is the responsibility of information systems researchers to help ensure alignment between technological solutions and user expectations. In the context of Nigeria, where telemedicine is relatively new, it is essential to explore validated adoption constructs such as Performance Expectancy, Effort Expectancy, and Facilitating Conditions. These constructs form the basis of the technological dimension of this study, offering a framework for understanding how clinicians engage with telemedicine systems.
Beyond the technology itself, human factors play a crucial role in adoption. Individuals often resist change when it disrupts familiar routines, particularly if the change involves complex or unfamiliar technology. Zakaria et al noted several human-related barriers, including lack of awareness, technological anxiety, disinterest, and scepticism about integrating digital tools into clinical practice. The more complex a system appears, the less likely it is to be adopted. This study adopts a definition of Human Factors based on Lee et al, who explored the relationship between human attributes and behavioural intention using the Theory of Planned Behaviour (TPB). Here, Human Factors refer to the personal characteristics that Nigerian clinicians consider before choosing to use telemedicine factors such as confidence in using the technology, trust in its benefits, and willingness to integrate it into existing routines. These human attributes are particularly important given that clinicians are the primary users of telemedicine systems. Furthermore, their adoption may influence patient trust and engagement, as patients often rely on clinician recommendations when navigating new healthcare technologies.
Equally important is the role of healthcare organisations in facilitating telemedicine adoption. Organisations serve as key enablers, responsible for creating supportive environments where clinicians can deliver care using innovative technologies. In this context, issues such as policy clarity, infrastructure availability, data security, and medico-legal guidelines must be carefully managed to encourage adoption. This study builds on Lee et al to define Organisational Factors as the expectations clinicians have of their healthcare institutions such as access to technical support, legal protection, and operational policies before they are willing to adopt telemedicine. Given the complex interplay between institutions and clinical staff in Nigeria, this dimension is critical to understanding the practical challenges of telemedicine implementation.
Social dynamics also influence telemedicine uptake. Social influence is understood as the extent to which clinicians are affected by the opinions of their peers, supervisors, or respected figures when deciding whether to use new technologies. This construct appears across multiple theoretical frameworks including TRA, TPB, TAM2, and UTAUT under terms such as subjective norm, social factors, and image. Previous research consistently demonstrates that when influential peers endorse a technology, others are more likely to follow suit. Therefore, this study examines whether such influences play a role in Nigerian clinicians’ decisions to engage with telemedicine systems.
Finally, reinforcement through extrinsic motivation has been identified as a potentially powerful driver of adoption. In contexts where telemedicine may be perceived as adding to clinicians’ workload or posing usability challenges, financial or professional incentives can provide essential encouragement. Studies by Davis et al, Fagan et al, Lasierra et al, and Zanaboni and Wootton point to financial rewards and professional recognition as effective motivators. This idea aligns with Skinner’s theory of operant conditioning, which suggests that rewarded behaviours are more likely to be repeated. Reinforcement is especially relevant in settings where telemedicine adoption is not mandatory, as is often the case in Nigeria. For this reason, the study includes Reinforcement as a core dimension to empirically examine how such incentives could support the voluntary adoption of telemedicine among Nigerian clinicians.
2.1 THEORETICAL PERSPECTIVES
This study adopts the Unified Theory of Acceptance and Use of Technology (UTAUT) as its foundational theoretical model, extending it to suit the specific context of telemedicine adoption among Nigerian clinicians. UTAUT, developed by Venkatesh and colleagues, is widely recognised as one of the most comprehensive models for examining technology adoption, implementation, and use. UTAUT synthesises elements from eight prominent technology acceptance theories: the Technology Acceptance Model (TAM), the Theory of Reasoned Action (TRA), the Motivational Model (MM), the Theory of Planned Behaviour (TPB), a combined TAM-TPB model (C-TAM-TPB), the Model of PC Utilisation (MPCU), Innovation Diffusion Theory (IDT), and Social Cognitive Theory (SCT). By integrating these diverse models, UTAUT introduces four core constructs; Performance Expectancy, Effort Expectancy, Social Influence, and Facilitating Conditions that have consistently been found to predict behavioural intention and actual technology use.
The appeal of UTAUT lies in its robustness, empirical validity, and ability to account for a wide range of contextual variables. In healthcare specifically, its application is particularly relevant, as telemedicine services often involve complex, high-stakes environments where technology must align closely with the cognitive workflows of clinicians. As noted by Holden and Karsh and Lin and Stead, existing health IT systems do not always fully support the cognitive needs of medical professionals, reinforcing the need for theoretical frameworks that can account for this gap. Holden and Karsh further argued that while TAM has been extensively applied in healthcare settings, it remains uncertain whether it can evolve into a theory of health IT, rather than merely a theory for it. This distinction underscores the importance of models like UTAUT that provide a more holistic understanding of adoption behaviour.
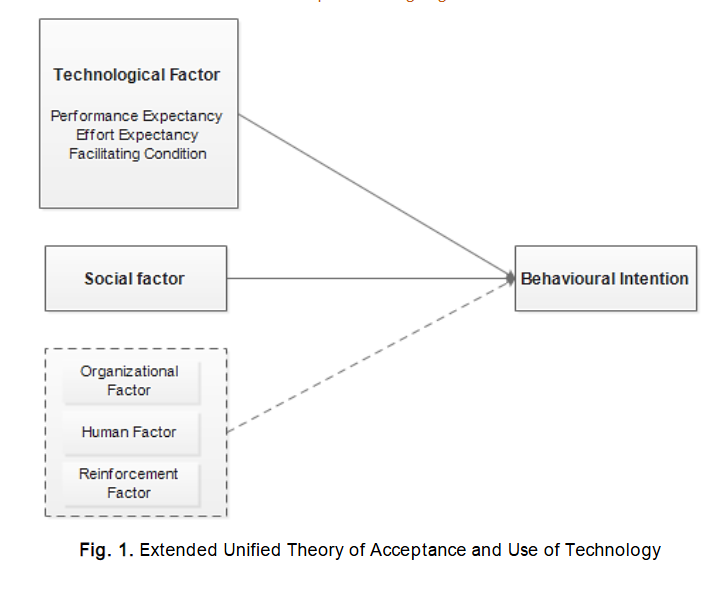
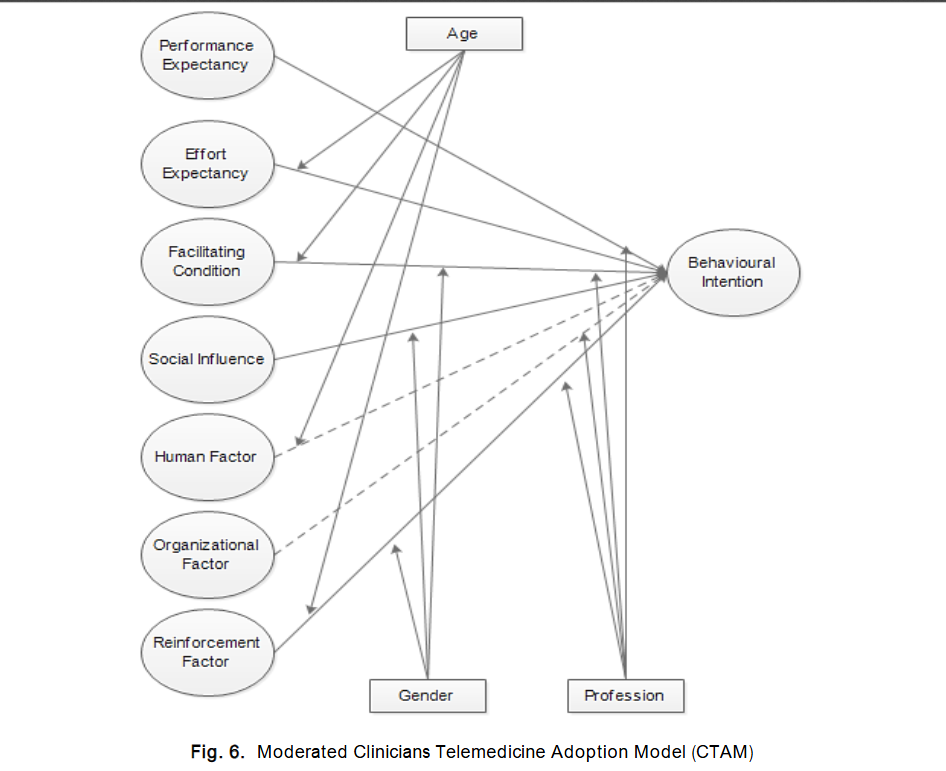
Furthermore, studies such as those by Burton-Jones and Hubona and Yarbrough and Smith highlight the significance of external variables in shaping technology acceptance, particularly in complex domains such as health information systems. Given telemedicine’s multifaceted nature, blending clinical, organisational, and technological considerations was deemed essential to enhance UTAUT with additional constructs that reflect the realities of healthcare delivery in Nigeria. Accordingly, this study proposes an extended version of the UTAUT model by incorporating three additional constructs: Human Factors, Organisational Factors, and Reinforcement. These dimensions were selected to capture the broader socio-technical context in which Nigerian clinicians operate. Human Factors refer to clinicians’ attitudes, beliefs, and readiness to embrace telemedicine. Organisational Factors reflect the support, policies, and infrastructure provided by healthcare institutions. Reinforcement addresses extrinsic motivators such as financial or professional incentives that may influence clinicians’ engagement with telemedicine systems. Together, these constructs, Performance Expectancy, Effort Expectancy, Social Influence, Facilitating Conditions, Human, Organisational, and Reinforcement form the basis of the Clinicians’ Telemedicine Adoption Model (CTAM), as illustrated in Figure 1. This extended model is intended not only to predict behavioural intention to use telemedicine but also to provide a nuanced understanding of the unique enablers and constraints faced by clinicians in the Nigerian healthcare system. Ultimately, this approach supports a more context-sensitive implementation of telemedicine technologies, aligning theoretical insight with practical realities.
