

Theory of Action in Art-Based Mental Health Rehab
Towards an Empirically Informed Theory of Action of the Art-based Mental Health Rehabilitation Program All on Stage
Kim Archambaulta, Noémie Beauregardb, Sarah Dufourc, Isabelle Archambaultd, Patricia Garele,
1.Kim Archambault
Associate professor, School of Psychoeducation, University of Montreal, 90 Vincent-d’Indy avenue, Montreal, Canada.
2.Noémie Beauregard
PhD. studen.t, School of Psychoeducation, University of Montreal, Montreal, Canada.
3.Sarah Dufour
Full professor, School of Psychoeducation, University of Montreal, Montreal, Canada.
4.Isabelle Archambault
Full professor, School of Psychoeducation, University of Montreal, Montreal, Canada.
5.Patricia Garel
MD Psychiatrist, Sainte-Justine University Hospital Center, 3175 Chem. de la Côte-Sainte-Catherine, Montreal, Canada.
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION Archambault, K., Beauregard, N., et al., 2025. Towards an Empirically Informed Theory of Action of the Art-based Mental Health Rehabilitation Program All on Stage. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6702
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i7.6702
ISSN 2375-1924
ABSTRACT
Despite increasing evidence supporting the efficacy of art-based programs for mental health rehabilitation, the active ingredients and therapeutic processes of these interventions are still poorly understood. In the present study, our objective was to empirically derive the theory of action of the program All on Stage, an innovative art-based rehabilitation program for youths with stabilized mental disorders. We conducted individual and group semi-structured interviews with twenty-four participants at post-program and three-month follow up. At post-program, we similarly interviewed the artists and psychoeducator who facilitated the program and the clinicians who referred participants to it. We also collected field observations throughout the program using a participatory approach. We performed qualitative thematic analyses on all relevant material. Analyses revealed four mechanisms that seem to be at work in the program: 1) social experience and gratification, 2) desensitization by gradual exposure, 3) success and valorization, and 4) normalization. The emergence or impact of these mechanisms appeared to be favored by various program characteristics, including the non-clinical setting and facilitation of the program, the heterogeneous composition of the groups, the use of performing arts, and the pursuit of a collectively achieved artistic product and its sharing with an external public. Our study offers a rare example of inductive theory building in the context of a real-world program evaluation. Study conclusions can guide the planning and delivery of future initiatives in the fields of youth mental health and arts in health.
Keywords: Youth, mental health rehabilitation, art-based interventions, theory of action, process evaluation
INTRODUCTION
It is now widely admitted that art-based interventions can play key roles in health promotion, the prevention of health problems, and the management and treatment of a range of different conditions, including mental disorders. Despite the growing body of evidence supporting the relevance and efficacy of such initiatives and their widening use among mental health services, art-based interventions are still poorly understood in terms of active ingredients and therapeutic processes.
The specification of a chain of causal assumptions linking a program to its objectives is commonly referred to as a theory of action, although other terms are sometimes used (e.g., theory of change, program theory, logic model). Research informing the theory of action behind art-based interventions for people with mental health problems has been scarce and is largely warranted. Knowledge about the mechanisms that mediate between the delivery of a program and the emergence of the outcomes of interest can foster improved program planning and management, support higher-quality evaluations, and contribute to fundamental theory about given issues. Recent review and consultation work has provided enlightening insights into the mechanisms of action of leisure activities and the active ingredients of arts-in-health initiatives, but very few studies have empirically investigated how art-based programs may produce benefits on the health and well-being of participants. The aim of the present study is to contribute to the limited understanding of the mechanisms underlying arts-for-mental-health interventions by empirically deriving a theory of action of the mental health rehabilitation program All on Stage.
THE PROGRAM ALL ON STAGE
All on Stage is a group-based participatory arts program developed by mental health practitioners in collaboration with professional artists. The main goal of the program is to foster the psychosocial rehabilitation of adolescents and young adults with mental health issues. Consistent with a personal recovery framework, it focuses on enhancing strengths and capacity rather than on symptom reduction. Hence, at the proximal level, it aims at improving participants’ affect, self-perception, social comfort and competence, and global functioning. The program is intended for individuals aged 14 to 25 years and primarily targets youths presenting with mental disorders of varied kinds for which they have received clinical services and sufficient stabilization of acute symptoms has been reached. In groups of 12 to 15 youths, these “target participants” are mixed with approximately one-third of same-age peers who do not present any mental health or adjustment problems requiring special services (henceforth “general population participants”). The relevance and adequacy of the program for each potential participant are assessed by experienced clinicians who do not share any clinical information with the artist facilitators and co-participants and encourage every youth to play a similar role in the program.
Workshops are two hours long and take place twice weekly during twelve consecutive weeks in a community setting. The program mainly consists of drama and circus workshops, including various exercises centered on self-expression, creative and physical exploration, as well as the acquisition of theater and acrobatic skills. Collective exercises favoring socialization are included in every workshop, and special care is devoted to the creation and preservation of a secure, non-judgmental environment. At the end of the program, participants are encouraged to present a collectively created work to a public of their choice. Workshops are facilitated by experienced artists who are not therapists, and clinical support is provided by the constant presence of a mental health practitioner. When necessary, this accompanying clinician (AC) follows up with the participants between the workshops and exchanges clinical information with their treating staff. An experienced team composed of a psychiatrist, a psychoeducator, and a multidisciplinary artist provides initial training to facilitators and supervises the delivery of the program.
We subjected All on Stage to a first independent evaluation during its second year of implementation. A thorough implementation assessment revealed that the program was relatively successful at reaching its target population and delivering its key planned components. Participants’ attendance was also found to be elevated, as were their global appreciation of the program and quality of participation. Furthermore, we conducted a mixed-methods evaluation of the program’s effects on target participants. We found that for most of them, aspects of global functioning, such as increased activation and decreased isolation, were significantly improved following the program, and that social comfort and competence, as well as self-perception, were improved in a fair proportion of them.
