





Theoretical Models in Public Health: Two Empirical Studies
Applying Theoretical Models in Public Health Research: A Rationale Illustrated Through Two Empirical Studies
Anastasiia A. Rudenko, Oleksandr M. Ocheredko, Volodymyr P. Klymenyuk, Olena V. Tkachenko
OPEN ACCESS
PUBLISHED 31 August 2025
CITATION Rudenko, A., A., Ocheredko, M., O., Klymenyuk, P., V., Tkachenko, V., O., Applying Theoretical Models in Public Health Research: A Rationale Illustrated Through Two Empirical Studies. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6886
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6886
ISSN 2375-1924
Abstract
Contemporary public health research demands a high level of methodological rigor. The use of theory based models allows researchers to formalize complex processes, strengthen the justification of hypotheses, and improve the quality of policy decisions. This is particularly relevant for disease prevention and the analysis of healthcare service delivery effectiveness under conditions of incomplete information. While clinical trials go through phases refining theory based hypotheses and gleaning evidences using particular gear mechanism, study of population health has to do with sociological behaviour related processes of quite different kind. The conspicuous definitive feature hard to evade is equilibrium based environment. In the paper we put into practicalities equilibrium based theory driven gear mechanisms related theoretical to empirical models.
Objective: To substantiate the relevance and advantages of applying theory based approach in public health research we illustrated two empirical studies: the effectiveness evaluation of a gastroduodenitis prevention program in patients with hypertension and the study of market efficiency of health services to the patients with atrial fibrillation.
Methods: In the first study, we used premorbid moral hazard theory and expected utility theory to develop equilibrium cost-effectiveness analysis (CEA) model. The second study based upon Dranove–Satterthwaite mode driven by production process theory. Using SEM approach we transformed it to empirical model to address issues of latent variables such as information noise, quality, comfort of health services, as well as demand elasticities as important constituents of theoretical model. directly Both studies involved patient samples and included retrospective and prospective elements. Evaluators given models complexity were Monte Corlo Markov Chain (MCMC) mostly Gibbs and Hamiltonian Dynamic samplers.
Results: Theoretical based approach enabled efficiency estimation by deviation from equilibrium. In first study it is defined as optimal trade-off between losses and gains due to increase of health services volume by units while in the second market equilibrium pursued. Results indicated target groups of beneficiaries. At the whole efforts to prevent gastroduodenitis in elderly patients with essential hypertension proved to be cost-effective. Key effectiveness modifiers identified: compliance, age, hypertension stage, and participation in administered by state reimbursement program. In the atrial fibrillation pathways study, several hypotheses of the Dranove–Satterthwaite model were confirmed, indicating responsiveness of healthcare services to demand elasticities. Differences in patient preferences across clinical stages leading to equilibrium shifts were observed.
Conclusion: Theory based approach suggests powerful tools for enhancing the quality of public health research. Their application enables a deeper understanding of patient and provider behavior, supports the design of tailored interventions, and informs evidence-based health policy. The findings demonstrated that models of moral hazard and market interaction can be effectively applied to assess prevention programs and service delivery pathways within the Ukrainian healthcare context and presumably worldwide.
Keywords
public health, economic modeling, Dranove-Satterthwaite, market efficiency, healthcare services, SEM, equilibrium, premorbid moral hazard.