2.2 RATIONALE BEHIND ADAPTED UNIFIED THEORY OF ACCEPTANCE AND USE OF TECHNOLOGY (UTAUT)
A growing number of studies in the social sciences and related fields have employed behavioural intention theories such as the Theory of Reasoned Action (TRA), the Theory of Planned Behaviour (TPB), the Diffusion of Innovation Theory (DOI), the Technology Acceptance Model (TAM), and the combined TAM-TPB model to investigate user adoption of information technologies. While these models have contributed valuable insights into user behaviour across diverse contexts, scholars have also noted their limitations, particularly in accounting for the complexity of real-world IT adoption. In response to these limitations, the Unified Theory of Acceptance and Use of Technology (UTAUT) was developed to offer a more integrative and predictive framework. UTAUT synthesises constructs from earlier models, streamlining them into four key determinants such as Performance Expectancy, Effort Expectancy, Social Influence, and Facilitating Conditions while also introducing moderating variables such as age, gender, experience, and voluntariness of use. Despite its theoretical strength and its success in explaining significant variance in behavioural intention and technology use, UTAUT has not been without critique. Venkatesh et al themselves acknowledged that the model may not apply uniformly across all contexts, that it omits potentially important relationships, and that it excludes several variables relevant to understanding IT adoption in specific settings.
Given these observations, Venkatesh, Chan, and Thong further highlighted that many researchers tend to apply only selected elements of UTAUT, often overlooking its moderating effects which is likely due to variations in research context or study design. For instance, although UTAUT originally suggested that Facilitating Conditions would only predict Behavioural Intention in the absence of Effort Expectancy, later empirical findings demonstrated that Facilitating Conditions can influence Behavioural Intention even when Effort Expectancy is included. Similarly, Dwivedi et al found that only about 25% of UTAUT applications incorporated all the constructs from the original model, indicating a trend of selective adaptation based on context.
This natural flexibility of the UTAUT framework makes it particularly suitable for emerging areas of research, such as telemedicine adoption in Nigeria. In this context, the adoption of telemedicine is still at a nascent stage, and understanding the behavioural intentions of clinicians who are the primary users is crucial for successful implementation. While UTAUT provides a solid foundation, it requires contextual enrichment to capture the unique factors shaping adoption in developing health systems.
Accordingly, this study extends the original UTAUT model by integrating three additional constructs identified through a comprehensive review of literature: Human Factors, Organisational Factors, and Reinforcement. These dimensions reflect key considerations specific to the Nigerian healthcare context, such as clinicians’ attitudes toward technology, institutional readiness, and the role of extrinsic motivation (e.g., financial or professional incentives). By enhancing the UTAUT framework with these empirically and contextually grounded variables, the study aims to provide a more holistic understanding of the factors influencing Nigerian clinicians’ behavioural intention to adopt telemedicine. This extended model not only addresses theoretical gaps noted in previous studies but also responds to the practical need for an evidence-based approach to technology implementation in healthcare systems.
2.3 RESEARCH HYPOTHESES
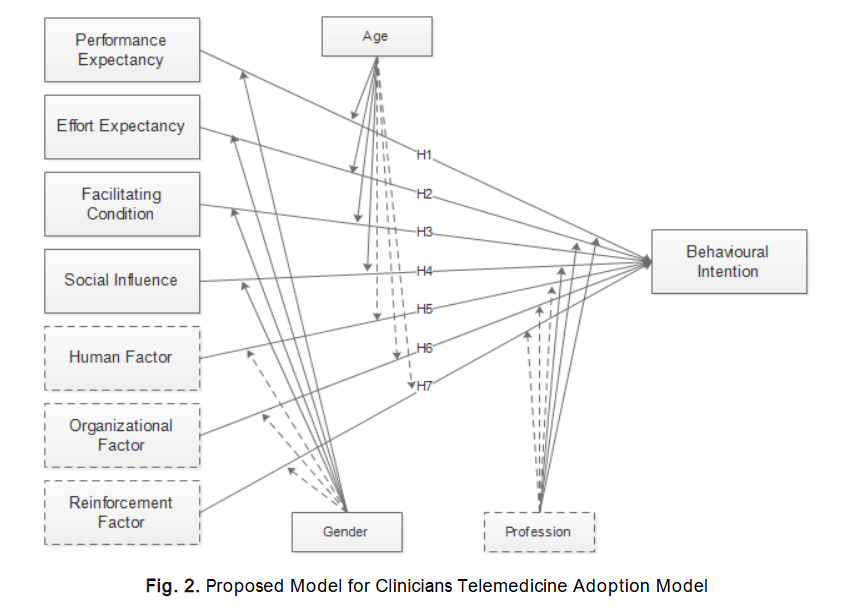
Based on insights drawn from the literature, this study identifies five core dimensions contributing to seven independent variables expected to predict Nigerian clinicians’ behavioural intention to adopt telemedicine a system that remains largely underutilised in many healthcare facilities across the country. The technological dimension is measured using three core constructs from the Unified Theory of Acceptance and Use of Technology (UTAUT): Performance Expectancy, Effort Expectancy, and Facilitating Conditions. These are supplemented by four additional constructs derived from empirical evidence: Social, Human, Organisational, and Reinforcement factors. Together, these seven constructs form the basis for exploring clinicians’ behavioural intention to use telemedicine (see Figure 2).
PERFORMANCE EXPECTANCY (PE) PERCEIVED USEFULNESS
Performance Expectancy refers to the extent to which clinicians believe that using telemedicine will enhance their job performance. Venkatesh et al identified PE as a strong predictor of behavioural intention, particularly when the perceived benefits of the system are evident. Accordingly, the following hypothesis is proposed:
H1: Performance Expectancy (PE) will have a significant positive relation to behavioural intention to use telemedicine systems.
EFFORT EXPECTANCY (EE) PERCEIVED EASE OF USE
Effort Expectancy relates to clinicians’ perceptions of how easy the telemedicine system is to use. This construct draws from the notions of ease of use, complexity, and perceived effort. If clinicians perceive the system as user-friendly, they are more likely to consider adopting it. This leads to the second hypothesis:
H2: Effort Expectancy (EE) will have a significant positive relationship with behavioural intention to use telemedicine systems.
FACILITATING CONDITIONS (FC)
Facilitating Conditions represent clinicians’ perceptions of the availability of the organisational and technical infrastructure needed to support their use of the telemedicine system. This includes access to reliable hardware, software, training, and institutional support. Adequate facilitating conditions are expected to influence adoption positively:
H3: Facilitating Conditions (FC) will have a significant positive relationship with clinicians’ behavioural intention to use telemedicine systems.
SOCIAL INFLUENCE (SI)
Social Influence in this context reflects the degree to which clinicians perceive that important others such as supervisors, colleagues, or institutional leaders believe they should use the telemedicine system. Prior studies have established social influence as a meaningful determinant of technology adoption:
H4: Social Influence (SI) will have a significant positive relationship with behavioural intention to use telemedicine systems.
HUMAN FACTOR (HF)
The Human Factor pertains to clinicians’ individual characteristics, such as awareness, confidence in using technology, or resistance to change, that may impact their willingness to adopt telemedicine. Although this factor has not been extensively modelled in prior telemedicine studies particularly in the Nigerian context – it is hypothesised to be influential:
H5: Human Factor (HF) will have a significant positive influence on clinicians’ behavioural intention to use telemedicine systems.
ORGANISATIONAL FACTOR (OF)
This factor represents the institutional policies, tools, and support systems that clinicians expect from their organisation in order to adopt telemedicine. It includes aspects such as clear guidelines, privacy assurances, and legal frameworks. Given the institutional role in technology uptake, the following hypothesis is proposed:
H6: Organisational Factor (OF) will have a significant positive influence on clinicians’ behavioural intention to use telemedicine systems.
REINFORCEMENT FACTOR (RF)
Reinforcement reflects the degree to which clinicians expect motivation, especially in the form of financial or professional incentives, to support the continued use of telemedicine. Based on behavioural theories, reinforcement is a well-established driver of repeated behaviour. Given the additional responsibilities telemedicine may impose on clinicians, reinforcement is hypothesised to significantly influence their behavioural intention to adopt telemedicine:
H7: Reinforcement Factor (RF) will have a significant positive influence on clinicians’ behavioural intention to use telemedicine systems.
MODERATING VARIABLES
Age
In the original UTAUT model, age was found to moderate the effects of all key constructs. Older clinicians may perceive new technologies differently compared to younger counterparts, particularly regarding ease of use and adaptability. Since this study involves both early- and late-career clinicians, age is considered a relevant moderator.
