





Thromboembolic Events in Emergency Care During COVID-19
Evaluation of patients diagnosed with thromboembolism in the emergency department before and during the Covid-19 pandemic
Introduction
A new coronavirus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread rapidly in late 2019 and caused a worldwide pandemic. This new respiratory infectious disease was first diagnosed in Wuhan, Hubei Province, China, in December 2019¹. This disease spread from Asia to Europe and America in a short time period and was declared as a “Pandemic” by the World Health Organization (WHO) on March 11, 2020². In Turkey, the first case was announced by the Ministry of Health of the Republic of Turkey on March 10, 2020³.
It is believed that there is a high risk of thrombosis in both the arterial and venous systems associated with COVID-19 infection. It has been reported that especially patients who are followed up in intensive care units have a higher risk of thrombotic complications and death⁴. It has also been stated that COVID-19 infection has an impact on the development of pulmonary embolism (PE) and deep vein thrombosis (DVT)⁴˒⁵.
Atherosclerosis and ischemic stroke are known as diseases that were caused by multiple pathophysiological factors, including cardiac and vascular pathologies. It is thought that COVID-19 infection also affects this pathophysiological condition and increases the tendency to thrombosis⁶. In a study, it was stated that COVID-19 infection increases the risk of myocardial ischemia and ischemic stroke⁷. Although it is more common in ischemic stroke, it has been observed that it affects especially elderly individuals and individuals with serious infections and comorbid diseases (hypertension (HT), diabetes mellitus (DM) and coronary artery disease (CAD))⁸.
The mechanism of thromboembolism, ischemia and stroke development in individuals with COVID-19 infection is not yet fully understood. Hypercoagulability developing due to systemic inflammatory response, cytokine storm, and endothelial inflammation secondary to coronavirus infection seems to be responsible in the etiology⁹˒¹⁰. In a prospective cohort study¹¹, it was found that 1.1% of patients with positive COVID-19 infection experienced a thromboembolic event within one year.
Due to the pandemic, people are hesitant to go to the hospital and they move much less compared to normal life, which has caused new health problems to emerge. While one of the risk factors for thromboembolism is a sedentary lifestyle, it is thought that people not leaving their homes during the Covid-19 pandemic may cause an increase in such pathologies. Another risk factor is the covid 19 infection itself. It is also known that people who have had the infection are more prone to thromboembolic events than other people.
This study aimed to examine the demographic characteristics of patients who admitted to the emergency department due to thromboembolic events before and during the COVID-19 pandemic in our country, and to investigate the effect of the pandemic on thromboembolic events. As a result, it was aimed to determine the effects of the COVID-19 pandemic on thromboembolic events and hospital admissions.
Methods
This study was conducted among patients with thromboembolic events who admitted to the second level adult emergency department, between July 01, 2019- December 31, 2019 (when the COVID-19 pandemic had not yet started), and July 01, 2020- December 31, 2020, (when the COVID-19 pandemic was at its most severe). Ethics committee approval was received for the study from Nevşehir Hacı Bektaş Veli University Rectorate Scientific Clinical Research Ethics Committee (decision number 2021.09.320 on 25/08/2021).
Patients with a thromboembolic event detected between July 01, 2019- December 31, 2019 were classified as Group I, and patients with a thromboembolic event detected between July 01, 2020- December 31, 2020 were classified as Group II. Therefore, patients who were admitted to the emergency department with a thromboembolic event before the COVID-19 pandemic were
included in Group I, while patients who had a thromboembolic event during the COVID-19 pandemic were included in Group II. Percutaneous transcoronary angiography was used for the diagnosis of acute coronary syndrome, while computed tomography and magnetic resonance imaging were used for the diagnosis of ischemic stroke, color Doppler ultrasonography for the diagnosis of deep vein thrombosis, and color Doppler ultrasonography as well as computed tomography angiography were used for the diagnosis of acute arterial occlusion.