Introduction
Evidence based approach paves its particular way in clinical trials. Usually study begins in lab environment yielding testable hypotheses to clinical phases. Empirical models serve as gear mechanism for lab endpoints, e.g., LD50, changes in plasma lipids etc. should be converted into clinical outcomes like 5-years survival, risk of relapse, curation rate. Both stages based on theories of particular street of biological knowledge. Situation though is somewhat different in population based medical sciences e.g., preventive and health promotion medicine, health services administration, health economics, and alike. Epidemiological approach has to be coupled with theoretical developments of these disciplines. What makes the difference is the study of population health has to do with sociology and behaviour related processes with conspicuous definitive feature hard to evade is equilibrium based environment. Equilibrium based theories are getting momentum. Unfortunately their implementation demands particular gear mechanism to transpill theoretical to empirical setup. Particular culprits to get through are theoretical notions like semielasticities, regression effects, etc., along with non-observables, e.g., utilities, preferences, equilibrium values. Paper presents the application of two equilibrium involved theories: (i) the premorbid moral hazard model used to study of the effectiveness of gastritis/duodenitis risk minimisation management of hypertension ridden patients; (ii) the Dranove-Satterthwaite balance model to study the market efficiency of case pathways applied to patients with atrial fibrillation. Paper offers a brief innovative outline supported by two studies conducted by authors both dealt with health services efficiency issue. We tentatively suggest streamline of balance theories based health researches into stages: 1) problem formulation: identification of a managerial or social dilemma; 2) Theoretical Framework: adaptation and formulation of health economic, demographic, behavioral, etc. theories into analytically derived structural equations; 3) hypotheses elaboration: theory-based formulation of clear, testable assumptions; 4) Empirical Framework: transformation of structural equations into statistical models with structural elements like latent factors, paths, loadings, etc. Most promising statistical models for the purpose are SEM, Verbal SEM, QA; 5) study design and data collection: These are based on Empirical Framework and feed the data for hypotheses tests; 6) hypothesis testing and model adequacy assessment; 7) feedback to theory: generation of new research questions and identification of the model’s limitations.
Research Objective
The objective of this study is to justify the relevance and advantages of applying theoretical approach and derivative models in public health research, specifically the premorbid moral hazard model and the Dranove-Satterthwaite model. The analysis is based on two original studies that reflect different approaches to evaluating the effectiveness of preventive interventions and the organization of healthcare service delivery.
Materials and Methods
General outline: Of 7 aforementioned steps special attention should be put to stages 2 and 4 for they are most challenging. Theoretical Framework stage requires knowledge both in analytics and particular process described by theory. Given the most complicated equilibrium involved setups we use equilibrium shaped factors, e.g., price, number of services, or sometimes unobservables, e.g., utilities, quality of services along with their shifters, e.g., segment of health or insurance market, tailored population, etc. Theoretical prepositions define the set of equations, e.g., classical demand-supply system of simultaneous equations. Acknowledging equilibrium existence, we arrive at derivatives of these equations by equilibrium shaped factors. Referring to equilibrium state as such at stable zero solutions we equate analytically obtained derivatives to zero with resulting balanced model, usually SSE.
Case 1. Theoretical Framework
Perceiving the patient as a rational agent, one can determine that her behavior is aimed at maximizing the expected utilities EU(V), namely (π(V) – the risk π of a disease at a certain amount of resources spent V, u[LP1]– utilities in the event of a disease, u[LP2]– utilities in the absence of a disease, LP1 and LP2 – linear predictors of utilities in the presence / absence of the disease): Equilibrium according to theory is achieved (shaped) by optimal volume of services or resources spent V, therefore focusing on the scale of admissible decision values for V > 0, the maximization of expected utilities of patient (the first derivative by V) condition is: The rearrangement of the components of gives a convenient form of the theoretical model: The left side of the equation expresses the marginal effect of an additional unit of prevention. The effect is represented by the multiplication of marginal risk reduction of disease occurrence due to prevention by benefit of staying healthy measured by difference of utilities in two states. The right side is the weighted mean of the marginal augmentation of utilities due to increase of prevention efforts V. Weights are represented by the probabilities of the presence or absence of disease given V, e.g., propensities to develop the gastroduodenitis given hypertension treatment). The derivatives are negative since additional costs reduce utilities in both states. Thus, the right side actually describes the marginal cost of unit increase in prevention efforts by marginal expected loss of utilities. Therefore, equilibrium describes equivalence in marginal gains in utilities of the person taking on additional unit of prevention efforts due to risk reduction and marginal losses in utilities because of additional costs of such efforts. This equilibrium satisfies maximum of expected utilities and therefore is being pursued by patient as rational agent.
Case 2. Theoretical Framework
Theoretical structural equations used in case are derived based on profit maximizing behavior of provider who seeks for profit maximizing levels of three attributes: price (p), quality of services (ql), and comfort (cm). Demand is function of these, i.e., q(p,ql,cm), decreasing in price and increasing in ql and cm. The total cost are function of demand q, as well as ql and cm, so that C(q, ql, cm)=q*(a+b*ql+c*cm) + F with a+b*ql+c*cm is constant marginal cost of production and F is fixed costs. So, the profit is the function of p, ql, and cm: Profit = p*q(p,ql,cm) – C(q(p,ql,cm), ql, cm) = q(p,ql,cm)(p – b*ql – c*cm) – F. By taking first derivatives by attributes p, ql, cm and solving for their optimal (equilibrium, marked with asterisk) values given attributes elasticities of demand (we can conceptualize theoretical model in system of three simultaneous equations derived by Dranove D., Satterthwaite M.): In this case there are 3 factors shaping equilibrium, so there is 3 equations SSE unlike case 1.