H8a: Age will significantly moderate the relationship between (PE, EE, FC, SI, HF, OF, and RF) and behavioural intention to use telemedicine systems.
Gender
Gender is another important moderator in technology acceptance research. Previous findings suggest that males and females may exhibit different attitudes and behavioural responses toward new technologies. Accordingly, gender is examined across all proposed constructs:
H8b: Gender will significantly moderate the relationship between (PE, EE, FC, SI, HF, OF, and RF) and clinicians’ behavioural intention to use telemedicine systems.
Profession
While UTAUT often uses experience as a moderator, in this study, profession is used instead given the relatively low utilisation of telemedicine systems in Nigerian hospitals. Medical doctors, nurses, and other healthcare professionals may hold differing perspectives based on their clinical roles. Therefore, profession is used to explore variation in intention:
H8c: Profession will significantly moderate the relationship between (PE, EE, FC, SI, HF, OF, and RF) and clinicians’ behavioural intention to use telemedicine systems.
3 Methods
3.1 DESIGN AND SETTINGS
A self-administered survey was carried out in early 2016 following the necessary ethical approvals from the Federal Medical Centre and Hospitals Management Boards in Ondo State, Nigeria. The inclusion of the Federal Medical Centre was deliberate, as it offers a broader and more representative sample for generalising findings within the Nigerian healthcare context. This is largely because the hospital is federally owned and staffed with a diverse pool of clinicians and specialists drawn from various regions across the country. Questionnaires were distributed using a purposive sampling technique, a subset of non-probability sampling, due to the unavailability of an exact population frame. This method was chosen to ensure that only clinicians familiar with telemedicine or those who have engaged with it in their professional practice were included in the study. Prior to the main survey, a preliminary investigation in the form of interviews was conducted to help define the research scope and refine the research instruments accordingly. Importantly, clinicians who participated in the preliminary interviews and pilot survey were excluded from the final survey sample to maintain data integrity.
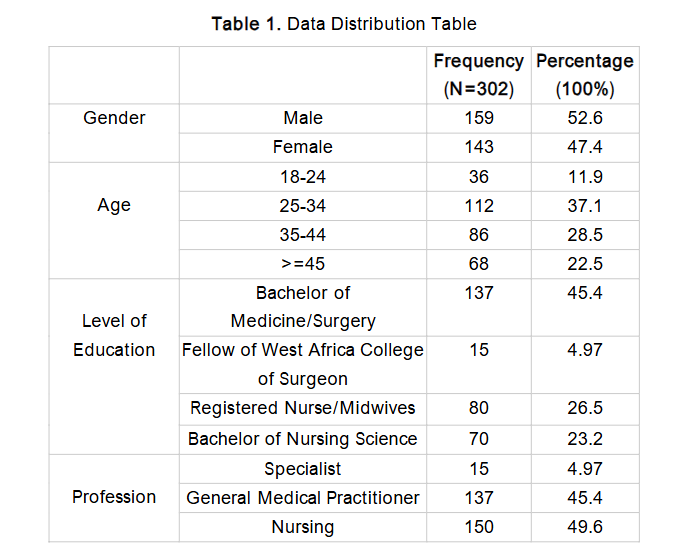
In total, 350 questionnaires were distributed across the selected government hospitals. Of these, 313 were returned. However, 11 responses were excluded due to significant incompleteness. This resulted in 302 valid responses being retained for analysis (as shown in Table 1), yielding a high and acceptable response rate of 89%.
4.0 Results
The Structural Equation Modelling (SEM) statistical approach was employed to determine whether both the measurement and structural models met the quality standards required for evidence-based research. In recent years, SEM has become increasingly common in empirical studies within the field of information systems. As a causal modelling technique, its primary aim is to maximise the explained variance of latent dependent variables, thereby allowing researchers to assess the quality of data in relation to the attributes of the measurement model.
4.1 MEASUREMENT MODEL
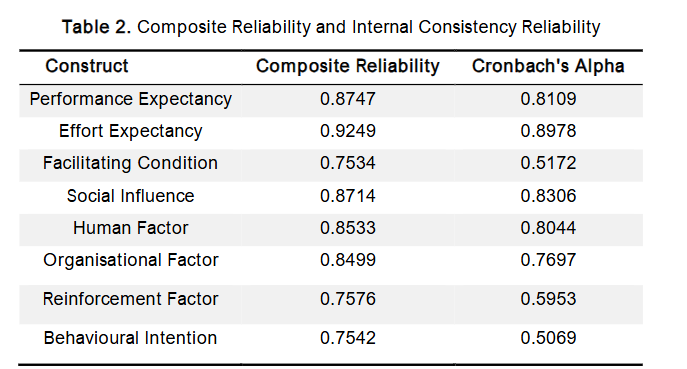
In assessing the measurement model, the first aspect to be evaluated is the internal consistency reliability. This is determined by estimating the degree of interrelatedness among the observed indicator cons s alpha has been the standard metric for assessing internal consistency. However, it is widely acknowledged that Cronb s alpha tends to underestimate reliability and is therefore often considered a conservative measure of internal consistency. Due to these limitations, composite reliability (CR) is frequently recommended as a more robust alternative. Reliability in measurement refers to the consistency with which a research instrument yields results. It reflects the extent to which a test consistently measures what it is intended to measure, with a focus on the stability of repeated measurements of constructs. A construct is deemed reliable when its composite reliability exceeds the threshold of 0.7. Hair, Sarstedt, Ringle, and Mena (2012) affirm that a CR value of 0.7 or above is acceptable. Similarly, Hair et al. (2006) note that the commonly accepted benchmark for Cronbach s alpha is 0.7, although values as low as 0.6 can still be deemed valid. Furthermore, Nunnally (1967) argued that in theoretical research, even relatively modest Cronbach s alpha values of 0.60 or 0.50 may be acceptable. In light of these considerations, the results indicate that the reliability of the constructs, as reported in Table 2, is acceptable.
Convergent validity in this study was assessed using three key criteria: item factor loadings, composite reliability (CR), and average variance extracted (AVE), as recommended by Fornell and Larcker (1981). First, factor loadings were examined within the measurement model, with a minimum threshold of 0.50, based on the guideline by Hair et al. (2012), who stated that loadings of 0.50 or higher are considered significant. In addition, Hair, Ringle, and Sarstedt (2011) suggested that composite reliability values should generally exceed 0.70 to indicate acceptable reliability. Finally, AVE values greater than 0.50 demonstrate that the items adequately converge to represent the underlying construct, in line with the standard proposed by Barclay, Higgins, and Thompson.
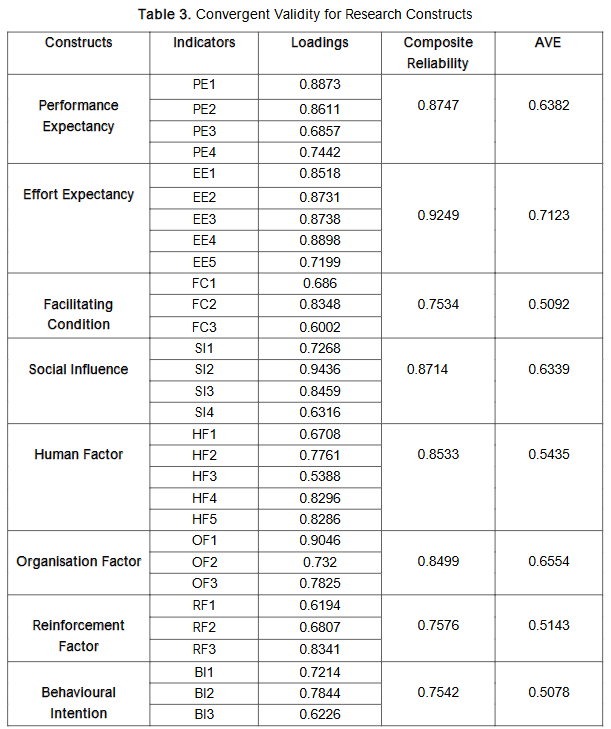
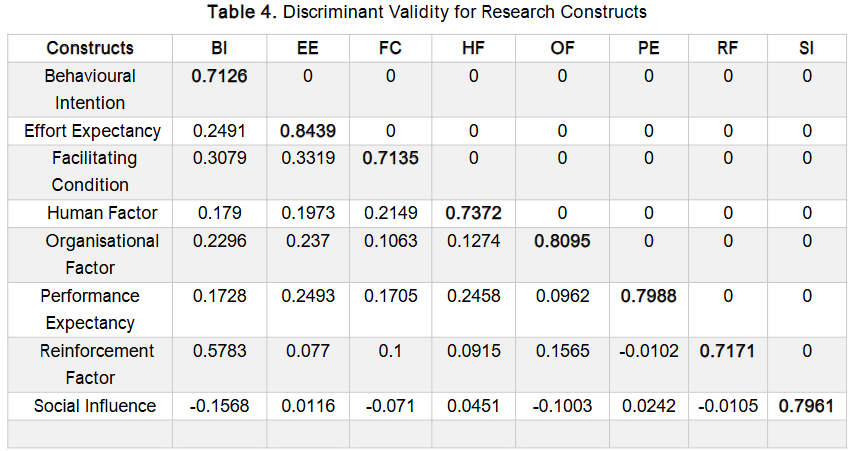
Discriminant validity refers to the extent to which a construct is empirically distinct from other constructs within the same model. It is established when a construct demonstrates unique characteristics that are not captured by any other construct in the model. In this study, discriminant validity was assessed using the Fornell-Larcker criterion. This method involves replacing the diagonal elements of the correlation matrix with the square root of the Average Variance Extracted (AVE). Discriminant validity is confirmed when these diagonal values are greater than the corresponding correlation coefficients in the off-diagonal positions, as illustrated in Table 4. The AVE values in this study ranged from 0.7126 to 0.8439. These results indicate that the square roots of AVE for all constructs exceeded the inter-construct correlations, thereby confirming that the model possesses adequate discriminant validity.