STUDY OBJECTIVE AND METHODOLOGICAL APPROACH
In the present study, we aimed to empirically identify the mechanisms leading to these reported positive effects and to integrate them into a comprehensive and explicit theory of action. In line with an empirical approach to program theory development, we inductively generated the program’s theory of action from interviews with involved actors and from direct participatory observation. We performed a selected review of relevant research literature a posteriori to compare and contextualize empirical results. We relied on naturalistic methods to capture the program in its “real-world” context of implementation. We consulted multiple informants and used two methods of data collection—interviews and participatory observation—to optimize the exhaustiveness and validity of the portrait obtained. We investigated two consecutive program sessions. Approval from the Institutional Review Board of all four sites of recruitment was obtained.
METHODS
PARTICIPANTS
The study sample was composed of all participants who completed one of the two evaluated program sessions (N = 24), as well as the two artist facilitators, the AC, and the clinicians who referred participants to the program (N = 9). Target participants (N = 15, 62.5%) were referred to the program by their treating psychiatrist or other mental health practitioner from four different hospitals in the same metropolitan area, whereas general population participants (N = 9) were mainly enrolled via word of mouth. The research team did not interfere with recruitment in the program and only contacted participants once enrolled to ask for their involvement in the study, which they all agreed to. All study participants, and one of their parents in the case of those aged under 18 years, provided written consent prior to the onset of the research procedures.
A nearly equal number of male (11; 45.8%) and female (13; 54.2%) participants made up the sample, their age varying between 13 and 23 years at program entry (M = 18.6 years, SD = 3.2). Target participants presented with a variety of mental health problems, namely anxiety, depressive, psychotic and eating disorders, as well as ADHD and relational or conduct problems. As for the other respondents (i.e., facilitators, AC, and referrers), 10 out of 12 (83%) were women. Among the nine referrers specifically, there were three child and adolescent psychiatrists, two psychiatric nurses, two social workers, one psychologist, and one psychoeducator. In every case, they were among the primary care providers of the participants they referred to the program.
DATA COLLECTION PROCEDURES
Interviews. We conducted individual semi-structured interviews with all program participants, the facilitators, the AC, and the referrers at post-program. We also re-interviewed all but two target participants approximately three months after program completion. Additionally, we conducted group interviews after each of the two evaluated program sessions, gathering 6 of the 9 participants to the first session and 13 of the 15 participants to the second. Individual interviews generally took place at the home or treatment center of participants and at the workplace of other respondents. Group interviews were conducted in university facilities. Individual interviews lasted on average 10 minutes (SD = 6:35) and group interviews, 52 minutes (SD = 3:19). All interviews were audio recorded and transcribed into written text afterwards. A single qualified professional clinician-researcher, the first author, conducted all the interviews to minimize procedure variability and ensure adequate support to the respondents if needed.
Individual interviews followed a semi-structured canvas, which was not limited to the present study’s objective and was composed of open questions on program experience and appreciation as well as direct questions on a variety of aspects of program implementation, effects, and putative mechanisms of action. With regards to the latter, we directly asked respondents what they believed may have produced the changes they had attributed to the program (e.g., “How do you explain these changes?”). Group interviews did not include any direct questions about program mechanisms but served to gather participants’ perceptions regarding the implementation of various program components (e.g., types of activities, program climate, final performance) and their general experience of the program.
Field observations. In addition to interview data, we gathered direct observations. We opted for a participatory observation approach to collect optimally rich and contextualized information and to reduce the potential impact of observation by an external actor on the behavior of participants and staff. The first author observed twelve workshops equally distributed throughout each of the two sessions under evaluation. Immediately after each of these workshops, she recorded her field notes in a semi-structured grid specifying the dimensions of interest, a recognized approach in field research. Observations focused on various aspects of program implementation and processes (e.g., quality of delivery, quality of participation, social interactions) and the grid included a specific section on putative mechanisms of action.
ANALYSES
We submitted interview and observation data to thematic analysis, a technique which consists of systematically identifying, codifying, and analyzing the themes addressed in a given corpus. First, as part of the broader program evaluation, we broadly categorized the totality of the interview material in accordance with the research questions it answered (e.g., implementation of specified program components, observed program effects, explanations of program effects). Then, we codified the material comprised under each of these large rubrics in an inductive manner to allow the free emergence of all the themes raised by respondents. We subsequently codified field observation notes using the thematic tree developed in preceding steps, yet in an open enough fashion to allow the emergence of new themes if appropriate. At every level of codification, we identified the themes in the verbatim of all the respondents or in the entire set of field notes in a horizontal fashion. We used the computer software QDA Miner 3.2 to assist in coding.
For the present study, the themes that we derived from the codification of material directly reflecting factors or mechanisms that could have explained the effects attributed to the program (i.e., under the rubric explanations of program effects) served as our first level of results. Then, we complemented these themes with relevant material pertaining to the implementation of different program components and characteristics (i.e., under different implementation themes) whenever we judged such material to add precision, context, or comprehensiveness to the provided explanations of program effects. For instance, when respondents or the observer raised putative explanatory mechanisms that took place around the final public performance, we integrated relevant material comprised under the final performance implementation theme to the analysis of these suggested mechanisms. Ultimately, we drew relations between the identified putative mechanisms of action, program components, and recorded program effects and integrated all of these into a global theory of action.
The entire coding and analysis were performed by the first author, who, at the time of data collection and analysis, was independent from the program yet greatly immersed in it through her field observations and collaborative research approach. Throughout the entire process, she kept a reflective journal and regularly shared thoughts and intermediary results with co-authors, including independent research supervisors and program stakeholders, to challenge, validate, or enrich analytic decisions and conclusions.
RESULTS
Our analysis revealed four mechanisms that seem to be at work in the program All on Stage: 1) social experience and gratification, 2) desensitization by gradual exposure, 3) success and valorization, and 4) normalization. In the next sections, we present these mechanisms, along with illustrative verbatim extracts.
