





Thrombolysis in Giant Cell Arteritis-Related CRAO
Successful Intravenous Thrombolysis of Central Retinal Artery Occlusion in a Patient with Giant Cell Arteritis
Anfal K. Shelig, MD ¹, G. Bryan Young, MD, ¹ Norman P. Mainville, MD ², Ivan I. Pacheco Blandino, MD, PhD ³
¹ Emeritus Professor of Neurology, Western University, London, Ontario and attending physician, Brightshores Health System, Owen Sound, Ontario
² Attending ophthalmologist, Brightshores Health System, Owen Sound, Ontario
³ Pathologist, Brightshores Health System, Owen Sound, Ontario
OPEN ACCESS
PUBLISHED 31 August 2025
CITATION Shelig, AK., Young, GB., et al., 2025. Successful Intravenous Thrombolysis of Central Retinal Artery Occlusion in a Patient with Giant Cell Arteritis. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6798
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i8.6798
ISSN: 2375-1924
ABSTRACT
Importance: Central retinal artery occlusion (CRAO) is an ophthalmologic emergency, most often from non-arteritic etiology, but occasionally due to arteritic causes, especially giant cell arteritis (GCA), an inflammatory vasculitis affecting large and medium sized arteries. While thrombolytic therapy with intravenous tissue plasminogen activator (IV tPA) has gathered interest in non-arteritic CRAO, its role in arteritic CRAO remains unexplored. We report a case of successful visual recovery following intravenous thrombolysis in a patient with GCA-associated CRAO, and compare this outcome with current literature.
Observations: A patient presenting with acute monocular vision loss in her left eye was diagnosed with CRAO in the setting of active GCA and received IV tPA within 2.5 hours of symptom onset. Visual acuity, fundus findings, and safety outcomes were documented post-treatment. Following treatment, the patient demonstrated significant visual improvement, regaining functional acuity. This contrasts sharply with the typically poor visual prognosis in arteritic CRAO, despite corticosteroid therapy alone. In non-arteritic CRAO, IV tPA, when administered within 4.5 hours, has been shown to improve vision in 30-60% of cases, with an excellent safety profile and very low incidence of symptomatic intracranial hemorrhage. No previous studies however have reported successful thrombolysis in arteritic CRAO.
Conclusion: This case presents new evidence that early intravenous thrombolysis, in conjunction with corticosteroid therapy, may preserve vision in GCA-related CRAO by targeting a superimposed thrombotic component. While current guidelines do not support thrombolysis for arteritic CRAO, our findings suggest that a dual anti-inflammatory and thrombolytic approach could be effective in select patients. Further research is warranted to characterize patient selection criteria, optimize timing, and assess safety in this unique population.
Keywords: Giant cell arteritis, central retinal artery occlusion, thrombolysis.
Introduction
Central Retinal Artery Occlusion (CRAO) is an ophthalmic emergency, essentially an ischemic stroke of the eye, typically caused by an abrupt interruption of retinal blood flow. The vast majority (~95%) of CRAO cases are non-arteritic, resulting from thromboembolic phenomena in the central retinal artery (most commonly cholesterol or platelet-fibrin emboli from carotid or cardiac sources). Non-arteritic CRAO (NA-CRAO) is characterized by a classic clinical presentation of permanent CRAO, including retinal infarction, cherry-red spot, retinal arteriolar changes, absent or poor residual retinal circulation on fluorescein fundus angiography, and no evidence of giant cell arteritis. In about 5% of cases, CRAO is arteritic, most commonly due to giant cell arteritis (GCA).
GCA/temporal arteritis is a granulomatous large-vessel vasculitis of older adults that can involve the ophthalmic artery and its branches, leading to occlusion via intense inflammation and intimal proliferation. Despite common treatments like hemodilution, ocular massage, and paracentesis, there is currently no evidence-based therapy for CRAO. While ocular massage might increase retinal perfusion pressure, it carries the risk of embolic migration and symptom exacerbation. Intravenous thrombolysis is currently used in CRAO, similar to the stroke thrombolysis protocol. The current window for thrombolysis in stroke is less than 4.5 hours from treatment onset. A small randomized controlled trial in CRAO found that only those who underwent thrombolysis within six hours saw an improvement in three or more lines of visual acuity. In CRAO, intra-arterial delivery of tPA (IA-tPA) is another alternative and offers two potential benefits over IV administration methods: it may have a longer time to treatment window and requires lower doses for therapeutic effect. Intra-arterial thrombolysis delivers the thrombolytic agent via a catheter directly into the ophthalmic artery. Higher local drug concentration and a longer window (some have treated up to 12-24 hours after onset) are theoretical advantages. According to certain nonrandomized trials, patients who received IA-tPA had a 13-36 times higher chance of seeing an improvement in their vision than those who did not receive treatment. However, the only randomized controlled trial did not find a significant difference between IA-tPA and conservative therapy at 1 month, noting a high rate of procedure-related complications. IA-tPA requires interventional neuroradiology expertise and is not available in many hospitals, making it impractical as a general solution. In the case of arteritic CRAO like GCA, IA-tPA would presumably be of little value unless a thrombus is present to lyse, similar to IV tPA. This report presents a clinically relevant case where IV tPA was successfully used to treat CRAO secondary to GCA. Through this case, the report seeks to highlight the role of thrombolysis in the treatment of CRAO, particularly in arteritic cases. It also aims to review the current literature on the treatment of CRAO and explore the implications of this case on future clinical practice and guidelines.