4.2 STRUCTURAL MODEL
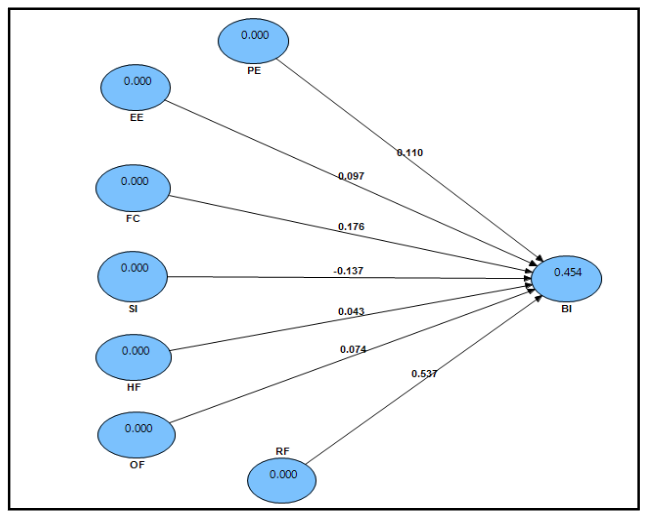
An essential initial step in evaluating the structural model is assessing the coefficient of determination (R²) for the dependent constructs. The R² value indicates the proportion of variance in the dependent variable that can be explained by the independent constructs. It reflects the model’s ability to interpret and predict outcomes related to the dependent variable. According to Chin (1998), R² values of approximately 0.670 are considered substantial, around 0.333 are deemed moderate, and values at or below 0.190 are regarded as weak. In this study, the R² value for the dependent variable behavioural intention to use telemedicine is 0.45, which falls within the moderate prediction range. This is illustrated in Figure 3.
4.3 TEST OF RESEARCH HYPOTHESES
The hypotheses in this study were tested by evaluating the statistical significance of the path coefficients using t-statistics, calculated via the bootstrap resampling method. Specifically, non-parametric bootstrapping was performed with 5,000 replications, in line with the recommendations of Efron and Tibshirani and Hair, Ringle, and Sarstedt. The t-values and degrees of freedom (DF) were then used to compute the p-values associated with each hypothesis. The resulting p-values, along with their corresponding significance levels, are presented in Table 5. The primary objective of this study was to examine the factors influencing Nigerian clinicians’ intention to adopt telemedicine. The analysis revealed that Performance Expectancy (PE) has a statistically significant and positive relationship with Behavioural Intention. This suggests that Nigerian clinicians recognise the potential benefits of telemedicine, perceiving it as a useful tool in clinical practice. These findings align with previous research on telemedicine adoption, including studies by Kohnke, Cole, and Bush, and Shibl, Lawley, and Debuse. Similarly, Kissi et al. found that Perceived Usefulness, a core construct of the Technology Acceptance Model (TAM), significantly influenced Behavioural Intention to use telemedicine services in Ghana.
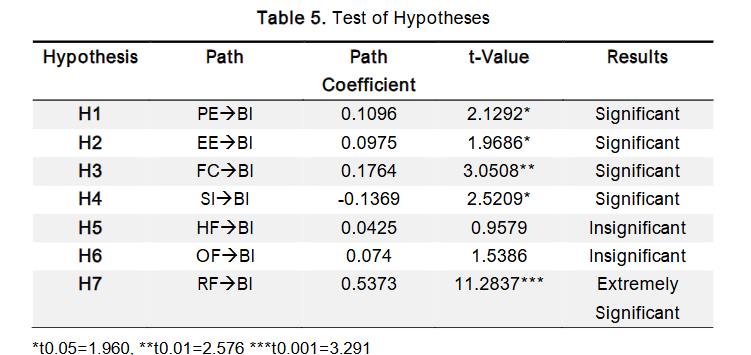
Effort Expectancy (EE) was found to have a significant positive relationship with Behavioural Intention. This finding aligns with previous research on telemedicine adoption. Similarly, Kissi et al. reported that perceived ease of use significantly influenced Ghanaian physicians’ intention to use telemedicine services. These results suggest that health professionals tend to favour technologies that are easy to use and require minimal effort. Facilitating Conditions (FC) also showed a positive relationship with Behavioural Intention, indicating that Nigerian clinicians recognise the importance of technical and organisational support in promoting the adoption of telemedicine. These conditions may include access to modern telemetric equipment, reliable internet connectivity, and a conducive environment for remote consultations. This result is consistent with the findings of Dwivedi et al., Taylor and Todd, Venkatesh et al., and Gagnon et al., who emphasised the role of infrastructure and support systems in technology adoption. Additionally, Sagaro, Battineni, and Amenta identified inadequate infrastructure as a key barrier contributing to resistance to telemedicine in Ethiopia, further supporting the relevance of this factor. Interestingly, Social Influence (SI) was found to be significant but demonstrated a negative relationship with Behavioural Intention, which contradicts the initial hypothesis and findings from prior studies that reported a positive association. Some earlier studies also reported no significant effect of social influence, especially among physicians who typically have autonomy in deciding whether to adopt new technologies. However, our findings are consistent with those of Kijsanayotin, Pannarunothai, and Speedie, who suggested that social influence may be more relevant among allied health workers subject to supervisory authority. In this context, the findings imply that influence from supervisors, colleagues, or other key figures might negatively impact Nigerian willingness to adopt telemedicine, possibly due to professional hierarchies or scepticism among peers. Lastly, the Human Factor (HF) did not show a significant relationship with Behavioural Intention. One possible explanation is that some respondents may have provided socially desirable answers or withheld full disclosure due to the ethical obligations tied to their professional roles. This could have influenced the validity of responses and may account for the insignificance of this hypothesis.
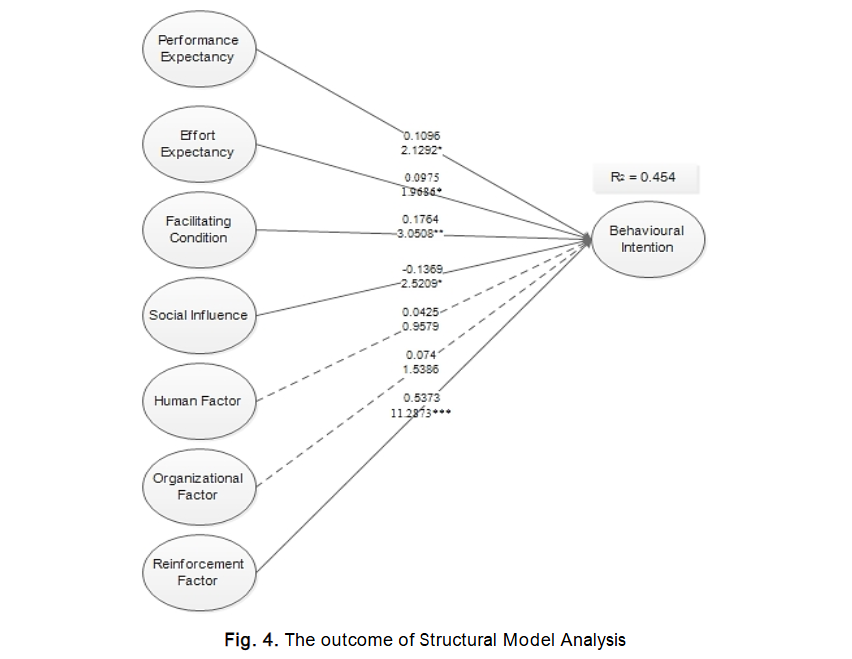
Similarly, the Organisational Factor (OF) was found to be statistically insignificant, which contrasts with the findings of Zailani, Gilani, Nikbin, and Iranmanesh (2014), who identified strong government policies and top management support as significant predictors of telemedicine acceptance in Malaysia.⁸⁹ Lee, Ramayah, and Zakaria (2012) also emphasised that healthcare organisations play a vital role in facilitating the adoption of new technologies by ensuring the necessary structures and support systems are in place.⁴⁶
In the Nigerian context, clinicians appear to recognise the importance of organisational involvement in technology adoption, especially given the Federal Ministry of Health’s installation of a telemedicine system that remains underutilised. Many clinicians expect that certain inter- and intra-organisational issues should be addressed before the mandatory imposition of such technologies. One possible explanation for the statistical insignificance of this factor is the cautiousness of Nigerian clinicians.
in expressing their opinions due to the civil service confidentiality rules, which are deeply embedded in the country’s public sector culture. Nonetheless, insights from interviews conducted in this study align with the findings of Sagaro, Battineni, and Amenta (2019), who identified lack of training and awareness as major barriers to telemedicine adoption in Ethiopia.⁶⁷ This reinforces the idea that healthcare organisations play a critical role in promoting telemedicine by implementing regular training programs and awareness campaigns.