SOCIAL EXPERIENCE AND GRATIFICATION
A great proportion of the tentative explanations provided by respondents to account for the effects that they attributed to the program pertained to the social interactions domain and referred to the group-based nature of the program. For some respondents, the simple fact that the program offered participants the occasion to acquire social experience by being in the company of people was among its major mechanisms of action. According to their sayings, the program offered a privileged context of exposure to contact with others and practice of basic social skills: “There are not so many other moments in his life when he is much in contact with others, but it gave him a good practice setting” (referrer). A few respondents more specifically alluded to the realization by some participants of their role and place in the group. For some, this theme referred to the recognition of the positive role they played in relation to others: “Yes, I discovered that I could be useful, that I wasn’t nothing. Because if I hadn’t been there, there are some things in the show that wouldn’t have been the same, and the scene would not have been the same” (target participant). For others, it referred to the increased awareness of the impact of one’s behaviors on others, of others’ expectations, and of the fact that one has to take others into account and be accountable to them: “The group was very useful: the regularity, the fact of having to be there, because if he wasn’t coming, it disorganized the final performance, so the commitment. It is a young man who is a bit immature regarding his commitment to others (…). So there is something of a certain altruism initiation and realization of the consequences of his behavior on others that was useful” (referrer).
Furthermore, certain respondents mentioned that the program represented a rare occasion for some participants to experience social gratification, such as feeling a sense of belonging to a group: “To have done it as a team, it brings these people closer. They are often alone in their head, their emotions, in their bodies. It’s like winning the game as a team; it brings participants closer to each other. To enjoy success as a gang creates a sense of belonging” (facilitator). Concordantly, the great majority of participants qualified their interactions during the workshops as globally satisfying to very positive, despite some difficult initial or sporadic interactions in certain cases: “It felt good to have social interactions. I am someone who’s more or less solitary in general, but it felt really good, everybody was respectful” (target participant). The final performance, in particular, was seen as a powerful catalyst for group cohesion by some respondents, which was also objectified by the field observer, who noted abundant interactions between participants directly following each performance and heightened enthusiasm and closeness characterizing these interactions.
A few participants mentioned the support received from their peers during the workshops as a factor contributing to the production of certain positive program effects: “I was often with X when we went out to smoke, and I could talk to him about my problems, and he would listen to me. I had problems all week long, and when I would get to the activity, it would calm down, and it was all right. Better than talking to adults who don’t understand a thing” (group interview). Many instances of mutual support and encouragement were also noted during field observation sessions, mostly verbal but also through applause and discreet physical demonstrations (e.g., pat on the back). Already at the end of the first workshop of one of the sessions, for instance, some participants offered to accompany a peer on her way home since she had expressed anxiety about using public transportation at night on her own. Although observed interactions between target and general population participants were mostly documented as undifferentiated (i.e., on an equal-to-equal basis), it was noted that, at times, the latter provided warranted and adequate support to peers who seemed to be particularly challenged. The latter observation was echoed in the verbatim of one of the participants from the general population: “Those who did not come from psychiatric referrals, we tried to help: to be calmer, to bring back the others, even to participate more in the activities to show that it didn’t matter. It helped a lot (…). Some youths also told me that it helped them, that it calmed them.” A fair proportion of participants reported that the different exercises and activities offered were favorable to social interactions and group cohesion: “I thought it was good. The group activities promoted good cohesion because, at first, we wouldn’t talk to each other as much.” “Yes, even if we were shy at the start, we didn’t have a choice but to be in the group. It was good; we ended up knowing each other” (group interview). Moreover, certain participants raised that the program’s informal moments, such as snack breaks, also allowed them to experience positive interactions with co-participants: “We socialized a lot during breaks; we chatted as with friends that I would have seen outside [the program]” (general population participant). However, an important proportion of participants expressed that they wished they could have had more occasions to socialize during the workshops, notably through opportunities to share in a collaborative creative process or to help each other practice: “we could have helped each other (…) it would have been a cool way to interact because often, there were more interactions between us and [the facilitator]. We would go one by one, and he would give us advice individually” (group interview). Field observation allowed for the identification of several types of group exercises that helped participants get to know each other or fostered the development of their social skills and comfort with others. The human pyramids exercise, a milestone of the circus workshops, appeared to be an emblematic example as it required participants to accept holding on to each other physically and closely, to trust those from lower positions that they would have the strength to support the others and those from upper positions that they would preserve their balance, and to efficiently collaborate in order for the entire formation to take shape and hold as intended. In line with the participants’ accounts however, the observer noted the paucity of activities promoting social interactions in some workshops, which seemed mainly due to the amount of structure and directedness of the facilitation. Lots of interactions were nonetheless observed during the informal moments, most of which appeared highly positive (i.e., characterized by laughter, friendly gestures, etc.). The field observer globally objectified a gradual increase in spontaneous interactions between participants throughout each program session.