A total of 1748 patients diagnosed with thromboembolic events were identified within the specified date ranges of 2019 and 2020. However, 889 patients who had a history of previous thromboembolic events, were pregnant, had underlying diseases that increase the risk of thromboembolism, such as cancer, etc., were excluded from the study. A total of 859 patients over the age of 18, who had no previous comorbidities, not pregnant, and were hospitalized and treated due to thromboembolic events were included in the study. 447 of these patients were in group I and 412 were in group II. Only 20 (4.9%) of the patients in Group II had a history of previous or current Covid 19 infection. Since the largest number of patients in both groups were those presenting with acute coronary syndrome, these patients were also classified separately for each group. Patients presenting with ischemic stroke, pulmonary thromboembolism, deep vein thrombosis and acute arterial occlusion were also evaluated separately in both groups. In order to investigate the seasonal effect on thromboembolic events, subgroups were also evaluated in terms of admission month. Patients hospitalized with a diagnosis of myocardial infarction (MI) were divided into groups as non-ST segment elevation (NSTEMI) and acute ST segment elevation (STEMI) (inferior, anterior, lateral and posterior wall MI) according to electrocardiogram (ECG) and percutaneous transcoronary intervention (PCI) results. All patients diagnosed with acute coronary syndrome underwent percutaneous transcoronary angiography. All patients in Group I had positive COVID-19 polymerase chain reaction (PCR) tests. The time period between the COVID-19 diagnosis date and the thromboembolic event date of these patients was determined and recorded in the study form.
Data collection and statistical analysis
Data scanned retrospectively using hospital information management system records were recorded in the previously created study form. Statistical Package for Social Sciences for Windows 21.0 (SPSS 21.0 IBM Corp., Armonk, NY, USA) program was used in the statistical analysis of the data obtained. Chi-square test were used to compare categorical variables and descriptive statistics (frequency, percentage distribution) between two groups. T test analysis was performed to compare two independent groups. Results are presented as mean ± SD or frequency (percentage), and p<0.05 at the 95 percent confidence interval was considered statistically significant.
Results
A total of 859 patients, 447 from Group I and 412 from Group II, were evaluated in the study. 577 (67.2%) of the patients were male, and the average age of all patients was 67.82±13.14 years. In cases with STEMI, inferior MI (42.7%) and anterior MI (13.9%) were most frequently diagnosed according to ECG findings. Demographic characteristics and diagnoses of the patients according to groups are shown in Table 1. When the patients in Group I and Group II were compared among themselves in terms of gender, thromboembolic events were significantly higher in male patients in both groups (Group I; p<0.05, Chi square: 25.632, Group II; p<0.05, Chi square: 31.999). In the comparative analysis made according to age ranges, it was determined that the diseases were significantly more common in the 61-80 age group in Group I (p<0.05, Chi Square: 53.863) and Group II (p<0.05, Chi Square: 54.479) (Table 2).