Finally, the Reinforcement Factor (RF) showed a highly significant and positive relationship with clinicians’ intention to adopt telemedicine, thereby supporting the corresponding hypothesis. This finding is consistent with Rho, Choi, and Lee (2014), who stressed the importance of establishing a comprehensive reimbursement policy to support telemedicine services in Korea.⁶⁵ Similarly, Sagaro et al. (2019) noted that strengthening Medicare reimbursement could mitigate barriers to telemedicine adoption in Ethiopia.⁶⁷ This result is further supported by Olver and Selva-Nayagam (2000), who reported that three out of five remote clinicians felt that telemedicine consultations increased their workload, while only two of thirteen clinicians in another setting observed such an increase; the rest reported no significant difference.⁶⁰
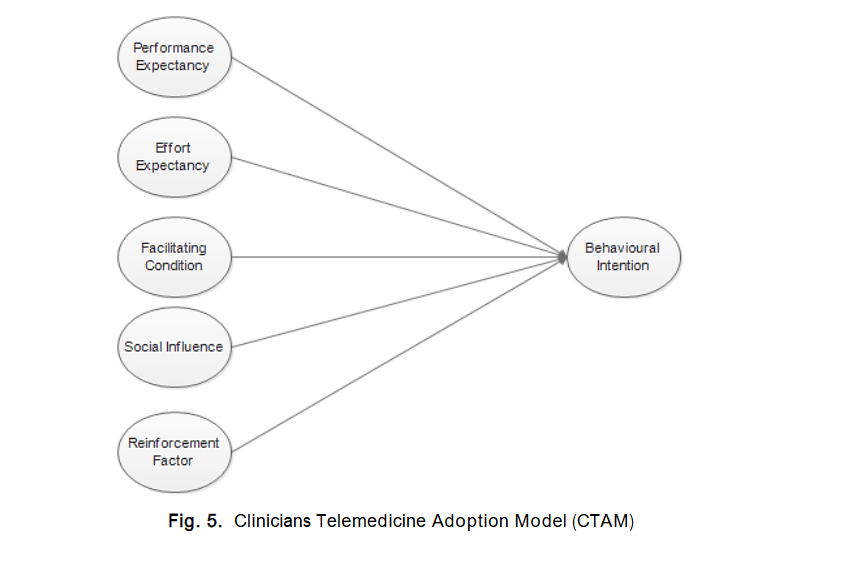
These findings align with the preliminary results of the present study, where all participants expressed concerns that adopting telemedicine in its current form would add to their already substantial workload. In summary, all but two of the hypothesised relationships in this study were statistically significant. Having validated both the structural model and the hypothesis testing, a final CTAM model was developed, as illustrated in Figure 5.
4.4 TESTING THE MODERATION EFFECT IN THE MODIFIED UTAUT
In the original Unified Theory of Acceptance and Use of Technology (UTAUT) model developed by Venkatesh, Morris, Davis, and Davis, age, gender, and experience were identified as moderating variables across all the constructs examined. In the current study, experience was replaced with profession, as experience was not deemed applicable within the specific context of this research, as explained earlier.
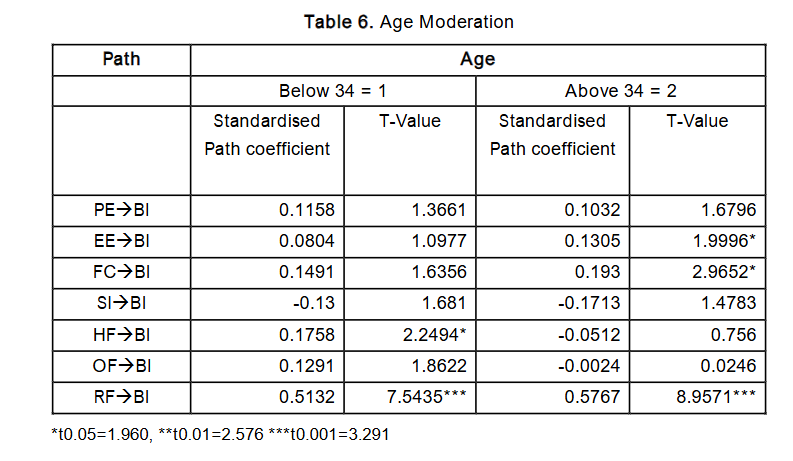
Age
For this study, age was categorised into two groups: a younger group comprising participants aged below 34 years, and an older group of those aged 34 years and above. This classification was based on observed disparities in educational attainment between the groups. The findings revealed that Human Factor and Reinforcement Factor significantly influenced the younger clinicians, while Effort Expectancy, Facilitating Condition, and Reinforcement Factor significantly influenced the older group. Interestingly, Social Influence was not statistically significant for either age group. This contradicts the findings of Venkatesh et al., where age significantly moderated the relationships between Performance Expectancy (PE), Effort Expectancy (EE), Social Influence (SI), Facilitating Condition (FC), and Behavioural Intention (BI).
Gender
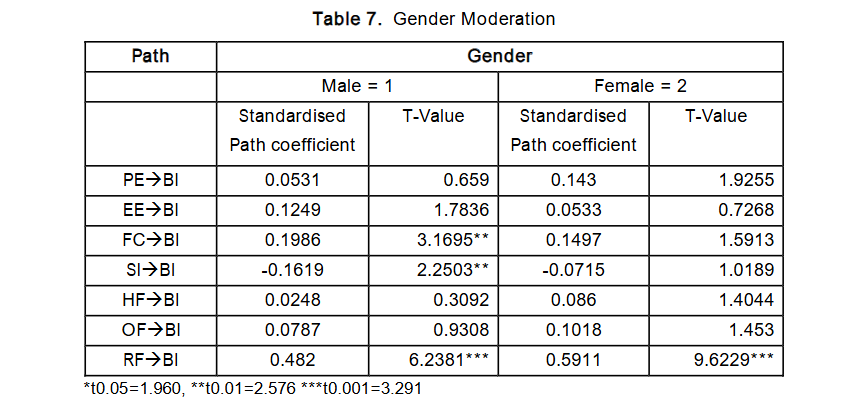
When examining gender as a moderating variable across the constructs PE, EE, FC, SI, Human Factor (HF), Organisational Factor (OF), and Reinforcement Factor (RF), the analysis showed that Facilitating Condition, Social Influence, and Reinforcement Factor were significantly moderated by male gender. For female clinicians, only Reinforcement Factor showed a significant moderating effect. Moreover, the moderating influence of gender was found to be stronger among males. This aligns with previous studies on health IT adoption where gender served as a moderating variable. However, this study also found that Social Influence had a negative effect on male clinicians, a result that diverges from the predominantly positive associations reported in existing literature. This suggests that male clinicians in Nigeria may be negatively influenced by the opinions of superiors, colleagues, or other significant individuals when it comes to adopting telemedicine technologies.
Profession
In terms of profession, the study found that Facilitating Condition, Organisational Factor, and Reinforcement Factor significantly influenced medical doctors, while the nursing profession significantly moderated the relationships between Performance Expectancy, Reinforcement Factor, and Behavioural Intention to adopt telemedicine. For physicians, the findings indicate that adoption would be encouraged by strong organisational structures and well-defined administrative policies governing the use of new technologies. This is supported by existing literature, which highlights the importance of addressing legal, regulatory, and ethical issues associated with telemedicine. The Code of Medical Ethics by the Medical and Dental Council of Nigeria acknowledges telemedicine as an emerging necessity due to advancements in technology that enable remote diagnoses. However, clinicians are advised to proceed with caution, particularly with respect to medico-legal considerations. It is therefore expected that clinicians would be more willing to utilise telemedicine systems if intra- and inter-organisational issues are adequately addressed, and if technical enabling conditions such as high-speed internet and appropriate telecommunication infrastructure are in place.
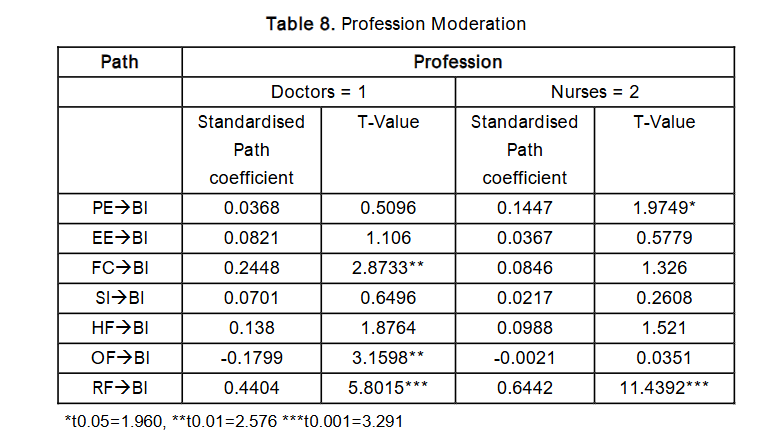
Overall, the findings suggest that all three moderating variables age, gender, and profession significantly influenced the relationships between the independent variables and clinicians’ behavioural intention to use telemedicine at different points. Notably, the Reinforcement Factor emerged as consistently significant across all three moderating variables, underscoring its central importance. Given these insights, the study concludes that reinforcing support mechanisms such as reimbursement policies, workload management, and infrastructural improvements are urgently needed to foster telemedicine adoption among Nigerian clinicians. The current perception of telemedicine as an additional burden highlights the necessity of addressing these barriers systematically.