DESENSITIZATION BY GRADUAL EXPOSURE
An important number of respondents reported mechanisms related to processes of desensitization through gradual exposure to explain some of the positive changes that they attributed to the program. These included reductions in shyness and fear of others’ negative judgment and consequent increases in relational comfort and openness. Respondents mentioned the gradual experimentation of diverse anxiety-eliciting or otherwise uncomfortable situations, often followed by the realization that these were not accompanied by negative consequences: “The little activities that show us that it doesn’t matter if we do silly things (…) we laugh at each other and we just have fun. It shows us that in life, we can be anybody, anything, anywhere, and we can have fun. That’s what helped me. Because I understood that in life, you just do what you think and you let go a bit of others’ ideals” (target participant, follow-up). Most respondents described situations specifically implying self-expression and/or the performance of unusual actions while exposed to the gaze of others: “X was so afraid to look ridiculous during the first exercises. He would even sometimes categorically refuse to play themes in front of others, saying that he was not comfortable with that. Finally, he went and dared to go a little further into the ridiculous to realize that everything went well and that nobody was laughing at him” (AC). For some participants, it seems that mere exposure to the group setting already represented a significant challenge and that simple social habituation may have led to important gains in social functioning: “The first workshops were very stressful because I knew only one person (…). Then, two or three weeks later, I started to get used to it and to ignore people. I started to relate a little more to people and talk to them more. Towards the last workshops, I opened up completely; I got used around people” (target participant). Based on field observations, the drama exercises seem to have particularly elicited gradual desensitization processes. In fact, many of them entailed the experimentation of awkward body positions, unusual movement or language utilization, voice projection and other self-expression techniques, while being constantly and increasingly exposed to others’ gaze. The final performance, which required that participants perform loudly and convincingly while exposed to the additional gaze of friends, families, and strangers, appeared to have represented the apogee of exposure situations, according to many participants as well as to field observations: “Certainly, that making a show in front of people, personally I found that it was a good experience because I am someone who doesn’t really like to express myself that way in a group. I am more of the reserved type. To be able to do the bacon on the floor and to let go of our foolishness, I think it helped me” (general population participant). Some respondents even highlighted the importance of the public representation in terms of social anxiety and stress modulation training: “What’s good in that is that it gives us a life experience that we can progress under stress if we manage it well” (group interview). The mutual support reported in the previous section appears to have considerably favored involvement in exposure activities, as mentioned by a few respondents and especially as noted by the field observer. In fact, it was observed on several occasions that reluctant participants were eventually led to take part in embarrassing or otherwise challenging exercises by a co-participant who offered to accompany them or who convinced them through sustained verbal encouragements. In some instances, it was also noted that the AC would offer individualized clinical support especially aimed at bringing a particularly reluctant participant to agree to take part in a challenging exercise, sometimes even explicitly referring to the psychological rational underlying exposure processes. These observations were corroborated by the verbatim of some participants, who emphasized the importance of the clinical support they received from the AC throughout the program, notably with regards to exposure processes: “I remembered things like when she would tell me to find my “off button” and to keep on going” (target participant). The non-judgmental climate of the program also seems to have contributed to the success of desensitization processes. All of the respondents interviewed on that aspect reported that they indeed perceived the program environment as relatively judgment-free, some specifying that it allowed them to express themselves freely and to present themselves as they really are without fear of others’ negative judgement: “It was good in the sense that you were not afraid of being yourself and to appear ridiculous” (target participant). Some respondents nonetheless mentioned that the imperatives of the public performance preparation, especially the professional-like artistic direction, induced a certain amount of pressure and stress in the workshops, which may have sometimes antagonized the secure and non-judgmental program environment intended to promote free experimentation: “I found it was a bit stressful, not at the beginning, but at the end. I found it stressful because we had to hurry to do things right” (group interview).
SUCCESS AND VALORIZATION
A certain number of participants reported they believed that experiencing success at accomplishing different program-related tasks or imperatives, such as interacting with others, achieving difficult exercises, or attending the program until the end, contributed to some of the benefits they retained from their participation: “There are some things that I didn’t think I would be able to do in such a crowded place. I succeeded anyway, and I know it helped me” (target participant). This was echoed by the AC and at least one referrer, who related the improvements in self-perception observed in some participants to their experience of success during the program: “Yes, I think she acquired better self-esteem. The fact that she could participate in a group; there was dancing or a theatre play in there, and she felt good; she felt she was succeeding and that it was good for her” (referrer). In a related way, a few respondents raised the fact that the program allowed certain participants to realize and valorize some of the talents or abilities that they already possessed, a process that they thought may have underpinned some of the program’s positive effects, especially on self-perception: “In terms of self-esteem, I think it was very positive. He realized that he had talent; that he was recognized for what he was bringing” (referrer). According to some referrers and the AC, the program also allowed participants’ entourage, especially family and clinicians, to witness their capacities and accomplishments, which was also viewed as an important mechanism contributing to program-attributed benefits: “For some, it’s the fact of having completed from the beginning to the end that allowed them to realize that they are able to do something and also to prove to others that they were able to complete; that they were able to function and to produce something” (AC). Although, to a certain extent, the success and valorization processes reported seem to have taken place throughout the program workshops, it appears that an important part occurred in the context of the final public performance. In fact, according to a great number of respondents, the final representation allowed participants to realize all that they had achieved during the course of the program and to derive a sense of pride from that realization: “I was proud and surprised of the result of the show. We really saw all the evolution and all that we did, the group cohesion. Everybody was proud” (group interview). The final performance was also a privileged occasion to show their efforts and accomplishments to meaningful others and to elicit their pride and recognition: “Afterwards, you feel relieved because you know you gave your maximum and your friends and family are proud of you” (target participant). Complimenting interactions between participants and their family, friends, or clinical staff, sometimes marked by highly emotional manifestations of pride and affection, were in fact objectified by the observer following the final performances, along with abundant verbal and physical manifestations of pride on the part of the participants themselves.
NORMALIZATION
A few respondents raised the program’s various normalizing characteristics as potential factors that could have underlain some of its positive effects, especially on self-perception. Among the program aspects considered to be “normalizing” is the fact that it was offered outside of the hospital context. Most participants who were questioned about this characteristic reported that they indeed perceived the program as dissociated from conventional care and service settings, some stating that it gave them the impression to be an activity like any other: “I thought it was an activity like if you had registered in a course. It didn’t give the impression of being with an institute or a hospital” (target participant). A few participants also highlighted that the facilitators did not interact with them as clinicians would have: “I think it’s good. It takes us out of the traditional [therapeutic] box (…). If you talk with [the facilitators], it’s more like if you were talking to someone on the street, normal” (target participant). Most participants seem to have appreciated the non-clinical setting and facilitation of the program, and some especially emphasized their normalizing impact: “It’s good because it allows to show the person that she’s able to do something outside of the psychiatric follow-up, something official conducted by persons that are not necessarily doctors” (target participant).
Another related normalizing aspect of the program that was reported is the fact that little attention was paid to each other’s mental health issues. In fact, although it appears that the intended anonymity with regards to participants’ backgrounds was not perfectly preserved by program facilitators, most participants reported that psychiatric and other personal antecedents took very little place in their interactions with each other and with the facilitators: “It was so not focused on that it seemed, I think it was never a subject during the workshops or even the breaks. I think that X and Y talked about their medications once, but I think that otherwise, it was never a subject. So it was just like being with normal youth. I found that this aspect was really not emphasized” (general population participant). Many reported that it was even hard to distinguish between participants referred by mental health practitioners and those who were not since psychiatric symptomatology was not so apparent and was not put forward during the workshops: “We could not know people who had had problems. It was not a question that we would ask, and it was not a subject that we touched on. We were there, we were at the activity, and we wanted to have fun. I thought that others wanted to have fun as well” (target participant).