Table 1. Demographic data
| Year | Group I | Group II | p** | |
|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | ||
| Age | 67,82±13,14 | 67,87±13,70 | 67,76±12,52 | 0,904 |
| Gender | n / (%) | n / (%) | n / (%) | |
| Male | 577 (67,2) | 290 (64,9) | 287 (69,7) | 0,136 |
| Female | 282 (32,8) | 157 (35,1) | 125 (30,3) | |
| Diagnosis* | ||||
| NSTEMI | 367 (42,7) | 207 (46,3) | 160 (38,8) | |
| Inferior MI | 119 (13,9) | 58 (13) | 61 (14,8) | |
| Anterior MI | 106 (12,3) | 51 (11,4) | 55 (13,3) | |
| Lateral MI | 13 (1,5) | 6 (1,3) | 7 (1,7) | |
| Posterior MI | 12 (1,4) | 7 (1,6) | 5 (1,2) | |
| Pulmonary Thromboembolism | 10 (1,2) | 6 (1,3) | 4 (1) | 0,097 |
| Ischemic stroke | 226 (26,3) | 109 (24,4) | 117 (28,4) | |
| Deep Vein Thrombosis | 3 (0,3) | 3 (0,7) | 0 (0) | |
| Peripheral Artery Embolism | 3 (0,3) | 0 (0) | 3 (0,7) | |
| Total | 859 (100) | 447 (100) | 412 (100) | 0,536 |
*MI: Myocardial infarction, NSTEMI: Non-ST elevation myocardial infarction
** T test was used to compare independent variables and p<0.05 was considered significant.
Table 2. Comparative analysis of demographic data
| Data* | Group I Gender Male n (%) | Group I Gender Female n (%) | Group I Statistical Analysis** | Group I Age 21-40 n (%) | Group I Age 41-60 n (%) | Group I Age 61-80 n (%) | Group I Age 81-100 n (%) | Group I Statistical Analysis** | Group II Gender Male n (%) | Group II Gender Female n (%) | Group II Statistical Analysis** | Group II Age 21-40 n (%) | Group II Age 41-60 n (%) | Group II Age 61-80 n (%) | Group II Age 81-100 n (%) | Group II Statistical Analysis** |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NSTEMI | 132 (63,8) | 75 (36,2) | p<0.05 Chi square:25.632 | 6 (2,9) | 64 (30,9) | 99 (47,8) | 38 (18,4) | p<0.05 Chi Square:53.863 | 120 (75) | 40 (25) | p<0.05 Chi square:31.999 | 2 (1,2) | 51 (31,9) | 87 (54,5) | 20 (12,5) | p<0.05 Chi Square:54.479 |
| Inferior MI | 49 (84,5) | 9 (15,5) | 2 (3,4) | 19 (32,8) | 30 (51,7) | 7 (12,8) | 47 (77) | 14 (33) | 1 (1,7) | 19 (31,1) | 36 (59) | 5 (8,2) | ||||
| Anterior MI | 39 (76,5) | 12 (23,5) | 1 (2) | 17 (33,3) | 30 (58,8) | 3 (5,9) | 45 (81,8) | 10 (18,2) | 0 (0) | 26 (47,2) | 21 (38,1) | 8 (14,7) | ||||
| Lateral MI | 4 (66,7) | 2 (33,3) | 0 (0) | 1 (16,7) | 5 (83,3) | 0 (0) | 6 (15,7) | 1 (14,3) | 0 (0) | 3 (42,8) | 4 (57,2) | 0 (0) | ||||
| Posterior MI | 3 (42,9) | 4 (57,1) | 0 (0) | 2 (18,6) | 4 (57,1) | 1 (14,3) | 5 (100) | 0 (0) | 0 (0) | 4 (80) | 1 (20) | 0 (0) | ||||
| PTE | 1 (16,7) | 5 (83,3) | 1 (16,7) | 1 (16,7) | 3 (50) | 1 (16,7) | 1 (25) | 3 (75) | 0 (0) | 0 (0) | 4 (100) | 0 (0) | ||||
| Ischemic stroke | 61 (56) | 48 (44) | 2 (1,8) | 19 (17,4) | 45 (41,3) | 43 (39,4) | 61 (52,1) | 56 (47,9) | 2 (1,7) | 13 (11,1) | 68 (58,1) | 34 (29,1) | ||||
| DVT | 1 (33,3) | 2 (66,7) | 1 (33,3) | 0 (0) | 1 (33,3) | 1 (33,3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||||
| PAE | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (66,7) | 1 (33,3) | 0 (0) | 0 (0) | 3 (100) | 0 (0) | ||||
| TOPLAM | 290 (64,9) | 157 (35,1) | 13 (2,9) | 123 (27,5) | 217 (48,5) | 94 (21,1) | 287 (69,7) | 125 (30,3) | 5 (1,2) | 116 (28,2) | 224 (54,4) | 67 (16,2) |
*NSTEMI: Non-ST elevation myocardial infarction, MI: Myocardial Infarction, PTE: Pulmonary Thromboembolism, DVT: Deep Vein Thrombosis, PAE: Peripheral Artery Embolism
** Pearson chi-square test was used to compare the data. p<0.05 was considered significant within the 95% confidence interval.