Empirical Framework stage is also required of analytical skills. On this stage one transpills theoretical SSE into empirical. Latter can be put into practice. One should find appropriate «substitutes» to all theoretical notions and unobservables, referring to random effects, latent factors and path analysis if appropriate.
Case 1. Empirical Framework
We have to deal with unobservable utilities here. Utility theory implies a nonnegative scale of utility measurements, usually ordinal or metric scales applied. The latter is convenient to use for model identification. Typically, an exponential transformation of linear predictors of utilities is used (I,R,V,C are economic variables, x – factors, influencing utilities all described in study overview), i.e. Simplification leads to a final empirical balanced model, used in case 1 study: with random effect of patient ln(consti) and intercept ln(β). Regression coefficients β of factors in LP proved to be unbiased and estimable by usual ML estimators even without simplification.
Case 2. Empirical Framework
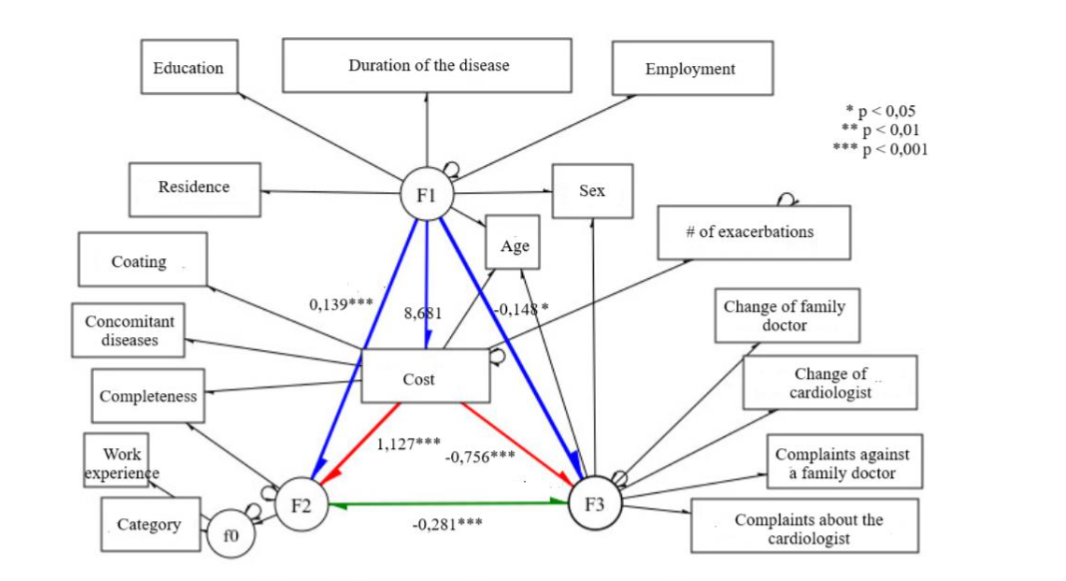
First of all we defined non-observables with the related observables. In terms of structural equation modelling (SEM) non-measurable variables are latent factors. Observables are measurable variables used to define latent factors by loadings. Latter are essentially regression coefficients so that latent factor regressed on related observables and so defined by them. For instance, quality of services (F2) is latent factor defined by hospital length of stay, surgery complications risks, quality of personnel, etc. The other latent factors are comfort of services (F3), and information noise (F1). Presence of F1 is a trick to render elasticities effects for F1 greatly influences all three of them. There are no demand elasticity coefficients per se among associations. Their influence on equilibrium values of attributes is traceable through associations of F1 with price, F2, and F3. We wrapped up these in SEM framework, so empirical model can be graphed in SEM terms: latent factors are encircled and named with beginning letter “F”, observable variables are beveled with rectangles, single-headed arrows denote directional associations, while two-headed indicate variances and covariative associations.