For several respondents, the fact that target participants were mixed with participants from the general population represented a crucial normalizing factor as it allowed youths with a history of mental health problems to realize that they are not that different from their peers who do not and that they can be part of the same group and achieve common goals: “I think it’s a good idea because it also allows us to see people who don’t all have problems. It allows us to see that they are not really different from us. We are very much alike. I could not distinguish between those who had problems or didn’t” (target participant). For one referrer, belonging to a group that appeared globally less impaired than those to which some of the participants were used to also carried a normalizing potential: “I think he had the impression to be with a gang of youths and that it was very normalizing for him; to be in a group of teenagers more normal than at the day hospital, which clash less, let’s say” (referrer). Conversely, other referrers mentioned that the program offered some participants the occasion to compare themselves with youths presenting with similar or more severe impairments, which they thought potentially favored normalizing processes for them: “To have a group composed of youths who were all as impaired as him or more, it played in his stopping to be a victim. A very normalizing setting for him, it was very important” (referrer).
According to some respondents, the mix of participants coming from different backgrounds and the relative anonymity preserved with regards to personal antecedents also offered target participants an occasion to be exposed to the gaze of people who were not aware of their mental health condition and who consequently offered them a normalizing reflection of themselves: “The fact of being with people who were not aware of her difficulties and who pushed her much further than people who would have known her earlier. So a new look on her.” (referrer). Concordantly, it was noted on several occasions during field observation that the facilitators acted similarly and maintained the same level of demand with youths whose symptoms were apparent than with those who did not show any signs of impairment. Furthermore, it was both unanimously reported by participants and directly observed that every participant was given an active and fairly equal part to play in the collective production, regardless of their background or level of impairment. Undifferentiated interactions between participants coming from similar and different backgrounds were also abundantly observed.
DISCUSSION
THEORY OF ACTION OF THE PROGRAM ALL ON STAGE
In this study, we thematically analyzed a corpus of data composed of interview verbatim and independent field observations to identify the explanatory mechanisms underlying the previously reported positive effects attributed to the participatory arts program All on Stage on the social comfort and competence, self-perception, and global functioning of adolescents and young adults living with varied mental health issues. Figure 1 offers a visual integration of our findings and reveals the first empirically derived theory of action of the program. This figure includes three program aspects -components, mechanisms, and effects-, and two types of arrows. Full arrows represent influences from one aspect to another, such as a program component promoting the emergence of a mechanism. Broken arrows represent program components that modulate – in this case, increase- the impact of mechanisms on effects.
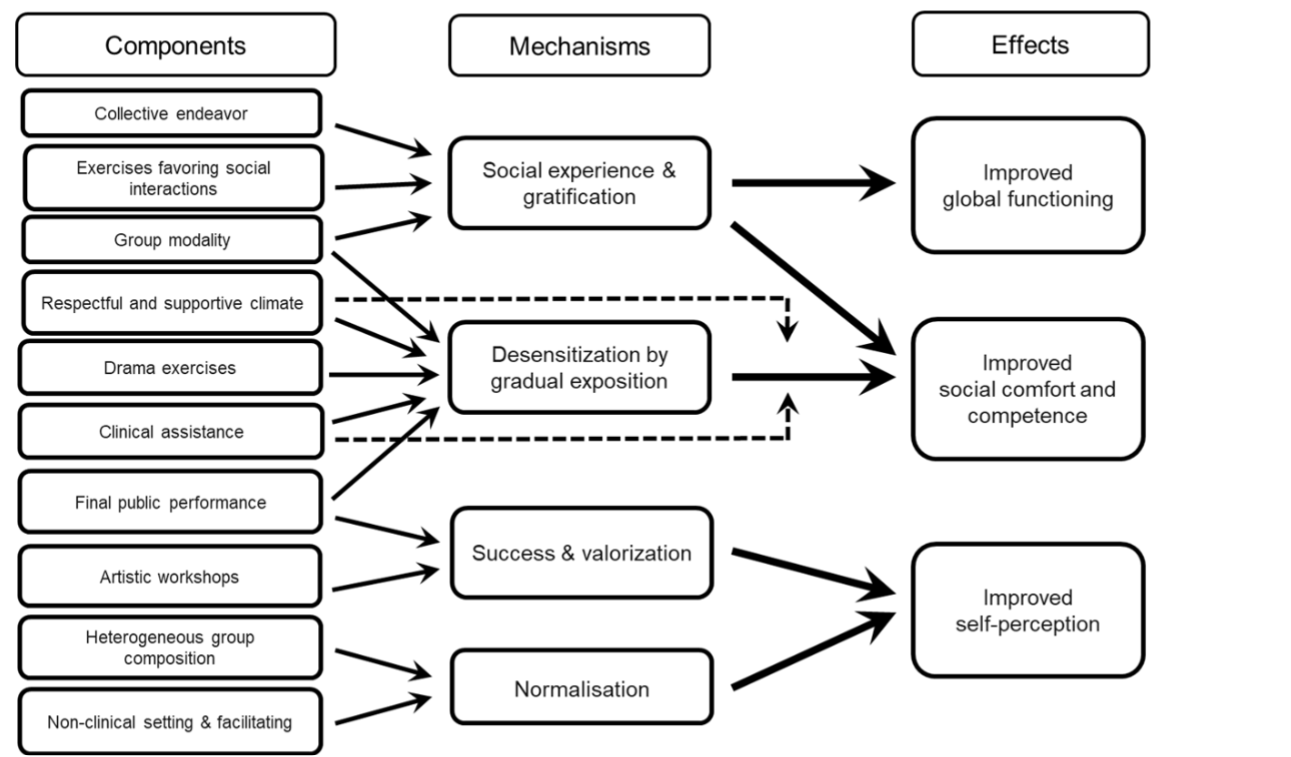
First, we identified social experience and gratification processes as key mechanisms underlying program-related improvements in social comfort and competence and decreases in social isolation, an aspect of improved global functioning. Results indicate that the program allowed participants to acquire social experience, notably by practicing important social behaviors and attitudes and realizing their role and place in relation to others, which led to concrete improvements in the social sphere. The social gratification derived from program participation, such as the experience of mutual support and social inclusion, also appears to have contributed to the documented social improvements. Similar mechanisms have been reported in other evaluations of art-based programs. For instance, group processes of artistic elaboration and the interactions they entail between participants have been found to foster the development of interpersonal skills and the acquisition of better-adjusted social attitudes and behaviors. Quite obviously, we identified the program’s group modality as a necessary condition for the implementation of the social mechanisms described above, which we found to be further fostered by exercises directly promoting social interactions, notably those that involved concrete collaboration, physical contact, or communication. We also found participation in the collective enterprise that the final performance represented to have especially fostered group cohesion. This finding is in line with those from previous studies, in which the sharing of a collective artistic endeavor has been similarly reported to promote group cohesion and participants’ sense of belonging.