It was observed that there was no significant difference in the comparison of the number of cases of thromboembolic events seen in Group I and Group II (p = 0.536). When looking at the distribution of diseases by month, a significant difference was detected in 2019 (mostly in October)(p=0.006 Chi Square: 59.844), while there was no significant difference in Group II (p=0.503, Chi square: 34.263). Figure 1 and 2 show case distributions in terms of months in both years.
It was observed that there was no significant difference in the comparison of the number of cases of thromboembolic events seen in Group I and Group II (p = 0.536). When looking at the distribution of diseases by month, a significant difference was detected in 2019 (mostly in October)(p=0.006 Chi Square: 59.844), while there was no significant difference in Group II (p=0.503, Chi square: 34.263). Figure 1 and 2 show case distributions in terms of months in both years.
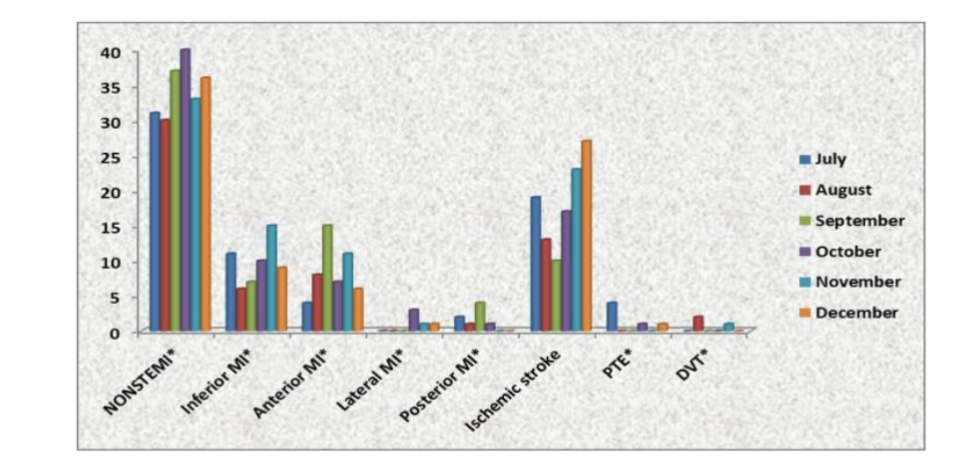
Figure 1. Distribution of patients admitted in 2019 by months
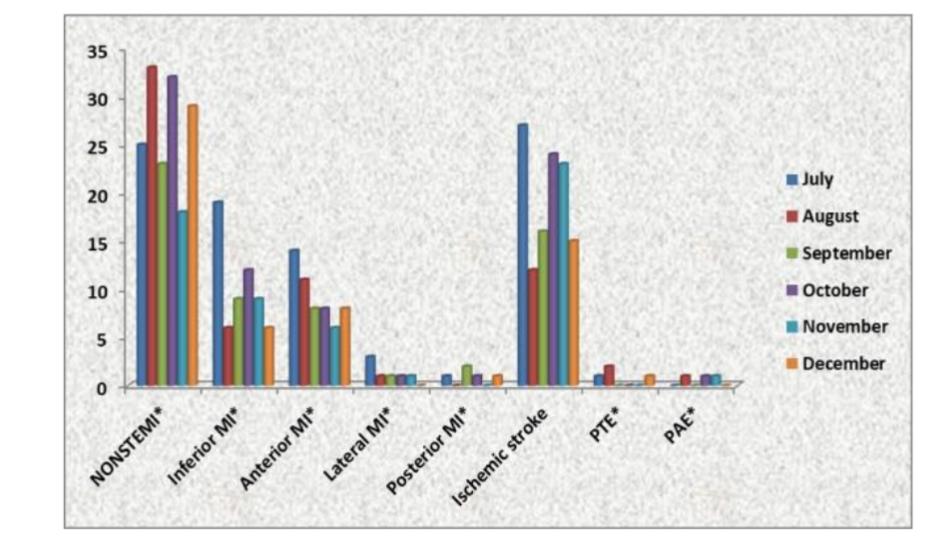
Figure 2. Distribution of patients admitted in 2020 by months
Only 20 (4.8%) of the patients in Group II had a history of COVID-19 disease before thromboembolic event. It was determined that NSTEMI (35%) was the most common in these patients. The average age of the patients was 71.2±9.26, and 70% were male. The average duration of thromboembolic event after COVID-19 infection was found to be 27±26.94 (1-90) days. The most cases were seen in December (40%) (Table 3).