Case
A 63-year-old woman noticed new onset headaches, which were concentrated in the occipital region, for one month before she lost vision in the left eye associated with pain in the eye. Vision was 20/30 in the right eye and light perception only in the left eye, which had a relative afferent pupillary defect (RAPD). Ophthalmoscopy of the left fundus revealed a cherry red spot in the fovea with -carr the retinal arterioles. Ophthalmoscopy of the right eye was normal. CT angiogram from the aortic arch to vertex was unremarkable.
Two and one-half hours after the onset of vision loss a decision was made to start treatment with intravenous tissue plasminogen activator. When examined two hours later the vision in the right eye had returned to 20/30 and the RAPD was no longer present and fundoscopy showed restoration of arteriolar circulation and the cherry red spot was no longer seen. The erythrocyte sedimentation rate was 23 (normal 0-12) mm/hour and C-reactive protein was 32.6 (normal <10) mg/L. The transthoracic echocardiogram and 48-hour Holter monitor (performed later) were normal as were two days of in-hospital cardiac monitoring.
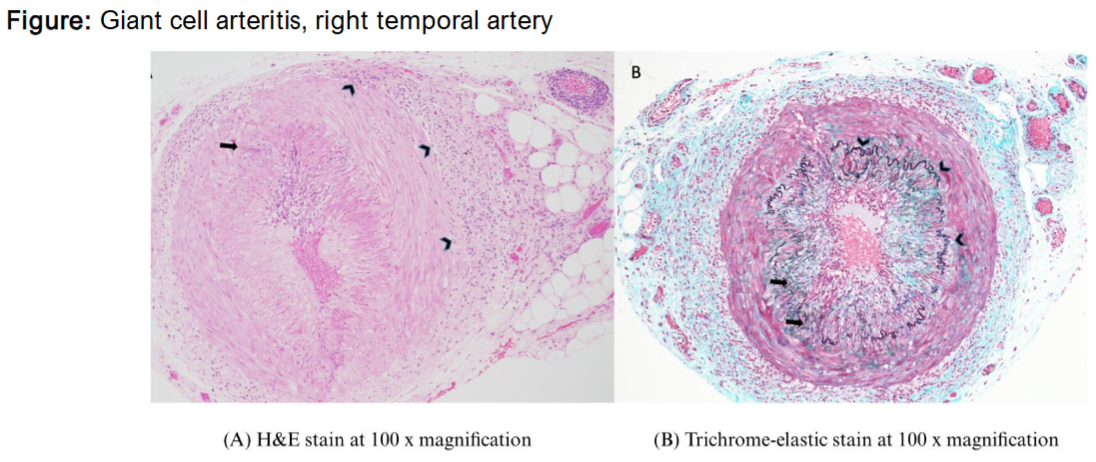
As inflammatory markers were elevated, a decision was made to proceed with bilateral temporal artery biopsies to rule out vasculitis as the cause of the central retinal artery occlusion. The left side was normal, while the right side showed features compatible with giant cell arteritis.
The patient was managed initially with prednisone, switching to tocilizumab; her vision remains normal.
The most common cause of CRAO is thromboembolism. The success in use of tPA in central retinal artery occlusion is variable, and is often unsuccessful, possibly because of the length of thrombus in the long, thin central retinal artery. However, intra-arterial thrombolysis was successful in 2 cases of CRAO treated within 2.75 and 5.5 hours from symptom onset, respectively.
In cranial arteritis, the lumen is progressively narrowed by inflammatory reaction and thickening of the intima. The administration of corticosteroids is recommended as the principal treatment. However, it has been recognized that some patients with threatened visual loss due to cranial arteritis respond to anticoagulants, suggesting a thrombotic or thromboembolic mechanism. In our case the visual loss resolved after thrombolysis, well before the administration of corticosteroid. The central retinal artery is the second most common site of GCA, the main site being the posterior ciliary arteries. We could not find another case of CRAO due to GCA that was successfully treated with thrombolysis but found a case report of thrombosed intraorbital arteries due to GCA that resolved with early thrombolytic treatment.