The second mechanism that we identified is desensitization by gradual exposure. It was mainly put forward to explain the program’s positive effects on social comfort and competence, especially reductions in shyness and fear of others’ negative judgment and correlate increases in relational ease and openness. We found desensitization processes to have been mainly triggered by the drama exercises through which participants were regularly brought to experiment with performance situations implying increasing levels of self-expression, awkwardness, or embarrassment from other sources while being exposed to the gaze of their peers. Results indicate that this gradual sequence of exposure culminated with the final public performance, in which every participant performed in front of a much larger audience composed of family, friends, and clinicians. Furthermore, regular immersion in a group setting was reported to have led to social habituation in some cases, which represents another form of desensitization by exposure, although not gradual per se. Gradual exposure interventions are among the most efficient strategies to reduce stress and anxiety related to social stimuli. However, whereas it can be hypothesized that such processes are at work in many other participatory arts programs, they have not been extensively discussed in this field.
Interestingly, our results suggest that two program components both directly influenced the taking place of desensitization by gradual exposure mechanisms and modulated their impact on participants’ social comfort and competence. On one hand, we found the respectful and supportive climate prevailing in the workshops as well as the clinical assistance provided by the AC to have promoted participation in the exposure tasks, especially for some more reluctant participants (depicted by full arrows in Figure 1). Establishing an accepting and trusting environment is central to many art-based programs and is considered essential to allow participants to feel secure enough to engage in learning, experimentation, and socialization. Additionally, our results suggest that the secure and respectful climate as well as the AC’s assistance also promoted the success of gradual exposure mechanisms at improving participants’ social comfort and competence (depicted by the broken arrows in Figure 1). The literature on gradual exposure interventions indeed informs that the sense of security and support felt by participants is not only essential in bringing individuals to experiment and to tolerate exposure to stressful conditions but is also a crucial determinant of the positive outcome of exposure procedures. In fact, the operant reconditioning underlying effective desensitization relies on the realization that the anxiety-eliciting situation is not followed by consequences as aversive as anticipated, such as being openly judged by peers or publicly ridiculed. Hence the importance of the spirit of mutual respect and support that seems to have largely prevailed throughout All on Stage’s workshops. Although this climate, along with the clinical support offered by the AC, seem to have globally fostered the taking place and success of exposure mechanisms in the program, it remains that some participants reported having found the drama exercises somewhat confronting at first and to have sometimes felt a difficult pressure related to the preparation of the final performance, factors that may have somewhat impeded these same mechanisms. These indications emphasize the delicate character of exposure procedures and suggest that careful consideration of challenge gradation should be at the center of workshop planning and facilitation.
Success and valorization processes represent the third type of mechanism that we identified. The program was widely reported to allow participants to experience a sense of success and accomplishment as well as to realize and value their abilities and talents, which was mostly associated with program-related improvements in self-perception. This finding is consistent with dominant psychological theories stipulating that self-perceived competence is among the main determinants of self-esteem. It is also in line with results from previous studies on art-based interventions for people with mental health needs, in which opportunities to experience success have been associated with the development of a more positive personal identity. We found success and valorization mechanisms to have taken place throughout the program’s artistic workshops. Yet, our results suggest that the final performance played a catalytic role in their occurrence, both by potently favoring participants’ realization of their individual and collective achievements and by allowing other people to witness their accomplishments and provide them with concordant positive feedback. According to previous studies on arts in health interventions, the feelings of accomplishment, pride, and personal value associated with the practice of an art and the production of art works can indeed be greatly reinforced by public performance or exhibition.
The last mechanism that we identified is normalization, which is believed to have mostly influenced participants’ self-perception. Results suggest that, by giving them the opportunity to function in an environment in which mental health issues were not emphasized, the program allowed certain participants to transform their self-image into a less marginalized one. The fact that the program was offered in a non-clinical setting and facilitated by non-therapist artists appears to have promoted the taking place of the reported normalization processes. According to previous studies, the «non-medicalized» character of many arts in health programs allows participants to relate to one another and to express and understand themselves outside of clinical frameworks, which has been associated with improvements in their self-perception. More generally, such programs’ common focus on strengths, interests, and abilities rather than on problems and limitations is believed to be key in giving participants the opportunity to build a more positive and less marginalized vision of themselves, a milestone of personal recovery. The heterogeneous composition of the groups, which mixed participants referred by mental health practitioners with peers from the general population, and the voluntary disclosure with regards to each other’s mental health history also seem to have been perceived as normalizing by respondents. They mostly shared that it allowed target participants to see themselves function positively alongside typically developing youths and to be exposed to the fresh gaze of people who ignored their mental health condition and who held high participation and performance expectations towards them. Other authors have highlighted the importance of allowing participants to engage with each other and with facilitators without the «mental health nametag», arguing that the dissociation of people from their problems helps render their aptitudes, interests, competencies, and engagement more easily accessible, to the benefit of their recovery. Yet, to our knowledge, very few arts-in-health programs mix participants with mental health needs with voluntary peers from the general population, and even fewer encourage undifferentiated roles and symmetrical interactions.
STRENGTHS AND LIMITATIONS
One of the main strengths of the present study is its reliance on naturalistic methods of data collection, which allowed for investigating the mechanisms at work in the program in its real-world context of implementation, without altering its course. The convergence of multiple perspectives and of two methods of data collection, including independent observation, which is regarded as one of the most efficient means to assess a program’s implementation and processes, favored the exhaustiveness of the investigation and strengthened the validity of its conclusions. Moreover, this investigation offered participants and program contributors an opportunity to voice their subjective experience of the program and their impressions of what brought about its attributed changes. We valued their accounts and opinions as a privileged starting point for the exploration of the program’s mechanisms of action, which aligns with the largely recognized need to incorporate the views of the main stakeholder groups in health research and in research on young people.