Table 3. Analysis of Patients with Thromboembolic event Following COVID-19 Infection
| Number | Thromboembolic event | Age | Gender | Time period (Day)* | Month of admission |
|---|---|---|---|---|---|
| 1 | Ischemic stroke | 91 | Male | 90 | July |
| 2 | Inferior MI | 76 | Male | 14 | September |
| 3 | Anterior MI | 71 | Male | 21 | September |
| 4 | Anterior MI | 76 | Female | 36 | October |
| 5 | Inferior MI | 61 | Male | 7 | October |
| 6 | Anterior MI | 55 | Male | 18 | October |
| 7 | Inferior MI | 81 | Male | 23 | October |
| 8 | Ischemic stroke | 77 | Male | 12 | November |
| 9 | Ischemic stroke | 70 | Male | 44 | November |
| 10 | NSTEMI** | 74 | Male | 15 | November |
| 11 | NSTEMI** | 63 | Female | 63 | November |
| 12 | Anterior MI | 69 | Male | 79 | November |
| 13 | Ischemic stroke | 70 | Female | 1 | December |
| 14 | NSTEMI** | 78 | Male | 4 | December |
| 15 | NSTEMI** | 57 | Male | 62 | December |
| 16 | NSTEMI** | 73 | Male | 16 | December |
| 17 | Anterior MI | 81 | Female | 1 | December |
| 18 | NSTEMI** | 70 | Female | 3 | December |
| 19 | Ischemic stroke | 71 | Male | 28 | December |
| 20 | NSTEMI* | 70 | Male | 3 | December |
*Time period between diagnosis of COVID-19 Infection and development of thromboembolic event
** Non-ST elevation myocardial infarction
Discussion
Thrombosis that develops due to COVID-19 disease can affect more than one system in the body and cause thromboembolic events, whether of arterial or venous origin¹². Some studies conducted in Western countries have reported a decrease in hospitalizations due to acute cardiovascular diseases such as AMI and stroke during the COVID-19 pandemic¹³˒¹⁴. In this study, we analyzed thromboembolic events before COVID-19 disease was seen in our country and after the disease appeared. However, we found that there was no significant difference in terms of thromboembolic events between the data of 2019 and 2020 (p = 0.536). While previous studies⁶˒⁸ have reported that the COVID-19 pandemic increases the susceptibility to thromboembolic events, the fact that no significant difference was found in our study suggests the need for a re-evaluation on this issue.