X1 and X2 are loadings of F1, they are factors that explain F1, like education, age, medical experience, etc. So are X3,X4,… that influence quality and X5,X6,… formulating comfort. Equilibrium values are substituted with observed values of attributes. Would we had have arrived at significant regression effects of F1 on price, quality of hospital services (F2), and comfort (F3) (marked with blue arrows) we would conclude that observed values of attributes are not so far from the equilibrium and so we have efficient health services in terms of their response to market environment. Supportive to theoretical equilibrium equations of Dranove D., Satterthwaite M. are regression effects of price on quality of health services and comfort (distinct with red arrows).
First Study Overview
The primary objective was to assess the optimal management efforts and medical input to prevent gastroduodenitis in elderly patients with essential arterial hypertension. Treatment of hypertension can instigate development and progression of gastroduodenitis. Although gastroduodenitis prevention programs are already established and implemented globally, regional characteristics are often overlooked. In Ukraine, the government’s “Affordable Medicines” program provides free medications for patients with essential hypertension though suspected to be less efficient and side effects prone. Therefore, the study was called for. To lay evidence-based foundation we opted for economic theory of patient as rational agency which was used to develop balanced cost-effectiveness empirical model. By having equilibrium operationalised we filled in two essential hard-to-address other way gaps: a) notorious effect-cost trade-off dilemma, b) blatant comparison of clinical effects routinely done at non-optimal volumes of treatment. One can add also problem of classical CEA to accommodate confounders. Efficiency given new opportunity best to address in terms of deviation from equilibrium. In the study it is defined as optimal trade-off between losses and gains due to increase of health services volume by unit. Exact formulation and technicalities of equilibrium derivation are given in. We judged on efficiency both in IECR (Incremental Effectiveness-Cost Ratio) and IBCR (Incremental Benefit-Cost Ratio) terms. The main hypothesis concerns benefit of participation in state reimbursement and preventive programs. We used nested panel design. Nesting accounts for physician, family, local health unit. Data obtained on elderly patients with essential arterial hypertension during 17 years. The methodological foundation pivoted on the premorbid moral hazard that induces behavioral response of patients while deciding whether to participate in preventive and reimbursement programs. Data collection involved patient surveys and analysis of medical records. Variables included age, gender, education level, social status, comorbidity, treatment compliance, economic variables required by theoretical framework, and social support. We reduced selection bias due to possible randomness blemishes in allocation to the PP by control function method.
The intervention group included 100 elderly patients with a history of essential hypertension (ranging up to 17 years) who developed gastroduodenitis due to antihypertensive therapy. The control group consisted of 50 elderly hypertensive patients (also up to 17 years of illness duration) who had not developed gastroduodenitis. In addition to general approaches, we identified specific categories of patients with essential arterial hypertension for whom gastroduodenitis prevention strategies require tailored management. These categories included: a) patients taking anticoagulants and/or antiplatelet agents who report gastrointestinal (GI) symptoms; b) patients taking anticoagulants and/or antiplatelet agents without any GI complaints; c) patients taking nonsteroidal anti-inflammatory drugs (NSAIDs) who report GI symptoms; d) patients taking NSAIDs without any GI complaints; e) patients with resistant hypertension and concurrent GI symptoms. Patients with resistant hypertension but without GI complaints; f) patients on long-term therapy with drugs that reduce lower esophageal sphincter tone and without GI complaints; g) patients on long-term therapy with drugs that reduce lower esophageal sphincter tone and with GI symptoms; h) patients receiving only antihypertensive therapy and reporting GI complaints. These subgroups were analyzed by CEA and CBA coefficients supplied by equilibrium model. MCMC samplers were used to estimate model parameters.
Second Study Overview
The main objective of the study was to evaluate market efficiency of health services administration to the patients with atrial fibrillation. In parallel we studied clinical and CEA efficacy of different care pathways as well as of the set of factors affecting clinical outcomes, which are transition to the next stage of disease, instances of complications (stroke, Pulmonary Embolism (PE), acute myocardial infarction (AMI)). Among others were qualification and experience of physicians, comorbidity, ownership and type of healthcare facilities. It is well established that the course of atrial fibrillation (AF) influences the likelihood of complications; however, we did not find any specific studies conducted within the territory of Ukraine. Furthermore, while reviewing international literature, we did not identify studies that comprehensively assessed the healthcare system’s organization by considering not only clinical but also organizational aspects of healthcare provision.