While we support the primacy of intravenous corticosteroid treatment for GCA, in cases of CRAO we suggest that, in addition, a trial of thrombolysis is safe and worth attempting, providing stroke best practice recommendations are followed and treatment can be administered promptly. One cannot be certain that the mechanism is thromboembolism unless retinal emboli are seen on ophthalmoscopy and other causes of thromboembolism need to be excluded before GCA can be accepted as the etiology. In our case we cannot be conclusive that thrombosis or that the CRAO was due to GCA alone, but the evidence is supportive of this hypothesis.
Discussion
This case challenges the current management paradigm, it questions the current practice of treating arteritic CRAO with corticosteroids alone. It also introduces the idea of treating arteritic CRAO with dual therapy; corticosteroids to address the inflammatory process of GCA, and IV tPA to manage the thrombotic process. Furthermore, it highlights the importance of early recognition and treatment in CRAO, a point which is also supported by the literature. Most of the literature excludes arteritic cases of CRAO. The outcomes of this case expand the scope and highlight the importance of exploring both arteritic and non-arteritic cases. The outcomes can be very similar, with a marked improvement in vision with rapid infusion of TPA. There is a diagnostic challenge in that it is important to avoid missing GCA, as this could place the eye at risk. However, it is also important to avoid being overly pessimistic and withholding potentially vision-saving thrombolysis if potentially there is a thrombotic or embolic pathogenesis. In practical terms, it may be reasonable to treat for both conditions when uncertain: administer thrombolysis if within the window and promptly initiate IV steroids, provided that there are no contraindications to either.
Whilst the outcomes of the case were promising, there are several limitations that need to be acknowledged. The treatment of this patient with corticosteroid poses as a potential confounder as it may independently improve visual acuity. Further, this was a single patient, with no control patient or group to compare treatment outcomes with. Despite this, it is important to note the importance of this case and acknowledge the fact that IV tPA can be used in the treatment of patients with arteritic CRAO; however, in order to explore this idea, further investigation is warranted.
In terms of research in this area, there are several shortfalls. Firstly, the literature surrounding the use of IV thrombolysis for CRAO is limited to case reports and small-scale studies, there are no proven the efficacy of IV tPA in the context of arteritic CRAO. Given the limited research on the subject, a prospective, multicentered, observational study could offer important insights into the effectiveness of thrombolysis for CRAO secondary to giant cell arteritis. In contrast to randomized controlled studies, which may pose ethical dilemmas by necessitating a placebo group for a potentially vision-threatening illness, an observational method permits the administration of intravenous thrombolysis to all patients identified with GCA-related CRAO. This strategy would enable the collecting of data on the success rates of vision restoration in this particular population, while also permitting thorough monitoring of results and adverse effects.
These limitations highlight gaps in research that can be explored. Most notable RCTs in this area exclude arteritic cases, however the outcomes of this case underscore the importance of including such cases in future literature to ensure a standard of care is set for patients with both arteritic and non-arteritic CRAO. Future work in this area should guide treatment and aim for the development of standardized protocols, including optimal treatment windows, dosages and imaging biomarkers to measure progress. Further, the comparison between mono-therapy (Steroids alone) and dual therapy (steroids and IV thrombolysis) may also be worth exploring in future studies as it may help us further understand the role IV thrombolysis plays in the treatment of arteritic CRAO.
Conclusion
This case report details a unique and noteworthy instance of effective intravenous thrombolysis in conjunction with high-dose corticosteroids in a patient with central retinal artery occlusion secondary to giant cell arteritis. This data illustrates that early reperfusion therapy can be successful in inflammatory etiology, in contrast to most published studies that concentrate on non-arteritic CRAO and systematically exclude arteritic causes. The patient’s marked visual recovery sharply contrasts with the typically lower prognosis of arteritic CRAO managed with steroids alone. Our findings align with evolving literature that supports early IV tPA within 4.5 hours as a promising intervention for CRAO and reinforce the paradigm of considering it an ophthalmic stroke. Importantly, this case extends the border by suggesting that, even in the presence of inflammatory vasculitis, a secondary thrombotic component may make thrombolysis beneficial when provided immediately alongside standard treatment. Nevertheless, evidence remains limited; hence, while our successful outcome supports the dual anti-inflammatory and thrombolytic approach, it remains exploratory. Future research is critical to identify GCA-CRAO patients most likely to benefit from tPA, determine appropriate imaging and biomarker criteria and establish safe and effective protocols that may ultimately shift clinical guidelines.
Conflict of Interest Statement: The authors declare no conflicts of interest.
Funding Statement: The authors declare no funding support for this paper.
Acknowledgements: None.