In a retrospective study conducted at Nihon Hospital in Japan¹⁵, patients diagnosed with AMI in the same time period in 2017, 2019 and 2020 were analyzed and it was reported that there was a 5.7% decrease in the number of patients during the pandemic period. Within the same study, it was observed that there was an increase in the number of STEMI and a decrease in the number of NSTEMI during the pandemic period compared to previous years¹⁵. In a similar study conducted in Korea, a 13.5% decrease was observed in the number of patients hospitalized with AMI during the pandemic period compared to the pre-pandemic period, and it was reported that the reason for this decrease was the 18.8% decrease in patients with NSTEMI¹⁶. In our study, the NSTEMI patient rate was 46.3% in 2019 and 38.8% in 2020. While the rate of patients with STEMI was 27.3% before the pandemic, this rate increased to 31% in the same period of 2020 during the pandemic. We think that this situation may be related to the hesitation to admit to the hospital due to the pandemic. It is not yet clear whether a direct thrombosis effect of COVID-19 infection is effective in the development of acute MI¹⁷. In a study, it was reported that complaints such as atypical chest pain and shortness of breath, which were among the symptoms of AMI in patients during the pandemic, were considered as symptoms of COVID-19 and the preference for recovery at home caused many patients with AMI to be diagnosed late¹⁸. This situation can be considered as the reason why NSTEMI cases are more common during the pandemic period. In our study, unlike the literature, the higher frequency of inferior myocardial infarctions among STEMI myocardial infections is another significant result. We believe that more comprehensive studies investigating the effects of Covid-19 infection on cardiac vessels may help explain this situation.
The second most common thromboembolic event in our study was ischemic stroke. When Group II data was examined, it was seen that 5(0.4%) of 117 patients diagnosed with ischemic stroke had a history of COVID-19 infection in a period before the disease. In a study conducted during the pandemic, it was reported that the hospitalization rate due to acute ischemic stroke in patients with COVID-19 was estimated to be around 5%¹⁹. In other studies, it has been predicted that the probability of experiencing an ischemic stroke in patients receiving standard thromboprophylaxis may vary between 1.3%-20²⁰˒²². According to a meta-analysis evaluating the analysis results of 26 studies on the subject, the rate of ischemic stroke in those with COVID-19 infection is 1.5% and varies between 0.1% and 6.9% among hospitalized patients⁶. In a multicenter, observational study, it was determined that 0.5% of 26,175 patients hospitalized due to COVID-19 infection had a risk of ischemic stroke, and 79 (0.3%) of these patients were diagnosed with ischemic stroke²³.
In the study conducted by Qureshi et al., 27,676 patients were analyzed and 103 (1.3%) of 8163 COVID-19 positive patients and 199 (1%) of 19513 COVID-19 negative patients were diagnosed with ischemic stroke²⁴. In our study, the rate of ischemic stroke during the pandemic period was 4% higher than the previous year, but there was no significant difference in the number of cases between the two periods (p = 0.429). Therefore, it is not possible to say that there is a clear correlation between Covid 19 infection and the risk of developing ischemic stroke. It was observed that the ischemic stroke cases seen before and during the pandemic were more common in male gender and in the age range of 61-80. In the study conducted by Qureshi et al., it was stated that the majority of cases with ischemic stroke were over the age of 70²⁴. In the same study, it was stated that among patients with ischemic stroke, 55.3% of those who were COVID-19 negative and 44.7% of those who were positive were male²⁴. In our study, 80% of the patients who had ischemic stroke after COVID-19 were male. The fact that this rate is significantly high shows that infection significantly increases the susceptibility to ischemic stroke, especially in the male gender. We think that future large-scale studies on the reasons for this will provide more accurate results. Moreover, some studies in the literature have reported that COVID-19 infection is a predisposing factor for the risk of ischemic stroke⁹˒²⁵˒²⁶.
Porfidia et al. stated that in their systematic review and meta-analysis; they found that the probability of venous thromboembolism (VTE) in patients with COVID-19 was between 6-26%²⁷. In a study conducted with a retrospective analysis of 388 patients in Italy, the VTE rate was found to be 20% despite the routine use of low molecular weight heparin (LMWH) in patients diagnosed with COVID-19 over a two-month period²⁰. According to the results of a single-center study, the PE rate in patients with this infection admitted to intensive care unit was 26.6²⁸. In another study conducted in France, it was observed that 20.6% of patients with COVID-19 who were followed up in intensive care during a one-month period had PE, and a higher rate of PE cases was reported, with an increase of 7.5% compared to the previous year²⁹. In our study, while the rate of cases hospitalized with a diagnosis of PE was 1.3% before the COVID-19 pandemic, only a 1% increase in this rate was detected during the pandemic period. We think that successful
thromboprophylaxis may be effective in this situation. Similarly, while the frequency of DVT was 0.7% before the pandemic, no patient was hospitalized with a diagnosis of DVT during the pandemic.