5.0 Discussion
This study set out to identify the key factors influencing clinicians’ adoption of telemedicine in Nigeria and to propose a suitable theoretical model that encapsulates these factors. The findings affirm that the proposed Clinicians Telemedicine Adoption Model (CTAM) offers a robust framework for understanding clinicians’ Behavioural Intention (BI) to use telemedicine for clinical diagnosis and medical care. While several hypotheses were supported, Human Factor (HF) and Organisational Factor (OF) were not statistically significant within the baseline CTAM model. However, both became significant when the model was moderated, highlighting the contextual nuances influencing their roles. From a theoretical standpoint, this study makes two significant contributions to the literature. First, it extends the original UTAUT model by developing and empirically validating a new theory-based framework CTAM that specifically captures the dynamics of telemedicine adoption among clinicians in Nigeria. Second, it enriches our understanding of the relationships among UTAUT constructs and newly added factors (HF, OF, RF) within a healthcare setting in a developing country. The CTAM highlights the interplay of multiple factors and provides a structured explanation of clinicians’ intention to adopt telemedicine, thereby offering a model that is not only applicable in Nigeria but also potentially transferable to other sub-Saharan African countries facing similar challenges in telemedicine adoption.
Practically, telemedicine adoption has the potential to revolutionise healthcare delivery in Nigeria by bridging the gap between urban-urban and rural-urban hospitals. It can significantly reduce the burden of specialist travel for consultations and facilitate timely medical interventions. Several sub-Saharan African countries including Ghana, Mozambique, Senegal, Uganda, Cape Verde, and Ethiopia have initiated telemedicine programs, but challenges remain in ensuring sustainable and widespread adoption. CTAM can serve as a guiding framework to support the Federal Ministry of Health in Nigeria, health policymakers, and hospital management boards in designing, implementing, and scaling telemedicine initiatives. It can also complement and enhance existing telemedicine blueprints and initiatives, such as those spearheaded by the Society for Telemedicine and eHealth in Nigeria.
5.1 LIMITATION OF THE STUDY
Despite its contributions, this study is subject to several limitations that should be acknowledged. First, the study was limited to selected government hospitals, which may affect the generalisability of the findings to private healthcare institutions or other public hospitals not included in the sample. Second, the focus was exclusively on practicing clinicians namely, physicians and nurses who are directly involved in clinical care. The perspectives of other healthcare professionals not engaged in direct patient care may differ. Third, due to the limited availability of established instruments for the newly added constructs (Human Factor, Organisational Factor, and Reinforcement Factor), the researchers developed measurement items based on thematic analysis. Although these items were validated during pilot and main studies, further testing in broader populations is necessary to establish stronger external validity. Future researchers should consider refining and validating these constructs across diverse healthcare settings in other sub-Saharan African countries.
5.2 CONCLUSION AND SUGGESTIONS FOR FUTURE STUDIES
This study developed and validated the Clinicians Telemedicine Adoption Model (CTAM) to explore factors influencing telemedicine adoption among Nigerian clinicians. The decision to extend UTAUT was informed by its robustness and widespread application in health IT adoption literature. Findings reveal that Performance Expectancy (PE), Effort Expectancy (EE), Facilitating Condition (FC), and Reinforcement Factor (RF) have significant positive relationships with Behavioural Intention. Notably, Social Influence (SI) showed a significant but negative relationship, suggesting that the influence of superiors and peers may discourage clinicians from adopting telemedicine.
The Reinforcement Factor emerged as the most critical predictor across both the base and moderated models, indicating that proper motivation such as fair workload compensation or policy incentives is central to telemedicine acceptance. Though Human and Organisational Factors were not significant in the unmoderated model, they became important under moderation by age and profession, supporting our previous qualitative findings where these factors were perceived as influential. Future research could build on these insights in several ways. First, subsequent studies should explore the Reinforcement Factor’s impact on the actual use of telemedicine, following the UTAUT framework’s assumption that Behavioural Intention leads to actual use. Second, the CTAM model could be replicated in other sub-Saharan African countries or adapted for use in private healthcare institutions to test its broader applicability and enhance its empirical generalisability.
Additionally, future studies could incorporate a mediating role of the organisation, investigating how internal organisational culture or policy structures influence the relationship between CTAM constructs and Behavioural Intention. This would provide valuable insights for hospital management and health ministries looking to implement telemedicine solutions effectively. Importantly, this study focused on practicing clinicians in government hospitals. Future research should aim to include a more diverse pool of participants, encompassing both public and private sector clinicians, to gain a more holistic understanding of adoption drivers. Given that CTAM is the first empirically validated model of its kind in this region, it presents a strong foundation for ongoing research and practice to promote telemedicine adoption in Africa and other developing contexts.
Acknowledgements
The authors would like to express their sincere appreciation to the Ministry of Higher Education Malaysia for providing a doctoral research scholarship through the Commonwealth Scholarship and Fellowship Plan, which supported this research. The authors also extend their gratitude to the entire board and medical staff of the Ondo State Hospitals Management Board and the Federal Medical Centre, Owo, Ondo State, Nigeria, for their invaluable assistance during the ethical approval process and data collection phase.
Declaration of Conflicting Interests and Funding
The authors declare that there are no conflicts of interest associated with this research. Furthermore, no financial support was received for the conduct, authorship, or publication of this study.
Author Contributions and Affiliations
- Dr. Kayode I. Adenuga is a Senior Lecturer at the University of Law Business School, Birmingham, United Kingdom. He conducted the study and prepared the manuscript. He completed his doctoral studies under the supervision of the second and third authors.
- Dr. Noorminshah A. Iahad is an Associate Professor in the Department of Applied Computing and Artificial Intelligence Faculty of Computing, Universiti Teknologi Malaysia UTM, Johor, Malaysia. She served as the primary supervisor for Dr. Adenuga during his doctoral research, provided continuous academic guidance throughout the study, and reviewed the manuscript prior to submission.
- Dr. Suraya Miskon is Associate Professor in the Department of Information Systems, Faculty of Management, Universiti Teknologi Malaysia, Malaysia UTM, Johor, Malaysia. She co-supervised Dr. Adenuga during his doctoral studies and contributed to the academic development of the research.
Survey Questionnaire
Performance Expectancy
- PE_1 Telemedicine would be beneficial in managing my patients.
- PE_2 Telemedicine service would be useful in my job.
- PE_3 Using Telemedicine would reduce frequent face to face consultations.
- PE_4 It would be easy to share knowledge with colleagues using Telemedicine.
- PE_5 Telemedicine would be beneficial in managing my patients.
Effort Expectancy
- EE_1 I will use Telemedicine if it is easy to use.
- EE_2 It would be easy for me to use Telemedicine if it is clear and understandable.
- EE_3 Telemedicine system would be easy for me to use if it is flexible to interact with.
- EE_4 It would be easy to use Telemedicine to manage my patient if it is easy to learn.
- EE_5 It would be easy for me to become skillful at using telemedicine systems.
Facilitating Condition
- FC_1 I have the necessary ICT knowledge to use Telemedicine.
- FC_2 I have sufficient technological facilities in place to use Telemedicine.
- FC_3 Given the resources and knowledge required to use telemedicine systems, it will be easy for me to use the system.
- FC_4 Using telemedicine system will fit into my work pattern.
Social Influence
- SI_1 My colleagues at work influence my decision to use telemedicine systems.
- SI_2 My supervisor thinks I should use Telemedicine systems.
- SI_3 People who are important to me think I should use Telemedicine.
- SI_4 My organisation has encouraged me to use Telemedicine.
Human Factors
- HF_1 It would be easy for me to use Telemedicine if there is legal backing.
- HF_2 It would be easy for me to use Telemedicine if it is not a threat to my job.
- HF_3 It would be easy for me to use the Telemedicine system if it can be trusted.
- HF_4 It would be easy for me to use Telemedicine if it’s free of impersonation.
- HF_5 If would be easy for me to use the Telemedicine, if it’s not an additional responsibility for me.
Organisational Factor
- OF_1 It would be easy for me to use the telemedicine system if there is sound policy guiding its usage.
- OF_2 It would be easy to use telemedicine system if it is protected by copyright.
- OF_3 It would be easy to use Telemedicine if it is safe and secure.
- OF_4 It would be easy to use telemedicine system if patients’ privacy and confidentiality are ensured.
Reinforcement Factor
- RF_1 It will encourage me to use Telemedicine system if there is a financial incentive.
- RF_2 I would strongly consider using the telemedicine system if I am motivated.
- RF_3 Telemedicine usage is an additional workload for me; incentive would be necessary.