References
- Chen C, Singh G, Madike R, et al. Central retinal artery occlusion: A stroke of the eye. Eye (Basingstoke). 2024;38(12): 2319-2326.doi:10.1138/s41433-024-03029-w
- Tripathy K, Shah SS, Waymack JR (2024). Central Retinal Artery Occlusion. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan
- Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140(3): 376-391.doi:10.1016/j.ajo.2005.03.038
- Olsen TW, Pulido JS, Folk JC, et al. (2017). Retinal and ophthalmic artery occlusions. Preferred Practice Pattern®. Ophthalmology. 2017;124(2): 120-143.doi:10.1016/jophtha.2016.09.024.
- Lin JC, Song S, Ng, SM et al. (2023). Interventions for acute non-arteritic central retinal artery occlusion. Cochrane Database Syst Rev.2023 Jan 30;1(1):CD1989.doi. 10.102/1465185.CD01989.pub3.
- Hazin R, Dixon JA, Bhatti MT. Thrombolytic therapy in central retinal artery occlusion: cutting edge therapy, standard of care therapy, or impractical therapy? Curr Opin Ophthalmol. 2009;20(3): 210-218. Doi: 10.1097/ICU.0b013e328329b5d5.
- Nakagawara, J, Minematsu, K, Okada, Y, et al. (2010). Thrombolysis with 0.6 mg/kg intravenous alteplase for acute ischemic stroke in routine clinical practice: the Japan post-Marketing Alteplase Registration Study (J-MARS). Stroke 2020;41(9): 1984-1989.
- Chen, C.S, Lee, A.W, Campbell, B, et al. (2011). Efficacy of intravenous tissue-type plasminogen activator in central retinal artery occlusion: report from a randomized, controlled trial. Stroke. 42(8): 2229-2234. doi.org/10.1161/STROKEAHA.110.589606.
- Dumitrascu, OM, Newman NJ, Biousse V. Thrombolysis for central retinal artery occlusion in 2020: time is vision! J Neuroophthalmol. 2020;40(3): 333-345.. doi:1.1097/WNO.0000000000001027.
- Liu Y, Cao S, Zhao Y, et al. Network meta-analysis of different thrombolytic strategies for the treatment of central retinal artery occlusion. Semin Ophthalmol. 2024;39(2): 129-138. doi: 10.1080/08820538.2023.2249549.
- Aldrich, E.M, Lee, A.W, Chen, C.S, et al. Local intraarterial fibrinolysis administered in aliquots for the treatment of central retinal artery occlusion: the Johns Hopkins Hospital experience. Stroke. 2008;39(6):1746-1750. doi: 10.1161/STROKEAHA.107.505404.
- Schumacher M, Schmidt D, Jurklies B, et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. 2010;117(7): 1367-1375.e1.doi: 10.1016,jophtha.2010.03.061
- Cugati, S, Varma, D.D, Chen, C.S, et al. Treatment options for central retinal artery occlusion. Curr Treat Options Neurol. 2013;15(1): 63-77. doi: 10.1007/s119940-012-0202-9.
- Biousse V, Calvetti O, Bruce BB, et al. Thrombolysis for central retinal artery occlusion. J Neuroophthalmol. 2007;27(3): 215-230. Doi:10.1097/WNO.0b013e31814b1f66.
- Donaldson L, Nicholson P, Margolin E. Visual recovery in 2 cases of central retinal artery occlusion treated with prompt intra-ophthalmic artery fibrinolysis. J Neuroophthalmol. 2023;43(3): 383-386. doi.10/1097/WNO.0000000000001785.
- Hayreh SS, Biousse V. Treatment of acute visual loss in giant cell arteritis: should we prescribe high-dose intravenous steroids or just oral steroids? J Neuroophthalmol. 2012;32(3): 278-287.doi: 10.1097/WNO.0b013e3182688218.
- Duff IF, Falls HF, Linman JW. Anticoagulant therapy in occlusive vascular disease of the retina. AMA Arch Ophthalmol. 1951;46(6): 601-617. doi: 10.1001/1rchophth.1951.01700020615001.
- Lee MS, Smith SD, Galor A, et al. Antiplatelet and anticoagulant therapy in patients with giant cell arteritis. Arthritis Rheum. 2006;54(10): 3306-3309. doi: 10.1002/art.22141.
- Donaldson, L, Margolin, E. (2022). Vision loss in giant cell arteritis. Pract Neurol. 22(2): 138-140. doi: 10.1136/practneurol-2021-002972.
- Dziadkowiak, E, Chojdak-Paradowski, B, et al. Isolated arteritis misdiagnosed as bilateral orbital tumors in a patient with acute ischemic stroke. Radiol Case Rep. 2022;17(10): 3927-3932.doi: 10.1016/j.rader.2022.07.023.
- Boulanger JM, Lindsay MP, Gubitz G, et al. Canadian Stroke Best Practice Recommendations for acute stroke management: prehospital, emergency department, and acute inpatient stroke care, 6th edition, update 2018. Int J Stroke. 2018;13(9): 949-984. doi:10.1177/1747493018786616.
“`