Theoretical Framework. To build an evidence base, we conducted an analysis of the market efficiency of healthcare service delivery to individuals with atrial fibrillation, based on the theoretical model developed by D. Dranove and M. Satterthwaite. Model derived from economic theory of firm and production process. System of simultaneous econometric equations that describe market equilibrium are derived based on profit maximizing behavior of provider who seeks for profit maximizing levels of three service attributes: price, quality, and comfort. The model possesses broad applicability, as it describes the production of any service under conditions of market competition. It establishes a relationship between the core attributes of a service—namely, quality and comfort—and key market characteristics such as demand and price, through their respective elasticities. This integrated framework of variables and parameters enables the determination of equilibrium values for price, quality, and comfort—values that represent a dynamic equilibrium and are thus considered optimal within the prevailing market environment.
Empirical Framework. We can’t put theoretical model to practice, for it enlists unobservables (e.g., demand elasticities, equilibrium values, etc.). We elaborated the general technique on transformation of theoretical SEQ to SEM. Hypotheses elaboration. The rationale for applying this model lies in the assumption that if the structure of equilibrium it predicts are confirmed by the data on service delivery, then the current values of the three key service characteristics (price, quality, and comfort) are to approximate their optimal values. The D. Dranove and M. Satterthwaite SEQ suggest fulfilment of certain statements that lay foundation to the set of hypotheses we tested in the study, hypotheses with tests described in results. Study design and Data collection. We used nested panel design. Nesting shaped by physician, local health unit. Data collected on 600 patients who received medical care across different healthcare system levels and 5 routes. Route 1 was particular, as it was the only pathway that did not involve inpatient care. This route served exclusively patients with the persistent form of AF. However, it is also an integral part of more complex routes. A large proportion of patients with atrial fibrillation were treated either directly via this route or through a care trajectory that included it. Two hundred patients received care at supracluster-level facilities. One hundred were treated at primary and cluster-level facilities. Two hundred patients received treatment only at the primary care level, and 100 received primary care services in an online format. All patients were of different ages and from various places of residence. Employment status, time the patient spent in each progressive clinical form of atrial fibrillation, characteristics of case management. Important factors also included the work experience and category of primary care physicians, outpatient cardiologists treating the patient, and inpatient cardiologists managing patients with AF. Additional quality-related factors included how frequently physicians changed, whether any patient complaints about physicians were recorded, doctor’s notes on patients’ non-adherence to prescribed treatments (compliance), the ownership form of the healthcare facility, and the patient’s geographical accessibility to the healthcare facility. Outcome variables measured by timing of clinical endpoints documented by physicians, e.g., transition to next clinical form of AF, incidence of stroke, TELA, AMI. Costs of services rendered annually were accounted for. Both retrospective and prospective research designs were applied. Although the study is still ongoing, the current findings on market efficiency of services are presented in this paper.
Results
Case 1. Study on effectiveness of gastroduodenitis prevention program in elderly patients with essential arterial hypertension with the application of the premorbid moral hazard model yielded the following key findings:
The main effect of program participation is significant in a model of fixed effects (β = -0.269; p = 0.0156), and even more supportive in the mixed model (β = -0.282; p = 0.0097). Other components with a variable “PP participation”, namely participation in the program given the group, participation in the program given GP duration, participation in the program given compliance, appeared to be nonsignificant, that suggest absence of substantial selection bias due to non-randomness of allocation. The greatest risk reduction due to program participation was in patients with hypertension who do not receive antihypertensive therapy. In groups a) – e) with more aggressive hypertension treatment the effects of program participation was obvious but less pronounced. Threshold cost values for the prevention program were identified, indicating the individual and group optimal volume of services. The effectiveness of the program was shown to be significantly influenced by patient motivation and levels of social support. Predictive models were developed to estimate the long-term impact of preventive measures in reducing hospitalizations due to gastroduodenal complications. The use of balanced model enabled estimation of the range of potential costs and benefits under varying patient participation scenarios. The study confirmed the critical role communication management and personification of preventive measures play in enhancing the overall efficiency of the program.
Case 2. Evaluation of market efficiency of health services administration to the patients with atrial fibrillation.