Behavioural Intention
- BI_1 I intend to use the Telemedicine system in the next 6 months.
- BI_2 I predict I will use Telemedicine in the next 9 months.
- BI_3 I will use Telemedicine system in the nearest future.
References
- Adenuga, K. I., Iahad, N. A., & Miskon, S. (2017). Towards reinforcing telemedicine adoption amongst clinicians in Nigeria. International journal of medical informatics, 104, 84-96.
- Agbeyangi, A. O., & Lukose, J. M. (2025). Telemedicine adoption and prospects in sub-Sahara Africa: a systematic review with a focus on South Africa, Kenya, and Nigeria. Paper presented at the Healthcare.
- Ahmad, S., & Afthanorhan, W. M. A. B. W. (2014). The importance-performance matrix analysis in partial least square structural equation modeling (PLS-SEM) with smartpls 2.0 M3. International Journal of Mathematics Research, 3(1), 1.
- Ajzen, I. (2011). The theory of planned behaviour: Reactions and reflections: Taylor & Francis.
- AlAwadhi, S., & Morris, A. (2008). The Use of the UTAUT Model in the Adoption of E-government Services in Kuwait. Paper presented at the Hawaii International Conference on System Sciences, Proceedings of the 41st Annual.
- Alibaygi, A., Karamidehkordi, M., & Pouya, M. (2012). Using the Delphi technique to assess cost-effectiveness of rural information and communications technologies (ICT) centers in Iran. Journal of Agricultural Extension and Rural Development, 4(20), 552-555.
- Barclay, D., Higgins, C., & Thompson, R. (1995). The partial least squares (PLS) approach to casual modeling: personal computer adoption and use as an illustration.
- Burton-Jones, A., & Hubona, G. S. (2006). The mediation of external variables in the technology acceptance model. Information & Management, 43(6), 706-717.
- Chang, I.-C., & Hsu, H.-M. (2012). Predicting medical staff intention to use an online reporting system with modified unified theory of acceptance and use of technology. Telemedicine and e-Health, 18(1), 67-73.
- Chang, I.-C., Hwang, H.-G., Hung, W.-F., & Li, Y.-C. (2007). Physicians acceptance of pharmacokinetics-based clinical decision support systems. Expert Systems with Applications, 33(2), 296-303.
- Chang, M.-Y., Pang, C., Tarn, J. M., Liu, T.-S., & Yen, D. C. (2015). Exploring user acceptance of an e-hospital service: An empirical study in Taiwan. Computer Standards & Interfaces, 38, 35-43.
- Chau, P. Y., & Hu, P. J. (2002). Examining a model of information technology acceptance by individual professionals: An exploratory study. Journal of management information systems, 18(4), 191-229.
- Cimperman, M., Brenčič, M. M., & Trkman, P. (2016). Analyzing older users home telehealth services acceptance behavior applying an Extended UTAUT model. International journal of medical informatics, 90, 22-31.
- Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS quarterly, 319-340.
- Davis, F. D., Bagozzi, R. P., & Warshaw, P. R. (1989). User acceptance of computer technology: a comparison of two theoretical models. Management science, 35(8), 982-1003.
- Davis, F. D., Bagozzi, R. P., & Warshaw, P. R. (1992). Extrinsic and intrinsic motivation to use computers in the workplace. Journal of applied social psychology, 22(14), 1111-1132.
- Dunnebeil, S., Sunyaev, A., Blohm, I., Leimeister, J. M., & Krcmar, H. (2012). Determinants of physicians’ technology acceptance for e-health in ambulatory care. Int J Med Inform, 81(11), 746-760. doi:10.1016/j.ijmedinf.2012.02.002
- Duyck, P., Pynoo, B., Devolder, P., Voet, T., Adang, L., Ovaere, D., & Vercruysse, J. (2010). Monitoring the PACS implementation process in a large university hospital discrepancies between radiologists and physicians. Journal of Digital Imaging, 23(1), 73-80.
- Dwivedi, Y. K., Rana, N. P., Jeyaraj, A., Clement, M., & Williams, M. D. (2017). Re-examining the Unified Theory of Acceptance and Use of Technology (UTAUT): Towards a Revised Theoretical Model. Information Systems Frontiers, 1-16.
- Dwivedi, Y. K., Rana, N. P., Jeyaraj, A., Clement, M., & Williams, M. D. (2019). Re-examining the unified theory of acceptance and use of technology (UTAUT): Towards a revised theoretical model. Information Systems Frontiers, 21(3), 719-734.
- Efron, B., & Tibshirani, R. J. (1994). An introduction to the bootstrap: CRC press.
- Esmaeilzadeh, P., Sambasivan, M., & Kumar, N. (2010). The challenges and issues regarding e-health and health information technology trends in the healthcare sector E-business Technology and Strategy (pp. 23-37): Springer.
- Fagan, M. H., Neill, S., & Wooldridge, B. R. (2008). Exploring the intention to use computers: An empirical investigation of the role of intrinsic motivation, extrinsic motivation, and perceived ease of use. Journal of Computer Information Systems, 48(3), 31-37.
- Foon, Y. S., & Fah, B. C. Y. (2011). Internet banking adoption in Kuala Lumpur: an application of UTAUT model. International Journal of Business and Management, 6(4), 161.
- Fornell, C., & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of marketing research, 39-50.
- Gagnon, M.-P., Godin, G., Gagné, C., Fortin, J.-P., Lamothe, L., Reinharz, D., & Cloutier, A. (2003). An adaptation of the theory of interpersonal behaviour to the study of telemedicine adoption by physicians. International journal of medical informatics, 71(2), 103-115.
- Gagnon, M.-P., Ouimet, M., Godin, G., Rousseau, M., Labrecque, M., Leduc, Y., & Abdeljelil, A. B. (2010). Study protocol Multi-level analysis of electronic health record adoption by health care professionals: A study protocol. Implementation Science, 30(5), 1-10.
- Gagnon, M. P., Ghandour el, K., Talla, P. K., Simonyan, D., Godin, G., Labrecque, M., . . . Rousseau, M. (2014). Electronic health record acceptance by physicians: testing an integrated theoretical model. J Biomed Inform, 48, 17-27. doi:10.1016/j.jbi.2013.10.010
- Gikandi, J. W., Morrow, D., & Davis, N. E. (2011). Online formative assessment in higher education: A review of the literature. Computers & Education, 57(4), 2333-2351. doi:10.1016/j.compedu.2011.06.004
- Hailemariam, G., & Garfield, M. (2016). A Contextualized IT adoption and Use Model for e-health: The Case of Telemedicine at Black Lion Teaching Hospital, Ethiopia. AMCIS 2016 Proceedings. San Diego, 1-10.
- Hair, J. F., Ringle, C. M., & Sarstedt, M. (2011). PLS-SEM: Indeed a silver bullet. Journal of Marketing theory and Practice, 19(2), 139-152.
- Hair, J. F., Sarstedt, M., Ringle, C. M., & Mena, J. A. (2012). An assessment of the use of partial least squares structural equation modeling in marketing research. Journal of the academy of marketing science, 40(3), 414-433.
- Han, S., Mustonen, P., Seppanen, M., & Kallio, M. (2004). Physicians’ behavior intentions regarding the use of mobile technology: an exploratory study. PACIS 2004 Proceedings. 49, 624-637.
- Heart, T., & Kalderon, E. (2013). Older adults: are they ready to adopt health-related ICT? International journal of medical informatics, 82(11), e209-e231.
- Holden, R. J., & Karsh, B.-T. (2010). The technology acceptance model: its past and its future in health care. Journal of biomedical informatics, 43(1), 159-172.
- Holden, R. J., & Karsh, B. T. (2010). The technology acceptance model: its past and its future in health care. J Biomed Inform, 43(1), 159-172. doi:10.1016/j.jbi.2009.07.002
- Hu, P. J., Chau, P. Y., Sheng, O. R. L., & Tam, K. Y. (1999). Examining the technology acceptance model using physician acceptance of telemedicine technology. Journal of management information systems, 91-112.
- Ifinedo, P. (2012). Technology acceptance by health professionals in Canada: An analysis with a modified UTAUT model. Paper presented at the 45th International Conference on System Science (HICSS) Hawaii.
- Isabalija, S. R., Mayoka, K. G., Rwashana, A. S., & Mbarika, V. W. (2011). Factors affecting adoption, implementation and sustainability of telemedicine information systems in Uganda. Journal of Health Informatics in Developing Countries, 5(2).
- Karahanna, E., Straub, D. W., & Chervany, N. L. (1999). Information technology adoption across time: a cross-sectional comparison of pre-adoption and post-adoption beliefs. MIS quarterly, 183-213.
- Kijsanayotin, B., Pannarunothai, S., & Speedie, S. M. (2009). Factors influencing health information technology adoption in Thailand’s community health centers: Applying the UTAUT model. International journal of medical informatics, 78(6), 404-416.
- Kissi, J., Dai, B., Dogbe, C. S., Banahene, J., & Ernest, O. (2020). Predictive factors of physicians satisfaction with telemedicine services acceptance. Health informatics journal, 26(3), 1866-1880.
- Kohnke, A., Cole, M. L., & Bush, R. (2014). Incorporating UTAUT Predictors for Understanding Home Care Patients’ and Clinician’s Acceptance of Healthcare Telemedicine Equipment. Journal of technology management & innovation, 9(2), 29-41.