Studies have found that the incidence of arterial thromboembolism (ATE) is much lower than VTE. It has been reported that the rate of these cases in all embolic events, including acute coronary syndrome, ischemic stroke, mesenteric ischemia and extremity ischemia, varies between 0.7% and 3.7 %²⁰˒²¹˒²⁹. In a single-center study conducted in Madrid, 1419 COVID-19 patients were examined and the incidence of ATE was found to be 1%³⁰. In our study, the frequency of ATE (98.5%) in patients hospitalized due to thromboembolic event was found to be quite high compared to VTE (1.5%). In a study, the incidence of acute extremity ischemia in COVID-19 patients was found to be 16.3% higher than in negative patients in cases seen in January, February and March in 2019 and 2020³¹. We think that this high rate may be due to the fact that COVID-19 infection damages the arterial system much more than the venous system through unknown mechanisms.
Conclusion
From the period after the beginning of the pandemic, we saw that the rate of hospitalization due to thromboembolic event was 4% less than in the same period of the previous year. We think that this may be due to fewer hospital admissions due to the risk of disease transmission during the pandemic period, or the fact that COVID-19 infection does not significantly increase the susceptibility to thrombosis.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
None.
Acknowledgements:
None.
References
1. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;15;395(10223):497-506.
2. WHO (2020). World Health Organization (WHO). Rolling updates on coronavirus disease (COVID-19), https://www.who.int/emergencies/diseases/novelcoronavirus-2019/eventsas-they-happen) . Access date: January 03, 2024.
3. Altınbilek E, Oztürk D, Atasoy C, Ozlem M, Yılmaz F, Kavalcı C. Analysis of the patients who admitted to a Turkish emergency department during covid-19 pandemic. Acta Biomed. 2020; 91(4):e2020201.
4. Mestre-Gómez B, Lorente-Ramos RM, Rogado J, et al. Infanta Leonor Thrombosis Research Group. Incidence of pulmonary embolism in non-critically ill COVID-19 patients. Predicting factors for a challenging diagnosis. J Thromb Thrombolysis. 2021;51(1):40-6.
5. Panigada M, Bottino N, Tagliabue P, et al. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J Thromb Haemost. 2020;18(7):1738-42.
6. Sagris D, Papanikolaou A, Kvernland A, et al. COVID-19 and ischemic stroke. Eur J Neurol. 2021;28(11):3826-36.
7. Katsoularis I, Fonseca-Rodríguez O, Farrington P, Lindmark K, Fors Connolly AM. Risk of acute myocardial infarction and ischaemic stroke following COVID-19 in Sweden: a self-controlled case series and matched cohort study. Lancet. 2021;14;398(10300):599-607.
8. Li Y, Man Li M, Wang M, et al. Acute cerebrovascular disease following COVID-19: a single center, retrospective, observational study. Stroke & Vascular Neurology. 2020;5:e000431.
9. Benussi A, Pilotto A, Premi E, et al. Clinical characteristics and outcomes of inpatients with neurologic disease and COVID-19 in Brescia, Lombardy, Italy. Neurology. 2020;95:910–20.
10. Beyrouti R, Adams ME, Benjamin L, Cohen H, Farmer SF, Goh YY, et al. Characteristics of ischaemic stroke associated with COVID-19. J Neurol Neurosurg Psychiatry. 2020;91:889-91.