The SEM analysis confirmed hypotheses derived from the Dranove-Satterthwaite model, proving the market efficiency of health services to patients with AF. Among others, significant negative impact of informational noise on both quality and comfort of healthcare services observed, positive association between quality, comfort, and the cost of service provision unveiled. Acceptance of these hypotheses indicated a convergence of cost, quality, and comfort of healthcare services toward a market equilibrium. The hypotheses concerning information noise are particularly important, their validation suggested that reduced individual elasticity of demand (by price, quality, or comfort), due to insufficient patient awareness, leads to a simultaneous decline in cost-efficiency, quality, and comfort levels in healthcare services. Findings advocated for overall market efficiency of health services administration to the patients with atrial fibrillation. Case management pathways were identified with indicators of quality, comfort, and cost closest to theoretical equilibrium values, suggesting their market efficiency. The model enabled identification of key barriers reducing the effectiveness of care delivery and supported the recommendations for pathways optimisation.
Discussion
Evidence based research takes hold in clinical studies of consequential phases. In lab stage, they may use standard research setup with standard effects. Hypotheses are built on specific theories accompanied by evidences on similar drugs/cultures. Say, hydroxychloroquine (EC50 = 0.72 µM) is three times more potent than chloroquine (EC50 = 5.47 µM) in SARS-CoV-2 infected cells in vitro. Clinical stage hypothesis substantiated with these lab stage findings put as: «Based on PBPK models results, a loading dose of 400 mg twice daily of hydroxychloroquine sulfate given orally, followed by a maintenance dose of 200 mg given twice daily for 4 days in SARS-CoV-2 infection cases reaches 3 times the potency of chloroquine phosphate. The gear mechanism are PBPK models known to virologists along with research setup. We use this example to demonstrate difference with health population based studies. For the most part they lack lab simplicity and reproducibility. In part, they are ridded of applicable clearcut theories. Additional complexity is introduced by behavioural nature of societal processes, where individuals or groups pursue some interests, profits, benefits, preferences, utilities whatever willing to maximise them. This is where equilibrium issue comes upon the scene which can solve multilateral interests competition or to the same safeguard benefit/loss optimal balance, better known in health research as cost-effectiveness optimisation. Therefore, wide spectrum of population health related researches should exploit equilibrium oriented theories. This is quite a new ground we tentatively explore. The hope is it’s manageable and as cases demonstrate worthwhile to develop for its numerous benefits and attractions. We illustrated two different applications. First based on individual preferences/risks, accordingly the theory of moral hazard put forth with equilibrium shaped by program efforts. The optimal trade-off between benefits in terms of risk minimisation and losses due to inconveniences, time, resources defines equilibrium as optimal consumption of services. Equilibrium is individual and shifts with different factors. Such construct permits to compare influences for the collation is no more odious. Rather it based upon optimal trade-off. To the contrary had one compare treatments each far from optimal personal dosage the results would have been equivocal. So to measure program participation benefit and losses one has to render individual trade-off which is done by the construct. It incapacitated conclusion on efficiency of program participation given natural adaptation to opt for personalised management efforts. Second case based on market equilibrium detailed in profit maximisation given demand constraints. Equilibrium shaped by main services attributes: price, quality, and comfort. SEM used as gear mechanism from theoretical to empirical framework. Application is different from previous in that we measure efficiency in terms of deviation from/reaching equilibrium. Accepting hypothesised by equilibrium model relationships indicate proper responses to market impetuses driving main attributes to equilibrium values. We may have audacity to claim there is no other way to check market efficiency beyond equilibrium. Any influences have their impact on equilibrium shifts. If health services quick to adapt to challenges then they are efficiently managed. Findings strongly suggested market efficiency of health services administration to the patients with atrial fibrillation. We should note that theory may not pursue equilibrium with great relief on SEQ SEM transformation step. Such are on the biochemistry, immunology, physiology streets. Theory then put into practice to explain structure of relationship and necessary variables. One can use such to develop evidence framework for most clinical trials. Extensions to two exemplified approaches may consider achieving the following objectives: a) further enhancing the validity and reliability of scientific conclusions; b) uncovering hidden patterns and dynamics within the healthcare system; c) justifying the need for changes in existing health services administration and financing.