The present study also holds some limitations. First, the proposed theory of action is limited to the relationships that were empirically found in the present investigation and thus may not be fully exhaustive. Respondents may not have reported on all active implicit program processes, either because they were not conscious of all of them or because they held biases towards the way the program works, and the non-systematic nature of the observation method we used did not allow for the precise and exhaustive documentation of program implementation and mechanisms at work. Moreover, we did not include the views of participants who did not complete the program, who may have contributed divergent perspectives about its mechanisms of action. Besides, although not a limitation per se, it must be acknowledged that the theory of action presented in this article was certainly colored by the analyst’s personal views and biases based on the intimate knowledge of the program she developed through her field observations and close collaboration with the promotor team and on her academic and clinical background in psychoeducation and youth mental health. Analysts with other experiences and theoretical references may have come up with a somewhat different model, though we believe that the credibility of the theory we presented is reinforced by the strong empirical approach we privileged and the frequent consulting with co-authors from diverse backgrounds and stances.
CONCLUSION
In conclusion, this study offers a rare example of inductive theory building in the context of a real-world arts-in-health program evaluation. The model we derived from our qualitative investigation may serve as a hypothetical basis for further research on the mechanisms of action of participatory arts programs and guide the planning and delivery of future initiatives in the fields of arts in health and youth mental health rehabilitation.
ACKNOWLEDGEMENTS
We wish to warmly thank all research participants and program collaborators for their precious implication, as well as late Professor Frédéric N. Brière for his valuable input.
ETHICS APPROVAL
Our study was approved by the Ethics Review Board of Sainte-Justine University Hospital Center (initial approval on October 25th, 2011; ref # 10.125), and of all the recruitment sites. All participants provided written informed consent prior to enrollment in the study.
FUNDING
This research was supported by private and corporate donations administered through the CHU Sainte-Justine Foundation and by doctoral grants from the University of Montreal. The content of this manuscript is the sole responsibility of the authors and was not influenced by the views of the funders.
CONFLICTS OF INTEREST
Authors have no pecuniary conflicts of interest to declare. P. Garel is the founder and general director of the Transition Space project, in which the program All on Stage is nested. K. Archambault is now the project’s scientific director, but she was independent from it when the study was conducted and the manuscript was written. All authors had full access to the data and are responsible for its integrity and accuracy of analysis.
AUTHORS’ CONTRIBUTION
K. Archambault is responsible for the study conception and design, as well as data analysis. She was closely supported and advised by S. Dufour and I. Archambault throughout the entire research process, especially with regards to data analysis. N. Beauregard contributed valuable ideas and helped with the literature review and manuscript preparation. P. Garel contributed to the program description and to the clinical interpretation of study results. The first draft of the manuscript was written by K. Archambault and all authors commented on previous versions. All authors read and approved the final manuscript.
REFERENCES
- Fancourt D, Finn S. What is the evidence on the role of the arts in improving health and well-being? A scoping review. Nord J Arts Cult Health. 2019;2(1):77-83. doi:10.18261/issn.2535-7913-2020-01-08
- Gordon-Nesbitt R. Creative Health: The Arts for Health and Wellbeing. All-Party Parliamentary Group on Arts, Health and Wellbeing; 2017. http://www.artshealthandwellbeing.org.uk/appg-inquiry/Publications/Creative_Health_Inquiry_Report_2017_-_Second_Edition.pdf
- Fancourt D, Aughterson H, Finn S, Walker E, Steptoe A. How leisure activities affect health: A narrative review and multi-level theoretical framework of mechanisms of action. Lancet Psychiatry. 2021;8(4):329–339. doi:10.1016/S2215-0366(20)30384-9
- Kelly S, Davies L, Harrop D, McClimens A, Peplow D, Pollard N. Reviewing art therapy research: A constructive critique; 2015.
- Patton MQ. Qualitative Research & Evaluation Methods. 4th ed. Thousand Oaks, CA: Sage Publications; 2014.
- Rogers P, Petrosino A, Huebner TA, Hacsi TA. Program theory evaluation: Practice, promise, and problems. New Dir Eval. 2000;87:5-14. doi:10.1002/ev.1177
- Rossi PH, Lipsey MW, Freeman HE. Evaluation: A Systematic Approach. 7th ed. Thousand Oaks, CA: Sage Publications; 2003.
- Warran K, Burton A, Fancourt D. What are the active ingredients of ‘arts in health’ activities? Development of the INgredients iN ArTs in hEalth (INNATE) framework. Wellcome Open Res. 2022;7:10. doi:10.12688/wellcomeopenres.17414.2
- Van Lith T, Schofield MJ, Fenner P. Identifying the evidence-base for art-based practices and their potential benefit for health recovery: A critical review. Disabil Rehabil. 2013;33(16):1309-1323. doi:10.3109/09638288.2012.732188
- Archambault K. Évaluation d’un programme novateur de réadaptation par les arts de la scène pour les jeunes présentant un trouble psychiatrique stabilisé : le programme Espace de Transition. [Doctoral dissertation, Université de Montréal]; 2014.
- Archambault K, Archambault I, Dufour S, Brière FN, Garel P. A mixed methods evaluation of the effects of an innovative art-based rehabilitation program for youths with stabilized psychiatric disorders. Ado Psych. 2015;5(3): 212-224. doi:0.2174/221067660503151204113049
- Lipsey MW, Cordray DS. Evaluation methods for social intervention. Annu Rev Psychol. 2000;51:345-375. doi:10.1146/annurev.psych.51.1.345
- Denzin NK, Lincoln YS. Handbook of Qualitative Research. 5th ed. Sage Publications; 2017.
- Miles MB, Huberman M, Saldaña J. Qualitative Data Analysis: A Methods Sourcebook. 4th ed. Thousand Oaks, CA: Sage Publications; 2020.
- Provalis Research. QDA Miner, Version 3.2 [computer program]. Montréal (QC): Provalis Research; 2009.