11. Rivera-Izquierdo M, Láinez-Ramos-Bossini AJ, de Alba IG, et al. Long COVID 12 months after discharge: persistent symptoms in patients hospitalised due to COVID-19 and patients hospitalised due to other causes-a multicentre cohort study. BMC Med. 2022;23;20(1): 92.
12. Tan BK, Mainbourg S, Friggeri A, et al. Arterial and venous thromboembolism in COVID-19: a study-level meta-analysis. Thorax. 2021;76(10):970-9.
13. Morelli N, Rota E, Terracciano C, et al. The baffling case of ischemic stroke disappearance from the casualty department in the COVID-19 Era. Eur Neurol. 2020;83(2):213-5.
14. Aguiar de Sousa D, Sandset EC, Elkind MSV. The curious case of the missing strokes during the COVID-19 pandemic. Stroke. 2020;51(7):1921-3.
15. Arai R, Fukamachi D, Ebuchi Y, et al. Impact of the COVID-19 outbreak on hospitalizations and outcomes in patients with acute myocardial infarction in a Japanese Single Center. Heart Vessels. 2021;36(10):1474-83.
16. Choi H, Lee JH, Park HK, et al. Impact of the COVID-19 pandemic on patient delay and clinical outcomes for patients with acute myocardial infarction. J Korean Med Sci. 2022;30;e167.
17. Gąsecka A, Borovac JA, Guerreiro RA, et al. Thrombotic complications in patients with covid-19: pathophysiological mechanisms, diagnosis, and treatment. Cardiovasc Drugs Ther. 2021;35 (2):215-29.
18. Mohammad MA, Koul S, Olivecrona GK, et al. Incidence and outcome of myocardial infarction treated with percutaneous coronary intervention during COVID-19 pandemic. Heart. 2020;106(23) :1812-8.
19. Mao L, Jin H, Wang M, et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683-90.
20. Lodigiani C, Iapichino G, Carenzo L, et al; Humanitas COVID-19 Task Force. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res. 2020;191:9–14.
21. Klok FA, Kruip MJHA, van der Meer NJM, et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: an updated analysis. Thromb Res. 2020;191:148–50.
22. Helms J, Tacquard C, Severac F, et al; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020;46:1089–98.
23. Shahjouei S, Naderi S, Li J, et al. Risk of stroke in hospitalized SARS-CoV-2 infected patients: A multinational study. EBioMedicine. 2020;59:102939.
24. Qureshi AI, Baskett WI, Huang W, et al. Acute ischemic stroke and COVID-19: an analysis of 27 676 Patients. Stroke. 2021;52(3):905-12.
25. Qin C, Zhou L, Hu Z, et al. Clinical characteristics and outcomes of COVID-19 patients with a history of stroke in Wuhan, China. Stroke. 2020;51:2219–3.
26. Morassi M, Bagatto D, Cobelli M, et al. Stroke in patients with SARS-CoV-2 infection: case series. J Neurol. 2020;267:2185–92.
27. Porfidia A, Valeriani E, Pola R. Venous thromboembolism in patients with COVID-19: Systematic review and meta-analysis. Thromb Res. 2020;196:67-74.
28. Beun R, Kusadasi N, Sikma M, Westerink J, Huisman A. Thromboembolic events and apparent heparin resistance in patients infected with SARS-CoV-2. Int J Lab Hematol. 2020;42(1):19-20.
29. Poissy J, Goutay J, Caplan M, et al. Lille ICU Haemostasis COVID-19 group. Pulmonary embolism in patients with COVID-19: awareness of an increased prevalence. Circulation. 2020;14:184-6.
30. Cantador E, Núñez A, Sobrino P, et al. Incidence and consequences of systemic arterial thrombotic events in COVID-19 patients. J Thromb Thrombolysis. 2020;50(3):543-7.
31. Bellosta R, Luzzani L, Natalini G, et al. Acute limb ischemia in patients with COVID-19 pneumonia. J Vasc Surg. 2020;72(6):1864-72.