- Lapão, L. V., & Lopes, M. (2013). Managing health systems in a globalized world: Telemedicine service improves access to pediatric cardiology in Cape Verde. Paper presented at the 2013 IST-Africa Conference & Exhibition.
- Lasierra, N., Alesanco, A., Gilaberte, Y., Magallón, R., & García, J. (2012). Lessons learned after a three-year store and forward teledermatology experience using internet: Strengths and limitations. International journal of medical informatics, 81(5), 332-343.
- Lee, H. W., Ramayah, T., & Zakaria, N. (2012). External factors in hospital information system (HIS) adoption model: a case on malaysia. Journal of medical systems, 36(4), 2129-2140.
- Lin, H. S., & Stead, W. W. (2009). Computational Technology for Effective Health Care: Immediate Steps and Strategic Directions: National Academies Press.
- Lister, G., & Jakubowski, E. (2008). Public engagement in health policy: International lessons. Journal of Management & Marketing in Healthcare, 1(2), 154-165.
- Maarop, N., & Win, K. T. (2012). Understanding the need of health care providers for teleconsultation and technological attributes in relation to the acceptance of teleconsultation in Malaysia: a mixed methods study. J Med Syst, 36(5), 2881-2892. doi:10.1007/s10916-011-9766-2
- Macabasag, R. L. A., Magtubo, K. M. P., & Marcelo, P. G. F. (2016). Implementation of telemedicine services in lower-middle income countries: lessons for the Philippines. Journal of the International Society for Telemedicine and eHealth, 4, e24 (21-11).
- Mansouri-Rad, P., Mahmood, M. A., Thompson, S. E., & Putnam, K. (2013). Culture Matters: Factors Affecting the Adoption of Telemedicine. Paper presented at the System Sciences (HICSS), 2013 46th Hawaii International Conference on.
- Mars, M. (2013). Telemedicine and Advances in Urban and Rural Healthcare Delivery in Africa. Progress in cardiovascular diseases, 56(3), 326-335.
- Mbarika, V. W. A., & Okoli, C. (2003). Telemedicine in sub-Saharan Africa: A proposed Delphi study. Paper presented at the 36th Annual Hawaii International Conference on System Sciences, 2003. Proceedings of the.
- Mullan, F., & Frehywot, S. (2008). Non-physician clinicians in 47 sub-Saharan African countries. The Lancet, 370(9605), 2158-2163.
- Murererehe, J., Uwambaye, P., Isyagi, M., Nyandwi, T., & Njunwa, K. (2017). Knowledge, attitude and practices of dental professionals in Rwanda towards the benefits and applications of teledentistry. Rwanda Journal, 4(1), 39-47.
- Nazari, J. A., Herremans, I. M., Isaac, R. G., Manassian, A., & Kline, T. J. (2011).
- Obi-Jeff, C., Garcia, C., Onuoha, O., Adewumi, F., David, W., Bamiduro, T., . . . Wonodi, C. (2021). Designing an SMS reminder intervention to improve vaccination uptake in Northern Nigeria: a qualitative study. BMC health services research, 21(1), 844.
- Onyeabor, U. S., Okenwa, W. O., Onwuasoigwe, O., Lasebikan, O. A., Schaaf, T., Pinkwart, N., & Balzer, F. (2024). Telemedicine in the age of the pandemics: The prospects of web-based remote patient monitoring systems for orthopaedic ambulatory care management in the developing economies. Digital health, 10, 20552076241226964.
- Organizational culture, climate and IC: an interaction analysis. Journal of Intellectual Capital, 12(2), 224-248.
- Olver, I. N., & Selva-Nayagam, S. (2000). Evaluation of a telemedicine link between Darwin and Adelaide to facilitate cancer management. Telemedicine Journal, 6(2), 213-218.
- Ozturk, M. A. (2011). Confirmatory Factor Analysis of the Educators’ Attitudes toward Educational Research Scale. Educational Sciences: Theory and Practice, 11(2), 737-748.
- Patel, R. N., & Antonarakis, G. S. (2013). Factors influencing the adoption and implementation of teledentistry in the UK, with a focus on orthodontics. Community Dent Oral Epidemiol, 41(5), 424-431. doi:10.1111/cdoe.12029
- Peeters, J. M., de Veer, A. J., van der Hoek, L., & Francke, A. L. (2012). Factors influencing the adoption of home telecare by elderly or chronically ill people: a national survey. Journal of clinical nursing, 21(21-22), 3183-3193.
- Peterson, R. A. (1994). A meta-analysis of Cronbach’s coefficient alpha. Journal of consumer research, 21(2), 381-391.
- Rho, M. J., Choi, I., & Lee, J. (2014). Predictive factors of telemedicine service acceptance and behavioural intention of physicians. International journal of medical informatics.
- Rogers, E. M. (2004). A prospective and retrospective look at the diffusion model. Journal of Health Communication, 9(S1), 13-19.
- Sagaro, G. G. G., Battineni, G., & Amenta, F. (2019). A Review on Barriers to Sustainable Telemedicine Implementation in Ethiopia.
- Saigí-Rubió, F., Torrent-Sellens, J., & Jiménez-Zarco, A. (2014). Drivers of telemedicine use: comparative evidence from samples of Spanish, Colombian and Bolivian physicians. Implementation Science, 9(1), 128.
- Santos, J. s alpha: A tool for assessing the reliability of scales. Journal of extension, 37(2), 1-5.
- Schaper, L., & Pervan, G. (2007). A model of information and communication technology acceptance and utilisation by occupational therapists. Stud. Health Technol. Inform, 130, 91-101.
- Shibl, R., Lawley, M., & Debuse, J. (2013). Factors influencing decision support system acceptance. Decision Support Systems, 54(2), 953-961. doi:10.1016/j.dss.2012.09.018
- Sitzia, J. (1999). How valid and reliable are patient satisfaction data? An analysis of 195 studies. International Journal for Quality in Health Care, 11(4), 319-328.
- Skinner, B. F. (1963). Operant behavior. American Psychologist, 18(8), 503-515.
- Susanto, T. D., & Aljoza, M. (2015). Individual acceptance of e-Government services in a developing country: Dimensions of perceived usefulness and perceived ease of use and the importance of trust and social influence. Procedia Computer Science, 72, 622-629.
- Taylor, S., & Todd, P. (1995a). Assessing IT usage: The role of prior experience. MIS quarterly, 561-570.
- Taylor, S., & Todd, P. (1995b). Decomposition and crossover effects in the theory of planned behavior: A study of consumer adoption intentions. International journal of research in marketing, 12(2), 137-155.
- Ukaoha, K., & Egbokhare, F. (2012). Prospects and Challenges of Telemedicine in Nigeria.
- van Gurp, J., Soyannwo, O., Odebunmi, K., Dania, S., van Selm, M., van Leeuwen, E., . . . Hasselaar, J. (2015). Telemedicine’s potential to support good dying in Nigeria: a qualitative study. PloS one, 10(6), e0126820.
- Venkatesh, V., Brown, S. A., & Bala, H. (2013). Bridging the qualitative-quantitative divide: Guidelines for conducting mixed methods research in information systems. MIS quarterly, 37(1), 21-54.
- Venkatesh, V., Chan, F. K., & Thong, J. Y. (2012). Designing e-government services: Key service preference structures. Journal of Operations Management, 30(1), 116-133.
- Venkatesh, V., & Davis, F. D. (2000). A theoretical extension of the technology acceptance model: Four longitudinal field studies. Management science, 46(2), 186-204.
- Venkatesh, V., Morris, M. G., Davis, G. B., & Davis, F. D. (2003). User acceptance of information technology: Toward a unified view. MIS quarterly, 425-478.
- Venkatesh, V., Morris, M. G., Sykes, T. A., & Ackerman, P. L. (2004). Individual reactions to new technologies in the workplace: the role of gender as a psychological construct. Journal of Applied Social Psychology, 34(3), 445-467.
- Venkatesh, V., Sykes, T. A., & Zhang, X. (2011). ‘Just what the doctor ordered’: a revised UTAUT for EMR system adoption and use by doctors. Paper presented at the 44th International Conference on System Sciences (HICSS), Hawaii.
- Ward, R., Stevens, C., Brentnall, P., & Briddon, J. (2008). The attitudes of health care staff to information technology: a comprehensive review of the research literature. Health Information & Libraries Journal, 25(2), 81-97.
- Xue, Y., Liang, H., Mbarika, V., Hauser, R., Schwager, P., & Getahun, M. K. (2015). Investigating the resistance to telemedicine in Ethiopia. International journal of medical informatics, 84(8), 537-547.
- Yarbrough, A. K., & Smith, T. B. (2007). Technology acceptance among physicians: a new take on TAM. Medical Care Research and Review.
- Yeow, P. H., & Loo, W. (2010). Acceptability of ATM and transit applications embedded in multipurpose smart identity card: An exploratory study in Malaysia. Applied Technology Integration in Governmental Organizations: New E-Government Research: New E-Government Research, 118.
- Zailani, S., Gilani, M. S., Nikbin, D., & Iranmanesh, M. (2014). Determinants of telemedicine acceptance in selected public