- Macpherson H, Hart A, Heaver B. Building resilience through group visual arts activities: Findings from a scoping study with young people who experience mental health complexities and/or learning difficulties. J Soc Work. 2016;16(5):541-560. doi:10.1177/1468017315581772
- Perez RM, Archambault K, Dupéré V. Déploiement et contribution des relations sociales au sein d’un programme parascolaire artistique conçu pour des jeunes vivant avec des difficultés socio-émotionnelles. Rev Psychoéduc. 2023;52(2):519-549. doi:10.7202/1107456ar
- Zarobe L, Bungay H. The role of arts activities in developing resilience and mental wellbeing in children and young people: A rapid review of the literature. Perspect Public Health. 2017;137(6):337-347. doi:10.1177/1757913917712283
- Logan ML. ‘There was something magical about this group’: Building cohesion in a psychiatric hospital [master’s thesis]. Cambridge, MA: Lesley University; 2019.
- Torrissen W, Stickley T. Participatory theatre and mental health recovery: A narrative inquiry. Perspect Public Health. 2018;138(1):47-54. doi:10.1177/1757913917723944
- Otto MW, Safren SA, Hearon BA. Mechanisms of action in the treatment of social anxiety disorder. In: Hofmann SG, DiBartolo PM, eds. Social Anxiety: Clinical, Developmental, and Social Perspectives. 3rd ed. Elsevier Academic Press; 2014:777-800. doi:10.1016/B978-0-12-394427-6.00027-3
- Stickley T, Wright N, Slade M. The art of recovery: Outcomes from participatory arts activities for people using mental health services. J Ment Health. 2018;27(4):367-373. doi:10.1080/09638237.2018.1437609
- Harter S. The Construction of the Self: Developmental and Sociocultural Foundations. 2nd ed. Guilford Press; 2012.
- Heenan D. Art as therapy: An effective way of promoting positive mental health? Disabil Soc. 2006;21(2):179-191. doi:10.1080/09687590500498143
- Lawson J, Reynolds F, Bryant W, Wilson L. ‘It’s like having a day of freedom, a day off from being ill’: Exploring the experiences of people living with mental health problems who attend a community-based arts project, using interpretative phenomenological analysis. J Health Psychol. 2014;19(6):765-777. doi:10.1177/1359105313479627
- Stickley T, Hui A. Social prescribing through arts on prescription in a UK city: Participants’ perspectives (Part 1). Public Health. 2012;126(7):574-579. doi:10.1016/j.puhe.2012.04.002
- Fenner P, Ryan B, Latai L, Percival S. Art making and the promotion of wellbeing in Samoa: Participants’ lived experience of a recovery-oriented intervention. Arts Health. 2018;10(2):124-137. doi:10.1080/17533015.2017.1334677
- Gallant K, Hamilton-Hinch B, White C, Litwiller F, Lauckner H. “Removing the thorns”: The role of the arts in recovery for people with mental health challenges. Arts Health. 2019;11(1):1-14. doi:10.1080/17533015.2017.1413397
- Thomas Y, Gray M, McGinty S, Ebringer S. Homeless adults engagement in art: First steps towards identity, recovery and social inclusion. Aust Occup Ther J. 2011;58(6):429-436. doi:10.1111/j.1440-1630.2011.00977.x
- Van Lith T, Fenner P, Schofield MJ. The lived experience of art making as a companion to the mental health recovery process. Disabil Rehabil. 2011;33(8):652-660. doi:10.3109/09638288.2010.505998
- Wimpenny K, Savin-Baden M. Using theatre and performance for promoting health and wellbeing amongst the 50+ community: An arts-informed evaluation. Int J Soc Polit Community Agendas Arts. 2014;8(1):47-64.
- Argyle E, Bolton G. Art in the community for potentially vulnerable mental health groups. Health Educ. 2005;105(5):340-354. doi:10.1108/09654280510617178
- Goodman-Casanova JM, Guzman-Parra J, Mayoral-Cleries F, Cuesta-Lozano D. Community-based art groups in mental health recovery: A systematic review and narrative synthesis. J Psychiatr Ment Health Nurs. 2023;31(2):158-173. doi:10.1111/jpm.12970
- Nitzan A, Orkibi H. The contribution of integrated arts-based groups to people with mental health conditions and community members: Processes and outcomes. Psychol Aesthet Creat Arts. Published online 2022. doi:10.1037/aca0000501
- Coholic D, Schinke R, Oghene O, Dano K. Arts-based interventions for youth with mental health challenges. J Soc Work. 2020a;20(3):269-286. doi:10.1177/1468017319828864
- Coholic D, Schwabe N, Lander K. A Scoping Review of Arts-Based Mindfulness Interventions for Children and Youth. Child Adolesc Soc Work J. 2020b;37(5):511-526. doi:10.1007/s10560-020-00657-5
- Leamy M, Bird V, Le Boutillier C, Williams J, Slade M. Conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. Br J Psychiatry. 2011;199(6):445-452. doi:10.1192/bjp.bp.110.083733
- Sweeney S. Art therapy: Promoting wellbeing in rural and remote communities. Australas Psychiatry. 2009;17 Suppl 1:S151-S154. doi:10.1080/10398560902948498
- Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry. 2010;10:113. doi:10.1186/1471-244X-10-113
- Lamb J. Creating change: Using the arts to help stop the stigma of mental illness and foster social integration. J Holist Nurs. 2009;27(1):57-65. doi:10.1177/0898010108323011
- Salaheddin K, Mason B. Identifying barriers to mental health help-seeking among young adults in the UK: A cross-sectional survey. Br J Gen Pract. 2016;66(651):e686-e692. doi:10.3399/bjgp16X687313
- Whittemore R, Chase SK, Mandle CL. Validity in qualitative research. Qual Health Res. 2001;11(4):522-537. doi:10.1177/104973201129119299
- Bowling A, Ebrahim S. Handbook of Health Research Methods: Investigation, Measurement and Analysis. Open University Press; 2005.
- Khoury E. Narrative matters: Mental health recovery – considerations when working with youth. Child Adolesc Ment Health. 2020;25(4):273-276. doi:10.1111/camh.12419