Conclusions
The application of theory-based models significantly enhanced the analytical quality and policy relevance of public health studies. The first study, using the premorbid moral hazard model, demonstrated that tailored gastroduodenitis prevention in elderly hypertensive patients is both clinically and economically justified. Participation in the state “Affordable Medicines” program, patient compliance (β = 0.80; p < 0.00001), age, and hypertension stage were significant effect modifiers. The prevention program showed a weighted average cost-saving of $1.58 per $1 spent, with subgroup-specific benefits reaching $4.02 in high-compliance married patients. Average risk reduction (Δπₐₜₑ = 0.351; p < 0.001) was highest in patients not yet on antihypertensive therapy. The second study, grounded in the Dranove–Satterthwaite market equilibrium model, revealed that outpatient-only care pathways (Route 1) for atrial fibrillation aligned well with theoretical equilibrium, confirming 5 of 6 hypotheses. In contrast, inpatient-dominant routes confirmed only 3 of 6 hypotheses, indicating a shift in demand elasticity toward quality and reduced responsiveness to price or comfort, especially in severe disease stages. Informational noise was a key negative factor across all pathways. These findings confirm that service organization in more complex clinical scenarios requires optimization based on evolving patient preferences and supports use of SEM for healthcare system efficiency evaluation.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
No financial disclosure.
Acknowledgements:
No acknowledgements.
References:
- Akhmedova AA. Otsinka efektyvnosti prohramy profilaktyky hastropatii u patsiyentiv pensiynoho viku z hipertonichnoyu khvoroboyu. In: Pershyy krok v nauku – 2020: Materialy XVII Naukovo-Praktychnoi Konferentsii Studentiv ta Molodykh Vchenykh z Mizhnarodnoiu Uchasiu. Vinnytsia National Pirogov Memorial Medical University; 2020:479.
- Akhmedova AA, Ocheredko OM. Adaptatsiya teoretychnoi modeli premorbidnoho moralnoho ryzyku dlia praktychnoho vchyennya ekonomichnoi efektyvnosti pervynnoi profilaktyky polimorbidnoi patolohii za metodamy vytraty–benefity ta vytraty–efektyvnistʹ. In: Zdorov’ya i suspilʹni vymiry v akademichnomu prostori ta poza nym: Materialy Mizhnarodnoi Konferentsii. Vinnytsia National Pirogov Memorial Medical University, National University of “Kyiv-Mohyla Academy,” Maastricht University; 2017:35-36.
- Akhmedova AA, Ocheredko OM. Obgruntuvannya modeli kliniko-ekonomichnoi otsinky efektyvnosti prohram profilaktyky, likuvannya ta dispanseryzatsii patsiyentiv z komorbidnymy stanamy na prykladi patsiyentiv z pidvyshchenym arterialnym tyskom ta duodenitom. Wiad Lek. 2018;71(3 pt. 1):479-484.
- Akhmedova AA, Ocheredko OM, Klimenyk VP. Assessment of the effectiveness of the gastropathy risk reduction program in patients with arterial hypertension. Wiad Lek. 2019;72(3):409-417.
- Akhmedova AA. Evaluation of the effectiveness of the prophylaxis of gastropathy in patients with hypertension. In: Pershyy krok v nauku – 2019: Materialy XVI Naukovo- Praktychnoi Konferentsii Studentiv ta Molodykh Vchenykh z Mizhnarodnoiu Uchasiu. Vinnytsia National Pirogov Memorial Medical University; 2019:424-425.
- Klimenyuk OV, Ocheredko OM, Klimenyuk VP, Rudenko AA. Analiz povedinky balansovykh znachenʹ vytrat, yakosti ta komfortu medychnykh posluh v zalezhnosti vid medychnoi osvity patsiyenta. Klinichna ta profilaktychna medytsyna. 2023;(2):81-88.
- Ocheredko OM, Klimenyuk OV, Rudenko AA, Klimenyuk VP. Sample size calculation in structural equation modeling of equilibrium. Wiad Lek. 2023;76(12):2641-2647. doi:10.36740/WLek202312113
- Dranove D, Satterthwaite M. Monopolistic competition when price and quality are imperfectly observable. Rand J Econ. 1992;23(4):518-534. doi:10.2307/2555903
- Ocheredko OM. Elaboration of economic cost-efficiency analyses based on equilibrium approach. The 2020 Meeting of ISDSA, Notre Dame, IN, USA. https://drive.google.com/file/d/10NOW1RwOO40haBDTBr80Y0YQX11JSbIV/view
- Xueting Yao, Fei Ye, et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clinical Infectious Diseases, ciaa237, https://doi.org/10.1093/cid/ciaa237 Published: 09 March 2020.